
Abstract
Abstract
Purpose:
Recent clinical and experimental studies have reported favorable results when using Rho-associated kinase (ROCK) inhibitors for ocular disease, and in cell culture. Disruption of the human, nonpigmented ciliary epithelial cells (HNPCECs) that comprise the blood–aqueous barrier (BAB) induces anterior uveitis; these cells therefore provide a useful cell model of ocular disease. In this study, we examined the effects of ROCK inhibitors in anterior uveitis and in HNPCECs.
Methods:
Aqueous flare values and intraocular pressures (IOPs) were determined in patients with anterior uveitis, 2 weeks after administration of ripasudil hydrochloride hydrate, a commercial ROCK inhibitor used to treat glaucoma or ocular hypertension. We also investigated the effects of Y-27632, a second ROCK inhibitor, in HNPCECs following exposure to matrix metalloproteinases (MMPs) and human tumor necrosis factor-alpha (TNF-α).
Results:
Patients with anterior uveitis, glaucoma, or ocular hypertension, referred to the Aichi Medical University from February to July 2015, were enrolled. Thirty eyes from 25 outpatients were studied. Aqueous flare values and IOPs were significantly decreased 2 weeks after ripasudil hydrochloride hydrate treatment, with no adverse events. In a cultured HNPCEC monolayer, permeability was markedly increased following exposure to MMPs-1, 3, 9, and TNF-α, with these effects attenuated by exposure to Y-27632. In cultured HNPCECs, Y-27632 provoked a marked alteration in cytoskeletal morphology without a significant change in expression levels of claudin-1 and occludin.
Conclusion:
ROCK inhibitors may confer favorable effects in anterior uveitis, possibly due to a reorganized BAB, although the relevant mechanisms remain unclear.
Introduction
T
Ripasudil hydrochloride hydrate (Glanatec ophthalmic solution 0.4%) is a small-molecule ROCK inhibitor, developed by Kowa Company, Ltd. for the treatment of glaucoma and ocular hypertension. 2 Administered twice daily as eyedrops, this product was approved in Japan in 2014. Ripasudil hydrochloride hydrate is a promising new topical medication to lower intraocular pressure (IOP) for at least 7 h after its administration in patients with primary open-angle glaucoma or ocular hypertension. 3 In monkeys, maximum IOP reduction was observed 2 h after topical instillation of 0.4% ripasudil hydrochloride hydrate, which was 4.36 ± 0.32 mmHg from the baseline IOP, and was significantly stronger than that of 0.005% latanoprost, which was 2.50 ± 0.16 mmHg from the baseline IOP observed 4 h after topical instillation. 4 Further, the survival of retinal ganglion cells after optic nerve crush was increased with oral ripasudil hydrochloride hydrate administration. 5 This effect was revealed by the analysis of Thy-1.2 and Brn3a, retinal ganglion cell markers. Nerve crush induced oxidative stress, including oxidation of lipids and production of reactive oxygen species, was significantly attenuated, and expression of Nox1, which is involved in the nerve crush-induced reactive oxygen species production pathway, was reduced. All these results indicate delayed retinal ganglion cell death and a neuroprotective effect by ripasudil hydrochloride hydrate administration. It may be of value as a neuroprotective treatment for glaucoma and other neurodegenerative diseases.
ROCK inhibitors such as ripasudil hydrochloride hydrate and Y-27632 directly alter the extracellular matrix of the trabecular meshwork, cell shape, and the Schlemm's canal.6–9 ROCK signaling is activated by either secreted bioactive molecules or integrin activation following extracellular matrix binding. This leads to the polymerization of actin stress fibers and the formation of focal adhesions. Actin cytoskeleton-modulation may be involved in aqueous outflow regulation, given that administration of ROCK inhibitors such as HA-1077, AR-12286, and AMA0076 reduced IOP10–12 and altered the cellular characteristics of human trabecular meshwork cells. 12
Okumura et al. demonstrated that ripasudil hydrochloride hydrate transiently alters the morphology of corneal endothelial cells. 13 Ripasudil hydrochloride hydrate and AMA0526, both ROCK inhibitors, were also found to promote corneal endothelial wound healing, which led to their development as an eyedrop formulation for treating acute corneal endothelial damage, particularly following cataract surgery.14,15
As ROCK inhibitors can impact multiple cell types, the inhibition of the ROCK pathway may contribute to clinical benefits, which is yet to be established. Y-27632 inhibited carbachol-induced constriction of ciliary muscle,6,16 suggesting effects in the ciliary body. In addition, apoptosis of nonpigmented ciliary epithelial cells was shown in acute anterior uveitis, 17 with exposure to Y-27632 diminishing the apoptosis. 18 Kaneko et al. indicated that ripasudil hydrochloride hydrate increased outflow facility of the aqueous humor and decreased in IOP due to the disruption of tight junction in Schlemm's canal endothelial cells by disrupting the cellular localization of ZO-1 expression. 19 In keeping with the data reported for wound healing,14,15 Y-27632 also promoted scratch wound healing and enhanced cell migration and adhesion to matrices. 20
We previously proposed an in vitro model of anterior uveitis. 21 Tumor necrosis factor-alpha (TNF-α) and matrix metalloproteinases (MMPs) induce anterior uveitis. We demonstrated an increase in expression of MMP-1, MMP-3, and MMP-9 in the presence of TNF-α, in human, nonpigmented ciliary epithelial cells (HNPCECs). Immunostaining showed that MMP-1, MMP-3, and MMP-9 degraded claudin-1 and occludin in HNPCECs and in nonpigmented ciliary epithelial cells of the swine ciliary body. In a monolayer of HNPCECs, we showed that permeability was significantly increased with each MMP treatment. Thus TNF-α increased MMP levels within the cells that comprise the blood–aqueous barrier (BAB), and these then degraded components of tight junctions, resulting in increased BAB permeability.
