
Abstract
Abstract
Purpose:
This study was designed to evaluate the effect of chitosan-N-acetylcysteine (C-NAC) eye drops on tear film thickness (TFT) in patients with dry eye syndrome (DES).
Methods:
This was a controlled, randomized, double-blind clinical investigation with patients assigned to 2 cohorts. In Cohort I, 21 patients were randomized to receive 1 instillation of C-NAC eye drops in 1 eye and placebo (normal saline solution) in the contralateral eye. In Cohort II, 17 patients were randomized to receive C-NAC eye drops once (QD) or twice (BID) daily for 5 days. TFT was assessed with a custom-built ultrahigh-resolution optical coherence tomography system.
Results:
In Cohort I, mean TFT increased from 3.9 ± 0.5 μm predose to 4.8 ± 1.1 μm 10 min postdose after treatment with C-NAC. The increase was significantly different from placebo over time (P < 0.0001) and remained stable until 24 h postdose. In Cohort II, TFT increased with QD and BID instillation, with no significant difference between regimens. In both groups, Ocular Surface Disease Index scores improved, fewer patients presented with corneal damage, and symptoms of ocular discomfort/conjunctival redness were reduced.
Conclusions:
A single instillation of C-NAC significantly increased mean TFT in patients with DES as early as 10 min after instillation and lasted for 24 h. The magnitude of the increase in TFT following a single instillation was comparable with that after instillation twice daily over 5 days. Corneal damage improved in >60% of patients. C-NAC could be a viable treatment option for DES.
Introduction
D
Patients with DES frequently use topical treatments containing biopolymers such as carboxymethylcellulose or hyaluronic acid (HA) to alleviate the symptoms of DES. These biopolymers lubricate the ocular surface, and their symptomatic benefit is largely related to an improvement of the tear film following instillation. The short residence of existing biopolymer-containing formulations, however, necessitates frequent instillation.4–6
We hypothesize that chitosan-N-acetylcysteine (C-NAC), a new biopolymer based on chemically modified chitosan, may overcome these limitations and can achieve longer ocular surface residence times. This, in turn, may provide dry eye patients with longer symptomatic relief, without the need for frequent instillation. C-NAC is based on a chitosan biopolymeric backbone, which is modified by the introduction of N-acetylcysteine (NAC) through nucleophilic substitution. Chitosan is a well-characterized polycationic polysaccharide derived from alkaline deacylation of chitin and exhibits low toxicity and excellent biocompatibility. 7 NAC, which is a derivative of amino acid L-cysteine, also has mucolytic properties and has been used to treat corneal and external eye diseases.7–10
C-NAC eye drops were awarded a CE mark in Europe in 2014 and launched under the trade name Lacrimera®. The objectives of the present study were 2-fold: (1) to evaluate the effects of topical C-NAC on tear film thickness (TFT) and (2) to evaluate the safety and efficacy of C-NAC eye drops (after single and multiple instillation) in the treatment of patients with DES.
Methods
Trial design
This was a controlled, randomized, double-masked clinical investigation to evaluate the safety and efficacy of C-NAC eye drops (0.1% w/v) in 2 cohorts of patients with DES. The study was conducted in accordance with the Declaration of Helsinki and in compliance with GCP, EN ISO 1455:2011, and other applicable national and local regulatory requirements.
Written informed consent was obtained at the screening visit after explanation of the nature and possible consequences of the study (day 14). Demographic, medical, and medication history data were collected and patients were evaluated for inclusion and exclusion criteria. A summary of study visits and scheduled assessments for both cohorts is provided in Table 1.
Patients in Cohort I were not eligible for Cohort II.
Predose for Cohort I and prefirst daily dose for Cohort II.
±3 minutes.
At 1, 2, 4, 8, and 10 h post-treatment ±10 minutes.
±20 min.
±60 min.
After first daily dose of C-NAC.
Eight to 10 h after first instillation, treatment with C-NAC or placebo.
For females of childbearing potential.
OSDI performed at screening for Cohort I and pretreatment for Cohort II.
TBUT and OSDI were assessed for patients in Cohort II before the first dose on day 1, but not on days 2–5.
C-NAC, chitosan-N-acetylcysteine; OSDI, Ocular Surface Disease Index; TBUT, tear breakup time; TFT, tear film thickness.
