
Abstract
Abstract
Purpose:
To report the efficacy and safety of interferon (IFN) α-2a in patients with cystoid macular edema (CME) associated with presumed ocular tuberculosis (TB).
Methods:
We reviewed the clinical records of 5 patients with presumed ocular TB who had been treated with IFN α-2a for recurrent CME during or after completion of anti-tubercular therapy. IFN α-2a was administered at an initial dose of 3 million IU per day and then tapered after the initial response. Treatment efficacy was assessed by central macular thickness (CMT) measurement using spectral-domain optical coherence tomography and visual acuity.
Results:
Three patients were men, and 2 were women. Patients were aged between 38 and 66 years. Mean CMT was 483 ± 178.6 μm at baseline, 302.3 ± 56 μm at 1 week, 312.3 ± 49.5 μm at 1 month, and 286.2 ± 31.9 μm at 3 months. Mean LogMAR visual acuity was 0.6 ± 0.4 at baseline, 0.4 ± 0.3 μm at 1 week, 0.3 ± 0.3 at 1 month, and 0.3 ± 0.3 at 3 months. The treatment was interrupted for 10 days because of neutropenia after 2 weeks in 1 patient and discontinued in another after 10 days because of intolerance. Total treatment duration was 3–24 months in the remaining 4 patients.
Conclusion:
The present small case series suggests that IFN α-2a may be an effective and safe therapeutic option for CME that is associated with presumed ocular TB.
Introduction
C
Conventional treatment of uveitic macular edema includes the use of topical nonsteroidal anti-inflammatory drops, oral, periocular, or intravitreal injections, or intravitreal implants of corticosteroids along with the treatment of underlying disease with immunomodulatory therapy (IMT) in non-infectious or anti-infectious agent(s) in infectious uveitic entities. 2 However, corticosteroids may need to be avoided in some patients. Moreover, in a number of patients, uveitic macular edema runs a chronic and persistent course, despite lack of active intraocular inflammation. Alternative treatment options include oral carbonic anhydrase inhibitor, 2 intravitreal bevacizumab,3–6 systemic octreotide,7,8 systemic or intravitreal tumor necrosis factor-alpha (α) inhibitors,9–13 or interferon (IFN) α-2a or −2b therapy.14–17
A recent study showed efficacy of IFN α-2a in the management of CME due to infectious uveitis, including viral and syphilitic posterior uveitis. 14 To the best of our knowledge, there has been no report on the use of IFN α-2a for the treatment of CME that is associated with ocular tuberculosis (TB). We herein report 5 cases with persistent and/or recurrent CME that is associated with presumed ocular TB treated with IFN α-2a, in addition to or after anti-tubercular therapy (ATT).
Methods
Four patients (patients 1–4) were treated at the Uveitis Service, Istanbul University, Istanbul Faculty of Medicine, Department of Ophthalmology, and 1 patient (Patient 5) was treated at V.K. Foundation, American Hospital, Department of Ophthalmology.
The research followed the tenets of the Declaration of Helsinki. The retrospective study protocol was approved by the Ethics Committee of Istanbul University, Istanbul Faculty of Medicine. An informed consent was obtained before all diagnostic and therapeutic procedures.
