
Abstract
Abstract
Human T cell leukemia virus type 1, also known as human T lymphotropic virus type 1 (HTLV-1), is a retrovirus that encodes a reverse transcriptase, which translates viral RNA into a DNA provirus that is integrated into the host genome. The virus was found to be a causative agent of adult T cell leukemia/lymphoma (ATL) in the early 1980s, and was also found to cause the neurological disorder tropical spastic paraparesis (TSP)/HTLV-1-associated myelopathy (HAM) and the inflammatory disorder HTLV-1 uveitis in the mid 1980s and early 1990s, respectively. This article reviews eye diseases caused by or related to HTLV-1: HTLV-1 uveitis, ocular and systemic complications of HTLV-1, keratoconjunctivitis sicca, interstitial keratitis, and ATL.
Introduction
H
After HTLV-1 was recognized to cause ATL,3–5 HLTV-1 was also found to cause a neurological disorder, tropical spastic paraparesis 9 (TSP)/HTLV-1-associated myelopathy (HAM), 10 in the mid-1980s and an intraocular inflammatory disease, HTLV-1 uveitis, in the early 1990s.11–14
This article reviews eye diseases caused by or related to HTLV-1: HTLV-1 uveitis, ocular and systemic complications of HTLV-1, keratoconjunctivitis sicca (KCS), interstitial keratitis, and ATL. In addition, this article includes long-term complications and prognosis of HTLV-1 uveitis.
Eye Diseases in HTLV-1 Infection
Since HTLV-1 was recognized to cause uveitis, many other eye diseases have been associated with HTLV-1 infection. These diseases can be classified into 4 groups depending on the type of eye disease and the systemic condition of the patient: (1) uveitis in HTVL-1 asymptomatic carriers and in HAM/TSP patients (HTLV-1 uveitis),11–14 (2) KCS,15,16 (3) interstitial keratitis,17,18 and (4) malignant cell infiltration/opportunistic infection in ATL patients.19–22
HTLV-1 uveitis
History of HTLV-1 uveitis
Several case reports23–26 described uveitis in HAM patients and/or in HTLV-1 asymptomatic carriers from an HTLV-1 endemic area, Kyushu Island of Japan. These reports suggested a possible relationship between HTLV-1 infection and uveitis. Therefore, we performed a clinical survey of uveitis in 3 cities located in different regions of Japan: Miyakonojo, which is located at southern Kyushu Island, where HTLV-1 is highly endemic; Kurume, which is located in northern Kyushu Island, where HLTV-1 is less endemic; and Tokyo, where HTLV-1 is not endemic. The clinical survey revealed that the proportion of etiology-unknown uveitis (idiopathic uveitis) is extremely high in Miyakonojo compared with the other 2 cities (Table 1) (Mochizuki M, Ikeda E, Hikita N, et al., 1991; Unpublished data). This observation led us to hypothesize that HTLV-1 infection might be etiologically related to the high proportion of etiology-unknown uveitis in Miyakonojo. To prove this hypothesis, we conducted 3 sets of studies: seroepidemiological surveys, 12 clinical assessments, 14 and molecular and immunological investigations. 13
The first clue was obtained by a seroepidemiological survey conducted in an HTLV-1 endemic region (Miyakonojo) and in a less endemic region (Kurume). 12 In the HTLV-1 endemic region, the seroprevalence of HTLV-1 in idiopathic uveitis was significantly higher than that in 2 control groups, uveitis with defined etiologies (Behcet disease, sarcoidosis, and others) and nonuveitis ocular diseases (cataract, glaucoma, and others). A similar observation was found in the HTLV-1 less endemic region. The risk factor (odds ratio) of idiopathic uveitis for HTLV-1 infection was estimated at 11.0 in the HTLV-1 endemic region and 7.8 in the HTLV-1 less endemic region. 12
