
Abstract
Abstract
Uveitis is one of the fields in ophthalmology where a tremendous evolution took place in the past 25 years. Not only did we gain access to more efficient, more targeted, and better tolerated therapies, but also in parallel precise and quantitative measurement methods developed allowing the clinician to evaluate these therapies and adjust therapeutic intervention with a high degree of precision. Objective and quantitative measurement of the global level of intraocular inflammation became possible for most inflammatory diseases with direct or spill-over anterior chamber inflammation, thanks to laser flare photometry. The amount of retinal inflammation could be quantified by using fluorescein angiography to score retinal angiographic signs. Indocyanine green angiography gave imaging insight into the hitherto inaccessible choroidal compartment, rendering possible the quantification of choroiditis by scoring indocyanine green angiographic signs. Optical coherence tomography has enabled measurement and objective monitoring of retinal and choroidal thickness. This multimodal quantitative appraisal of intraocular inflammation represents an exquisite security in monitoring uveitis. What is enigmatic, however, is the slow pace with which these improvements are integrated in some areas. What is even more difficult to understand is the fact that clinical trials to assess new therapeutic agents still mostly rely on subjective parameters such as clinical evaluation of vitreous haze as a main endpoint; whereas a whole array of precise, quantitative, and objective modalities are available for the design of clinical studies. The scope of this work was to review the quantitative investigations that improved the management of uveitis in the past 2–3 decades.
Introduction
C
Outcome measurements for uveitis in the past
In 1959, the Proctor group at University of California San Francisco (UCSF) published two articles in which the authors put forward a grading system for anterior uveitis 1 and a classification of the posterior manifestations of uveitis. 2 Their work represented an important development, especially for the grading of inflammation of the anterior segment that was systematized for flare and cells. Both flare and cells were graded from 0+ to 4+, which allowed clinicians to have a unified system to determine the level of inflammation. In 1985, Nussenblatt et al. proposed a grading system for the evaluation of vitreous haze in intermediate and posterior uveitis based on a set of photographs of vitreous haze from absent haze to very dense haze with which the vitritis in the patients' eyes was compared. Vitreous haze was graded from 0+ to 4+. 3
These evaluation methods were taken over, respectively, 46 and 20 years later, almost integrally, during a consensus conference on the standardization of uveitis nomenclature (SUN). 4 When these scoring systems were proposed, in the past, they certainly represented a progress. Nevertheless, these evaluation methods were essentially subjective, qualitative, or semi-quantitative at most for anterior chamber cells, evaluation methods. Rejuvenated by the SUN publication in 2005, they were recommended to be used as outcome measures in uveitis trials and became the standard to design study protocols for clinical trials. Numerous trials were performed by using outcome criteria that were based on such subjective grading systems, including anterior chamber flare examined by slit-lamp or vitreous haze score (VHS) using comparative photographs. These scoring systems had only 4 grades of severity and, hence, were not very adequate to obtain statistically significant results. The uneasiness in the design of clinical trials and the choice of outcome measures for posterior segment uveitis has been noted in a recent article titled: “Heterogeneity of primary outcome measures used in clinical trials of treatments for intermediate, posterior and panuveitis.” 5
Quantitative outcome measures for uveitis
In the meantime, tremendous progress had been achieved in quantifying intraocular inflammatory parameters, including fluorescein angiography (FA) in 1964, 6 indocyanine green angiography (ICGA) 7 and laser flare photometry (LFP)8–12 in the early 1990s, retinal optical coherence tomography (OCT),13–18 and choroidal enhanced-depth imaging OCT (EDI OCT). 19 Some more modalities have emerged in the recent past, such as fundus autofluorescence (FAF) 20 or OCT angiography (OCT-A), for which it will take some time to know whether they will contribute usable quantitative data.
All these methods have contributed to transform uveitis into a precise clinical science. Many of them have been standardized, such as LFP, 21 FA, and ICGA22,23 representing quantitative numbered parameters and outcome measures. The problem was that these methods only reluctantly found their way into routine uveitis practice in specialized uveitis centers and are still not used as outcome measures in clinical trials.
Fluorescein and indocyanine green angiography
One of the essential procedures performed in uveitis to complement clinical appraisal of the patient with intraocular inflammation is angiographic investigation of the posterior segment. Angiography may be performed to confirm elements already revealed by clinical examination or other investigational methods such as OCT. A second reason to perform an angiography is to better grade the inflammation of the fundus. A third reason is to have a good baseline record of inflammatory involvement to subsequently use it for follow-up purposes. In follow-up situations, angiography is usually performed to monitor disease intensity and impact of therapy. Astonishingly, angiography has rarely been used as one of the outcome measures in clinical trials on posterior uveitis, although it allows quantification of inflammatory involvement of both the retina (FA) and the choroid (ICGA) if an angiographic scoring system is used.
One drawback of angiography is that it is invasive, costly, and time consuming. Therefore, attempts are made to find alternative methods that could replace angiography. Much hope to achieve this has been put into OCT for the investigation of both the retina and the choroid. Retinal OCT clearly is unable to replace FA, as it is merely giving morphological data and cannot account for vascular leakage so crucial to establish the activity of inflammation and to monitor its follow-up evolution. Similarly, OCT-A can show drop-out of retinal vessels (superficial or deep) as well as choriocapillaris, but it cannot be used to measure intensity of retinal inflammation/vasculitis.
In recent years, there has been substantial interest in the possibility of using EDI OCT to replace ICGA. Although EDI OCT is a non-invasive tool that might be useful for the long term follow-up of stromal choroiditis such as Vogt-Koyanagi-Harada (VKH) disease or birdshot retinochoroiditis (BRC), it was shown not to be suited for precise and close monitoring of choroiditis during the acute phase of these diseases when therapeutic adjustment is crucial. 24 In addition, both FA and ICGA have a substantial advantage, as they do not only give information on the posterior pole but also encompass the whole fundus. In the same line of thought, angiography has become even more performed by the introduction of wide-field or ultra-wide-field (UWF) angiography. 25
Fluorescein angiography
FA has been performed for more than 40 years. 6 Because fluorescein sodium fluoresces in the wavelengths of the visible light, it mainly gives information on the superficial structures of the fundus and mostly only confirms signs already known to the clinician, as in most instances OCT is already available when FA is performed. However, it gives quantifiable information on superficial inflammation of the fundus, including optic disc and retina, 26 and many times reveals leakage not detected by OCT, apart from analyzing a much wider area of the retina.
