
Abstract
Abstract
Purpose:
To determine the changes in the anterior chamber flare and central macular thickness (CMT) under topical antiglaucomatous therapy.
Methods:
This study included 121 eyes of 73 patients and 36 eyes of 18 controls. Glaucoma patients were divided into 3 groups (timolol maleate, latanoprost, and bimatoprost). Control eyes did not receive any medications. Flare and CMT measurements were performed at baseline and follow-up visits (15th day, and 1st, 3rd, 6th, and 12th month).
Results:
Statistically significant increases were detected in the flare values in the bimatoprost and latanoprost groups (P < 0.001, P = 0.011, respectively). Significant increases were also found in CMT values measured in these 2 groups (P < 0.001, P = 0.002, respectively). However, increased flare and CMT values were not clinically manifested as uveitis and macular edema. Flare and CMT values did not change statistically in the timolol maleate and control groups.
Conclusions:
Although the use of prostaglandin (PG) analogs was found to be associated with increased flare and CMT, these increases were not clinically significant. PG analog monotherapy may be safely and effectively used in the treatment of glaucoma.
Introduction
M
Among the antiglaucomatous drugs used in the ophthalmology practice, prostaglandin (PG) analogs are commonly preferred ones due to their efficacy, the ease of use as a result of once-daily dosing. This group of drugs is also effective in the control of daily fluctuation of IOP. 1
PGs are known to be chemical mediators that play a role in the inflammatory process. In case of a damage or dysfunction of blood–aqueous barrier, PG analogs may cause intraocular inflammation 2 and anterior chamber flare increase. 3 Inflammatory mechanism includes the induction of PGE-2 secretion by PGF-2 alpha and subsequent activation of phospholipase II and arachidonic acid release. Arachidonic acids cause inflammation by increasing the amount of eicosanoids that are proinflammatory for the eye. Furthermore, they diminish the integrity of the blood–aqueous and blood–retina barriers. Consequently, cystoid macular edema (CME) and increased flare values in the anterior chamber may be observed. 4
In a number of studies, PG analogs have been shown to cause CME, uveitis, and herpetic keratitis activation in aphakic and pseudophakic eyes.5,6 Risk factors for developing CME during topical PG treatment include history of aphakia, pseudophakia, and CME.7–10 Although in certain studies it has been shown that PGs did not cause any increase in the flare values in humans, a possible association has been shown between increased aqueous humor flare and PG analog use in rabbits.11,12
This study aimed at prospectively observing the changes in the anterior chamber flare and central macular thickness (CMT) measurements in patients treated with topical PG analogs and timolol maleate.
Methods
Study design and patient population
In the study, 121 eyes of 73 patients attending the Glaucoma Unit of the Department of Ophthalmology of the Medical School of Ankara University and 36 eyes of 18 patients attending the outpatient clinic for a routine visit between November 2011 and June 2013 were included. Patients had no previous history of antiglaucomatous agent use. The newly diagnosed glaucoma patients were divided into 3 different treatment groups, including timolol maleate 0.5% (Timoptic®), latanoprost 0.005% (Xalatan®), and bimatoprost 0.03% (Lumigan®). In all patients, glaucoma diagnosis was given by the same glaucoma specialist (O.T.) on the basis of a raised IOP together with glaucomatous optic nerve head and/or visual field changes. Visual field evaluation was performed with Humphrey automated perimetry in both glaucoma patients and healthy controls.
After the study procedures were explained to the participants fully, written informed consents were obtained. The study was conducted in line with the Declaration of Helsinki. The approval of the Ethics Committee of Ankara University was obtained before the initiation of the study.
Inclusion criteria for glaucoma patients were as follows:
1. Open anterior chamber angle and a normal structure in gonioscopic examination (grade 3, 4 in Schaffer classification). 2. Patients aged 18 years and older. 3. No history of any intraocular surgery or laser surgery.
