
Abstract
Abstract
Purpose:
This study compared the effects of 3 antivascular endothelial growth factor (VEGF) agents (bevacizumab, ranibizumab, and aflibercept) on corneal epithelial cell viability and wound healing using human corneal epithelial cells (HCECs).
Methods:
To determine the cytotoxic effects of anti-VEGF agents on HCECs, HCEC viability was determined at various concentrations of these agents. An in vitro migration assay was used to investigate the migration of HCECs treated with 3 anti-VEGF agents. The protein level of extracellular signal-regulated kinase was used to evaluate the effect of anti-VEGF treatment on cell proliferation. The protein levels of p38 mitogen-activated protein kinase (MAPK) were analyzed by Western blotting to investigate cell migration.
Results:
After 24 or 48 h of exposure, aflibercept treatment showed no apparent effect on cell viability; however, bevacizumab and ranibizumab treatment decreased cell viability at high concentrations (1 and 2 mg/mL). A migration assay showed that HCEC migration was different among the 3 anti-VEGF treatment groups. Bevacizumab significantly delayed HCEC migration. Western blotting showed that bevacizumab treatment decreased the expression levels of phosphorylated p38 MAPK.
Conclusions:
Bevacizumab, the most widely used and investigated anti-VEGF agent, decreased epithelial cell migration and viability. Anti-VEGF agents other than bevacizumab might therefore be better for treating corneal neovascularization complicated with epithelial defects.
Introduction
C
Ranibizumab is a recombinant, humanized monoclonal antibody (Fab) that neutralizes all biologically active isoforms of VEGF-A. 7 Several clinical investigations have shown the efficacy of ranibizumab in the treatment of corneal neovascularization.8–10 Aflibercept is a newly developed anti-VEGF agent that combines a truncated form of fms-like tyrosine kinase (Flt), kinase insert domain-containing receptor (KDR), and the Fc portion of human immunoglobulin G. 11 Studies have reported potent antiangiogenic effects of aflibercept after topical or subconjunctival administration.12–14
The objective of this study was to compare the effects of 3 anti-VEGF agents (bevacizumab, ranibizumab, and aflibercept) on corneal epithelial cell viability and wound healing using human corneal epithelial cells (HCECs).
Methods
Reagents
Bevacizumab (Avastin®), ranibizumab (Lucentis®), and aflibercept (EYLEA®) were obtained from Roche Diagnostics (Basel, Switzerland), Novartis (Basel, Switzerland), and Bayer Regeneron Pharmaceuticals (Tarrytown, NY), respectively.
Cell culture
HCECs, an SV40-immortalized HCEC line, were purchased from the American Type Culture Collection (Rockville, MD) and cultured in Dulbecco's modified Eagle's medium/Nutrient Mixture F-12 (Gibco-Life Technologies, Carlsbad, CA), supplemented with 5% fetal bovine serum (Gibco-Life Technologies), 5 μg/mL insulin (Sigma-Aldrich, St. Louis, MO), penicillin/streptomycin (1:100), 500 ng/mL hydrocortisone (Sigma-Aldrich), 30 ng/mL cholera toxin (Sigma-Aldrich), and 10 ng/mL human epithelial growth factor (Sigma-Aldrich) in a 37°C incubator with a humidified atmosphere containing 5% CO2. The composition of the medium was derived from previous studies in which the virus-free immortalization and characterization of HCECs were successfully accomplished. 15 Cells were subcultured to 80% confluency by being trypsinized in 0.25% trypsin. This study was conducted in compliance with the regulations of the Institutional Review Board of Daejeon St. Mary's Hospital.
Cell viability assay
To determine the cytotoxic effects of the anti-VEGF agents, the viability of HCECs was determined using an Ez-Cytox Cell Viability Assay Kit (DoGen, Seoul, Republic of Korea). HCECs were seeded in 96-well plates at 1 × 104 cells/well and incubated under standard conditions for 24 h. The cells were then treated with various concentrations of bevacizumab (0.25, 0.5, 1.0, or 2.0 mg/mL), ranibizumab (0.25, 0.5, 1.0, or 2.0 mg/mL), or aflibercept (0.25, 0.5, 1.0, or 2.0 mg/mL) for 24 or 48 h. After 24 or 48 h of incubation, 10 μL of the kit reagent was added and the cells were incubated for an additional 2 h. The absorbance was recorded at 450 nm using a microplate reader (Bio-Rad, Hercules, CA).