In this retrospective study, the clinical records of patients were reviewed for demographic data, ocular and medical history, ocular findings, color fundus photographs (Carl Zeiss Meditec, Hennigsdorf, Germany), fluorescein angiography (FA) images (Heidelberg Engineering, Heidelberg, Germany), spectral-domain optical coherence tomography (SD-OCT) scans (Heidelberg Engineering, Heidelberg, Germany), laboratory results, and treatment modalities. A complete ocular examination was performed at each visit, including best-corrected Snellen visual acuity, slit-lamp biomicroscopy, tonometry, and indirect ophthalmoscopy. Anterior chamber flare was measured by a laser flare photometer (Kowa FC-2000; Kowa Company Ltd., Electronics and Optics Division, Tokyo, Japan) at the Uveitis Service, Istanbul Faculty of Medicine. Standardization of uveitis nomenclature criteria was used for anatomical classification of uveitis. 18
The diagnosis of presumed ocular TB was made based on a positive tuberculin skin test and/or QuantiFERON-TB Gold test positivity as well as suggestive findings on chest imaging and exclusion of other infectious and non-infectious etiologies. All patients received ATT with or without concomitant systemic corticosteroids. No other immunosuppressive treatment was used before or along with IFN therapy. Peribulbar corticosteroid injections or intravitreal injections of dexamethasone implant and/or bevacizumab, topical and/or systemic non-steroidal anti-inflammatory drugs were also used initially for the treatment of CME. IFN α-2a (Roferon-A, Hoffmann-La Roche, Nutley, NJ) was administered at an initial dose of 3 million IU (MIU) per day subcutaneously and tapered to twice or thrice weekly after 1–2 weeks. To lessen flu-like symptoms, oral paracetamol twice a day was additionally administered in the initial treatment phase. Routine blood parameters, including complete blood count and liver enzymes, were measured before treatment and weekly during the first month and then every 4 weeks to monitor possible side effects. IFN α-2a dose was adjusted based on side effects.
The main outcome criterion of the analysis was the efficacy of IFN α-2a treatment assessed as the decrease in central macular thickness (CMT), which was measured by OCT at each visit. As a secondary outcome criterion, visual acuity was measured in Snellen decimals and converted to a logarithm of the minimum angle of resolution (logMAR) for computing.
Results
Five patients (3 men and 2 women) with 7 affected eyes were included in this study. The age of the patients at the initiation of IFN α-2a treatment ranged between 38 and 66 years. Demographic features, type of uveitis, and previous and concomitant medication of the patients are shown in Table 1.
IFN treatment was started 6 and 5 months after completion of anti-tubercular therapy.
F, female; IFN, interferon; LE, left eye; M, male; NSAID, nonsteroidal anti-inflammatory drug; RE, right eye.
For all 5 patients, the diagnosis of ocular TB was made according to the clinical evidence and an extensive work-up. All patients revealed QuantiFERON-TB Gold test positivity. Tuberculin skin test was performed in 4 patients (patients 1–4), and it was >15 mm in all. In addition, chest computerized tomography (CT) revealed calcified pulmonary nodules in these 4 patients. Patient 5 had a history of culture-proven skin TB that had been treated with ATT 24 years ago.
ATT was given to all patients, including patient 5 who received a second course of ATT for the treatment of intraocular inflammation. Four-drug (isoniazid, rifampicin, ethambutol, and pyrazinamide) (patients 2 and 5) or 3-drug (isoniazid, rifampicin, and pyrazinamide) (patients 1, 3, and 4) ATT was administered in all patients for 2 months. Subsequently, 2-drug ATT (rifampicin and pyrazinamide) was completed at 7 months in 1 patient (patient 5), at 10 months in 2 patients (patients 1, 2), and is ongoing in patients 3 and 4 for 5 and 7 months, respectively. Two patients (patients 1, 2) also received concomitant systemic corticosteroid treatment. It was not given to 2 patients because of gastric ulcer (patient 3) and osteoporosis (patient 4). IFN α-2a 3 MIU was started 6 and 5 months after the completion of ATT in patients 1 and 2, respectively, and along with 2-drug ATT in patients 3, 4, and 5.
The average interval between development of CME during ATT and initiation of IFN treatment was 9 ± 5.7 (range 4–16) months. Pretreatment of CME included systemic corticosteroids (3 patients), peribulbar corticosteroid injection (1 eye), or intravitreal injections of extended-release dexamethasone implant 0.7 mg (Ozurdex®; Allergan, Inc., Irvine, CA) (4 eyes) and/or bevacizumab (1 eye), topical (all eyes) and/or systemic non-steroidal anti-inflammatory drugs (1 patient). Patients 1 and 5 had glaucoma, and patients 2 and 4 had intraocular pressure (IOP) rise after intravitreal dexamethasone implant injection.