Exclusion criteria for glaucoma patients were as follows:
1. Closed-angle glaucoma. 2. Presence of diabetic retinopathy, senile macular degeneration, central serous retinopathy, and similar retina diseases that may affect the CMT. 3. Diseases that may affect flare meter measurements such as uveitis, corneal opacity, corneal edema, and mature cataract. 4. Previous use of any antiglaucomatous agent. 5. Hypersensitivity to the topical agent or presence of a systemic disease that may interfere with the use of the agent. 6. Active eye infection or inflammation. 7. Wearing contact lens or severe dry eye syndrome. 8. Inability to carry out the measurements with the Goldmann applanation tonometer.
Additional inclusion criteria for the controls were as follows:
1. IOP values below 21 mm Hg as measured by the Goldmann applanation tonometer. 2. Absence of any eye disease that may affect measured parameters. 3. Absence of pseudoexfoliation (PEX) 4. No current use of any eye drop medication. 5. No history of any intraocular surgery or laser surgery.
Ophthalmological evaluation
The baseline examination included best-corrected visual acuity measurements, examination of the anterior segment, gonioscopy, fundoscopy, and IOP measured by the Goldmann applanation tonometer.
Aqueous flare measurements
All patients underwent flare measurements with a Laser Flare Cell Meter (Kowa FC 600; Acculas, San Jose, CA) at all visits. [Flare values were measured at 45 min after dilatation of the pupil with 0.5% tropicamid. At least 7 measurements per patient were taken, and the highest and lowest values were discarded for averaging. The machine automatically calculated the mean and standard deviation (SD) of the remaining 5 flare readings.]
CMT measurements
CMT was measured [macular cube 512 × 128, a computer algorithm was used to profile the inner and outer retinal boundaries, and the retinal thickness was computed automatically from these boundaries. CMT was analyzed by optical coherence tomography (OCT) software] by Cirrus OCT (software; Carl Zeiss Meditec, Inc. Dublin, CA).
Follow-up period
All patients were seen at baseline visit and were called for follow-up visits on the 15th day, and at months 1, 3, 6, and 12. CMT measured by OCT and flare measured by flare meter were noted in baseline and each follow-up visit. All measurements were performed by the same investigator (F.S.). Patients with progressive glaucomatous damage despite the treatment or patients who required additional treatment due to uncontrolled IOP were excluded from the study in the follow-up visits.
Statistical analysis
All data were analyzed using Statistical package for social science 15, statistical software. The Shapiro–Wilk test was used to analyze the normality of the measurement data distribution. Descriptive statistics for continuous measurable variables were shown as mean ± SD. The statistical significance of the intergroup differences was assessed by Kruskal–Wallis variance analysis. In case of a significant difference, a Bonferroni-corrected Mann–Whitney U test was used to determine the group from which difference originated. The results were evaluated within a 95% confidence interval and a P value of <0.05 was considered significant.
Results
While a total of 91 subjects were assessed in this study, 18 of the participants were normal. Thirty-six eyes of 18 controls were included in this study and 121 eyes of 73 glaucoma patients were divided into 3 groups. No significant differences were found in gender, age, and follow-up duration between the groups (P > 0.05).
Data on groups regarding gender, age, the mean follow-up duration, and number of eyes and laterality are given in Table 1. The best-corrected visual acuity of all subjects was 20/20 and no change was observed throughout the follow-up period.
n, number of the cases; SD, standard deviation.
In the assessment of the groups in term of PEX, while PEX was not detected in any of the subjects in the control group, 9 eyes of PEX glaucoma (20.9%) and 34 eyes of primary open angle glaucoma (POAG) (79.1%) were detected in the timolol maleate group, PEX glaucoma was detected in 12 eyes (32.4%) and POAG was detected in 25 eyes (67.6%) in the latanoprost group, and PEX glaucoma was detected in 18 eyes (43.9%) and POAG was detected in 23 eyes (56.1%) in the bimatoprost group. There was not statistical significant difference in the distribution of PEX glaucoma patients between treatment groups (P = 0.79).