In the present study, we examined aqueous flare values and IOPs in anterior uveitis patients with glaucoma or ocular hypertension who were treated with ripasudil hydrochloride hydrate. We also investigated the effects of Y-27632 in TNF-α and MMP-exposed HNPCECs using a cell-based permeability assay and assessed cellular morphology in conjunction with claudin-1 and occludin expression levels. Our data suggest that ROCK inhibition may confer favorable effects in anterior uveitis, although the underlying mechanisms remain unclear.
Methods
Patients
This retrospective study was conducted at Aichi Medical University Hospital. The study protocol was in accordance with the tenets of the Declaration of Helsinki. The institutional review board granted approval (reference No.: ASAI20161001), and clinical trial registration number is UMIN000022560 (May 2016). Anterior uveitis patients with glaucoma or ocular hypertension that consulted MZ at Aichi Medical University from February 1st, 2015 to July 31th, 2015 were enrolled. Exclusion criteria were corneal disease, primary glaucoma, exfoliation syndrome, and glaucoma, or a history of trauma or surgery to the globe. Patients who had small-incision cataract surgery more than 1 year previously were included.
Examinations
Each visit included a complete ophthalmologic examination, including slit-lamp biomicroscopic examination, Goldmann applanation tonometry, and indirect ophthalmoscopy. Anterior chamber flare was evaluated based on the aqueous flare value measured with the Kowa FM-600 laser flare meter (Kowa Medicals, Nagoya, Japan) in photon counts per millisecond (pc/ms). Best-corrected visual acuity (BCVA) was assessed using a Landolt broken ring, and the logarithm of the minimal angle of resolution (LogMAR) value was calculated for statistical analyses. A clinical diagnosis of anterior uveitis was based on history, typical slit-lamp biomicroscopic, and fundus findings. To assist with diagnoses; peripheral blood samples were taken from patients who gave their approval for lysozyme, angiotensin-converting enzyme and human leukocyte antigen analyses to be conducted.
This study included patients with anterior uveitis, regardless of intermediate and/or posterior uveitis. Uveitis was classified according to the Standardization of Uveitis Nomenclature consensus. 22 Anterior uveitis included iritis, iridocyclitis, and anterior cyclitis, with the primary site of inflammation being the anterior chamber. Intermediate uveitis included pars planitis, posterior cyclitis, and hyalitis, with the primary site of inflammation being vitreous. Posterior uveitis included choroiditis, chorioretinitis, retinochoroiditis, retinitis, and neuroretinitis, with the primary site of inflammation being the retina or choroid.
Treatment
All patients were treated with 2 times per day of 0.4% ripasudil hydrochloride hydrate for more than 2 weeks and 1 mg/mL of betamethasone sodium phosphate eyedrops (Rinderon ophthalmic solution; Shionogi & Co., Ltd., Osaka, Japan) 1–6 times daily, depending on the severity of anterior uveitis. Eight patients were treated with 5 mg to 20 mg/day systemic oral prednisolone (Predonine; Shionogi & Co., Ltd.). For the treatment of glaucoma or ocular hypertension, we used prostaglandin analogs [travaprost 0.004%; (TravatanZ; Alcon, Inc., Tokyo, Japan), bimatoprost 0.03% (Lumigan; Senju Pharmaceutical Co., Ltd., Osaka, Japan), latanoprost 0.005% (Xalatan; Pfizer, Inc., Tokyo, Japan)], an alpha agonist (brimonidine tartrate 0.1%; Aiphagan; Senju Pharmaceutical Co., Ltd.), beta blockers (timolol maleate 0.5%; Timoptol XE; Santen Pharmaceutical Co., Ltd., Osaka, Japan), and carbonic anhydrase inhibitors [brinzolamide ophthalmic suspension 1% (Azopt; Alcon, Inc.), dorzolamide HCI 1% (Trusopt; Santen Pharmaceutical Co., Ltd.)]. The topical medications applied for glaucoma or ocular hypertension in the participants of this study are shown in Tables 1 and 2; oral acetazolamide was not used. In measuring aqueous flare value, tropicamide and phenylephrine hydrochloride eyedrops were excluded as such treatments can influence the aqueous flare value. 23 No topical or oral medications, including dosage, were altered following the commencement of ripasudil hydrochloride hydrate administration.