In vitro scratch wound healing assay
HCECs were counted and plated into 6-well plates. After growth to 90% confluency, the surface of the plate was scraped with a 200-μL pipette tip to generate a cell-free zone. Free cells were then removed with 2 washes of phosphate-buffered saline, and the cells were incubated in medium containing 0.5 mg/mL of the 3 different anti-VEGF agents. After incubation for 24 h, 3 fields of each wound were selected and photographed with an inverted light microscope (Eclipse TE300; Nikon, Tokyo, Japan) equipped with a digital camera. The area of wound closure was quantitatively determined using ImageJ software (National Institutes of Health, Bethesda, MD). The percentage of wound closure was calculated as 100% minus the percentage of the denuded area/the initial scraped area.
Western blot analyses
A standard Western blotting method was used. Briefly, HCECs were serum-starved overnight and stimulated with different anti-VEGF agents (0.5 mg/mL). After 60 min, the cells were harvested and lysed in RIPA buffer (Elpis Biotech, Daejeon, Republic of Korea) containing protease inhibitor cocktail tablets (Roche Diagnostics, Mannheim, Germany). Cell lysates were centrifuged at 13,000 rpm for 15 min at 4°C, and the supernatants were collected. After measuring the protein concentration (BCA Protein Assay Kit; Pierce, Rockford, IL), equal amounts of protein were separated by electrophoresis on a 10% sodium dodecyl sulfate–polyacrylamide gel and transferred electrophoretically to a nitrocellulose membrane (Bio-Rad). The membrane was then blocked with 5% nonfat milk in Tris-buffered saline containing 0.05% Tween-20 (TBST buffer) for 1 h and incubated overnight at 4°C with a rabbit polyclonal antibody against major subfamilies of mitogen-activated protein kinases (MAPKs) as follows: anti-extracellular signal-regulated protein kinase 1/2 (ERK1/2) (p-ERK, 1:1,000; Cell Signaling, Danvers, MA), anti-phospho-p44/p42 ERK (p-ERK, 1:1,000; Cell Signaling), anti-total p38 (p38, 1:1,000; Cell Signaling), and anti-phospho-p38 (p-p38, 1:1,000; Cell Signaling). β-Actin was used as an internal control. The intensities of the signals were recorded and quantified using a molecular imaging system (Molecular Imager ChemiDoc XRS+; Bio-Rad).
Statistical analyses
Unless indicated otherwise, all data are expressed as the mean ± standard deviation. Cell viability, wound healing, and Western blot densitometric results were analyzed by a Kruskal–Wallis Test. A value of P < 0.05 was considered statistically significant. SPSS statistical software for Windows, version 17.0 (SPSS, Inc., Chicago, IL) was used for the statistical analyses.
Results
The effect of anti-VEGF agents on cell viability
Cell viability following the treatment of HCECs with different concentrations of aflibercept, bevacizumab, or ranibizumab was examined. After 24 (Fig. 1A) or 48 h (Fig. 1B) of exposure, aflibercept treatment showed no effect on cell viability; however, bevacizumab and ranibizumab decreased cell viability at high concentrations (1 and 2 mg/mL; Fig. 1A, B). To exclude a high concentration-related effect on cell viability, additional experiments were performed at 0.5 mg/mL to ensure that there were no adverse effects on cell viability.