IFN α-2a doses and follow-up of CMT and LogMAR visual acuities are shown in Table 2. There was a rapid improvement at the first week with a reduction of mean CMT from 483 ± 178.6 to 302.3 ± 56 μm and an improvement of mean LogMAR visual acuity from 0.6 ± 0.4 to 0.4 ± 0.3 μm. Treatment was discontinued after 10 days in patient 4 because of intolerance of symptoms such as fatigue, myalgia, and loss of appetite and CME did not recur during 3 months of follow-up. In the remaining 4 patients who continued to receive IFN treatment, mean CMT remained at 312.3 ± 49.5 μm at 1 month, and it further decreased to 286.2 ± 31.9 μm at 3 months. Mean LogMAR visual acuity was 0.3 ± 0.3 at 1 and 3 months. Visual acuities showed improvement in all eyes; however, it was worse than 0.3 LogMAR at the final visit in 4 eyes because of epiretinal membrane (ERM) formation and/or ellipsoid zone defects.
Recurrence of cystoid macular edema was treated with an increased dose of IFN 3 MIU every other day for 2 weeks.
IFN was stopped after the second week because of neutropenia and restarted at 3 MIU for 1 week after the first month.
IFN was discontinued after 10 days because of intolerance.
The final visit was at 6 months; the patient continued IFN therapy for 24 months. Follow-up information was provided by the patient' ophthalmologist in Iraq by email.
CMT, central macular thickness; MIU, million international units; N/A, not available; OS, oculus sinister; OD, oculus dexter; VA, visual acuity.
Side effects of IFN α-2a therapy included flu-like symptoms in all patients, neutropenia and thrombocytopenia in 1 patient, and neutropenia in another patient. Cytopenias were controlled with dose reduction or interruption of IFN therapy. No patient had elevation of liver enzymes. Total duration of treatment was 3, 9, 3, and 24 months in patients 1, 2, 3, and 5, respectively. Patients 2 and 3 are still on 3 MIU twice-weekly treatment without any side effects. Patients 1, 4, and 5 remained stable for the next 3–6 months after cessation of IFN therapy.
Patients
Patient no. 1
A 63-year-old Turkish man was referred with bilateral recurrent granulomatous anterior uveitis for 15 years, bilateral broad based posterior synechiae, and elevated IOP in the left eye. LogMAR visual acuity at presentation was 0.2 in the right eye and 0.3 in the left eye. Fundus examination at presentation was unremarkable. Chest CT showed calcified hilar lymph nodes, and tuberculin skin test was 20 mm. He was started on 3-drug ATT along with systemic corticosteroid therapy. CME developed in the left eye 6 months after the completion of ATT. Macular edema responded well to systemic corticosteroid and topical nepafenac therapy; however, it recurred during corticosteroid taper. Local corticosteroid injection could not be administered because of glaucoma. He was started on IFN α-2a 3 MIU/day. LogMAR visual acuity was 0.5, and CMT was 703 μm before initiation of IFN therapy. CME resolved at the first week of treatment. Reduced platelet count and neutropenia was managed by tapering IFN dose to 3 MIU twice weekly. The patient continued IFN α-2a 3 MIU twice weekly for 3 months without any side effects and remained stable for the next 3 months of treatment (Table 2). His final LogMAR visual acuity remained 0.3 because of ellipsoid zone defects on OCT.
Patient no. 2
A 43-year-old Turkish woman presented with progressive blurring of vision in the right eye over 2 years. Her LogMAR visual acuity was 1.3 in the right and 0.0 in the left eye. She had medium-sized pigmented keratic precipitates and 1+ cells in the anterior chamber in both eyes. Ophthalmoscopic findings were optic disk hyperemia, CME, multiple choroiditis scars (underlying the retinal vessels in 1 quadrant), periphlebitis, and snowball opacities in the right eye; optic disk hyperemia and inferior periphlebitis in the left eye. FA revealed staining of the optic disk, extensive deep capillary leakage at the posterior pole with CME, areas of capillary nonperfusion in peripheral retina, and retinal neovascularizations in the right eye. There was perivascular staining and leakage at the inferior peripheral retina in the left eye.
Chest CT showed a few enlarged hilar lymph nodes bilaterally, fibrotic parenchymal changes in the apex of the lungs, low-density millimetric nodules in the right middle lobe, and peribronchial ground-glass appearance on the left side. QuantiFERON-TB Gold test was positive. Serum angiotensin-converting enzyme and lysozyme levels were within normal limits.