Topical medications used for glaucoma or ocular hypertension in this study included prostaglandin analogs [travaprost 0.004% (Travatan Z, Alcon, Inc., Tokyo, Japan), bimatoprost 0.03% (Lumigan, Senju Pharmaceutical Co., Ltd., Osaka, Japan), latanoprost 0.005% (Xalatan, Pfizer, Inc., Tokyo, Japan)], an alpha agonist (brimonidine tartrate 0.1%; Aiphagan, Senju Pharmaceutical Co., Ltd.), beta blockers (timolol maleate 0.5%; Timoptol XE, Santen Pharmaceutical Co., Ltd., Osaka, Japan), carbonic anhydrase inhibitors [brinzolamide ophthalmic suspension 1% (Azopt™, Alcon, Inc.), and dorzolamide HCL 1% (Trusopt, Santen Pharmaceutical Co., Ltd.)]. All participants were administered with ripasudil hydrochloride hydrate (Glanatec ophthalmic solution 0.4%).
A, alpha agonist; B, beta blocker; B27, HLA-B27 related acute anterior uveitis; BCVA, best-corrected visual acuity; BD, Behçet disease; C, carbonic anhydrase inhibitor; DM, diabetes mellitus iridocyclitis; HSV, Herpes simplex virus anterior uveitis; IOP, intraocular pressure; LF, aqueous flare value measured with laser flare meter; LogMAR, logarithm of the minimal angle of resolution; P, prostaglandin analog; Sa, Sarcoidosis; UK, unknown; VKH, Vogt–Koyanagi–Harada disease; VZV, varicella-zoster virus iridocyclitis.
Outcomes
The primary outcomes were aqueous flare value and IOP, before and 2 weeks after administering ripasudil hydrochloride hydrate. The follow-up for each patient was 2 weeks after initiating treatment with ripasudil hydrochloride hydrate eyedrops.
Cell culture
HNPCECs were purchased from ScienCell Research Laboratories (Carlsbad, CA) and maintained in tissue culture flasks (Biocoat Poly-
For cytoskeletal staining, cells were cultured on coverslips (Matsunami, Osaka, Japan), precoated with BD Matrigel Basement Membrane Matrix (BD Biosciences, Bedford, MA) diluted at 1:100. Cells were cultured in Epithelial Cell Medium (EpiCM; ScienCell Research Laboratories) supplemented with 2% fetal bovine serum (FBS), an epithelial cell growth supplement (EpiCGS, Cat. No. 4152; ScienCell Research Laboratories), and penicillin/streptomycin (P/S) solution (Cat. No. 0503; ScienCell Research Laboratories). Cells were allowed to reach confluence and were then subcultured into a 6-well plate (Biocoat Poly-
Drug exposure experiments using the cell model
For the cell-based permeability assay and western blot analyses, confluent HNPCECs cultured in EpiCM supplemented with 2% FBS were exposed for 5 min to recombinant human MMP-1 (10 ng/μL; R&D Systems, Inc., Minneapolis, MN), MMP-3 (10 ng/μL; R&D Systems, Inc.), or MMP-9 (10 ng/μL; R&D Systems, Inc.), and for 24 h to recombinant human TNF-α (10 ng/mL; R&D Systems, Inc.). Confluent HNPCECs were also exposed to Y-27632 (50 μM), in the same culture conditions, for 72 h. For the cytoskeletal staining, HNPCECs were exposed to Y-27632 (50 μM) for 24 h as described later.
Cell-based permeability assay
For the detection of macromolecular passage across a cellular monolayer, a tracer solution was prepared by adding 50 μg/mL bovine serum albumin (BSA) conjugated to Alexa Fluor® 488 (Life Technologies) to the cell culture medium. Before our analyses, the apical chamber of a dual-chamber cell culture well (BD Falcon 24-well Cell Culture Insert Companion Plate; pore size: 0.4 μm; Becton Dickinson and Company, Franklin Lakes, NJ) was coated with poly-
Sodium dodecyl sulfate–polyacrylamide gel electrophoresis
Confluent HNPCECs after Y-27632 treatment at each concentration were homogenized in lysis buffer (20 mM TrisHCl, 150 mM NaCl, 2 mM EDTA, 1 mM EGTA, 1% Triton X-100, 0.1 mM phenylmethanesulfonyl fluoride, 1 μg/mL leupeptin; pH 7.4) and incubated on ice for 1 h as described previously. 21 Homogenates were centrifuged at 15,000g at 4°C for 30 min and pellets loaded onto a AnyKD polyacrylamide gel (Bio-Rad Laboratories, Inc.), under reducing conditions, for analyses of occludin. Confluent HNPCECs were lysed with CelLyticM Cell Lysis Reagent (Sigma). Samples were subject to protein extraction using 6 M guanidine HCl, 100 mM TrisHCl (pH 8.0), and 150 mM NaCl. The protein extracts were treated with 1% protease inhibitor cocktail (Sigma) and incubated at 4°C for 48 h. The samples were then treated with Benzonase nuclease (Novagen, Madison, WI) and loaded on an AnyKD polyacrylamide gel (Bio-Rad Laboratories, Inc.) under reducing conditions for analyses of claudin-1 and occludin.
Western blotting
Western blot analyses were with the rat anti-human claudin-1 antibody (1:1,000; R&D Systems, Inc.) and mouse anti-human occludin antibody (1:1,000; R&D Systems, Inc.), respectively. 21 Human claudin-1 was detected using horseradish peroxidase-conjugated goat anti-rat immunoglobulins (1:5,000; ZYMED, San Francisco, CA); human occludin was detected with horseradish peroxidase-conjugated goat anti-mouse immunoglobulins (1:5,000; DakoCytomation, Glostrup, Denmark). Molecular weights were estimated using protein standards (Invitrogen, Thermo Fisher Scientific, Yokohama, Japan). Band densities were quantified with Image J software (US National Institutes of Health, http://rsb.info.nih.gov/ij).