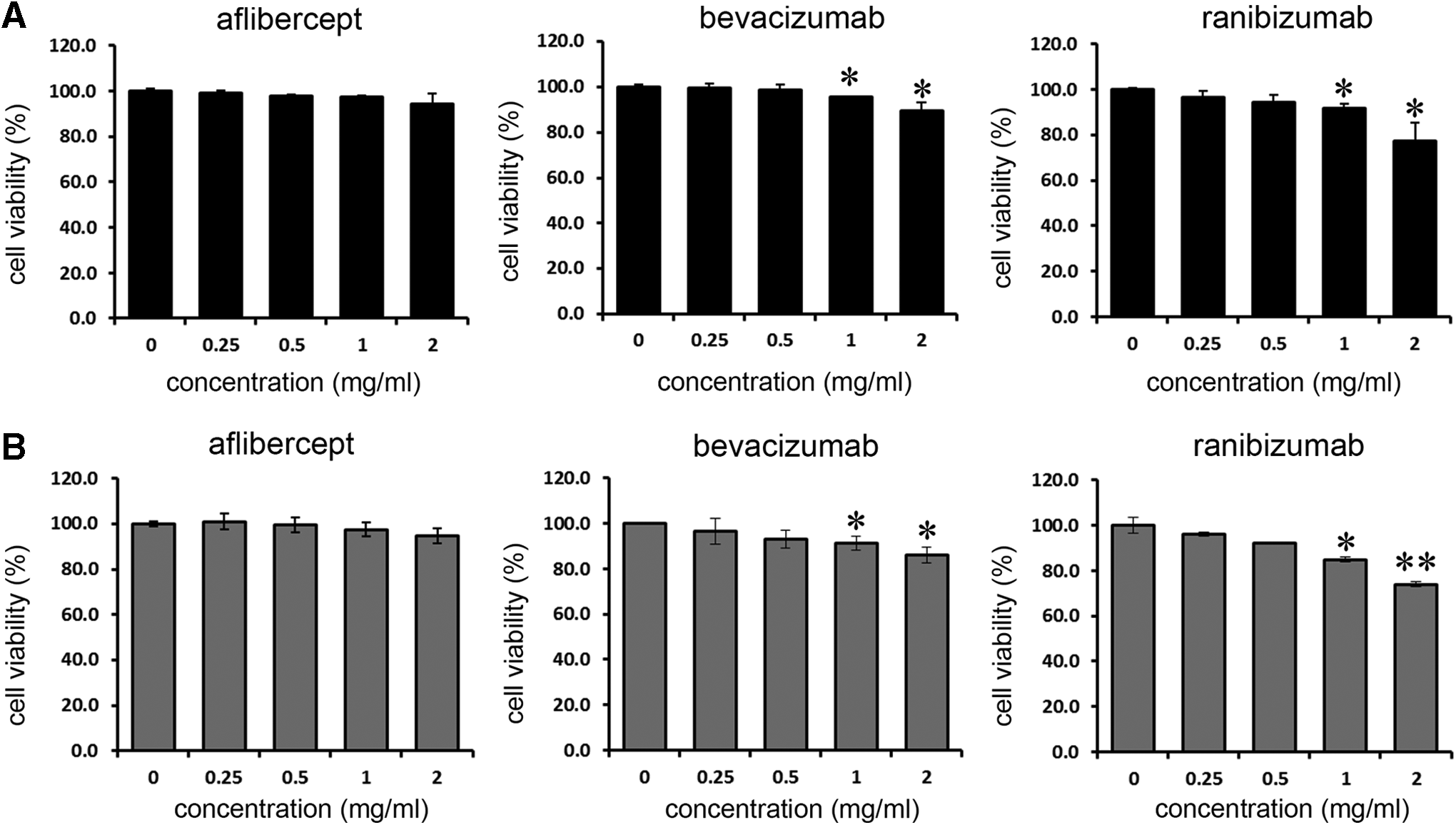
Cell viability assays after treatment with various concentrations of aflibercept, bevacizumab, or ranibizumab for
The effect of anti-VEGF agents on an in vitro scratch assay
Wound healing using an in vitro scratch assay was used to determine the effect of anti-VEGF agents on epithelial wound closure. The results showed different effects of the anti-VEGF agents on HCEC migration (Fig. 2A). Bevacizumab delayed HCEC migration significantly. Treatment with ranibizumab or aflibercept produced comparable effects on migration to the control treatment. F-actin staining with phalloidin (green) shows the morphology of the migrating HCECs (Fig. 2B).