Fluorescein angiographic concepts classically described also apply to inflammatory diseases. Increased fluorescence can be due to three main mechanisms: (1) leakage producing pooling (in a space) or staining (in tissues); (2) increased transmission of fluorescence due to fundus atrophy with removal of the RPE producing larger hyperfluorescent areas or due to smaller window defects produced by areas of RPE defects; and (3) presence of abnormal vessels (retinal vessels or choroidal neovascular membranes). Decreased fluorescence can be due to either transmission decrease (blockage) or filling defect (vascular delayed perfusion or non-perfusion). 27
Specific inflammatory FA signs relevant to investigate uveitis comprise disc hyperfluorescence to establish optic disc inflammation, macular edema that has been well graded in the literature, retinal vascular staining or leakage, capillary leakage, retinal nonperfusion, neovessels on the disc and/or in the periphery as well as subretinal staining and pooling, and all FA signs that can be graded to obtain a precise evaluation of superficial posterior inflammatory involvement (see later).
Because of the narrow field of view in conventional FA, peripheral sweeps and montage photography are essential to document peripheral retinal inflammatory lesions, retinal vasculitis, and retinal nonperfusion. On the other hand, this technique is biased by the montage of frames taken at different time points during dye transit. UWF FA can capture up to 200° of the fundus in a single frame and allows imaging of a mean 1.5 × the area captured by montage photography. 25 Additional major advantages of UWF FA include improved imaging through small pupils and simultaneous imaging of the posterior pole and the retinal periphery during dye transit. 28 Furthermore, high-resolution images allow better identification of peripheral microvascular architecture. Several studies have shown that the use of UWF FA may improve management of uveitis patients.28–32
ICGA (choroidal angiography)
For the past 20 years, a second angiographic procedure has been available using indocyanine green, a dye that fluoresces in the infrared wavelengths and, therefore, allows imaging of the choroid that was poorly accessible to imaging beforehand. It gives crucial information on choroidal inflammatory involvement. The procedure, in contrast to FA, gives often additional information, undetected by clinical examination or FA or OCT. Therefore, to make a proper assessment of inflammatory involvement in posterior segment uveitis, ICGA is indispensable, as it gives information that is otherwise unrecognized. ICGA has very often a diagnostic value as well, which is rarely the case for FA. For all these reasons, in most cases where angiographic work-up is decided and choroidal involvement cannot be excluded, dual FA and ICGA should be performed. As this type of angiography is much less familiar than FA to the clinician, the procedure and its interpretation will be dealt with in a more detailed manner.
When analyzing ICGA in posterior inflammatory disorders, important differences with FA interpretation have to be borne in mind to correctly analyze the images obtained. During initial circulation, ICG is comparable to fluorescein showing the passage through arteriovenous compartments, except that it shows superimposed retinal and choroidal circulations. The difference occurs during recirculation time when ICG is progressively leaking out from the fenestrated choriocapillaris, gradually and physiologically impregnating the whole choroidal thickness. A standard protocol to analyze ICG behavior in choroiditis has been designed.7,33
Interpretation of ICGA 7
Decrease and increase in fluorescence are the two ways by which pathological changes affecting the choroid can manifest in ICGA.
The impregnation of the choroidal space can be decreased or absent (hypofluorescence). Two main mechanisms have been identified:(1) decrease of the physiological extrusion of the ICG from the choriocapillaris (non-perfusion or hypoperfusion) that takes a confluent geographic aspect34,35 and is seen in primary inflammatory choriocapillaropathies, including multiple evanescent white dot syndrome (MEWDS), acute posterior multifocal placoid pigment epitheliopathy (APMPPE), and multifocal choroiditis;36–38 (Fig. 1A) (2) impairment of the filling of the choroidal tissue by the ICG molecule because of the presence of space-occupying lesions (inflammatory foci) that tend to be round even in size and regularly distributed (Fig. 1B).39,40 The latter lesions are hypofluorescent in the intermediate angiographic phase. If they remain hypofluorescent in the late phase, this signifies that the inflammatory lesion occupies the whole thickness of the choroidal stroma. This should not be confused with focal atrophy of the RPE and of the whole choriocapillaris and choroid tissues; that is, atrophic scars with visualization of the sclera. When lesions become isofluorescent in the late angiographic phase, inflammation causes only partial thickness infiltrates. This type of mechanism characterizes stromal choroiditis entities such as VKH disease, BRC, sarcoidosis, and ocular tuberculosis.41–44 Thus, in ICGA performed for inflammatory disorders, the main information is obtained less from the analysis of the early circulatory phase than from the analysis of the altered pattern of the filling of the choroidal space.

On the other hand, impregnation of the choroidal space can be enhanced (hyperfluorescence) by increased leakage from the larger choroidal vessels, which adds to the physiological background fluorescence coming from the leakage through the fenestrations of the choriocapillaries. The vessels appear fuzzy in the intermediate time frames, and extrusion of the dye from large vessels causes late diffuse hyperfluorescence. In case of the presence of inflammatory foci in the choroidal stroma, hyperfluorescence is associated with hypofluorescent dark dots due to inflammatory infiltrates. ICGA showed occult choroidal lesions, not shown by fundoscopy and/or FA in 100% of patients with a well-established diagnosis known to involve the choroid, and these findings had an essential impact either on diagnosis or on management in 12.3% of these cases, stressing the importance of ICGA for the proper management of most inflammatory processes of the back of the eye. 45
ICGA impact on the management of the patient with posterior uveitis
(1) Precise assessment of choroidal inflammatory involvement (Fig. 1B). The choroid is the starting point of the inflammation in many diseases, including MEWDS, APMPPE, multifocal choroiditis, serpiginous choroiditis, VKH disease, sympathetic ophthalmia, and BRC, and is involved in the inflammatory process in many other diseases such as sarcoidosis, tuberculosis, syphilis, toxoplasmosis, posterior scleritis, and many more that have extensively been analyzed by ICGA. A reliable assessment of fundus inflammatory involvement can, therefore, only be performed with the help of ICGA. It will contribute essentially to the assessment of disease extension in those conditions involving the choroid.