She was started on 4-drug ATT along with systemic corticosteroid therapy. Nonperfused peripheral retinal areas were photocoagulated. She was given 2 intravitreal injections of dexamethasone implant in the right eye for chronic CME at initiation and at the seventh month of ATT (Fig. 1A). Temporary elevation of IOP was controlled by topical antiglaucoma medication. Two months after cessation of ATT, the patient presented with CME and a CMT of 518 μm (Fig. 1B) and was started on IFN α-2a 3 MIU/day. CME resolved at first week (Fig. 1C). The dose was tapered to 3 MIU thrice weekly after the first week and to twice weekly after the first month. Recurrence of CME at the third month was treated with an increased dose of IFN α-2a 3 MIU for 2 weeks and then, the maintenance was achieved with 3 MIU twice weekly. The patient is still on IFN α-2a for 9 months without recurrence of CME (Fig. 1D) (Table 2).
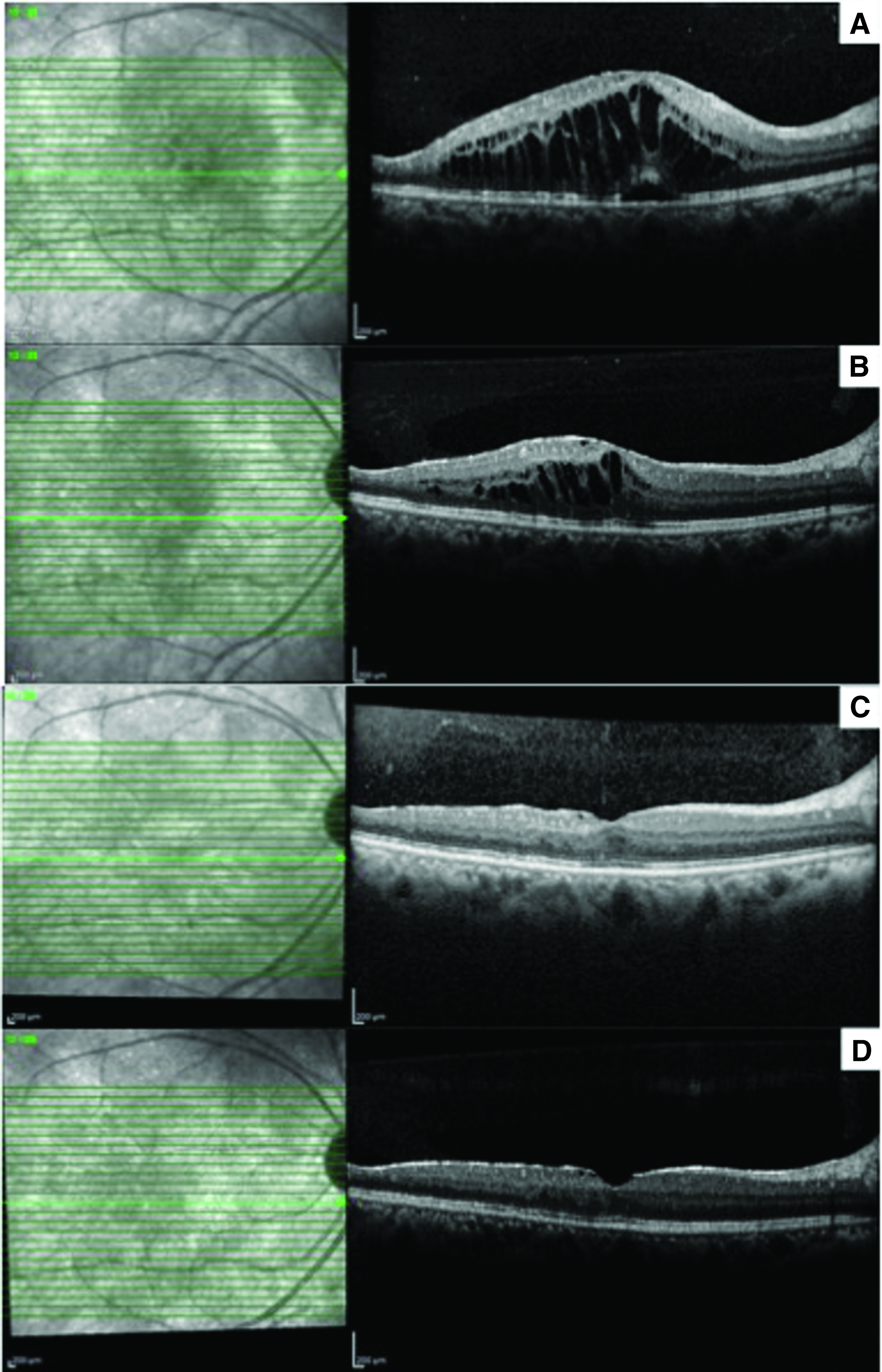
Serial spectral-domain OCT of the right eye of patient no. 2. CME and subretinal fluid is evident at the seventh month of ATT before the second intravitreal dexamethasone implant injection; CMT is 754 μm
Patient no. 3
A 38-year-old Turkish man was referred with bilateral intermediate uveitis for 7 years. Past medical history was significant for gastric ulcer. Ocular examination at presentation revealed LogMAR visual acuities of 1.3 in the right eye and 0.0 in the left eye. He had bilateral vitritis and intravitreal opacities. Fundus examination revealed bilateral optic disk hyperemia and CME in the right eye. Intravitreal dexamethasone implant was performed for CME in the right eye. Extensive laboratory work-up revealed a positive QuantiFERON-TB Gold test, tuberculin skin test of 16 mm, and bilateral pulmonary nodules on chest CT. He was started on 3-drug ATT with isoniazid, rifampicin, and pyrazinamide for 2 months followed by isoniazid and rifampicin. Systemic corticosteroid therapy could not be given because of gastric ulcer. At the fourth month of ATT, visual acuity was 1.3 in the right eye and 0.0 LogMAR in the left eye. CMT was 245 μm in the right eye and 344 μm in the left eye. FA revealed diffuse perifoveal microcystoid edema in the right eye and perifoveal capillary leakage in the left eye. IFN α-2a 3 MIU/day was started. LogMAR visual acuity improved to 1.0 in the right eye. IFN was stopped after 2 weeks due to neutropenia and restarted 10 days later because of recurrent CME. At the final visit, he was still on IFN α-2a 3 MIU twice-weekly therapy without any side effects (Table 2).