The basal wound healing percentage of the HCECs in the control was 41.2% at 24 h. At 24 h after wounding, the corneal epithelial wound healing percentages in the aflibercept-, bevacizumab-, and ranibizumab-treated cells were 36.9%, 15.4%, and 40.2%, respectively (Fig. 2C). Statistical significance was noted in the bevacizumab-treated HCECs at 24 h postwounding (P < 0.05), showing that bevacizumab significantly decreased the migration rate of HCECs and delayed the epithelial wound closure time.
The effect of anti-VEGF agents on p-ERK activation
To investigate the effect of anti-VEGF agents on cell proliferation, p-ERK expression was determined by Western blot analyses (Fig. 3). p-ERK/ERK expression decreased after anti-VEGF treatment compared to the control. No differences were found among the 3 anti-VEGF agents. The expression levels of phosphorylated p38 MAPK relative to those of total p38 MAPK in the aflibercept-, bevacizumab-, and ranibizumab-treated HCECs were 0.82, 0.86, and 0.82, respectively.

HCECs were treated with anti-VEGF agents (0.5 mg/mL) for 1 h. The expression of total and phosphorylated forms of extracellular signal-regulated protein kinase (ERK) was determined by Western blot analyses. Representative Western blots of phosphorylated and total protein, and densitometric analyses of the ratio of phosphorylated/total protein are shown. Bars represent the mean ± standard error of values obtained from 3 independent experiments. *P < 0.05 versus the control (untreated cells).
The effect of anti-VEGF agents on p38 MAPK activation
P38 MAPK plays crucial roles in cell migration, especially in its directionality. We therefore investigated the effects of anti-VEGF agents on the activation of p38 MAPK phosphorylation in HCECs. Western blot analyses showed that the expression levels of phosphorylated p38 MAPK decreased after bevacizumab treatment. The expression levels of phosphorylated p38 MAPK relative to those of total p38 MAPK in the aflibercept-, bevacizumab-, and ranibizumab-treated HCECs were 1.08, 0.62, and 0.95, respectively, showing that a significant difference was found in bevacizumab-treated cells (P < 0.05; Fig. 4).