(2) ICGA monitoring of disease evolution and response to therapy (Fig. 2). As choroidal lesions can only be detected by ICGA, it is obviously also the recommended test to monitor the evolution and to evaluate the impact of treatment on choroidal inflammatory processes. In case of VKH disease, clinical disease, meaning inflammation involving extrachoroidal structures that are accessible to fundus observation, to OCT and FA, can be followed by classical means. However, once clinical disease is under control, it has been shown that subclinical disease is ongoing, resulting in a great majority of cases in sunset-glow-fundus (SGF) and ICGA is truly the only way that this ongoing process of the choroid, which will result in further damage, can be recognized. 46 It was recently shown that ICGA-guided treatment of VKH disease could avoid evolution toward SGF when also treating subclinical disease shown by ICGA. 47 Therefore, except for conditions such as pars planitis or Behçet disease (BD) where choroiditis is absent or insignificant, dual FA and ICGA should be performed for the assessment of posterior uveitis if angiographic analysis is deemed necessary, as choroiditis cannot be excluded “a priori.”
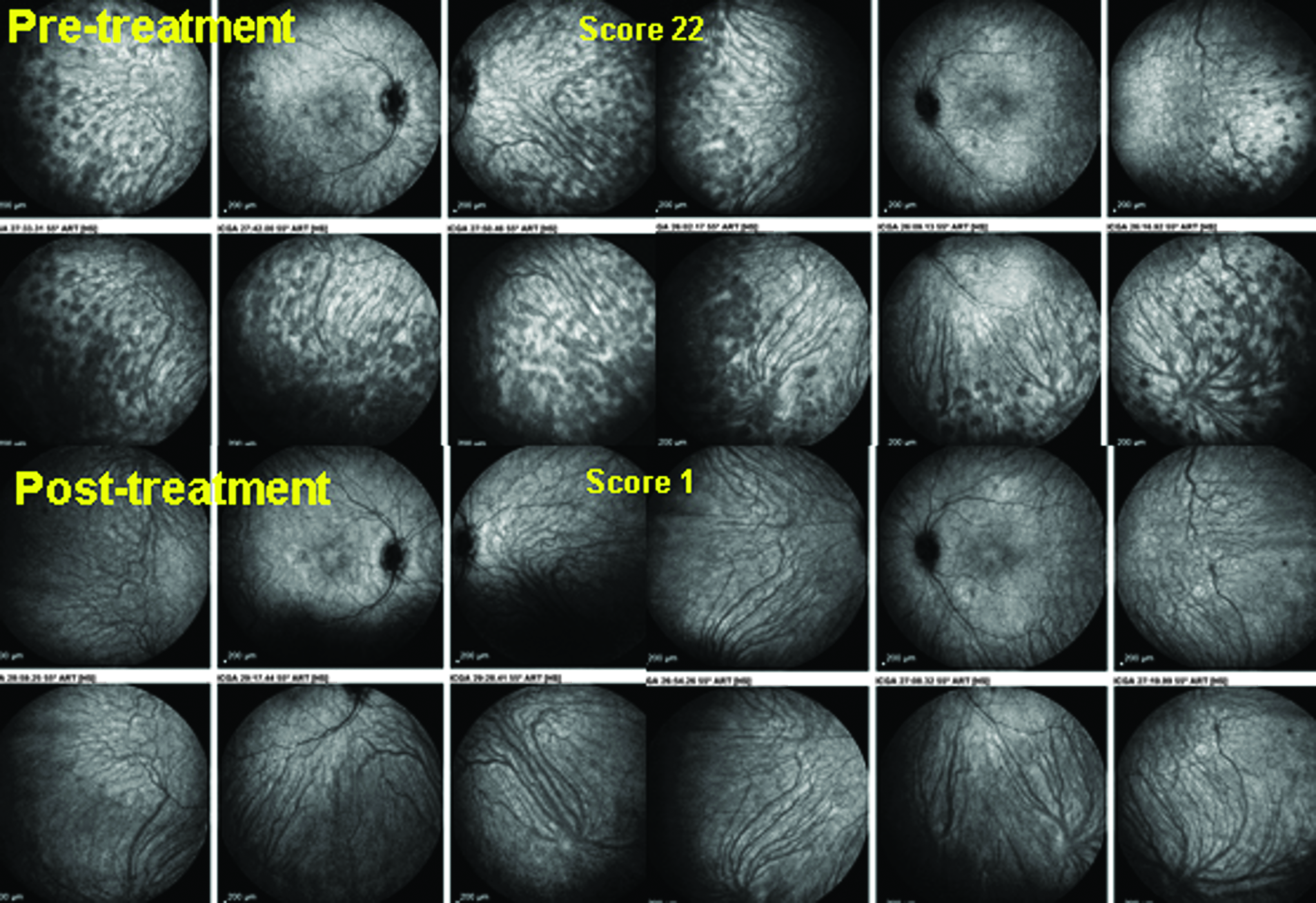
ICGA monitoring of choroiditis in a case of VKH. VKH patient with clinical resolution of inflammation after initial aggressive combined corticosteroid and cyclosporine treatment but complaining of persistent headaches. ICGA shows prominent occult choroiditis with numerous HDDs and fuzzy indistinct choroidal vessels (mean ICGA score = 22/40) in the right eye (“pre-treatment” top left and top middle quartet of pictures) and in the left eye (top right quartet of pictures). Five weeks after initiation of Remicade® therapy (infliximab, 5 mg/kg), there is complete resolution of occult choroiditis, with a decrease of mean ICGA score from 22 to 1 (“post-treatment,” bottom quartets of pictures), giving an idea of the high precision obtained by ICGA to monitor efficacy of therapeutic intervention. VKH, Vogt-Koyanagi-Harada.