As shown in Table 2, there were no significant changes in the mean flare value between baseline and last follow-up visit in the control and timolol maleate groups. However, in the latanoprost and bimatoprost group, there was a statistically significant increase in flare values (P = 0.011, P < 0.001, respectively). In the latanoprost group, significant difference occurred only at last visit, whereas in the bimatoprost group, the increase became statistically significant in comparison to the baseline beginning from the third month (P = 0.037). No statistically significant difference was detected in the intergroup comparisons of the baseline flare values (P > 0.05).
P value compared baseline and last month visit.
In the comparison of mean flare values of the last visit, statistically significant differences were found between the control and bimatoprost groups, between the control and latanoprost groups, between the timolol maleate and latanoprost groups, and between the timolol maleate and bimatoprost groups (P = 0.003, P = 0.004, P < 0.001, P < 0.001, respectively). Namely, in the last visit, the increases in the mean flare value were statistically significant in the latanoprost and bimatoprost users when compared to the other groups. The change in the mean flare values of groups was shown in Fig. 1 throughout each visit.
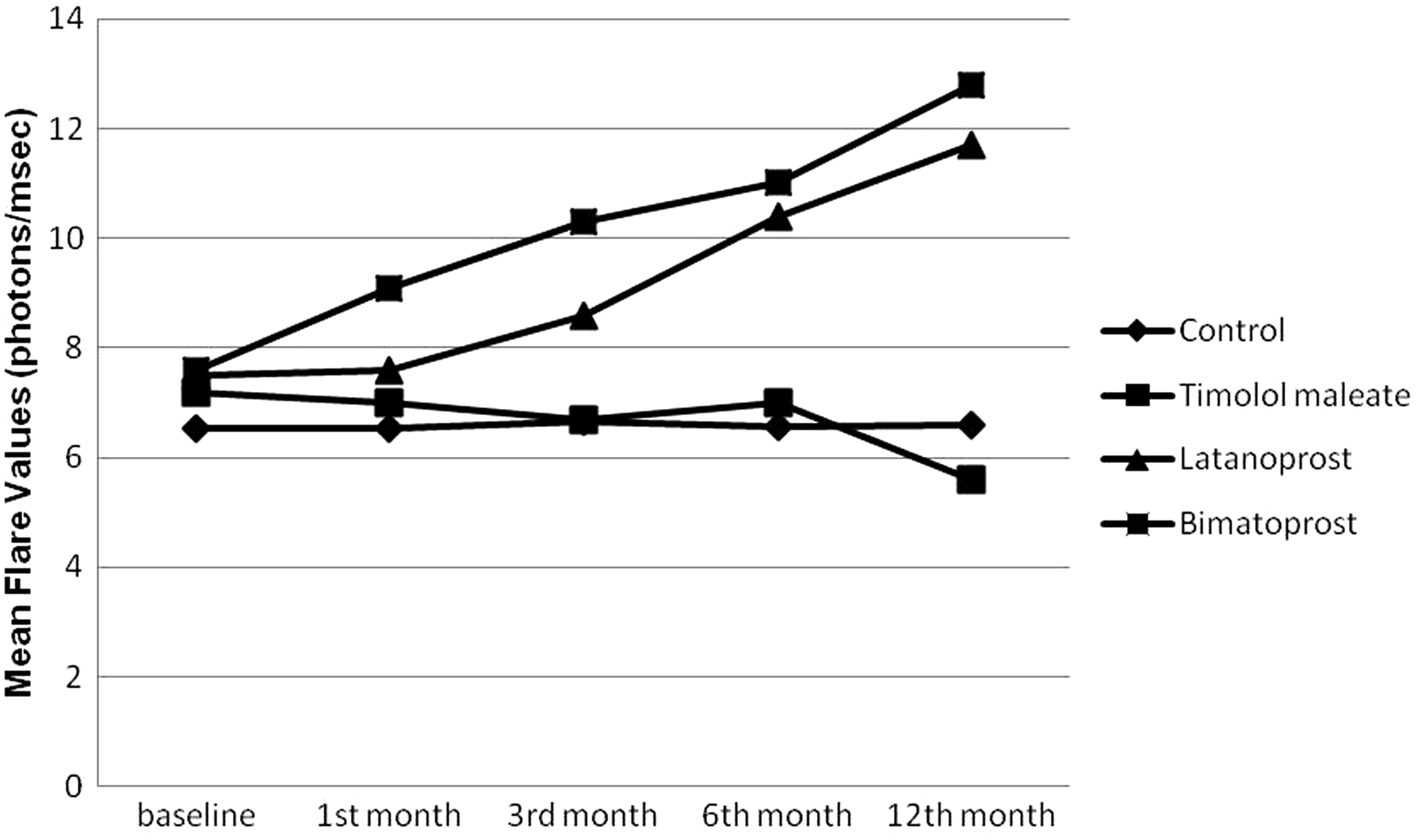
The change in the mean flare values of groups was shown throughout each visit.
As regarding CMT, no statistically significant change was observed during the follow-up period in the timolol maleate group and control group. However, in latanoprost and bimatoprost groups, the difference between the baseline and last visit values was statistically significant (P = 0.002 and P < 0.001, respectively) (Table 3). The CMT values revealed a slow increase during the follow-up period in the latanoprost and bimatoprost groups, and these increases were significant beginning from the sixth month in the latanoprost group (P = 0.006) and at the 12-month in the bimatoprost group (P < 0.001). The change in the mean CMT of latanoprost and bimatoprost groups was shown in Fig. 2 throughout each visit.
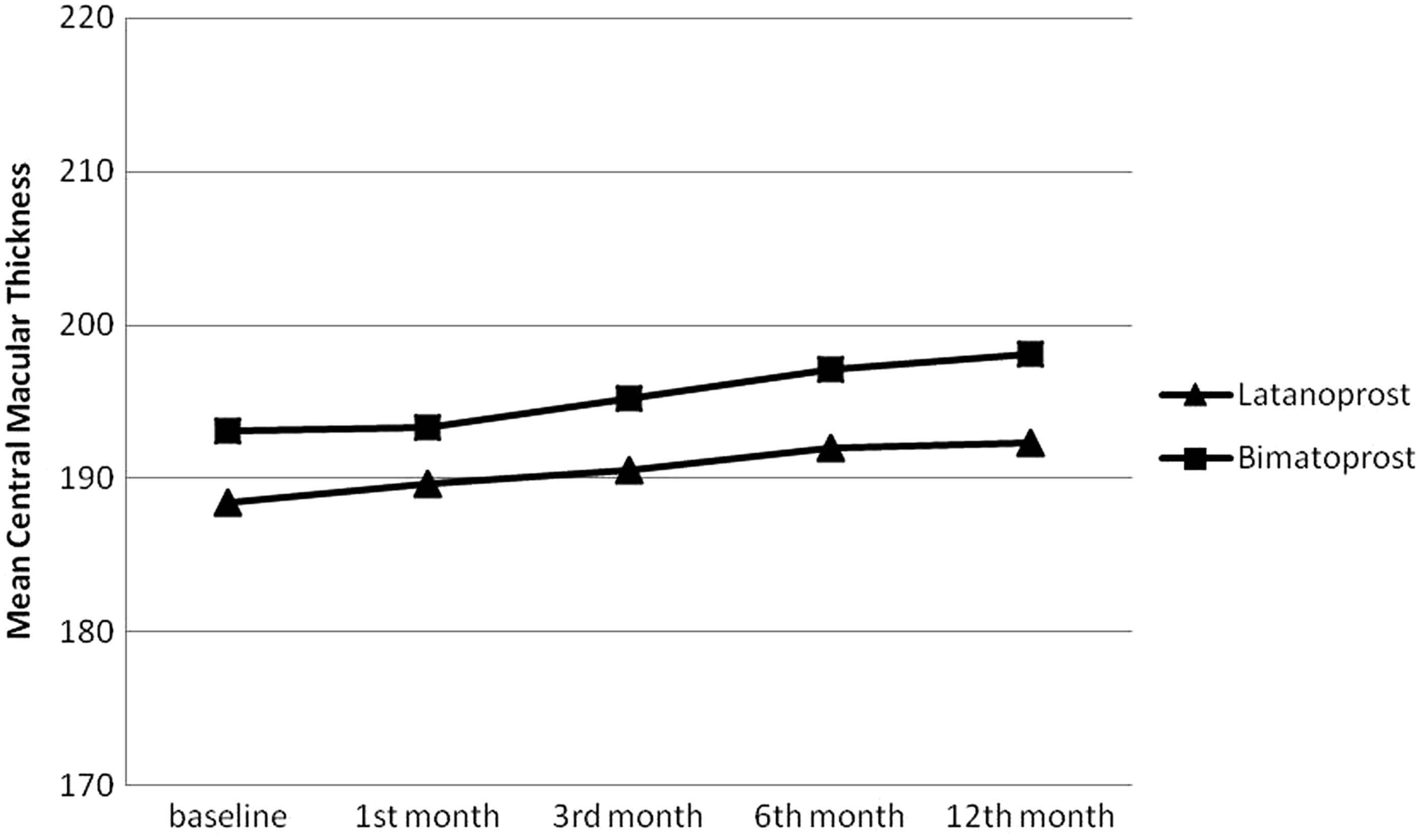
The change in the mean central macular thickness of prostaglandin groups was shown throughout each visit.