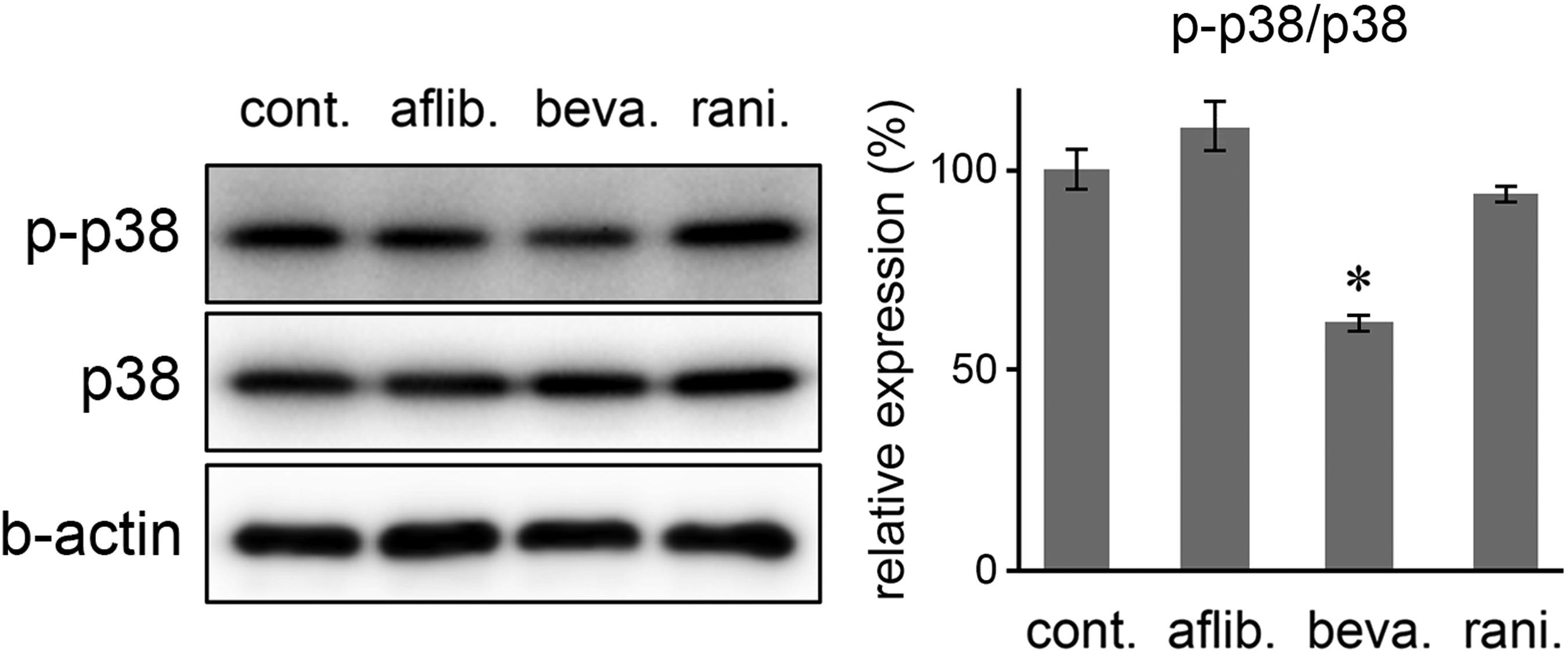
HCECs were treated with anti-VEGF agents (0.5 mg/mL) for 24 h. The expression of total and phosphorylated forms of the p38 MAPK subfamily was determined by Western blot analyses. Representative Western blots of phosphorylated and total protein, and densitometric analyses of the ratios of phosphorylated/total protein are shown. Bars represent the mean ± standard error of values obtained from 3 independent experiments. *P < 0.05 versus the control (untreated cells).
Discussion
Antiangiogenic therapy using anti-VEGF agents is an important treatment for corneal neovascularization and for the treatment of neovascular macular degeneration. One important consideration in using anti-VEGF agents such as bevacizumab to treat the cornea is its adverse effect on epithelial wound healing. Several studies have reported that this agent delays corneal epithelial wound healing.4–6 The mechanism was attributed to decreases in growth factors required for wound healing. However, previous studies used only bevacizumab, and other new agents for possible inhibition of wound healing in HCECs were not tested. This study was therefore designed to compare the differential effects of bevacizumab, ranibizumab, and aflibercept on cell viability, wound healing, and proliferation. It was an unlabeled use of anti-VEGF agents on HCECs.
In a previous comparative study of the toxicity of bevacizumab and ranibizumab on corneal fibroblasts, bevacizumab induced cellular toxicity, but ranibizumab did not cause cellular damage. 16 Lactate dehydrogenase (LDH) activity increased at 1.0, 1.5, and 2.0 mg/mL of bevacizumab treatment, but LDH activity after ranibizumab treatment did not increase at concentrations up to 2.0 mg/mL. In the present study, aflibercept had no adverse effects on cell viability at 1.0 and 2.0 mg/mL, at which concentrations bevacizumab and ranibizumab treatment resulted in decreased cell viability. We speculate that each anti-VEGF agent has differential effects that cannot be explained solely by their anti-VEGF activities.