The second clue was provided by clinical assessments identifying clinical features of idiopathic uveitis in HTLV-1 seropositive patients. 14 HTLV-1 seropositive patients with etiology-unknown uveitis had common ocular manifestations: intermediate uveitis with or without mild iritis and mild retinal vasculitis, but no or minimal involvement of retinitis or choroiditis.14,27 When the clinical features of idiopathic uveitis were compared between HTLV-1 seropositive patients and seronegative patients, intermediate uveitis was significantly higher in seropositive patients than in seronegative patients. 27
The third clue was provided by molecular and immunological analyses that revealed: (1) the detection of HTLV-1 provirus DNA by reverse transcriptase polymerase chain reaction (PCR) from the ocular infiltrating cells of HTLV-1 seropositive patients with uveitis13,28; (2) the detection of HTLV-1 mRNA, HTLV-1-related protein expression, and viral particles of 102-nm diameter on T cell clones derived from ocular infiltrating cells of the uveitis patients 29 ; (3) a significantly higher HTLV-1 provirus load in the peripheral blood mononuclear cells (PBMC) in HTLV-1 uveitis patients than in HTLV-1 asymptomatic carriers without uveitis, but lower than in HAM/TSP patients 30 ; (4) a significant correlation between provirus load in PBMC and clinical activity of uveitis in terms of vitreous inflammatory intensity and interval of uveitis recurrence 31 ; (5) a higher provirus load of HTLV-1 in the eye than in PBMC of the HTLV-1 seropositive patients with uveitis, indicating a significant accumulation of HTLV-1-infected cells in the eye 28 ; and (6) the polyclonal usage of T cell receptors by the intraocular infiltrating cells of the patients, indicating that the ocular infiltrating cells are not ATL malignant cells, but rather inflammatory cells. 32
These 3 lines of evidence strongly implicate that HTLV-1 is a causative agent of uveitis. Since then, uveitis in HTLV-1 asymptomatic carriers and in HAM/TSP patients has been recognized as a distinct clinical entity caused by HTLV-1, and the disease is now designated as HTLV-1 uveitis33,34 or HTLV-1-associated uveitis. 35
Immunopathology of HTLV-1 uveitis has been extensively investigated by using ocular-infiltrating cells from patients. Although the mechanism by which HTLV-1-infected lymphocytes get into the immune-privileged site of the eye remains to be determined, a significantly higher provirus load of HTLV-1 was found in the eye as compared with the PBCM, 28 indicating active accumulation of HTLV-1-infected cells in the eye. HTLV-1 activates CD4+ T lymphocytes 7 and stimulates lymphocytes to produce inflammatory cytokines.28,29 T cell clones derived from ocular-infiltrating cells 29 as well as primary ocular-infiltrating cells of the patients 28 produced a large amount of inflammatory cytokines, such as interleukin 6 (IL-6). Coculturing HTLV-1-infected T cells with corticosteroids suppressed the production of IL-6 and other inflammatory cytokines by the HTLV-1-infected T cell clones. 29 In clinical situations, corticosteroids are an effective cure for the inflammation of HTLV-1 uveitis.14,33 Thus, HTLV-1 uveitis is considered to be caused by inflammatory cytokines produced by HTLV-1-infected lymphocytes that have infiltrated the eyes.
Patients with HTLV-1 uveitis experience some systemic complications: 17% of patients with HTLV-1 uveitis or 25% of women with HTLV-1 uveitis had a previous history of Graves' disease. 36 The mechanisms by which HTLV-1 uveitis occur in patients with Graves' disease is unknown, but presumably thyroid hormone or medication used to treat Graves' disease may play a significant role. Only a few patients with HTLV-1 uveitis develop HAM/TSP,23,25 but no literature has reported that ATL develops in patients with HTLV-1 uveitis during their clinical course at present. Our long-term observation of HTLV-1 uveitis patients will be discussed in more detail in the following section.
