
Abstract
Abstract
Purpose:
To investigate the effect of a single intravitreal dexamethasone implant (IVT-DI; Ozurdex; Allergan, Inc.) on visual acuity, macular thickness, and intraocular pressure (IOP) in active noninfectious uveitis.
Methods:
Medical records of patients with noninfectious active uveitis treated by IVT-DIs were retrospectively reviewed. Uveitis etiologies, treatment indications, best corrected visual acuity (BCVA), central retinal thickness measured by ocular coherence tomography, IOP, and systemic, local, and topical treatments were collected. Parameters were analyzed before the injection of the implant, after 1.5 ± 0.8 months and 4.4 ± 0.9 months for the BCVA, after 2 ± 1.3 months and 4.6 ± 1.3 months for the ocular coherence tomography, and after 1.3 ± 0.7 months and 4.4 ± 1 months for the IOP.
Results:
We included 14 patients (20 eyes, 20 implant injections) with cystoid macular edema (78%), vasculitis (7%), choroiditis (7%), and vasculitis associated with choroiditis (7%). Before the injection, mean visual acuity was 0.4 ± 0.5 logMAR (logarithm of the minimum angle of resolution) that improved to 0.3 ± 0.5 logMAR (P = 0.0002) after 1.5 ± 0.8 months and to 0.3 ± 0.5 logMAR (P = 0.005) after 4.4 ± 0.9 months. A statistically significant decrease of macular thickness was observed both at 2 ± 1.3 months and at 4.6 ± 1.3 months after IVT-DI. Mean IOP was 16 ± 5 mmHg before injections, 18 ± 6 mmHg (P = 0.13) at 1.3 ± 0.7 months, and 15 ± 4 mmHg (P = 0.65) at 4.4 ± 1 months. By Kaplan–Meier analysis, we found that after 3.3 months, 17% of the eyes still present a BCVA amelioration ≥0.3 logMAR.
Conclusions:
In our patients with active noninfectious uveitis, injection of a first single dexamethasone implant was found to improve visual acuity and decrease macular thickness without significant increase of IOP, although the effect seems limited in time.
Introduction
U
A systemic treatment based on steroids and/or immunosuppressors can be classically proposed. 3 However, this approach exposes the patients to several side effects. A local approach, either subconjunctival or intravitreal, offers an interesting alternative. Intravitreal steroid administration has been widely studied in this context.4–8 Intravitreal corticosteroids have been demonstrated to induce cataract and sight-threatening glaucoma.4,6 In this regard, the safety profile of the intravitreal dexamethasone implant (IVT-DI) might be safer than the fluocinolone acetonide intravitreal implant. The eyes treated with fluocinolone acetonide implant may need more glaucoma medications, surgery or laser, and developed more cataract than the eyes treated with IVT-DI. However, eyes treated with DI may more likely need a second implant. 9
In this study, we are evaluating the effect of a single injection of IVT-DI for the treatment of active noninfectious uveitis.
Methods
We conducted a retrospective study including 14 patients with an active noninfectious uveitis not responsive to standard treatment with oral corticosteroids and/or immunosuppressive therapy (according to standard of care10–12 ). The dose of the systemic treatment was adapted according to the clinical response to the injection. Twenty IVT-DIs were injected into 20 eyes between March 2013 and November 2014. The study design adhered to the Declaration of Helsinki. The use of IVT-DI was approved by the patient and an institutional review board approval for the record review was obtained.
The IVT-DI (Ozurdex; Allergan, Inc., Irvine, CA) is a biodegradable, sustained-release implant of 0.7 mg of dexamethasone embedded in a solid polymer drug. 13 A study on monkeys demonstrates sustained levels of IVT-DI and biological activity for 6 months, with peak levels of drug for the first 2 months 14 . It is approved by the United States Food and Drug Administration for the treatment of macular edema secondary to retinal vein occlusion and noninfectious uveitis affecting the posterior segment of the eye.15–17
All patients had a previous systemic work-up with exclusion of systemic infection. Uveitis etiologies; treatment indications; visual acuity; slit lamp and fundus examination; central retinal thickness (CRT) measured by optical coherence tomography; intraocular pressure (IOP); and systemic, local, and topical treatments were collected. Parameters were analyzed before the injection of a first implant, after 1.5 ± 0.8 months and 4.4 ± 0.9 months for the best corrected visual acuity (BCVA), after 2 ± 1.3 months and 4.6 ± 1.3 months for the ocular coherence tomography (OCT), and after 1.3 ± 0.7 months and 4.4 ± 1 months for the IOP.