In Cohort I, patients were randomized to receive 1 instillation of C-NAC eye drops (∼35 μL) in 1 eye and placebo (0.9% sterile physiological saline) in the other eye. In Cohort II, patients were randomized to receive C-NAC eye drops once daily (QD) or twice daily (BID), respectively. C-NAC eye drops were instilled in both eyes in the morning. To maintain double-masked conditions, in the evening, only 1 eye received C-NAC eye drops (BID), while placebo was instilled in the other eye (QD).
Patients in Cohort I were evaluated at screening, days 1 and 2. Patients in Cohort II were evaluated at screening, at every dosing day (days 1–5), and at the final examination (day 6).
Inclusion and exclusion criteria
Inclusion criteria included adult patients >18 years, with a history of DES for at least 3 months, and at least 2 of the following 3 criteria: tear breakup time (TBUT) <10 s and/or Schirmer I test <7 mm and/or at least 2 symptoms of DES (foreign body sensation, burning, photophobia, blurred vision, pain, itching). Patients had to have normal ophthalmic findings except DES and ametropy <6 diopters (Dpt). No administration of topical lubricants was permitted 24 h before the screening examination.
Exclusion criteria included symptoms of a clinically relevant illness other than dry eye in the 3 weeks preceding the screening visit, the presence or history of a severe medical condition as judged by the clinical investigator, ocular infection or clinically significant inflammation, ocular surgery in the 3 months preceding the clinical investigation, glaucoma, Sjögren's syndrome, Stevens–Johnson syndrome, or history of allergic conjunctivitis. Patients were also excluded if severe dry eye was diagnosed by Schirmer I test <2 mm or if the difference in TBUT between the 2 eyes was ≥4 s or if ametropy ≥6 Dpt.
Further exclusion criteria included requirement for contact lens use during the study, treatment with corticosteroids in the 4 weeks preceding the clinical investigation, topical treatment with any ophthalmic drug except topical lubricants in the 4 weeks preceding the clinical investigation, use of parasympathomimetic or antipsychotic drugs, participation in a clinical trial in the 3 weeks preceding the screening visit, and pregnancy, planned pregnancy, or lactation.
Optical coherence tomography
An ultrahigh-resolution spectral domain optical coherence tomography (OCT) was custom-built for measurement of TFT as described previously. 11 By employing a titanium–sapphire laser as light source, an axial resolution of 1.3 μm was achieved at the cornea. Three-dimensional volumes centered on the apex of the cornea, with a size of 4 × 4 × 1 mm (horizontal × vertical × depth), were acquired and each contained 512 × 128 × 1,024 pixels. Central TFT was evaluated from the tomograms around the central reflex of the probe at the apex (indicated by saturation of the spectrometer's CCD camera). System parameters, such as focus of the probe beam and exposure time of the CCD camera, were set to enable optimal tear film imaging. The patient's head was stabilized on a modified slit-lamp headrest. Patients were asked to look straight ahead onto an internal fixation target and blink normally. Data acquisition started immediately after opening of the eye. Four 3D volumes were recorded within 4 s and TFT was gained from the second and third volumes. All axial distance values for the TFT obtained with OCT were divided by the average group refractive index for the tear film of 1.339 to obtain geometrical distances. 11
Objective scattering index
Scattering of the tear film was measured noninvasively with the commercially available Optical Quality Analysis System (OQAS, Visometrics, Spain), in accordance with the manufacturer's instructions. In principle, a punctual light source produced by a 780 nm laser is imaged on the retina. The size and the shape of the light spot (light passes twice through ocular media after retinal reflection) are then analyzed by an OQAS computer system. Based on these data, the objective scattering index (OSI) is calculated. Given that changes in the tear film are also reflected in the image produced on the retina, the OSI can be used as a measure of tear film quality. The measurement took about 20 s and was well tolerated.
TBUT and Schirmer I test
TBUT and Schirmer I test (without anesthesia) were measured as outlined in published guidelines in the Report of the International Dry Eye Work Shop 2007. 12
Symptoms of dry eye
Symptoms of dry eye were assessed subjectively using the Ocular Surface Disease Index© (OSDI©), 13 with higher scores representing greater disability.
Patients were also asked to assess ocular discomfort and conjunctival redness based on the following parameters: burning, stinging, erythema, swelling, pruritus, blurring, and other signs and symptoms using a 4-point scale (graded from 0 to 3) corresponding to no symptoms (grade 0), mild (grade 1), moderate (grade 2), or severe symptoms (grade 3), respectively.