ICGA is one modality contributing to the evolution of uveitis toward being an exact “clinical science,” as investigational procedures allow an increasingly precise appraisal of lesions in most ocular compartments. It provides essential information and a security to the clinician that no other method can furnish in the assessment and follow-up of choroiditis. It is more sensitive and reactive than EDI OCT measurement of choroidal thickness (which is not possible beyond the posterior pole) to monitor therapeutic intervention and is not matched by EDI OCT for short-term follow-up and adjustment of therapy. Therefore, management of posterior uveitis in cases where the choroid is involved cannot be meaningfully performed without ICGA.
In view of all these benefits, it is difficult to understand why such a quantitative parameter is not used as one of the outcome measures in clinical trials on new therapeutic agents in posterior uveitis.
The dual FA/ICGA scoring system allows quantitative, numbered assessment of the retinal and choroidal compartments
The use of dual FA/ICGA angiography allowed to differentiate the respective retinal and choroidal involvement in posterior uveitis. For instance, in a disease such as BRC, where both compartments are involved in the inflammatory reaction, both FA and ICGA angiographic scores are high (Fig. 3A). 48 In contrast, in VKH disease where an inflammatory reaction exclusively takes place in the choroidal stroma and where the choroid is principally involved with only spill-over inflammation taking place in the (outer) retina, FA score is much lower than the high ICGA score (Fig. 3B). The use of such a scoring system, as explained later, allows for a precise and quantitative assessment of posterior uveitis, but it has not been used so far in clinical trials, in spite of being much more relevant and objective than vitreous opacities used in most clinical trials as the main outcome measure.

A few years ago, a dual FA/ICGA scoring system was designed with excellent inter-observer agreement.22,23 Briefly, a total maximum score of 40 was assigned to the 8 FA signs: optic disc hyperfluorescence, macular edema, retinal vascular staining and/or leakage, capillary leakage, retinal capillary nonperfusion, optic disc neovascularization, neovascularization elsewhere, pinpoint leaks, and retinal staining and/or subretinal pooling. A total maximum score of 40 was also assigned to the 4 ICGA signs: early stromal vessel hyperfluorescence, choroidal vasculitis, dark dots or areas (excluding atrophy), and optic disc hyperfluorescence. As there were 8 scored FA signs and 4 scored ICGA signs, each ICGA score point was doubled so that the importance of involvement was proportionally scored and comparable in both compartments. This system has started to be used around the world, 49 and has also been shown to be a reliable method of scoring UWF FA, 50 but it still needs to be widely accepted by the uveitis community. It appears as much more adequate than vitreous haze for clinical trials for the evaluation of novel therapeutic agents, giving quantitative, numbered data on both retinal and choroidal inflammation.
Laser flare photometry
Intraocular inflammation causes disruption of the blood-ocular barriers and entry of proteins and inflammatory cells into the aqueous humor.
Limitations of slit-lamp grading of anterior chamber inflammation
Increased protein content of the aqueous humor is perceived as flare and graded subjectively at the slit lamp from 0 to 4+ based on the ability to visualize iris and lens details. A faint flare is graded as 1+; a moderate flare with clear iris and lens details is graded as 2+; a marked flare with haziness of iris and lens details is graded as 3+; and an intense flare with the presence of fibrin or plastic aqueous is graded as 4+. 4 In a study that investigated inter-observer variability in grading of intraocular inflammation, flare grades assigned by different uveitis specialists were skewed toward low grades, indicating failure of the clinical flare grading system to define different levels of inflammatory activity. 51 The use of this subjective grading system for flare introduces an unavoidable element of bias in clinical study cohorts where longitudinal follow-up of flare is an outcome measure and more importantly, in multicenter clinical trials where investigators with variable clinical experience participate.
Principle of LFP
LFP, developed and introduced by Sawa et al. in the 1980s,8–10 is the only objective method to measure flare in the aqueous humor.11,12 In principle, LFP is based on the measurement of scattered light in the anterior chamber by an incoming laser beam. Light scattered by small molecules (proteins) in the aqueous humor is detected by a photomultiplier and processed by a computer, giving flare values expressed in photon counts per millisecond (ph/ms), (Fig. 4). The intensity of the scattered light, that is, flare count, is proportional to the amount and size of proteins in the aqueous humor. This linear relationship between laser flare intensity and protein concentration has been shown in both in vitro and in vivo experiments.8,52,53 Since error codes are displayed by the LFP instrument when measurements are unreliable, such as in the case of corneal opacity, extensive posterior synechiae, or mature cataract causing an increased background scattering of light, and the average of 5–7 reliable measurements is used as the flare count, highly reproducible results are obtained.

Laser flare photometry. The Kowa FM-700 laser flare photometer is the latest instrument measuring flare, commercialized in 2013. It benefits from completely new engineering and is more user-friendly. Measurements are in concordance with the previous model, the FM-500. Therefore, both machines can be used in multi-center studies. Schematic explanation of measurement principle (top left, PMT = photometer). Observer's view through slit-lamp during measurement (bottom left); to the left of the image, reflection on the cornea (1); to the right, posterior reflection on the iris (2) and on the lens (3) Laser beam (4) measuring window (5) placed in the posterior and inferior third of the anterior chamber between anterior and posterior reflections. Picture of LFM-700 during measurement session (right picture).
Comparison between LFP and slit-lamp grading of anterior chamber flare
Flare counts by LFP correlate with clinical grades of flare at the slit lamp 12,54–56 However, there are large variations of flare counts within clinical grades and overlapping flare counts between grades, because of the subjective and nonlinear nature of the clinical grading of flare, whereas LFP yields a measure of flare ranging from 3 to 1,000 ph/ms on a linear scale. Furthermore, there is a high inter-observer variability of clinical grading of flare, especially by clinicians with different levels of experience; and flare grades of the more experienced clinician correlate better with the gold standard, LFP flare.55,56 Thus, LFP is the only objective, precise, and linear measure of anterior chamber flare and eliminates an important element of bias in clinical studies on new therapeutic agents in uveitis.