Cytoskeletal staining
HNPCECs were cultured at 2 × 105 cells in 200 μL of culture medium for 24 h, and then 2 mL of EpiCM with or without Y-27632 (50 μM) was added to the culture medium. After additional incubation for 24 h, cells were then washed twice with PBS, fixed with 4% formaldehyde in PBS for 10 min at room temperature, and washed again twice with PBS. The fixed cells were incubated with 50% Starting Block T20 (PBS) Blocking Buffer (Thermo Fischer Scientific K.K., Yokohama, Japan) in TBS containing 0.1% Tween-20 (TBST) for 15 min at room temperature and washed again 4 times with PBS, then incubated in rhodamine–phalloidin (Cat. No. R415; Thermo Fisher Scientific K.K.; Molecular Probes) to visualize actin cytoskeleton. After washing 4 times with PBS, coverslips were inverted onto glass slides (Matsunami), mounted within DAPI-Fluoromount-G (Southern Biotech). The slides were sealed using Mount Quick (Daido Sangyo, Tokyo, Japan). The stained cells were analyzed by a scanning confocal microscope LSM 700 (Zeiss, Tokyo, Japan), using 10% laser power. Samples were detected with 543 or 388 nm laser excitation and double immunofluorescence-labeled view using sequential scanning. Actin cytoskeleton-stained rhodamine was observed using 543 laser with +893 gain and −1 offset. DAPI was observed using 388 laser with +622 gain and −10 offset. These images were obtained with 20 × objective lens. Scanning was done at a pinhole size at 1.0 airy unit and 8 times line average. Whole-cell view was observed with maximum projection of 9 z-stacks images.
Statistical analyses
Our results are presented as the mean ± standard deviation (SD), or median (with interquartile range). The change in aqueous flare values and IOPs following exposure to ripasudil hydrochloride hydrate were analyzed by using the paired t-test or Wilcoxon's signed rank test as appropriate. For the cell-based permeability assays, we defined permeability without MMPs or TNF-α as the control value. Two group comparisons of permeability were performed using the Student's t-test. The effect of multiple medications was analyzed using one-way analysis of variance with Tukey's test for multiple comparisons. All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC), with P values of <0.05 considered to be statistically significant.
Results
A total of 30 eyes from 25 outpatients were included in our analyses. Individual data of patients participating in this study are shown in Table 2. Our patient cohort comprised 11 men and 14 women, with a mean age ± SD of 57.9 ± 15.2 years (range, 19–76 years). The mean follow-up period, before commencement with the ripasudil hydrochloride hydrate treatment was 16.4 ± 4.7 weeks. Table 3 shows the summary of diagnoses of anterior uveitis in the patients who participated in this study and each number. From the positional point of view, we identified anterior uveitis, anterior with intermediate uveitis, and panuveitis, at frequencies of 24%, 24%, and 52%, respectively.
Aqueous flare values, IOPs and BCVAs before and after ripasudil hydrochloride hydrate treatment
Figure 1A and B shows the aqueous flare values and IOPs for patients before and after ripasudil hydrochloride hydrate treatment, as measured by laser flare meter and the Goldmann applanation tonometer, respectively. The aqueous flare values before and after treatment were 16.6 (10.3, 27.0) and 12.3 (7.0, 23.3) pc/ms, respectively. The IOPs before and after treatment were 20.1 ± 6.1 and 16.9 ± 5.0 mmHg, respectively. Both values significantly decreased after ripasudil hydrochloride hydrate treatment (P = 0.024 and P < 0.001, respectively). Mean visual acuity (LogMAR) was 0.28 ± 0.29 and 0.22 ± 0.25 before and after the treatment, respectively, which was found to be statistically significant (P = 0.003).

Aqueous flare values and intraocular pressures before and after ripasudil hydrochloride hydrate treatment, analyzed by laser flare meter and a Goldmann applanation tonometer, are shown with box-whisker plots.
A confounding effect of multiple medications on the aqueous flare and IOP was analyzed, and it is shown in Table 4. There was no evidence that the number of medications affected the change in the aqueous flare and IOP (P = 0.33 and 0.056, respectively). The baseline values in LF and IOP were dependent on the number of medications because the serious patients tended to receive more medications. It is difficult to conclude the effect of multiple medications in the present study due to nonrandomization with small-sample size.
n Is the number of eyes. Data are expressed as mean (SD). Difference = after − before.
Indicates P value for the comparison before and after treatment from the paired t-test.
Indicates P value for the comparison among the number of medications from the one-way analysis of variance.
Indicates P value for the pairwise comparison between the number of medications using the Tukey test.
SD, standard deviation.