Patient no. 4
A 56-year-old Turkish woman was referred with bilateral granulomatous panuveitis for 18 months. She had received an intravitreal dexamethasone implant in the right eye before presentation. Her past medical history was significant for osteoporosis.
Visual acuity was 0.3 in the right eye and 0.7 LogMAR in the left eye at presentation. Biomicroscopic examination revealed bilateral granulomatous keratic precipitates, broad based posterior synechiae, and 2+ vitreous cells in both eyes. Fundus examination showed bilateral retinal vascular sheathing and choroiditis scars; active choroiditis in the left eye. CMT was 317 μm in the right eye and 554 μm in the left eye. FA revealed staining of the optic disk, perifoveal hyperfluorescence, areas of capillary nonperfusion in peripheral retina, and window defects that were consistent with choroiditis scars in the right eye. There was optic disk staining, extensive capillary leakage with CME, and areas of capillary nonperfusion in peripheral retina in the left eye.
Latent TB was diagnosed based on positive QuantiFERON-TB Gold test and tuberculin skin test (20 mm) as well as bilateral fibrotic sequelae in the apex of the lungs and calcified nodules on chest CT. She was started on 3-drug ATT with isoniazid, rifampicin, and pyrazinamide for 2 months followed by isoniazid and rifampicin. Systemic corticosteroid therapy was not given because of osteoporosis. Intravitreal dexamethasone implant was injected to the left eye. Because of IOP elevation after injection in the left eye, an intravitreal bevacizumab injection was administered for CME in the right eye. Non-perfused peripheral retinal areas were photocoagulated.
CME recurred at the fourth month of ATT, and IFN α-2a 3 MIU/day was started. Although CME resolved at the first week of treatment, she could not tolerate IFN therapy and the treatment was stopped at the 10th day because of side effects such as fatigue, myalgia, and loss of appetite. She did not have recurrent CME during the 3 months of follow-up (Table 2).