Fluorescein staining of the cornea
Fluorescein staining of the cornea was performed using Minims fluorescein sodium 2.0% eye drops (Chauvin Pharmaceuticals, United Kingdom) to detect corneal damage using a slit-lamp examination. The Oxford grading scheme was used, 14 which rates ocular staining with fluorescein according to a picture scale with 6 grades (0 = absent, I = minimal, II = mild, III = moderate, IV = marked, and V = severe).
Endpoints
The primary efficacy endpoint was TFT as measured with OCT. Secondary endpoints included OSI, TBUT, OSDI, Schirmer I test, staining of the cornea with fluorescein, patient's evaluation of ocular discomfort, and conjunctival redness.
Statistical methods
Statistical analyses were conducted by patient and by eye. The safety analysis dataset (SAF) included all patients who were randomized to receive at least 1 instillation of either C-NAC eye drops or placebo. The intent-to-treat (ITT) analysis set included all patients who received at least 1 instillation of test substance. The per-protocol analysis set (PPS) included all patients who completed the study without major protocol violations.
The primary efficacy and all secondary efficacy variables were analyzed based on the PPS and ITT analysis set. The analysis of the primary efficacy variable based on PPS was confirmatory; all other analyses were considered exploratory. Other relevant variables were analyzed based on the ITT analysis set. Analyses of safety variables, demographics, and other covariates were based on the SAF.
TFT was analyzed descriptively by treatment group, visit, and time. The absolute change and percentage change in TFT from predose on days 1–8, 10, 12, and 24 h postdose (24 h = day 2) in Cohort I and from predose on days 1–6 in Cohort II were analyzed stratified by treatment group. A regression analysis considering the repeated measurements in both factors (eye and time) was used to detect differences between treatment groups. All secondary efficacy variables were analyzed descriptively by visit, time within study day (if applicable), and treatment group.
Results
A total of 38 patients were enrolled, 21 in Cohort I and 17 in Cohort II (Fig. 1). The majority of patients in both cohorts were females (71% and 77%, respectively), with median ages of 36 and 24 years, respectively.
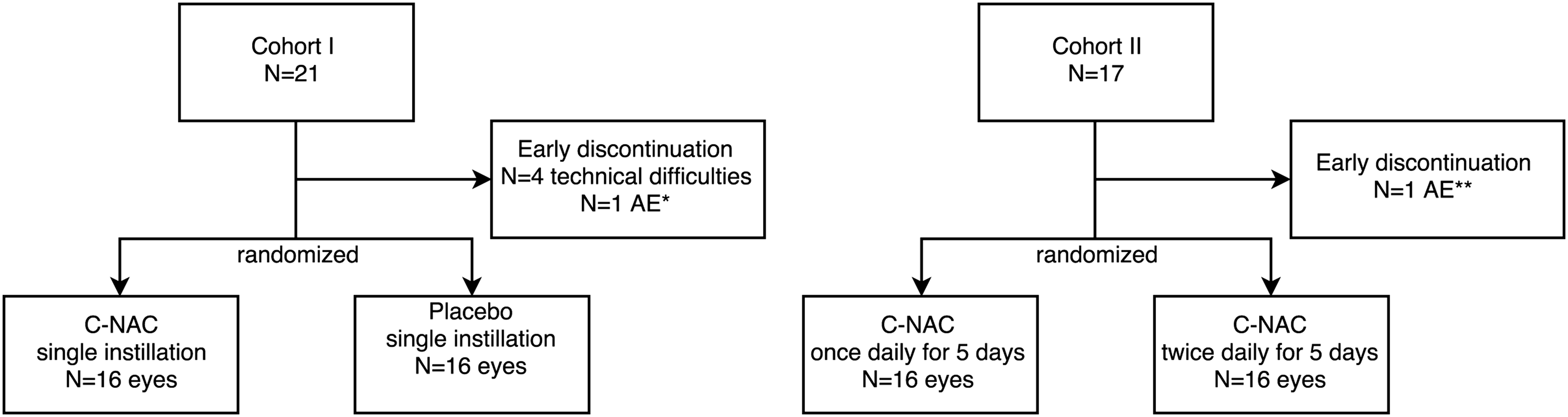
Patient disposition. *Corneal erosion, **Gastroenteritis; N = number of patients.