In uveitis practice, slit-lamp flare has not been regarded as an indication of active inflammation but has been traditionally considered a sign of chronic blood-ocular barrier breakdown. In a recent survey of registered uveitis trials, Denniston et al. 5 have found that anterior chamber flare was not an outcome measure in clinical trials that used a single primary outcome measure or even in those that used composite outcome measures, but it was included in only 2 of the 23 (9%) trials that used multiple primary outcome measures. This may be explained by the concept of flare being a sign of chronicity and also by the subjectivity of clinical grading of flare. On the other hand, VHS, a subjective parameter in current practice, was the leading activity outcome in clinical trials. 5 Thus, the concept of flare being a treatable activity measure needs to be first acknowledged by the uveitis community, because LFP studies have shown that clinically meaningful changes in flare counts could be achieved in both low- and high-flare situations.
It was shown that LFP flare was superior to slit-lamp cell evaluation for the follow-up of inflammation in acute uveitic entities such as HLA-B27-related uveitis. 21 It was also shown that LFP could detect active and treatable inflammation even in the absence of anterior chamber cells in JIA-associated chronic anterior uveitis, where a significant flare reduction after introduction of maximal therapy could be obtained. 57 In posterior uveitis, LFP proved useful for the follow-up of inflammation, as long as there was a minimum of associated anterior chamber spill-over flare of 15 ph/ms. 58 In BD uveitis, a panuveitic entity, LFP proved extremely useful as a global marker of disease activity, since LFP flare correlated well with both anterior and posterior signs of clinical activity.59,60 More importantly, LFP values correlate well with fluorescein angiographic leakage,59,60 and even minimally elevated flare values during clinically quiescent periods indicate persistent subclinical retinal vascular inflammation and a higher risk of exacerbation in patients with BD uveitis. 59 In VKH disease, another panuveitic entity, the finding of significantly higher flare values in patients with recurrent disease than in those with initial-onset VKH, has confirmed that recurrent VKH is a more severe and refractory disease and needs to be treated more aggressively than is suggested by clinical signs alone. 61
LFP and prognosis
The prognostic significance of LFP flare has been suggested in both adult and pediatric populations with uveitis.62–65 An inverse relationship between LFP flare and visual acuity and a strong relationship between flare and ocular complications, such as posterior synechiae and macular edema, have been found in a cohort of uveitis patients aged between 5 and 85 years. 62 In children with chronic uveitis, high LFP flare values (>20 ph/ms) were associated with complications at baseline and poor visual acuity and predicted development of new complications and visual loss.63–65 Most importantly, clinical assessment of anterior chamber cells or flare did not show such strong associations with ocular complications or poor vision.62–64 Thus, in both acute and chronic uveitic entities, management should be guided by LFP, and treatment should be maintained or even increased as long as a decrease of flare is obtained. In chronic uveitis, there may be a threshold corresponding to permanent blood-aqueous barrier disruption that can be reached only after intensive therapy is employed.
In summary, accumulated clinical experience and studies using LFP show that LFP should become the standard to quantify intraocular inflammation in uveitis patient care and research. As the only objective, quantitative, precise, and reproducible measure of intraocular inflammation, inclusion of LFP flare as an outcome measure in uveitis research will improve the standardization and yield of clinical trials.
Optical coherence tomography
OCT is an imaging modality that is routinely used for the diagnosis and management of retinal diseases. OCT can be considered a major development in ophthalmology and represents a quantitative modality in the appraisal of posterior uveitis, as it allows non-invasive in vivo quasi histological analysis of the retina. 13 Since its introduction in ophthalmology in the early 1990s, 13 OCT was prevalently used to study the retinal morphology, particularly the abnormalities of the vitreoretinal interface and the presence of fluid in retinal tissues.14–18 First-generation OCT machines used time domain technology that is characterized by low-coherence, near-infrared light from a superluminescent diode light source split to go to a reference mirror and to the retina. Later, OCT technology has been implemented by introducing frequency-domain OCT, which is also known as spectral-domain (SD) OCT. The advantages provided by SD OCT are a superior resolution and faster signal acquisition. SD OCT is capable of providing qualitative and quantitative information and, therefore, has become an indispensable imaging modality in the diagnosis and management of inflammatory diseases involving the posterior segment of the eye.
Indeed, OCT is a fast, reliable, and precise method for the detection and monitoring of uveitic macular edema. 66 SD OCT can accurately define the three macular morphologic features of uveitic macular edema, including cystoid macular edema, diffuse macular edema, and subretinal fluid. Other quantitative information that is gathered by imaging the posterior pole of the retina in uveitis includes changes in the inner and outer retinal architecture and vitreoretinal interface and has been extensively described in the literature. 18 Among these abnormalities, those involving the outer retina and particularly disruption of photoreceptor inner segment/outer segment junction line have been shown to be associated with poor visual outcomes in uveitis. Other qualitative information associated with poor visual outcome in eyes with uveitis includes cystoid changes in the outer plexiform and inner nuclear layer and the presence of epiretinal membrane. 18 Thus, qualitative information provided by OCT can serve to determine the prognosis and potential for visual recovery in patients with posterior uveitis entities.
Current software in commercially available OCT machines is capable of providing reproducible automatically calculated measurements of foveal thickness and volume. All instruments identify the vitreoretinal interface as the inner retinal border. The segmentation of the outer retinal border differs among the instruments significantly. Therefore, there may be variability for foveal measurements between different OCT systems. Both thickening and thinning in the fovea have important implications clinically and are important parameters for prognosis and potential of visual recovery in eyes with posterior uveitis. 18 By the use of foveal thickness measurement and/or volume maps, it is possible to reliably detect and measure small changes in uveitic macular edema and to quantitatively evaluate the efficacy of different therapeutic modalities. This fact and its non-invasive nature makes OCT superior to other imaging modalities in the detection and following the response to therapy for macular edema in patients with uveitis, although FA is still more sensitive in detecting subtle inflammatory macular edema (leakage). As there may be discrepancies between macular thickening (OCT) and macular leakage (FA) because of the potential role of the RPE and Muller cells to absorb fluid leakage, it is mandatory to perform both exams as complimentary imaging methods for reliable management of patients with uveitis.
Besides macular thickening, the importance of foveal thinning has been stressed by Forooghian et al. 67 The authors have characterized foveal atrophy in a heterogeneous group of uveitis patients using SD OCT and defined foveal atrophy as a center point foveal thickness of less than 150 μm. Foveal atrophy can be quantitatively identified by OCT and is a potentially severe sequela of uveitis that can lead to permanent visual impairment. The cause of foveal atrophy is multifactorial and includes dysfunction and atrophy of RPE and choroid, macular edema, macular ischemia secondary to occlusive retinal vasculitis, choroidal neovascularization, retinal detachment, and selective antibody-mediated damage directed against photoreceptors.