The increased HNPCEC permeability provoked by exposure to MMP-1, MMP-3, MMP-9, and TNF-α was significantly attenuated by Y-27632
To evaluate the impact of increased MMP and TNF-α expression on the integrity of a cellular barrier, we examined the permeability of a HNPCEC monolayer to a high-molecular-weight fluorescent BSA conjugate (n = 4) (Fig. 2A). For the MMP treatments, the permeability values of controls (±Y-27632) were 48 ± 6 and 47 ± 8, increasing to 315 ± 57 and 154 ± 24 with the addition of MMP-1, 193 ± 33 and 137 ± 21 for MMP-3, and 257 ± 44 and 133 ± 17 for MMP-9 (Fig. 2B). The equivalent values following TNF-α exposure were, in controls, 45.0 ± 6.3 and 43.0 ± 5.7, and following TNF-α addition, without and then with Y-27632, 71.0 ± 7.4 and 42.5 ± 6.8, respectively. A significant increase in fluorescence-conjugated BSA permeability was detected after 5-min treatments with the MMPs or following a 24-h exposure to TNF-α. This increased permeability was significantly attenuated by the inclusion of Y-27632 for MMP-1 (P = 0.002), MMP-3 (P = 0.028), MMP-9 (P = 0.002), and TNF-α (P = 0.001), as shown in Fig. 2B; exposure to Y-27632 alone, provoked no changes in permeability.
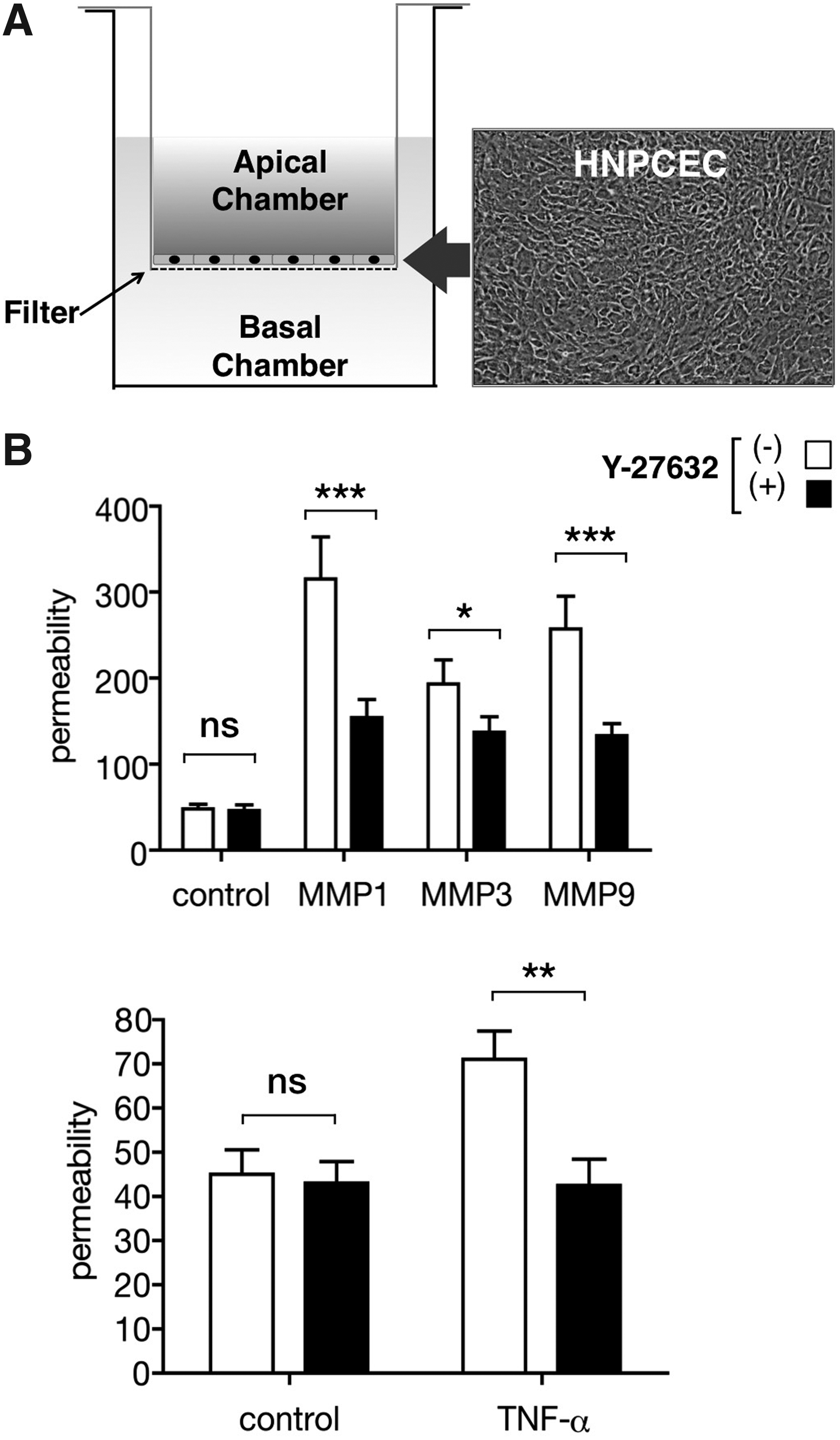
Relative permeability measured for a monolayer of HNPCECs following exposure to MMP-1, −3, or −9, and human TNF-α, with or without Y-27632.