Tear film thickness
The mean, baseline TFT value for Cohort I was 3.91 ± 0.50 μm in the group randomized to receive C-NAC and 4.02 ± 0.66 μm in the placebo group. Ten minutes after instillation, the mean TFT increased significantly to 4.82 ± 1.13 μm in the C-NAC group compared with 4.38 ± 1.11 μm in the placebo group. The increase in TFT remained stable (P < 0.0001, regression analysis) over the 24-h period studied (Fig. 2).
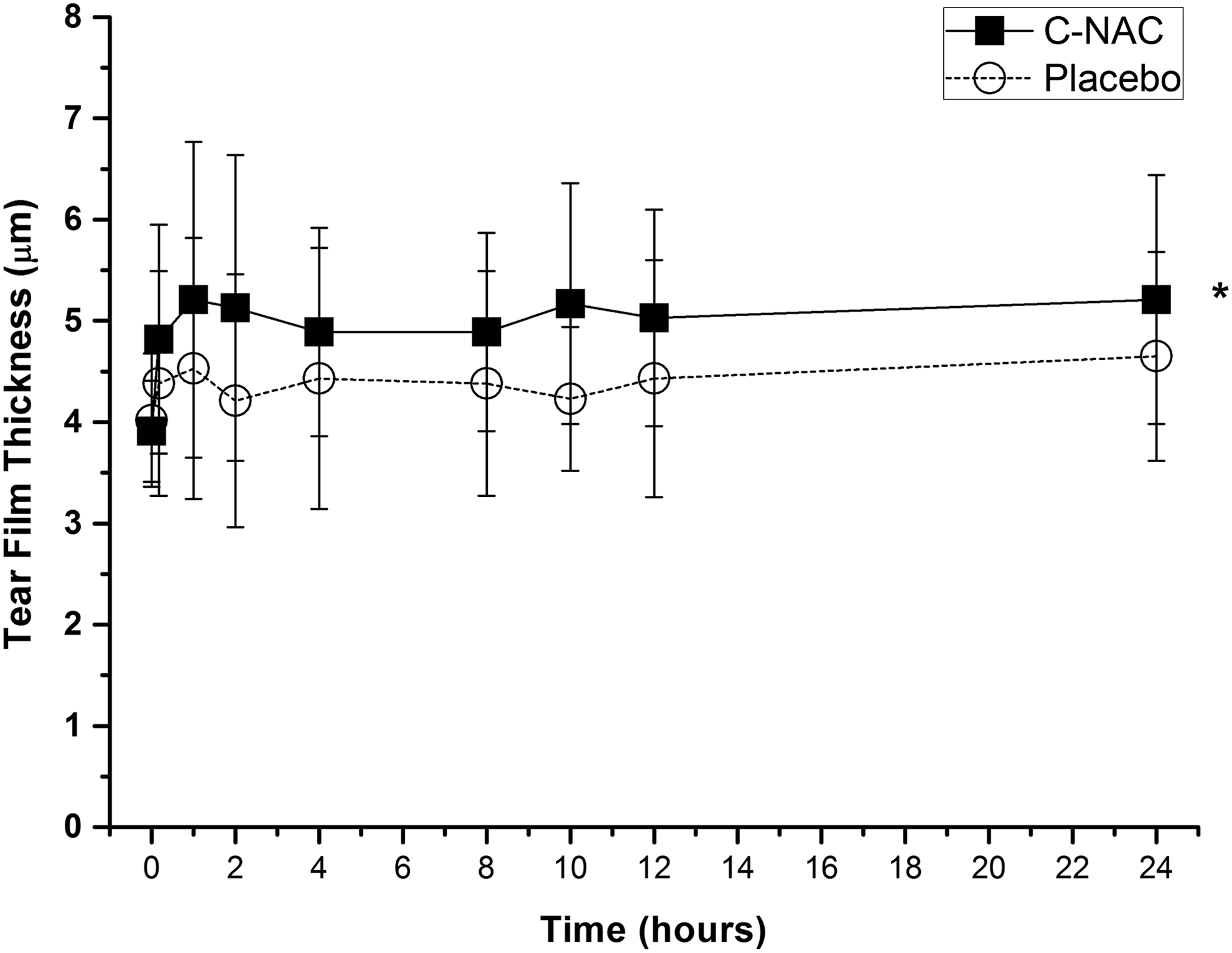
Mean TFT values (μm) over time for C-NAC and placebo-treated eyes for patients in Cohort I. Mean TFT measured by optical coherence tomography in patient's eyes predose and at 10 min, 8, 10, 12, and 24 h post-treatment with C-NAC eye drops or placebo (normal saline). Error bars are standard deviations and include the sample size. *Significant increase in TFT after treatment with C-NAC versus placebo (P < 0.0001, Regression analysis). C-NAC, chitosan-N-acetylcysteine; TFT, tear film thickness.