En face OCT, which produces C-scan (coronal) images of retinal and choroidal layers at any specified depth, allows evaluation of the location and extent of inflammatory changes in posterior uveitis. 68 In a recent study using en face OCT, Cohen et al. 69 have shown that the proportion of preserved retinal tissue on baseline C-scan images placed between the ganglion cell layer and the outer plexiform layer correlated with visual outcome in eyes with uveitic macular edema and was a better predictor of visual prognosis than macular thickness or volume measurements. However, cross-sectional B-scan images are principal images that guide diagnosis, prognosis, and response to therapy in routine practice.
Very recently, vitreous inflammation has become a study item by OCT. Keane et al.70,71 reported measurement of vitreous signal intensity from SD OCT image sets in patients with uveitis. The authors proposed OCT-based indices as an objective marker to quantify vitreous inflammatory activity for use in routine clinical assessment and as an outcome measure in clinical trials for intermediate, posterior, and panuveitis. There is still a long way to go to make this method accessible by incorporation of automated vitreous measurements in commercial OCT software and to make it easy to use in therapeutic trials (see later).
In summary, OCT enables a non-invasive, safe, accurate, reproducible, and quantifiable analysis of the retinal tissue, allowing precise monitoring of uveitis activity in the posterior pole of retina in everyday practice and clinical trials. Recently, OCT has also become available for precise evaluation of choroidal thickness using EDI OCT.
Enhanced-depth imaging OCT
In recent years, there has been substantial interest in the use of EDI OCT, available since 2008, to replace ICGA to monitor choroiditis. 19 EDI OCT, integrated into most commercially available OCT systems, is a non-invasive tool that can investigate the choroidal space with the capability of imaging deeper choroidal structures qualitatively and it enables quantitative measurements of choroidal thickness. 72 The advantages of the technique include non-invasiveness and ease of use. However, current technology does not allow for automated measurements of the choroidal thickness. There is need for manual measurement using digital calipers provided by OCT software. There is also need to include more than one experienced observer to measure the choroidal thickness to assess for reproducibility of choroidal thickness measurements in clinical trials. Such measurements, however, are tedious and time consuming. It is also difficult to identify the choroidoscleral junction in diseased and healthy eyes with a thick choroid.
The disadvantage of EDI OCT, or other choroidal OCT devices that image deep choroidal structures, is their inability to examine global panfundal choroidal inflammation, especially considering that stromal choroiditis entities (VKH disease or BRC) are disease processes that involve the entire fundus. 73 In addition, unlike ICGA, EDI OCT is much less sensitive and reactive to detect short-term changes in level of choroiditis and cannot detect subtle, visit-by-visit variations. It is, therefore, unsuited for close monitoring and to adjust therapy for which ICGA has become the gold standard.24,48 Several studies have, however, established that EDI OCT measurements of choroidal thickness decrease over time in stromal choroiditis such as VKH disease or BRC in response to treatment (Fig. 5).74,75 In that regard, it is an additional modality, suited for long-term follow-up of stromal choroiditis and contributing to a better appraisal of choroidal inflammation. Despite its inherent insufficiencies, it still represents a quantitative outcome parameter that could be used to follow choroiditis in clinical studies on new therapeutic agents. 76
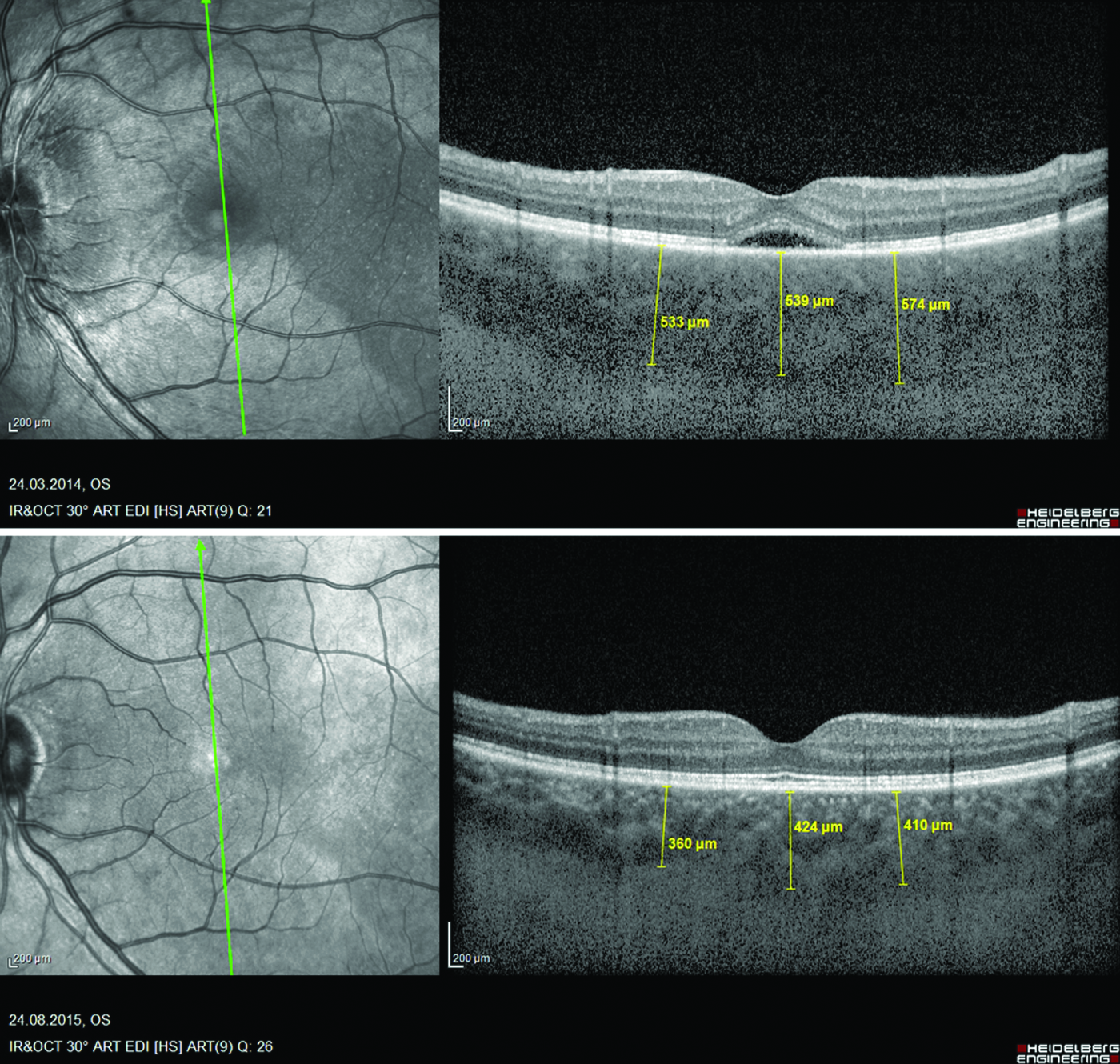
Evolution of choroidal thickness in a patient with VKH disease, measured by EDI-OCT. At the initial stage of disease, the choroid is substantially thickened (top picture, mean thickness, vertical axis = 548 μm). After 5 months of treatment, choroidal thickness decreased to 398 μm, vertical axis (bottom picture). EDI, enhanced-depth imaging; OCT, optical coherence tomography.