Prevalence rates of HTLV-1 uveitis per 100,000 HTLV-1 carriers are estimated to be 58.6 in men, 152.0 in women, and 112.2 in both sexes. 37 The prevalence rates of HTLV-1 uveitis are slightly higher than those of HAM/TSP (35.7 in men, 86.9 in women, and 77.6 in both sexes). 38
Long-term follow-up of HTLV-1 uveitis
After the establishment of HTLV-1 uveitis as a disease entity, clinical surveys of uveitis were conducted at Miyata Eye Hospital in Miyakonojo, an HTLV-1 endemic region of southern Kyushu Island. HTLV-1 uveitis was the leading clinical entity of uveitis in the past 2 surveys: 17.8% of 1,008 uveitis patients reported in 200039 and 17.1% of 1,338 uveitis patients reported in 2009. 40
To determine if clinical features of HTLV-1 uveitis have changed in recent years, we conducted a new survey at Miyata Eye Hospital (Terada Y, Komizo T, Mochizuki M., 2016; Unpublished data). This was a retrospective chart review study performed in accordance with the Declaration of Helsinki. All procedures were approved by the Institutional Review Board of Miyata Eye Hospital. Clinical charts of consecutive patients with uveitis at Miyata Eye Hospital between 2010 and 2014 were retrospectively reviewed. A total of 949 patients with uveitis (586 women and 363 men) were enrolled in this survey. HTLV-1 uveitis was the leading clinical entity of uveitis, accounting for 14.2% of uveitis cases (135/949) (Table 2), which is similar to the findings of the past 2 surveys.39,40 The follow-up period of the HTLV-1 patients was 10.8 ± 7.9 years (mean ± SD). Using the 135 patients, clinical features of HTLV-1 uveitis were analyzed.
(1) Age and sex: The distributions of age of uveitis onset and sex of 135 patients with HTLV-1 uveitis are illustrated in Fig. 1. Women greatly outnumbered men in the patient group (women/men: 105/30 = 3.5). The peak age at uveitis onset was in the 50 s followed by in the 60 s for women and in the 60 s followed by in the 70 s for men. These findings are in agreement with a previous study 39 of 112 HTLV-1 uveitis patients.

Age at onset and gender of 135 patients with HTLV-1 uveitis. Open column: male patients. Closed column: female patients. HTLV-1, human T lymphotropic virus type 1.
Symptoms: The chief symptoms reported by patients at the initial presentation were foggy vision in 65.2%, ocular floaters in 43.7%, blurring of vision in 43.7%, ocular hyperemia in 8.1%, ocular pain in 2.2%, and photophobia in 0.7%.
(2) Laterality of affected eye: Throughout the follow-up period, unilateral involvement was seen in 72 patients (53.3%), whereas bilateral involvement occurred in 63 patients (46.7%).
(3) Type of uveitis: The type of uveitis was determined in each patient based on the major site of intraocular inflammation. The most common type was panuveitis (67 patients, 49.6%) characterized by moderate to severe vitreous opacities and mild anterior uveitis and retinal vasculitis. The second most common type was intermediate uveitis (39 patients, 28.9%) with vitreous opacities, but without anterior uveitis or retinal vasculitis, followed by anterior uveitis in 28 patients (20.7%), and posterior uveitis in 1 patient (0.7%).
The vitreous opacities were characterized by fine cells and lacework-like membranous opacities (Fig. 2, left). Anterior uveitis was characterized by small cells in the anterior chamber with or without fine keratic precipitates. Retinal vasculitis was identified as vasodilation of the retinal vessels visualized by ophthalmoscopy and as dye leakage demonstrated by fluorescein angiography (Fig. 2, right).