For patients in Cohort II, mean baseline TFT values were 3.89 ± 1.09 μm in the eye that was to receive C-NAC eye drops BID and 3.94 ± 1.14 μm for the eye that was to receive C-NAC eye drops QD. TFT increased with both treatment regimens, with TFT values on all study days greater than those measured on day 1 (P = 0.0015 BD on day 2; P = 0.0005 QD on day 2. PPS data sets, paired t-test). An increase in TFT up to 4.90 ± 1.49 μm was seen in the eye that received C-NAC eye drops BID (day 6) and up to 4.86 ± 1.73 μm in the eye that received C-NAC eye drops QD (day 5). There was no statistically significant difference in TFT between the QD and BID regimens (P = 0.8837, regression analysis, Fig. 3).

Mean TFT values (μm) for Cohort II patients treated with C-NAC once or twice daily for 5 days. Mean TFT (μm) measured by optical coherence tomography in patient's eyes predose and each day before treatment with C-NAC administered once (QD) or twice (BID) daily for 5 consecutive days. Error bars are standard deviations and include the sample size.
Staining of the cornea with fluorescein
Staining of the cornea with fluorescein was performed only on patients in Cohort II. At screening, 6 patients (37.5%) in the BID group and 7 patients (43.8%) in the QD group presented with corneal damage as estimated by fluorescein staining. From screening to day 6, there was an improvement with both treatment regimens, with corneal staining reported in only 3 patients (18.8%) in the BID group and 2 patients (12.6%) in the QD group.
OSDI score
For patients in Cohort I, OSDI was assessed only at screening, with baseline OSDI ranging from 15 to 65 (median 33.0). For patients in Cohort II, the baseline OSDI ranged from 2 to 83 (median 38.5). By day 6, the OSDI had decreased, ranging from 2 to 67 (median 13.0), corresponding to an absolute change from baseline ranging from −53 to −23 (median −16.5). This corresponds to a decrease in OSDI of 60.5% from day 1 to 6, indicating that the subjective severity of DES, as assessed with OSDI, improved after 5 days of treatment with C-NAC eye drops.
OSI, Schirmer test, or tear breakup time
No significant differences in OSI, Schirmer I test, or TBUT were observed between the 2 treatment groups in either of the 2 cohorts. Detailed data are given in Tables 2 and 3.
Data are presented as median and minimum to maximum range.
OSI, Objective Scattering Index.
Data are presented as median and minimum to maximum range.
Patient's evaluation of ocular discomfort and conjunctival redness
Patients in Cohort I reported symptoms of ocular discomfort, including burning, stinging, erythema, pruritus, blurred vision, and foreign body sensation. Overall, for most symptoms, no apparent effect of C-NAC was observed, that is, there were no differences between C-NAC and placebo treatments (Table 4) in Cohort I. For Cohort II, reported symptoms also included burning, stinging, erythema, pruritus, blurred vision, and foreign body sensation. In cohort II, for both the 2 times instillation and the 1 time instillation, the frequency of reported symptoms declined with the time treated with C-NAC. No significant difference between the 2 times instillation and 1 time instillation was observed regarding the frequency of patients reporting symptoms (PPS data set, P = 0.4460, regression analysis).
All symptoms were mild if not indicated otherwise.
Ten minutes postinstillation.
Twenty-four hours postinstillation.
Change from day 1 predose to 10 min postinstillation (day 1 postdose).
Change from day 1 predose to 24 h postinstillation (day 2 postdose).
I, improvement; N, number of patients; NC, no change; W, worsening.
Including 1 case of moderate symptom.
Including 2 cases of moderate symptom.