Discussion
PG analogs are a group of antiglaucomatous agents that are commonly used in the current practice due to their success in monotherapy, advantage of single daily dosing, rare systemic and ocular side effects, and unlikely negative impact on the quality of life. It has been reported that flare values might rise to 30 photon counts/ms in glaucoma patients who have been treated with a PG analog, however, these values may not be manifested as a clinical symptom in general. Actually, flare values measured by flare meter may be as high as 60 photon counts/ms after cataract surgery and 300 photon counts/ms in the cases of chronic and acute uveitis. 13 In many studies, latanoprost-related CME has been reported to be associated with certain risk factors such as a history of CME or anterior uveitis, epiretinal membrane, retinal vein occlusion, rupture of posterior capsule, aphakia, and diabetes mellitus.8,9,14–18
In a dose-ranging trial of latanoprost conducted by Linden et al., after 2 weeks of follow-up, photophobia, moderate intensity flare, and +1/+2 cells in the anterior chamber were reported in 15 out of 28 healthy subjects who used latanoprost 4 times a day. The investigators detected the association between the latanoprost overdose and transient moderate inflammation in the anterior chamber. 19 In a study conducted by Warwar et al., 163 eyes in 94 patients were treated with topical latanoprost and anterior uveitis was detected in 8 eyes (4.9%), while CME was detected in 2 eyes (1.2%) after 1 year of follow-up. 18 In a case presentation, it was reported that conjunctival hyperemia, anterior chamber flare, and cells were detected at the first week of once-daily treatment with bimatoprost in a 72-year-old female patient with PEX glaucoma. After bimatoprost treatment was discontinued, the inflammatory symptoms in the right eye resolved spontaneously without any medication within about 2 weeks. 20 In a study conducted by Chang et al., 163 high-IOP eyes were examined in 84 cases (27 unilateral, 57 bilateral cases) of uveitis. During a 3-month period of follow-up, while 1 eye of the patient was treated with a topical PG analog, the other was treated with a non-PG analog medication. At the end of follow-up, no deterioration in the uveitis was detected, while IOP was lowered. In a similar way, no case of treatment-related CME was detected. 6