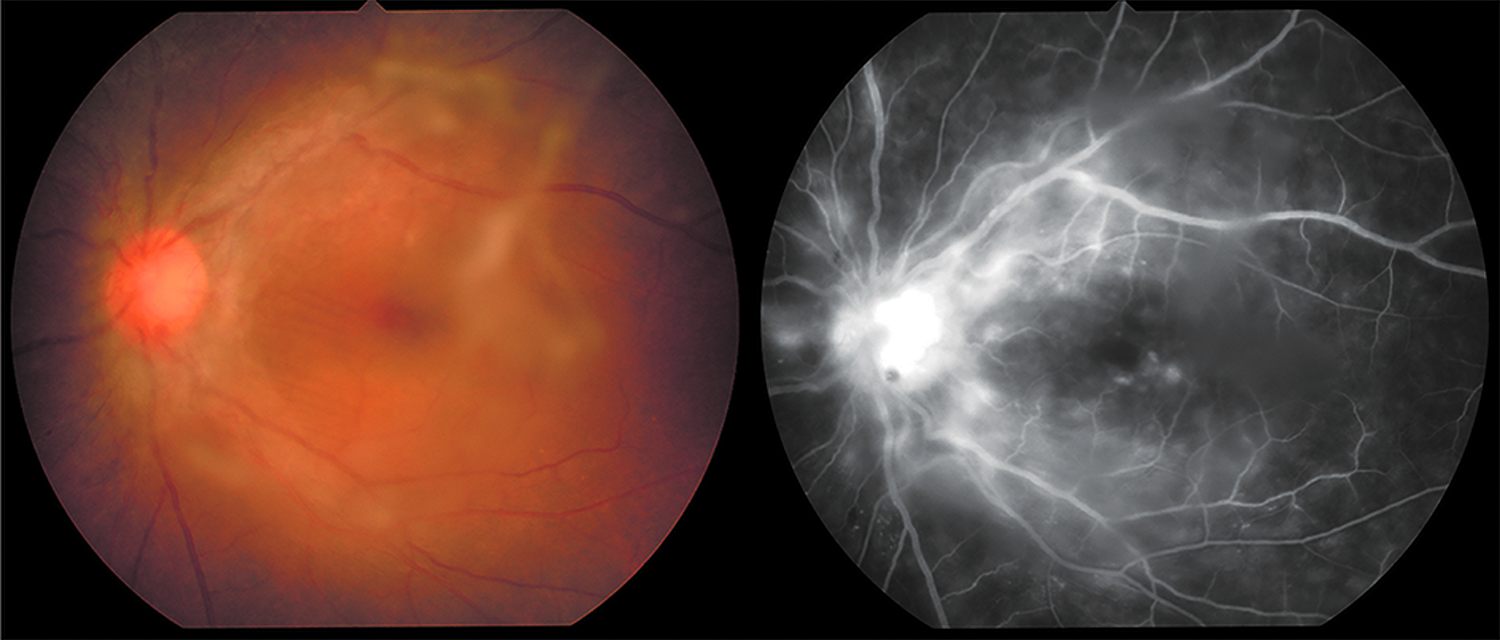
Color funds picture and fluorescein angiography of a 54-year-old woman with HTLV-1 uveitis. She was otherwise healthy HTLV-1 carrier: serum anti-HTLV-1 antibody was x4096 by the particle agglutination assay. Left: a color fundus picture of the left eye 1 week after the onset of ocular floaters, showing vitreous opacities and mild vasodilation of retinal vessels. Right: early phase of the fluorescein angiography of the same eye, showing moderate fluorescein dye leakages from the retinal blood vessels indicating retinal vasculitis. The best corrected visual acuity of the eye was 0.7 and recovered to 1.5 by the therapy with topical and systemic corticosteroids for 6 weeks. The right eye had also uveitis similar to the left eye. HTLV-1, human T lymphotropic virus type 1.
(4) Recurrence of uveitis: Ninety-five patients (70.3%) had only a single episode of uveitis with no recurrence during the follow-up period. The remaining 40 patients (29.6%) experienced recurrence: 2 episodes in 26 patients, 3 episodes in 7 patients, 4 episodes in 6 patients, and 5 episodes in 1 patient.