Safety
No serious adverse events (AEs) were reported during the clinical investigation and a total of 11 AEs were reported in 7 patients (19.0%), all of which were assessed as mild. Eight AEs were reported in 4 patients in Cohort I. Eye-related AEs in Cohort I included corneal erosion in 1 placebo-treated eye, foreign body sensation (in 2 placebo and 2 C-NAC-treated eyes), and pruritus (C-NAC-treated eyes). Noneye-related AEs included headache and pruritus in 1 patient each.
Three AEs were reported in 3 patients in Cohort II (17.6%). One eye-related AE, eye irritation, occurred in 1 patient with both the BID and QD treatment regimens and was considered possibly related to C-NAC instillation. Noneye-related AEs included gastroenteritis and headache in 1 patient each.
No changes in intraocular pressure were reported in patients after treatment with C-NAC or placebo or with either treatment regimen (data not shown).
Discussion
Since tear film instability is a core mechanism of DES, the development of new molecules, which combine a long residency time on the ocular surface with a good safety profile, would be desirable. The data of the current study indicate that topical administration of C-NAC is safe in patients with DES and increases TFT as measured with ultrahigh-resolution OCT up to 24 h after instillation. To the best of our knowledge, this is the first study to report a significant increase in TFT lasting for 24 h after a single instillation.
Although a variety of different lubricants such as cellulose esters, venyldeviates, or HA-derived substances are available and widely used, the current approaches for topical lubricant therapies are either limited by the short residence time on the ocular surface or by high viscosity, which may interfere with sharp vision.15–19
C-NAC, tested in this study, is a positively charged macromolecule that contains reactive NAC substitutions. On the ocular surface, C-NAC is expected to electrostatically and chemically bind to negatively charged reactive mucins on the ocular surface. 10 In particular, covalent interactions of free thiol moieties originating from C-NAC and disulfides from mucosal glycoproteins produce an artificial glycocalyx-like structure on the eye. This in turn may lead to an enhanced stability of the polymer–mucin network.
The theoretical consideration suggesting that C-NAC shows an increased adhesion to the ocular surface is supported by the data of this study. In Cohort I, a single administration of C-NAC eye drops resulted in a significant increase in TFT, compared with patients who received placebo. This effect was evident 10 min after treatment and lasted over the entire observation period of 24 h, indicating a residency time of at least 24 h for C-NAC. This is also supported by data from Cohort II, which showed no significant difference between BD and QD instillation, which suggests that a single daily treatment with C-NAC is likely to be effective in increasing TFT in patients with DES.
The results of the current study are in good agreement with those from preclinical studies of ocular residence time and biodistribution of C-NAC in rabbits using microPET technology. 20 The latter study showed that radioactively marked C-NAC was detected on the ocular surface during the entire imaging period (up to 22 h) after application, whereas aqueous control was detected only during the first hour after application. Furthermore, from calculated time–activity curves, the area under the curve of C-NAC formulations was 2.2-fold higher when compared with the unmodified chitosan. This indicates an ocular residency time of C-NAC on the ocular surface of 24 h or more and supports the concept that a once-a-day instillation of C-NAC leads to stabilization of the tear film.
Using the same OCT technology, we have recently reported that HA significantly increases TFT after topical administration, an effect that was observed for as long as 30 min postinstillation. 21 However, since the latter study was performed in healthy subjects, it is not clear to what extent these results hold true for patients with DES. Other studies investigating TFT with OCT have reported comparable results, notably administration of a combination of unpreserved trehalose and sodium hyaluronate increased TFT up to 240 min in patients with mild to moderate DES, 22 which is again considerably shorter than the increase in TFT observed in the current study. This is also consistent with other previously published studies using different OCT-based imaging techniques to investigate the effect of eye drops on the ocular tear film, all reporting shorter ocular residency times compared with C-NAC.23,24
In the current as well as in previous studies, we have used a custom-built ultrahigh-resolution OCT to assess TFT. 11 Based on a broadband titanium:sapphire laser operating at 800 nm and a high-speed charge-coupled device, this system allows for measurement of TFT with high reproducibility and resolution. As described previously, this system provides a resolution of 1.3 μm in tissue, defined as the ability of the system to separate 2 structures within 1 A-scan. Modeling of the OCT signal, in particular the improved detection of 2 signal peaks within the coherence functions, allows for the measurement of TFT with excellent reproducibility and validity.24,25 Changes in TFT much smaller than the resolution can be detected, which have been demonstrated theoretically and experimentally.24,25
Subjective assessments of the severity of DES also support the effectiveness of treatment with C-NAC. On the basis of OSDI questionnaires, our results show that after 5 days of treatment with C-NAC, the median OSDI score decreased by 60.5% from 38.5 to 13.0, consistent with a reduction in the severity of DES.