Lima et al. retrospectively reviewed 225 aphakic or pseudophakic eyes treated with topical latanoprost. Of them, 44% had posterior capsule rupture during surgery and a worsening of 2 Snellen lines was detected in the visual acuity in 3 patients, as a result of CME. While 2 of them had undergone cataract surgery requiring anterior vitrectomy, 1 of them had developed CME before the glaucoma treatment. The authors indicated that if there was a cause-and-effect relationship between latanoprost therapy and clinically significant CME, the incidence appeared to be low. 8
Linden et al. followed up 26 patients on latanoprost for about 12 months. Laser flare photometry measurements did not reveal any change at the end of the 12th month. 21
A study conducted by Martin et al. compared 0.03% bimatoprost and 0.5% timolol maleate administered to 30 eyes of 30 patients. Intragroup and intergroup comparisons did not reveal any difference between the 2 groups or any finding in terms of anterior chamber flare and CME. 22
In a study conducted by Diestelhorst et al., 30 patients with POAG or PEX were divided into 3 groups and 1 dose of latanoprost 0.005% was administered to 1 of the group, while 2 doses of latanoprost 0.0015% were administered to the other group, and timolol was administered to the third group. A slight increase of anterior chamber flare was observed in all 3 groups, predominantly in the timolol group. However, none of these was statistically significant. 23 Similarly, treatment groups included both POAG and PEX glaucoma patients in this study and PEX glaucoma patients had similar distribution between treatment groups. Furuichi et al. performed CMT measurements using OCT in 68 patients on latanoprost who had no risk factor for CME. No case of CME was detected after 6 months of follow-up. 7
In this study, the increases in the flare values became prominent beginning from the third month in the bimatoprost group and from the 12th month in the latanoprost group. Although these increases are not clinically significant, we can say that the long-term use of PG analogs may affect the blood–aqueous barrier at a minimal level. Concerning CMT, despite the fact that our patients