(5) Ocular complications: Cataract was the most common ocular complication (111 patients, 82.2%), followed by glaucoma in 38 patients (28.1%), including steroid-induced glaucoma in 11 patients (8.1%); cystoid macular edema in 7 patients (5.2%); and epiretinal membrane in 5 patients (3.7%). Cataract surgery was performed in 47 patients (34.8%), and glaucoma surgery (trabeculectomy with mitomycin) was performed in 3 patients (2.2%).
KCS, as determined by the criteria of a tear film breakup time shorter than 10 s together with dry eye symptoms, occurred in 29 patients (21.5%).
Corneal endothelial cell loss, as determined by the criteria of <2,000 cells/mm2 or a 10% decrease compared with the fellow eye, was seen in 4 patients among 52 patients (7.7%) whose corneal endothelial cell density was measured before cataract surgery. Another 3 patients (3.3%) developed bullous keratopathy without any events that might cause corneal endothelial cell damage, such as intraocular surgery or trauma. Taken together, a total of 7 patients (5.2%) had corneal endothelial cell damage. It is not known if the corneal endothelial cell damage in HTLV-1 uveitis patients is significant or not, and this point remains to be clarified.
(6) Therapy: At the time of ocular inflammation, topical or systemic corticosteroid was given to the patients. All HTLV-1 uveitis patients were treated with corticosteroid eyedrops; 13 patients (9.6%) were treated with sub-Tenon injections of triamcinolone acetonide; 45 patients (33.3%) were treated with oral prednisolone (initial dose of 20–30 mg/day, tapered off in 1–2 months); and 2 patients (1.5%) were treated with steroid pulse therapy.
(7) Visual prognosis: The best corrected visual acuity (BCVA) in affected eyes at the onset of HTLV-1 uveitis and at 3, 5, and 10 years after the onset is shown in Fig. 3. The BCVA at onset improved by the treatments with corticosteroids, and the vision at 1 year was significantly better than that at the uveitis onset. The BCVA at 10 years after the uveitis onset was slightly lower than the first year, although there was no significant difference. The BCVA at the 10th year after onset had a large deviation due to various factors, such as the development of cataracts and other ocular complications related to uveitis and/or aging.

Visual prognosis of HTLV-1 uveitis. The figure shows the mean and standard deviation of best corrected visual acuity at the onset of HTLV-1 uveitis (199 eyes), at 1 year (178 eyes), 3 years (122 eyes), 5 years (99 eyes), and 10 years (74 eyes) after uveitis onset. *P < 0.00001. HTLV-1, human T lymphotropic virus type 1.
The majority of patients had good visual prognosis. However, 7 patients (5.2%) had poor vision worse than 0.1 (logMAR = 1.0) at the last presentation. The causes of poor vision were cataracts in 1 patient, glaucoma in 3 patients, and bullous keratopathy in 3 patients.
(8) Systemic complications: Twenty-three patients with HTLV-1 uveitis (17.0%) had dysthyroidism; 21 patients developed hyperthyroidism before the onset of uveitis, and 2 patients were diagnosed with hyperthyroidism at the onset of uveitis. Sixteen patients (11.9%) were treated with methimazole before the onset of uveitis.
An association with HAM/TSP was seen in 6 patients with HTLV-1 uveitis (4.4%); 2 patients developed HAM/TSP before the onset of uveitis, and 4 patients developed HAM/TSP after the onset of HTLV-1 uveitis.
An association with ATL was seen in 3 patients (2.2%). One patient developed chronic ATL during the follow-up period of HTLV-1 uveitis, and 2 patients were diagnosed with smoldering ATL by systemic investigations when HTLV-1 uveitis was diagnosed. In the other 132 patients (97.8%), ATL was not associated with HTLV-1 uveitis during the follow-up period.
Other systemic complications in the 135 patients with HTLV-1 uveitis were rheumatoid arthritis in 5 patients (3.7%), interstitial pneumonia in 3 patients (2.2%), and Sjogren's syndrome in 3 patients (2.2%).