Patient no. 5
A 41-year-old man from Iraq presented with a 10-year history of uveitis in both eyes and decreased vision in the right eye. His medical history revealed that he had been given ATT for culture-proven skin TB 24 years ago. Past ocular history revealed bilateral retinal laser photocoagulation, after vitreous hemorrhage in the left eye, cataract extraction in both eyes, and trabeculectomy in the right eye. He had been treated with systemic corticosteroids, colchicine, and IMT, including methotrexate, azathioprine, and cyclosporine in the past.
At presentation, a skin scar on the left forearm due to healed skin TB was observed. He was otherwise healthy. Best-corrected LogMAR visual acuity was 0.4 in the right eye and 0.0 in the left eye. Ocular examination and FA at presentation revealed no active intraocular inflammation. However, he had CME in the right eye with CMT of 544 μm and bilateral peripheral retinal nonperfusion. Other than QuantiFERON-TB Gold test positivity, extensive laboratory workup regarding infectious and autoimmune etiologies was unrewarding. Chest CT was within normal limits. He was given periocular corticosteroid injection in the right eye for persistent CME, and laser photocoagulation was scheduled. However, the patient was lost to follow-up for 1 year.
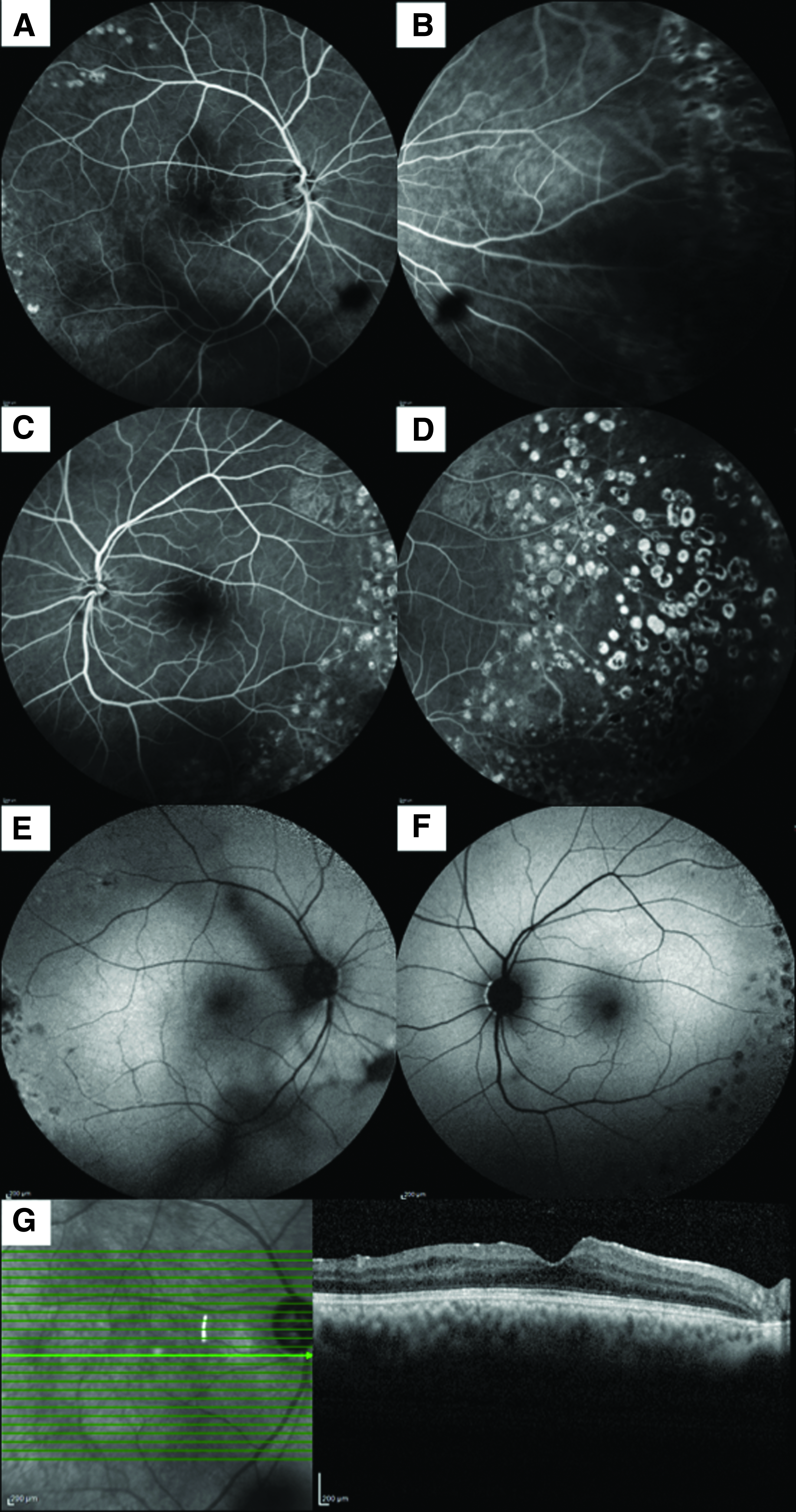
One year later, he presented with a decline of LogMAR visual acuity to 0.7 in the right eye. Fundus examination revealed vitritis in both eyes and active retinal vasculitis with persistent CME in the right eye. Retinal vascular staining and leakage, macular hyperfluorescence that was consistent with CME in the right eye, and areas of peripheral retinal nonperfusion in both eyes were observed on FA (Fig. 2A–D). Fundus autofluorescence (FAF) showed perifoveal petaloid hyperautofluorescence (Fig. 2E), and OCT showed CME (Fig. 2G) in the right eye. CMT was 548 μm. The patient was started on ATT with isoniazid, rifampicin, ethambutol, and pyrazinamide for 2 months followed by isoniazid and rifampicin for 7 months. Non-perfused peripheral retinal areas were photocoagulated; systemic and topical non-steroidal anti-inflammatory drugs were started. Recovery of retinal vasculitis and vitritis occurred within 3 months of ATT. The patient presented for follow-up at 6 months of ATT with worsening of CME, and CMT was 725 μm (Fig. 2H). IFN α-2a was added to the treatment. Three MIU of IFN α-2a was given for 14 days, and maintenance was achieved with 3 MIU thrice weekly. Two months after IFN