had no risk factors for CME, the CMT measurements were found to be increased in patients on latanoprost or bimatoprost. However, CME was not detected in any of the patients and neither were subretinal fluid or intraretinal cysts. In the patients on latanoprost or bimatoprost, the changes in the CMT values were significant beginning from the sixth month in the latanoprost group and at the 12th month in the bimatoprost group. The vision acuity of the patients did not change; therefore, the mild increase in the CMT values was not clinically significant.
Major limitation of this study is the benzalkonium chloride (BAK) presence in all the preparations. Stevens et al. evaluated 28 untreated patients with ocular hypertension. 24 Of these patients, 1 randomly selected eye received BAK-preserved timolol and the fellow eye received preservative-free timolol. Flare meter measurements were performed at baseline and after 1 month. Flare values were increased in both groups; however, the increase in BAK-preserved timolol-using eyes was statistically higher than preservative-free timolol-using eyes. In this study, the highest increase in flare values was observed in the bimatoprost group, which had the minimum BAK exposure (Timoptic 0.5%, 0.1 mg/mL BAK; Xalatan 0.005%, 0.2 mg/mL BAK; Lumigan 0.03%, 0.05 mg/mL BAK).
Another limitation of the study is the absence of the functional tests to evaluate the macular performance. Macular functional tests could be helpful to reveal whether clinically insignificant CMT changes caused any functional alteration.
In conclusion, in contrast to timolol maleate, PG analogs may cause a slight increase in the anterior chamber flare and in the CMT. However, this effect is not considered clinically significant. A larger patient population and longer follow-up period are required to obtain more accurate results. Considering all these results, PG analog monotherapy may be safely and effectively used in the treatment of glaucoma. However, their side effects should be taken into consideration in the follow-up of these patients.
Footnotes
Acknowledgments
All authors conceived the study, participated in its design and coordination, and revised the article critically for important intellectual content. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.