Expressions of claudin-1 and occludin following exposure to Y-27632 with and without MMP-1, MMP-3, and MMP-9 treatments
Western blot analyses of HNPCEC samples probed with anticlaudin-1 and antioccludin antibodies revealed bands corresponding to the predicted molecular weights of the claudin-1 and occludin proteins (Fig. 3A). Claudin-1 and occludin migrated as 23- and 65-kDa proteins, respectively. Protein expression levels, evaluated before and after exposure to Y-27632 by quantitative band densitometry, revealed no significant changes (data not shown), irrespective of the concentration of Y-27632 used (2, 10, 50 μM).
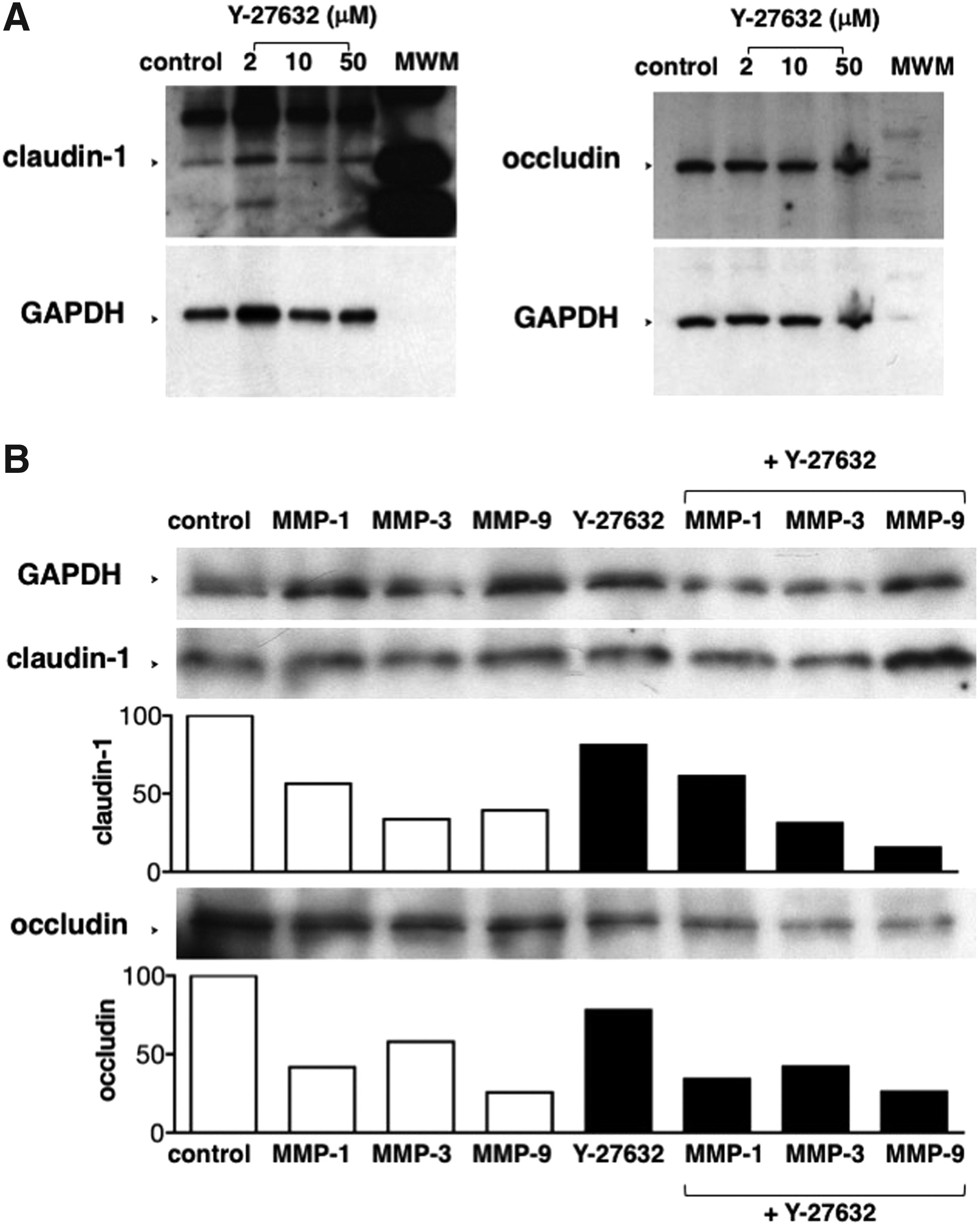
Expressions of claudin-1 and occludin following exposure to Y-27632 with and without MMP-1, MMP-3, and MMP-9 treatments.
Relative expression levels of claudin-1 and occludin were quantified with the band densities and were normalized to the expression levels of GAPDH. The levels of claudin-1 and occludin were attenuated after treatment with MMP-1, MMP-3, and MMP-9 as previously we reported, 21 but showed no prominent difference in the presence or absence of Y-27632 (Fig. 3B).
Effects of Y-27632 on cytoskeleton of HNPCECs
Next, effects of Y-27632 on cell shape and actin stress fibers of HNPCECs were analyzed (Fig. 4). Cell bodies possessed an appearance exhibiting long thin filamentous actin cytoskeleton accompanied by the extension of long filopodia (Fig. 4, arrows) homogeneously throughout the cells after treatment with Y-27632, while cell–cell separation was distinct and the actin cytoskeleton formed stress fibers (Fig. 4, arrowheads) without Y-27632 treatment.