Assessment of vitritis
Assessment vitreous inflammatory infiltration is an important outcome parameter. It is useful as long as it is not used alone and is part of a global inflammation scoring system. Nussenblatt et al. 3 published clinical photographs illustrating 6 grades of vitreous haze in 1985. It has been widely used and formed the basis for SUN Working Group scale for vitreous haze grading. 4 Later in 2010, Davis et al. 77 proposed a 9-step photographic scale for grading vitreous haze in uveitis by use of digitized photographs. To create optical blur that would simulate vitreous haze, photographs were obtained from a normal fundus through Bangerter occlusion filters, digitized, and graded on an ordinal scale from 0 (no haze) to 8 (highest level of opacification). This photographic scale was validated a year later. 78 In a subsequent study, reproducibility of the 9-step scale versus the 6-step scale was compared; both scales were found to be reliable for clinical research as long as a 3-step change for the former and a 2-step change for the latter scale were used. 79 The 9-step scale was more reliable with photographic grading than clinical grading, suggesting that the use of a Reading Center approach would be more preferable for clinical trials. 79
Recently, there has been an attempt to develop a more objective and quantitative method to assess vitreous haze using OCT, which will hopefully be sufficiently user-friendly to be able to replace the subjective method presently used.70,71 Keane et al. 70 reported the measurement of vitreous signal intensity from SD OCT image sets in patients with uveitis. The authors proposed precise quantification of vitreous involvement in patients with active uveitis. The data supported the evidence that SD OCT may provide reliable measurements of vitreous signal intensity, which may represent a promising outcome measure for the correct quantification of vitreous haze. On the other hand, the authors stressed the need to validate such techniques, to obtain a repeatable method for an objective, quantitative disease activity endpoint. Furthermore, the authors speculated that the incorporation of automated vitreous analysis in commercial OCT systems may provide a user-friendly technology that might improve the follow-up methods. Very recently, the same group published a second report in a larger cohort of uveitis eyes, including pseudophakic and vitrectomized eyes. 71 The authors retrospectively reviewed SD OCT images by using custom software. Vitreous (VIT) and RPE signal intensities were compared to create a relative optical density ratio with arbitrary units. These data were then compared with clinical VHS. The authors concluded that VIT/RPE-relative intensity values confirmed the results obtained in the previous study. Moreover, phakic status and previous vitrectomy surgery did not seem to affect the values, although they acknowledged that such preliminary findings have to be interpreted under the light of the retrospective nature and the limited cohort analyzed. Again, they stressed the need to validate such preliminary data with prospective studies, which may take considerable time and will not be available in the very near future.
Other
FAF. FAF is useful in choriocapillaritis entities; helps to follow lesions in MEWDS, APMPPE, serpiginous choroiditis, and idiopathic multifocal choroiditis; and may be useful to follow the evolution in the interval between two ICGAs, the latter remaining necessary to trace lesions in such cases, and FAF not being sufficiently reliable nor quantitative. This mainly qualitative modality will probably not be developing into a quantitative parameter to be used in trials on new therapeutic agents. Moreover, its utility is limited to a small number of pathologies such as inflammatory choriocapillaritis entities.20,80,81
OCT angiography
OCT-A is a non-invasive imaging technique detecting blood flow in superficial and deep retinal vessels as well as in the choriocapillaris but at the present stage of technology, it is probably not reliable enough to detect or quantify changes in the deeper choroidal vessels. We followed a case of serpiginous in parallel with ICGA and OCT-A. Non-perfused areas of the choriocapillaris were apparent with both techniques, with ICGA being, however, more precise in delineating the lesions. Although OCT-A is superior to FA in showing superficial and deep retinal capillary details in the retina, it cannot show vascular leakage, which is a major limitation for uveitis practice. Moreover, information given by OCT-A is limited to the posterior pole, in contrast to ICGA giving global panfundal information,82–84 and will probably not develop into a quantitative parameter to be used in trials on new therapeutic agents.
Which study design and which clinical trial endpoints for studies on posterior segment uveitis?