Keratoconjunctivitis sicca
KCS is a chronic, bilateral discomfort of the conjunctiva and cornea due to insufficient and poor-quality tears with a tear breakup time of shorter than 10 s. A previous study conducted in San Paulo reported that the prevalence of decreased tear breakup time was significantly higher in HTLV-1 carrier blood donors than in age- and sex-matched noncarrier blood donors. 41 Sjogren's syndrome is one of the representative systemic diseases that cause KCS. An association between Sjogren's syndrome and HTLV-1 infection has been reported in several studies.15,16,42 In an HTLV-1 endemic area, the prevalence of Sjogren's syndrome was significantly higher in HTLV-1 carriers than in the noninfected control group. 43 An animal study confirmed that tear film alternation that was clinically similar to Sjogren's syndrome was seen in HTLV-1 Tax gene-expressing transgenic mice. 44
The developmental mechanism of KCS in HTLV-1 carriers might differ from typical ocular mechanism in Sjogren's syndrome, because the immunological alteration is not caused by autoimmunity, but rather by HTLV-1 infection.42,45,46 Some patients have >1 HTLV-1-associated inflammatory condition, which is referred to as overlap syndrome. HTLV-1 infection can change the immunological status by T cell activation and cytokine secretion, which may contribute to the development of the overlap syndrome. HTLV-1-infected activated T cells derived from eyes of HTLV-1 uveitis patients secrete a variety of cytokines, including IL-1, IL-2, IL-3, IL-6, TNF-α, and IFN-γ.47–49 The HTLV-1-infected cells are believed to behave the same way in other organs, such as the lacrimal gland that are infiltrated by infected cells.
Transgenic mice expressing HTLV-1 Tax develop an inflammatory arthropathy, 48 and transgenic rats expressing HTLV-1 env-pX develop Sjogren's syndrome, arthropathy, vasculitis, and polymyositis. 50 Regulatory T cells in HTLV-1 bZIP factor transgenic mice are functionally impaired. 51 These observations imply that HTLV-1-induced regulatory T cell dysfunction may be one of the mechanisms that induce immune activation by HTLV-1-infected cells. As shown by our current data, the association between KCS and HTLV-1 uveitis can be explained in part by the mechanism of overlap syndrome.
As for treatments, the ocular surface lubricating is very important for patients with a tear disorder. Lubricating drops are selected to reduce tear film disorders and to prevent the ocular surface from developing superficial punctate keratitis and corneal ulcers. 52
Interstitial keratitis
Chronic interstitial keratitis related to HTLV-1 infection was identified by a series of reports in the early 2000s.17,18 Patients with keratitis have no subjective symptoms, such as pain or visual loss, but round or patchy whitish opacities confined bilaterally to the anterior stroma are observed in the cornea. The corneal lesions are located at the periphery of the cornea and spare the visual axis without ulceration or neovascularization. Keratitis was reported in 10% of HTLV-1-infected patients 18 and was strongly associated with HAM/TSP, of which the HTLV-1 provirus load in PBMC was very high compared with other HTLV-1-related diseases. 53 This observation may imply that high provirus HTLV-1 load contributes to the pathogenesis of the keratitis. On the other hand, one-third of the patients have histories of HTLV-1 uveitis, 45 of which HTLV-1 provirus load in PBMC is not that high. 53
As for treatments, the topical administration of corticosteroids did not elicit a response, and the corneal lesions remained chronic. Therefore, further investigation is needed to identify the mechanism of the keratitis so that treatments can be developed.