One eye had a vitrectomy with epiretinal membrane peeling between the first and the second follow-up. The data of this eye at the second follow-up were thus excluded from the BCVA and OCT analyses.
The primary end point was the evaluation of the BCVA evaluated by Snellen charts and converted to logarithm of the minimum angle of resolution (logMAR) units. The secondary end points were the measure of the IOP obtained by applanation and the evaluation of the CRT measured by SD-OCT (Optovue RTVue 100, Simovison and OCT Spectralis Plus by Heidelberg Engineering). Fifty-two of 60 measurements were performed on OCT Spectralis Plus. The 8 measurements performed on the Optovue RTVue100 were at baseline (5) and after 2 ± 1.3 months (3).
Statistical analysis
Continuous data are presented as mean ± standard deviation and categorical data as numbers or percentage. Changes in BCVA, CRT, and IOP are analyzed using an analysis of variance for repeated measurements with missing data at baseline before the injection, after 1.5 ± 0.8 months and 4.4 ± 0.9 months for the BCVA, after 2 ± 1.3 months and 4.6 ± 1.3 months for the OCT, and after 1.3 ± 0.7 months and 4.4 ± 1 months for the IOP.
The Kaplan–Meier estimate is used to evaluate (1) the cumulative probability of nonimprovement BCVA after a single IVT-DI and (2) the cumulative probability of recurrence of cystoid macular edema (CME) after IVT-DI.
The improvement in BCVA was defined as in the Standardization of Uveitis Nomenclature (SUN) guidelines as ≥0.3 logMAR unit change. 18 Recurrence of CME was defined as a CRT ≥20% from baseline as described in the MUST (Multicenter Uveitis Steroid Treatment) Trial Research Group. 19
A P value <0.05 was considered significant. Analyses were performed by a statistician with Statistix 9.0 (Analytical Sofware, Tallahassee, FL) and Medcalc 11.4 (Medcalc, Oostende, Belgium).
Results
The characteristics of 20 eyes of 14 patients are reported in Table 1. The mean age is 48 years and the majority are women (78%). The anatomical classification of uveitis according to the SUN classification 18 is mostly posterior (64%) but also panuveitis (29%) and intermediate uveitis (7%). There are 57% of unilateral uveitis. The etiologies are mostly idiopathic (71%); birdshot chorioretinitis (14%); presumed tuberculous-related uveitis (7%); and idiopathic retinitis, vasculitis, aneurysms, and neuroretinitis (7%).
F, female; M, male; U, unilateral; B, bilateral; IRVAN, idiopathic retinitis, vasculitis, aneurysms, and neuroretinitis; CME, cystoid macular edema.
The indication of treatment is CME associated with inflammatory signs in 78%, active vasculitis in 7%, active choroiditis in 7%, and active vasculitis plus choroiditis in 7%.
The mean BCVA at baseline (before injection) is 0.4 ± 0.5 logMAR, 0.3 ± 0.5 logMAR at 1.5 ± 0.8 months after the IVT-DI, and 0.3 ± 0.5 logMAR at 4.4 ± 0.9 months after the IVT-DI (Fig. 1).