Inadequacies in study designs
So far, clinical trials for posterior segment uveitis mostly included different types of non-infectious uveitis entities and in most trials, the main outcome measure was vitreous haze, meaning that many trials were dependent on this one subjective criterion. Vitreous haze, although subjective and semi-quantitative at best, may be used for entities such as intermediate uveitis, where vitreous haze is the preponderant clinical sign. Even in such circumstances, it appears as hazardous to have a clinical trial relying on such a sole subjective clinical sign. Since intermediate uveitis is associated with retinal vasculitis, it would benefit from a more objective and better quantifiable outcome measure such as FA for monitoring of retinal vasculitis. This indicates that classically used vitreous haze is questionable, even if trials were including only intermediate uveitis cases. As previously mentioned, trials, however, mostly included a potpourri of posterior segment uveitis entities. In many posterior uveitis entities, vitreous haze is an utterly inadequate parameter, just because this sign is absent or modest or when present, minimally relevant. In VKH disease, vitreous haze is rarely present or moderate in most cases, the principal clinical or investigational sign being choroiditis adequately and quantitatively analyzed only by ICGA or EDI OCT measurement of choroidal thickness. In case of Behçet uveitis, many cases do not present sufficient vitreous haze and are, therefore, hard to include. In a study of Behçet uveitis that enrolled all consecutive patients who presented with an acute exacerbation, only 35% had 2+ or higher VHSs 59 ; whereas in another study that enrolled only patients refractory to conventional immunosuppressive treatment, only 77% had 2+ or higher VHSs at entry. 85 Variable severity of uveitis attacks, not always causing significant vitreous haze, makes it hard to use vitreous haze as a single primary outcome measure in Behçet uveitis. It is even harder in such cases to obtain a two-step improvement on a scale that contains only four. In a recent series where results of biologic therapy were reported, the median VHS was 1+ at baseline and reduced to 0 at 1 year of treatment. 86 BRC presents with vitritis, a sign that is, however, slowly reactive to therapy and much less relevant for disease evolution in comparison to retinal vasculitis investigated by FA and to choroiditis investigated with ICGA and EDI OCT, all methods giving quantitative and numerical data. These are a few examples showing that the primary outcome measure, vitreous haze, used in a majority of trials, is utterly inadequate. It is, therefore, astonishing that such trials could have a positive result. On the other hand, it should be asked how many studies failed because of the inadequate study design and how many potentially useful therapeutic agents were lost for the sake of our uveitis patients.
Conducting single-entity trials
The ideal way to conduct uveitis trials would be to perform studies on specific entities. This would allow to have homogeneous collectives and would increase the probability to have clear-cut results on the efficacy of a given treatment. It is also easier to determine meaningful outcome measures corresponding and tailored to the pathological process involved. For instance, if a trial would involve patients with VKH disease, main outcome measures should focus on choroiditis, as this is the main structure involved in which inflammation starts and tends to persist in case of insufficiently efficacious treatment. Main outcome measures should absolutely include ICGA score and choroidal thickness measured with EDI OCT.
In case of Behçet uveitis, various outcome measures have been used because of the relapsing and remitting natural course and variable involvement of the anterior and/or posterior segment of the eye during exacerbations. Visual acuity has been consistently used as a primary outcome, although exacerbations can occur without affecting vision, but still indicating uncontrolled disease activity, based on the emergence of new retinal infiltrates and/or occlusive or non-occlusive retinal periphlebitis that may involve only the peripheral fundus. Therefore, frequency of exacerbations, especially those involving the posterior segment, or clinical remission (absence of exacerbations) has been used as a primary outcome measure in several trials.87–91 On the other hand, severity of inflammatory episodes and evolution of posterior inflammatory signs after treatment determine the visual prognosis. A composite severity score, Behçet's disease ocular activity score (BOS24), has been recently developed, where anterior chamber cells, vitreous haze, peripheral, posterior pole, foveal, and optic disc lesions were scored individually, and the sum of these 6 inflammatory parameters yielded a total maximum score of 24. 92 Anterior chamber flare or fluorescein angiographic signs of activity were not included in this system. In fact, only few studies have included fluorescein angiographic leakage as one of the main outcome measures. 93 Since both leaky and occlusive retinal vasculitis and retinal capillaritis exist with variable severity during active and clinically quiescent periods, fluorescein angiographic scoring or at least anterior chamber flare measured by LFP, as a surrogate marker of fluorescein leakage, should be included in outcome measures in clinical trials of Behçet uveitis.
Unfortunately, such single-entity trials are difficult to perform, as some of the uveitis entities such as BRC are too scarce to enable a trial because too many centers would have to be involved and the duration of such a trial would be too long: This is the reason why most uveitis trials involve multiple uveitis entities.
Multiple uveitis-entity trials
Most trials on posterior segment uveitis are multiple entity trials putting together diseases with diverse mechanisms and expressions rendering such studies difficult to conduct. Because uveitis is rare, very often, trial promoters were forced to proceed in such a way. What made things critical was the choice of inadequate outcomes.
If the choice is made to conduct studies including diverse intermediate, posterior, and panuveitis entities, at least correct outcome choices should be chosen. Ideally, because multiple mechanisms are involved, a composite inflammation score should be generated based on quantitative parameters, taking into account the general level of inflammation measured by LFP, the amount of choroiditis evaluated by ICGA and EDI OCT, retinal involvement evaluated by FA, and vitreous haze. For each entity, the preponderant clinical or investigational sign involved should be given a multiplying coefficient allowing to privilege the preponderant sign(s) on which the therapy is going to have an impact or not. For instance, for a VKH disease patient, the ICGA score should be given a coefficient, as this is the preponderant structure involved that will respond (or not) to a novel therapy. In case of BRC, a multiplying factor should be given to choroiditis (ICGA score or/and choroidal thickness) and to retinitis (FA score). In case of Behçet uveitis, FA score, LFP flare, and central macular thickness on OCT should be given a multiplying coefficient.
Our group is presently working on the design of a composite inflammation score that is easily usable in centers equipped with the essential instruments, including, LFP, FA, ICGA, OCT, and EDI OCT.
Conclusion
In view of the significant development of objective and quantitative modalities for the precise appraisal of inflammatory parameters in posterior segment uveitis, including LFP accounting for global inflammation, FA giving a quantifiable measurement of retinal inflammation and ICGA precisely accounting for choroidal inflammation, OCT precisely measuring retinal thickness, and EDI OCT measuring choroidal thickness, we have now the means of designing studies that do not rely any more on subjective and inadequate outcome parameters to design studies assessing new therapeutic agents for posterior segment uveitis. A weighted use of these methods to compensate for the primary site of inflammation of the different entities may provide a very good way to overcome the problems that we all encounter when recruiting patients into specific entity studies (small numbers), and still analyze the impact of the effect of therapy for each of the different entities included.
Footnotes
Author Disclosure Statement
No competing financial interests exist.