treatment, a complete resolution of CME was observed, CMT decreased to 359 μm, and LogMAR visual acuity increased to 0.3. At 6 months, no abnormal fluorescence was detected on FA (Fig. 3A–D). Resolution of CME was apparent on FAF and SD-OCT (Fig. 3E–G). Thereafter, follow-up information was obtained from his ophthalmologist in Iraq. The patient received IFN α-2a for a total of 24 months concomitantly with ATT for the first 2 months and then as monotherapy. There has been no flare-up of intraocular inflammation or recurrence of CME during IFN therapy. He remained stable for the next 6 months after cessation of IFN α-2a.

FA, FAF and spectral-domain OCT of patient no. 5 before initiation of ATT. FA shows optic disk staining, petaloid pattern of hyperfluorescence at the fovea, segmental vascular staining of the inferotemporal retinal vein, retinal capillary leakage, and peripheral capillary nonperfusion in the right eye
FA, FAF and spectral-domain OCT of patient no. 5 at the sixth month of IFN α-2a therapy. FA shows complete resolution of CME, and laser photocoagulation scars covering retinal capillary dropout areas of hypoperfusion in the right eye
Discussion
The cases described herein demonstrate the efficacy and safety of IFN α-2a in the management of persistent and/or recurrent CME that is associated with presumed ocular TB. IFNs are a group of cytokines with known antiviral, anti-inflammatory, antiproliferative, and proapoptotic activities. IFN α-2a has been shown to have a significant efficacy and safety in the treatment of retinal vasculitis that is associated with Behçet disease and other uveitides.19–21 IFN has also been demonstrated to relieve chronic and persistent uveitic CME of a noninfectious source.15–17 A recent study showed efficacy of IFN α-2a in the management of CME of viral and syphilitic posterior uveitis as well. 14
Patients with ocular TB may present with a spectrum of clinical signs. The most common clinical presentation of ocular TB is posterior uveitis followed by anterior uveitis, panuveitis, and intermediate uveitis. The diagnosis of ocular TB is often presumptive as there is no confirmatory evidence. 22 In the present study, all patients were diagnosed with presumed ocular TB based on ocular clinical findings that were compatible with ocular TB and evidence of latent TB, including a positive IFN gamma release assay and/or tuberculin skin test, presence of healed tubercular lesions on chest CT (4 patients), and a history of culture-proven extrapulmonary TB of skin (1 patient).