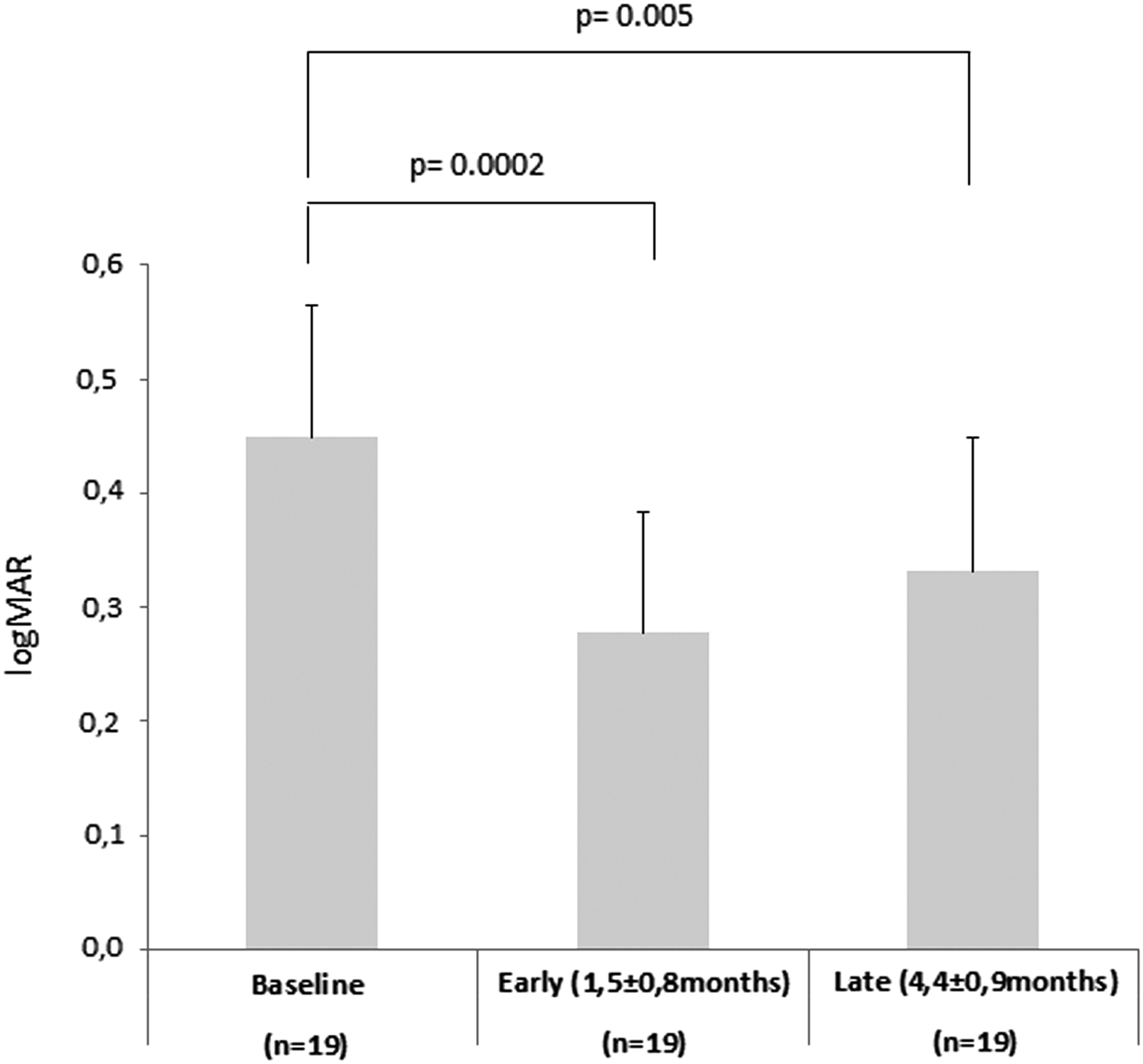
Mean initial BCVA in logMAR, at 1.5 ± 0.8 months and at 4.4 ± 0.9 months after IVT-DI. BCVA, best corrected visual acuity; IVT-DI, intravitreal dexamethasone implant.
The improvement of the BCVA between the baseline and 1.5 ± 0.8 months after IVT-DI and between the baseline and 4.4 ± 0.9 months after the IVT-DI is statistically significant (P < 0.05).