Adult T cell leukemia/lymphoma
HTLV-1 causes ATL, an extremely rare form of leukemia with a high fatality rate. According to a recent survey in Japan, infiltration of ATL cells to the eye and ocular opportunistic infection are common among ATL patients. 49
As for ocular infiltration of ATL cells, previous case reports revealed that ATL cells have the potential to infiltrate almost all ocular tissues, such as the orbit, conjunctiva, cornea, iris, lens, vitreous, choroid, retina, sclera, and optic nerve.20,21
As ATL is one of the most aggressive types of leukemia, opportunistic infections are seen even in patients who do not undergo chemotherapy or allogeneic hematopoietic stem cell transplantation. 54 In the eye, the most common opportunistic infection is cytomegalovirus retinitis.22,47
Distinguishing leukemic infiltrates from an opportunistic infection is important in clinical practice. Recent developments in molecular biology technologies, such as PCR and flow cytometry, have enabled the rapid and accurate diagnosis of pathogenic microorganisms of infectious diseases. Screening with multiplex PCR/broad-range PCR is useful to rule out opportunistic infections such as viral, bacterial, and fungal infections.55–58 In addition, detection of HTLV-1 provirus DNA and monoclonal T cell receptor γ chain gene rearrangement by PCR can confirm ATL infiltration. 20 Further investigation with flow cytometry can detect the expression of ATL-specific surface molecules, which is also helpful for the diagnosis of ATL. ATL cells are characterized by the expression of IL-2 receptor alpha (IL-2Rα) (CD25), which is not expressed in normal resting T cells. Detection of elevated levels of soluble IL-2Rα may suggest direct ocular infiltration of ATL cells, as ATL cells secrete soluble forms of IL-2Rα. 21
Intensive chemotherapy and allogeneic hematopoietic stem cell transplantation are currently chosen as therapies for ATL patients, but these treatments are not sufficient to improve the prognosis of ATL patients. Clinical trials with new agents for ATL are ongoing, including a defucosylated humanized anti-CC chemokine receptor 4 monoclonal antibody. 54
Conclusions
HTLV-1 is a human retrovirus that encodes a reverse transcriptase, which translates the viral RNA into a DNA provirus and is integrated into the host genome. When monoclonal expansion takes place in CD4+ T lymphocytes, malignant transformation is believed to take place in HTLV-1-infected T cells, that is, ATL. If polyclonal expansion occurs, the infected T cells are assumed to be activated and produce a large number of cytokines that induce inflammatory disorders in many organs, including the eye. Knowledge of eye diseases caused by or related to HTLV-1, that is, HTLV-1 uveitis in HTLV-1 carriers or HAM/TSP patients, KCS in HTLV-1 carriers, interstitial keratitis in HTLV-1 carriers and HAM/TSP patients, and malignant cell infiltration/opportunistic infection in ATL patients, will be useful in clinical practice for ophthalmologists not only in HTLV-1 endemic regions of the globe but also in nonendemic regions.
Clinical features and pathogenic mechanisms of HTLV-1-related eye diseases have been clarified as reviewed in this article. However, several issues remain to be answered in future studies. Although previous studies have determined that HTLV-1-infected activated T cells accumulate in the eye and produce a large amount of inflammatory cytokines resulting in ocular inflammation, the mechanism by which the HTLV-1-infected T cells get through the blood–ocular barrier and accumulate in the eye is unknown. To answer this question, an animal model for HTLV-1 uveitis will be useful; however, despite many efforts, it has not been established. The association between HTLV-1 infection and ocular surface/corneal diseases, such as KCS, interstitial keratitis, and corneal endothelial cell damage, should be studied with more patients to collect more evidence. Another important question is: what are the long-term systemic complications of HTLV-1 uveitis? Although previous studies demonstrated that Graves' disease and HAM/TSP are associated with HTLV-1 uveitis, it is not clear if patients with HTLV-1 uveitis develop ATL, a life-threatening malignant disorder, during the long-term clinical course. In our series, a couple of patients with HTLV-1 uveitis developed ATL during the long-term follow-up, but this question should be clarified by future studies with more patients and longer follow-up periods.
Footnotes
Author Disclosure Statement
No competing financial interests exist.