The clinical dose calculated for the 4 mL of vitreous is 0.125, 0.313, and 0.5 mg/mL for ranibizumab, bevacizumab, and aflibercept, respectively. 17 Malik et al. used 1/2 ×, 1 ×, 2 ×, and 10 × clinical concentrations of anti-VEGF agents for the in vitro experiment using human retinal pigment epithelium cells (adult retinal pigment epithelial [ARPE]-19). 17 Another study treated ARPE-19 cells with clinically relevant concentrations of bevacizumab (0.125, 0.25, or 0.5 mg/mL), ranibizumab (0.125, 0.25, or 0.5 mg/mL), or aflibercept (0.125, 0.5, or 2.0 mg/mL). 18 We used 0, 0.25, 0.5, 1.0, and 2.0 mg/mL concentrations, which include the clinical dose for the vitreous. However, we tested HCECs which are different from the previous cells tested (ARPE-19). Again the cornea has tear layer on its surface and it has a relatively open environment compared to the vitreous. Therefore, considering the different cells, environment, and several variables, we tested various concentrations of anti-VEGF agents (0–2.0 mg/mL) for its cellular toxicity and chose 0.5 mg/mL to minimize cell toxicity-related effects on corneal wound healing. Our results show that bevacizumab treatment of HCECs decreased wound healing. Based on our p38 MAPK Western blot results, the decrease resulted from decreased cell migration. Saika et al. 19 reported that p38 MAPK has a major role in the acceleration of cell migration and in the suppression of cell proliferation in migrating mouse corneal epithelial cells. Aflibercept and ranibizumab treatment showed comparable migration results to the control, and we found no difference in the p-ERK Western blot results.
Early corneal wound healing is required to maintain corneal transparency and to provide a barrier to the external environment. Bevacizumab has been used to investigate the effect of anti-VEGF agents on corneal epithelial wound healing.4–6 Kim et al. 5 reported that the application of bevacizumab eye drops inhibited both VEGF and nerve growth factor, and it decreased the rate of wound healing. In addition, corneal stromal responses, assessed by MMP-2, MMP-9, and TGF-β levels, were overexpressed after treatment with bevacizumab eye drops. 6 Bevacizumab treatment also inhibited integrin expression in rabbit corneas. 4 However, Lee et al. 20 reported that subconjunctival injections of bevacizumab improved corneal wound healing after alkali burn injury. In that experiment, the corneal epithelial wound was accompanied by acute inflammation. The experimental model should therefore be considered when determining the effect of bevacizumab on corneal epithelial wound healing.
Differential effects of the 3 anti-VEGF agents were also found in studies using retinal pigment epithelial cells. 18 In this study, bevacizumab treatment, but not aflibercept or ranibizumab treatment, suppressed the phagocytic activity of human ARPE-19 cells. Based on the results of cell viability and phagocytic activity assays, it was suggested that the mechanism of action of bevacizumab differs from that of aflibercept and ranibizumab in ARPE-19 cells. Multiple nitration of humanized antibodies can result in unknown functional consequences, as well as changes in antigenic properties. 21 Wan et al. 22 showed that bevacizumab underwent multiple tyrosine nitration on its light and heavy chains to produce nitrotyrosine or aminotyrosine. Bevacizumab may therefore have cellular effects that are not a direct result of the VEGF pathway. Consistent with this possibility, the effects on wound healing of anti-VEGF agents could not be fully explained by their VEGF binding affinity, so other factors besides their antiangiogenic properties should be investigated.
A limitation of this study is that we diluted the 3 anti-VEGF agents to the same concentration. The concentrations for intravitreal injection are 40 mg/mL for aflibercept, 25 mg/mL for bevacizumab, and 10 mg/mL for ranibizumab. In addition, previous studies reported that healing of the corneal epithelium is influenced by the stromal response. 6 Since in vivo studies include environmental effects, further studies are needed.
Ideally, anti-VEGF agents should inhibit corneal neovascularization without affecting corneal epithelial cell viability and wound healing. However, bevacizumab decreased epithelial cell migration and viability. In previous studies comparing the antiangiogenic activities of bevacizumab and aflibercept, aflibercept was reported to have anti-VEGF activity even at relatively low concentrations. 12 Other anti-VEGF agents beside bevacizumab might therefore be a better option for treating corneal neovascularization complicated with epithelial defects.
Footnotes
Acknowledgment
This work was supported by a Clinical Research Institute Grant funded by The Catholic University of Korea Daejeon St. Mary's Hospital (CMCDJ-2015-013).
Author Disclosure Statement
No competing financial interests exist.