A significant decrease of the mean macular thickness measured by OCT in micrometers (Fig. 2) is observed after 2 ± 1.3 months (P = 0.0009) but also 4.6 ± 1.3 months after IVT-DI (P = 0.0232). Statistical analyses were also performed only with the eyes affected with CME at baseline and still showed a significant decrease of macular thickness. As mentioned in the Methods section, all measurements were not performed on the same OCT. However, it has been demonstrated that OCT Optovue RTVue both in normal and pathological edema underestimates the CRT as compared with Spectralis Plus OCT.20,21
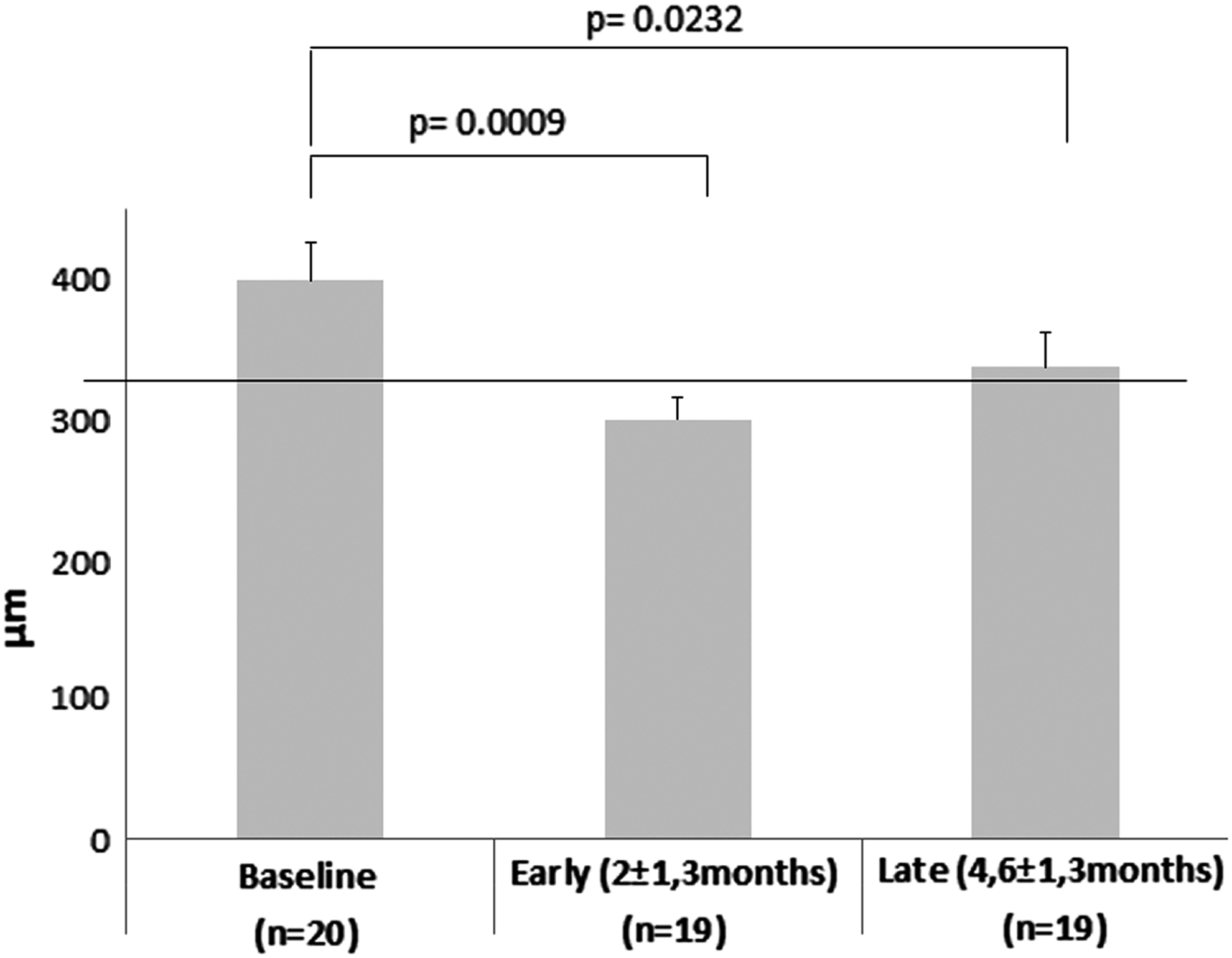
Mean initial macular thickness (μm), measured by OCT, at 2 ± 1.3 months and at 4.6 ± 1.3 months after IVT-DI. The horizontal marker corresponding to a 20% CRT reduction from baseline. CRT, central retinal thickness; OCT, ocular coherence tomography.
The Kaplan–Meier survival curve (Fig. 3) of the time to BCVA deterioration after 3.3 months of IVT-DI shows that 17% of the eyes still present a BCVA amelioration that is ≥0.3 logMAR. The Kaplan–Meier survival curve (Fig. 4) of the time to CME recurrence after 6 months of IVT-DI shows that 42% of the eyes present a CME recurrence defined as ≥20% of the baseline CRT.