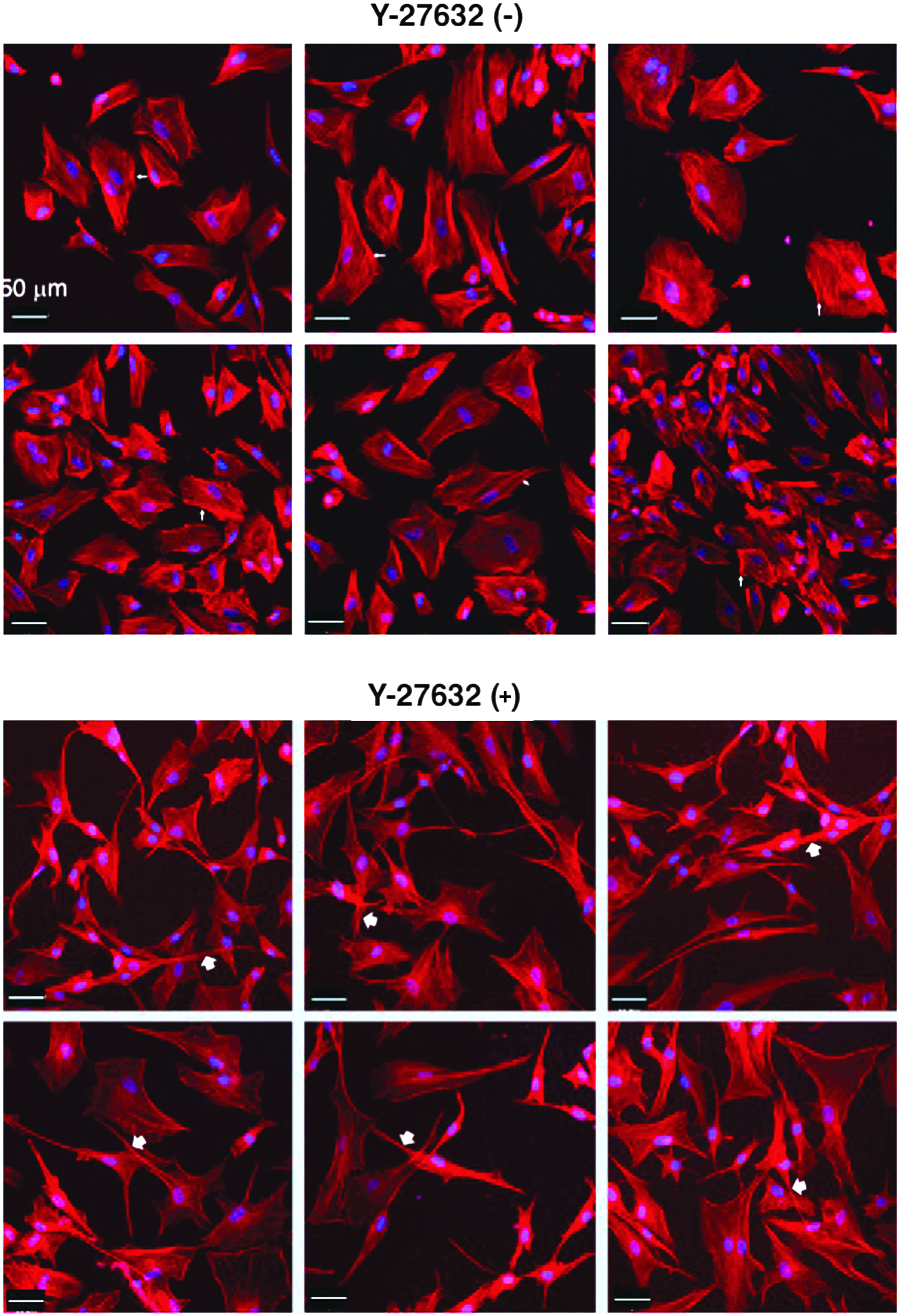
Effects of Y-27632 on cell shape and actin stress fibers of HNPCECs. HNPCECs were treated with (upper panel) or without (lower panel) Y-27632. Long thin filamentous actin cytoskeleton accompanied by the extension of filopodia (arrows) was shown after treatment with Y-27632, while cell–cell separation was distinct and the actin cytoskeleton formed stress fibers (arrowheads) without Y-27632 treatment. Actin fibers were stained by rhodamine–phalloidin (red) and DAPI was used to stain nuclei (blue) as described in Methods section. Scale bars denote 50 μm.
Discussion
Clinical studies have shown the beneficial effects of the ROCK inhibitor, ripasudil hydrochloride hydrate, for glaucoma and ocular hypertension2,3 and for corneal endothelial cells.13,24 These data demonstrated the transfer of the ROCK inhibitor from the surface of the cornea to the anterior chamber, where the inhibitor may directly contribute to wound healing at the BAB. In the present study, we show that a ROCK inhibitor decreased both the IOP values, and aqueous flare, in patients with anterior uveitis. Using HNPCEC monolayers, we also found that permeability was increased by the addition of MMP-1, MMP-3, MMP-9, and TNF-α treatments and was significantly attenuated by the ROCK inhibitor. Although protein expression levels of claudin-1 and occludin were unaltered by exposure to the ROCK inhibitor, altered cell shape was evident. There were no significant differences observed in the bands of claudin-1 and occludin in the presence or absence of Y27632, which implicates that the attenuation of the MMP-mediated increase in permeability in HNPCECs by the Y27632 may not be mediated by the expression levels of claudin-1 and occludin. The precise mechanisms underlying these favorable effects of ROCK inhibitors in anterior uveitis remain unclear and warrant further study.