Corneal damage (assessed by fluorescein staining) was reduced in magnitude and/or severity from day 1 to 6 in both treatment regimens in Cohort II. For the secondary variables, OSI, TBUT, and Schirmer I test, there were neither clinically relevant changes nor statistically significant differences between both treatment groups in Cohort I and both treatment regimens in Cohort II, respectively.
With regard to evaluation of ocular discomfort and conjunctival redness, patients in both Cohorts reported symptoms of burning, stinging, erythema, pruritus, foreign body sensation, and blurred vision, which are commonly reported symptoms of DES. 3 Symptoms occurred in the C-NAC-treated eye as well as in the placebo-treated eye, with comparable incidence. Few patients in Cohort I reported symptoms of ocular discomfort and conjunctival redness and most of those reported were mild and none was severe. Similarly, in Cohort II, symptoms were mild and the frequency of reported symptoms declined with the time treated with C-NAC.
When interpreting the abovementioned results, it has to be kept in mind that the current study was designed and statistically powered to detect changes in TFT after single and multiple instillation of C-NAC and provide information regarding the ocular residency time and the optimal treatment schedule for C-NAC eye drops. Given the high variability of the classical parameters to assess the clinical efficacy of DES treatment such as BUT or Schirmer test, it is likely that the sample size was not high enough to detect changes in these variables. Furthermore, it has to be taken into account that the treatment period of only 5 days is most probably not long enough to induce pronounced changes in BUT, Schirmer test, and the subjective burden of the patients. A large, long-term, controlled multicenter study is currently being performed in Europe to assess the clinical benefit of C-NAC eye drops in patients with DES to investigate the clinical effect of long-term treatment with C-NAC.
As stated above, the technique of ultrahigh-resolution OCT allows for direct visualization of the most critical component in DED, the tear film itself. Although this may be a promising approach in the clinical management of DED, the question to what extent TFT reflects other classical subjective and objective parameters of DED warrants further investigation. Data of a recent study show a moderate but statistically significant correlation of TFT with both OSDI and BUT. 22 In view of the fact that the association between signs and symptoms is generally weak in DED, measurement of TFT may in future become a valuable tool in the management of DES patients. Larger studies are, however, needed to fully understand the potential of TFT measurement in DED research and clinical management.
The safety data of the current study indicate that C-NAC was safe and well tolerated, with no SAEs reported during the course of the clinical investigation. A total of 11 AEs were reported in 7 patients, comprising 8 AEs in 4 patients in Cohort I and 3 AEs in 3 patients in Cohort II, all of which were judged as mild and had resolved by the end of the study. Eye-related AEs in Cohort I included corneal erosion, eye pruritus, and foreign body sensation, with no relevant difference between treatment with C-NAC and placebo.
In conclusion, this study has demonstrated that C-NAC eye drops are safe and effective when applied once or twice per day for 5 consecutive days in patients with DES. Treatment with C-NAC led to a significant increase in TFT over time compared with placebo and lasted for 24 h after a single instillation. Moreover, the clinical improvement of C-NAC treatment was confirmed by improved OSDI scores, reduced incidence of corneal damage, and reduced frequency of symptoms of ocular discomfort and conjunctival redness in Cohort II after 5 days of C-NAC treatment. As current DES therapies often require multiple daily instillations, C-NAC could provide a viable option for the treatment of DES and could improve the quality of life of the vast number of people suffering with DES. A multicentric phase 4 study investigating the efficacy and safety of C-NAC during long-term use is currently ongoing to further elucidate the clinical effectiveness of C-NAC.
Footnotes
Author Disclosure Statement
The study was sponsored by Croma-Pharma GmbH. R.B., S.H., M.O.’R., and M.P. are employees of Croma-Pharma, W.P. is a past employee of Croma-Pharma, and L.S. and G.G. received consultancy fees from Croma-Pharma. For the remaining authors, no competing financial interest exists.