Intraocular inflammation may be associated with active or latent TB. Successful treatment requires ATT in both conditions. In some cases, ocular complications, including CME, retinal vasculitis, or refractory intraocular inflammation, may occur despite ATT. Therefore, systemic and/or local corticosteroids and/or IMT may need to be added to the treatment.22,23 Two different treatment approaches for patients with latent TB-associated uveitis are seen in the present case series. Systemic corticosteroid therapy was given along with ATT to patients treated at Istanbul Faculty of Medicine, and the preferred approach at V.K.V American Hospital was ATT without concomitant systemic corticosteroid therapy. In this case series, intraocular inflammation was observed in all patients who rapidly responded to ATT with or without concomitant systemic corticosteroids. However, the patients developed recurrent CME in the absence of active intraocular inflammation. The underlying mechanism of chronic uveitic CME is believed to be a diffuse damage of the blood-retina barrier. 1 It has been shown that IFN α-2b enhances barrier function of bovine retinal microvascular endothelium in vitro. 24 Deuter et al. have suggested a similar mechanism of action of IFN α-2a in the treatment of macular edema.15,16 A dramatic improvement of CMT at the end of the first week of IFN α-2a treatment in the present series could also be attributed to rapid restoration of the blood-retina barrier. Although visual acuities showed improvement in all eyes, it was less than 0.3 LogMAR at the final visit in 4 eyes because of ERM and/or permanent ellipsoid zone defects.
There is no consensus on the dose of IFN α-2a for the treatment of macular edema. In the present study IFN α-2a was administered at an initial dose of 3 MIU/day subcutaneously and tapered to twice or thrice weekly after 1–2 weeks. However, in the study by Deuter et al., 15 IFN α-2a was administered at an initial dose of 3 or 6 MIU/day subcutaneously depending on body weight and the initial dose was 3 MIU 3 times a week in the study by Qian et al. 14 In addition, to initiate IFN therapy, patients were hospitalized in these 2 studies14,15; however, in our study, the treatment was administered in an outpatient setting from the beginning. The optimum duration of treatment also remains unclear. Although macular edema resolves promptly after initiation of IFN α-2a therapy, as seen in all studies including ours, recurrences after treatment cessation or dose tapering may be observed. However, patients respond to reinstitution of therapy.14,15
Side effects occur frequently during IFN α-2a therapy; however, they are mostly dose dependent. As reported in the literature, the most common side effect in our series was a flu-like syndrome that was always observed at the introduction of treatment or at reinstitution after treatment interruption and relieved by oral paracetamol in a few days. Other common side effects were reported to be mild leukopenia (30%) and alopecia (10%). Furthermore, systemic side effects, including bone marrow fibrosis, erythema, depression, hypothyroidism, and endocrine disorders, were shown to have an overall frequency of <1%. 25 Fatigue, loss of appetite, and feeling unwell may necessitate discontinuation of IFN therapy. In our series, 1 patient developed neutropenia and thrombocytopenia, which resolved with dose tapering, and in another patient, the treatment had to be interrupted for 10 days because of neutropenia.
In conclusion, the use of IFN α-2a resulted in a resolution of persistent CME in a small series of patients with presumed ocular TB without systemic or intraocular TB reactivation. Prospective larger studies are needed to determine the minimal effective dose and the optimum duration as well as the safety of IFN therapy for the treatment of CME that is associated with presumed ocular TB.
Footnotes
Author Disclosure Statement
No competing financial interests exist. I.T.-T. has received financial support outside the submitted work, including honoraria from Servier, AbbVie, Santen, and Allergan.