In this study, the ripasudil hydrochloride hydrate eyedrop solution resulted in an inhibitory effect on inflammation in the anterior chamber. ROCK is considered to induce inflammation,25,26 with the suppression of inflammation a plausible outcome of its inhibition.27,28 Previous reports indicated the ability of ROCK inhibitors to reduce inflammation, particularly in ocular diseases. Lee et al. investigated the effect of the Y27632 on corneal xenotransplantation and showed Y27632 promoted corneal endothelial cell proliferation, prevented corneal endothelial cell death, and enhanced in vitro wound healing. 29 It suggests the application of the Y27632 may provide a novel therapy to reduce inflammation in corneal xenotransplantation. Hollanders et al. showed that targeting ROCK with AMA0428 not only reduced neoangiogenesis but also blocked inflammation and fibrosis (contrary to VEGF suppression), which indicates a potential therapeutic benefit of ROCK inhibition in neovascular age-related macular degeneration. 30 Further, the promotion of wound healing by ripasudil hydrochloride hydrate was also demonstrable,15,31 although, again, the mechanistic aspects of this outcome remain unclear. These reports support anti-inflammatory effect of ripasudil hydrochloride hydrate in anterior uveitis as shown in the present study.
In this study, our patient cohort was limited to patients with anterior uveitis. In a previous clinical study, mean IOP reduction following the administration of ripasudil hydrochloride hydrate eyedrop in patients with glaucoma and ocular hypertension were −6.4 mmHg at 2 h after the first dose (−2.0 mmHg for placebo) and −7.3 mmHg, 2 h after the second dose (−4.1 mmHg for placebo), respectively. 3 In our present study, IOPs before and after the ripasudil hydrochloride hydrate eyedrop treatments were 20.1 ± 6.1 and 16.9 ± 5.0 mmHg, respectively, with a difference of −3.2 mmHg. The differences between these 2 data sets may be derived from the influence of anterior uveitis.
Cell shape may well be of importance for BAB function. Collectively, MMPs and TNF-α provoke a variety of inflammatory responses,32–34 and we previously indicated that MMPs and TNF-α were candidate triggers for uveitis in an in vitro model of Behçet disease. 21 In our previous model, claudin-1 and occludin were involved in the disruption and healing of tight junctions in the BAB. 21 Ripasudil hydrochloride hydrate decreases IOP by increasing outflow facility in association with the modulation of trabecular meshwork cell behavior and Schlemm's canal endothelial cell permeability in association with disruption of tight junction. 19 ROCK inhibitors are known to alter cell shape.9,12,13 In our present study, the absolute expression levels of claudin-1 and occludin were not changed by Y-27632, but altered cell shapes. We anticipate this morphological change in HNPCECs, which may contribute favorable effects in anterior uveitis, possibly due to a reorganized BAB.
The effect of Y-27632 shows different aspects, which implicates that the effect is not one sided. Ma et al. showed ROCK signaling in bradykinin-induced increase in murine blood-tumor barrier permeability was inhibited by Y-27632, and cytoskeleton rearrangement and disassembly of tight junction proteins such as occludin and claudin were associated with this inhibition. 35 Similarly Breslin et al. suggested that ROCK promoted microvascular leakage in association with actin–myosin-mediated tension development in porcine coronary venular endothelial cells, and it was inhibited by Y-27632. 36 Thus some reports showed ROCK inhibitor Y-27632 decreased permeability model in vitro. On the contrary, Rao et al. showed human Schlemm's canal primary cell monolayer permeability increased in response to Y-27632 treatment. 7 Darenfed et al. showed Y-27632 enhanced wound closure rates in mouse fibroblast cells with demonstrating the formation of thin actin-rich membrane extensions, a phenotype that closely resembles the reduction of ROCK-I. 37 However, Honjo et al. showed Y-27632 inhibited wound healing and fibroproliferation in rabbit glaucoma filtration surgery model. 38 The effects of Y-27632 analyzed on such as cell permeability and wound healing may have different aspects in different organs and cells assayed, which implicate that the effect of ROCK inhibitors may not be one sided.
In the present study, the HNPCECs treated with Y-27632 alone showed obvious detectable effect on morphology, but did not show detectable effect on monolayer permeability. We speculate HNPCECs at confluent condition have already reached minimum level on monolayer permeability, and thus Y-27632 may not decrease the permeability any more.
To conclude, we anticipate that ROCK inhibitors may have favorable effects not only in glaucoma and ocular hypertension but also in anterior uveitis. Further clinical studies are now needed to corroborate the clinical utility of ROCK inhibitors.
Footnotes
Author Disclosure Statement
M.G. received writing fees from Kowa Company, Ltd. All other authors have no competing financial interests.