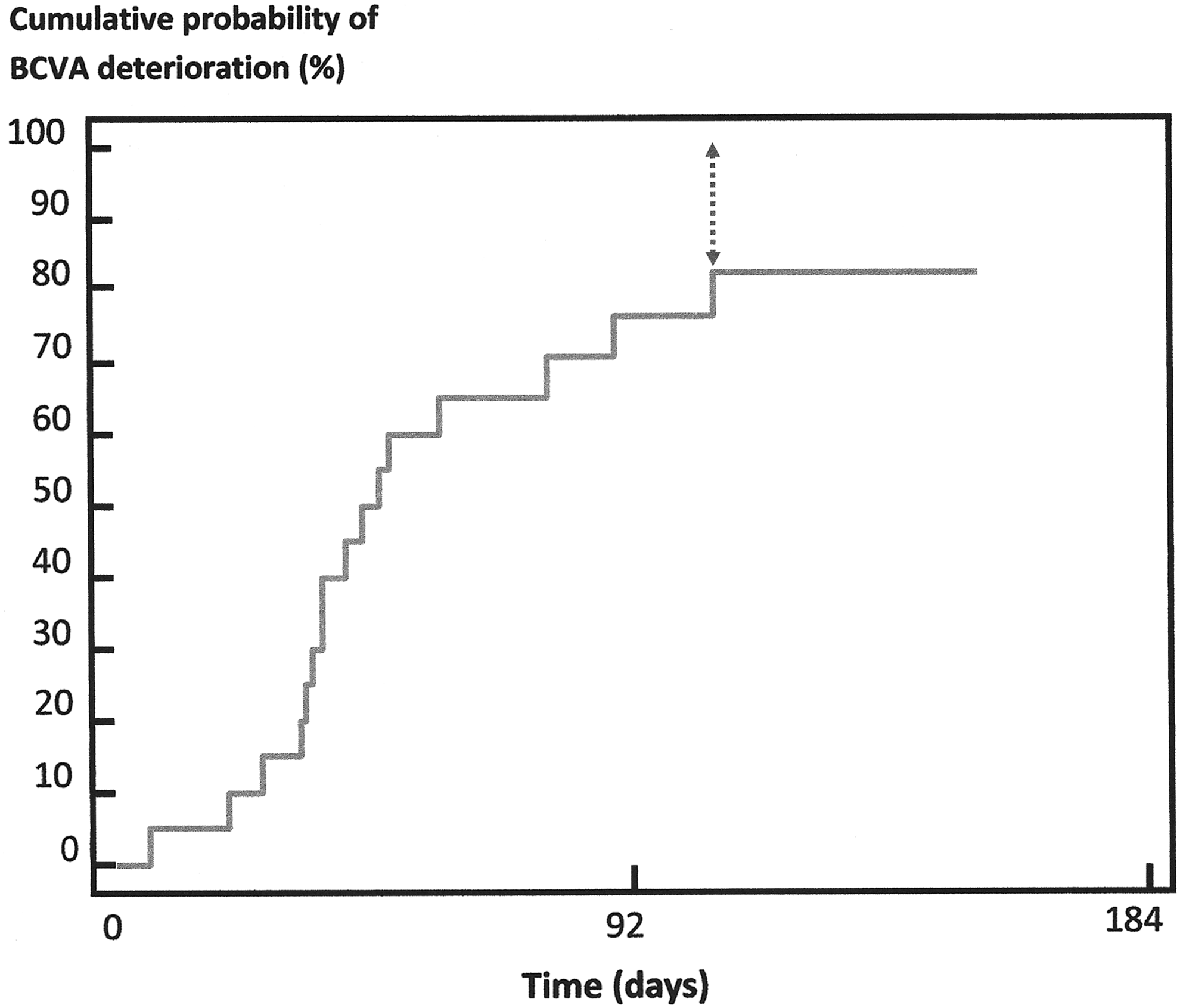
Kaplan–Meier survival curve of the time to BCVA deterioration after IVT-DI. At 100 days (3.3 months) after the IVT-DI, 17% of the eyes still present a BCVA improvement ≥0.3 logMAR.
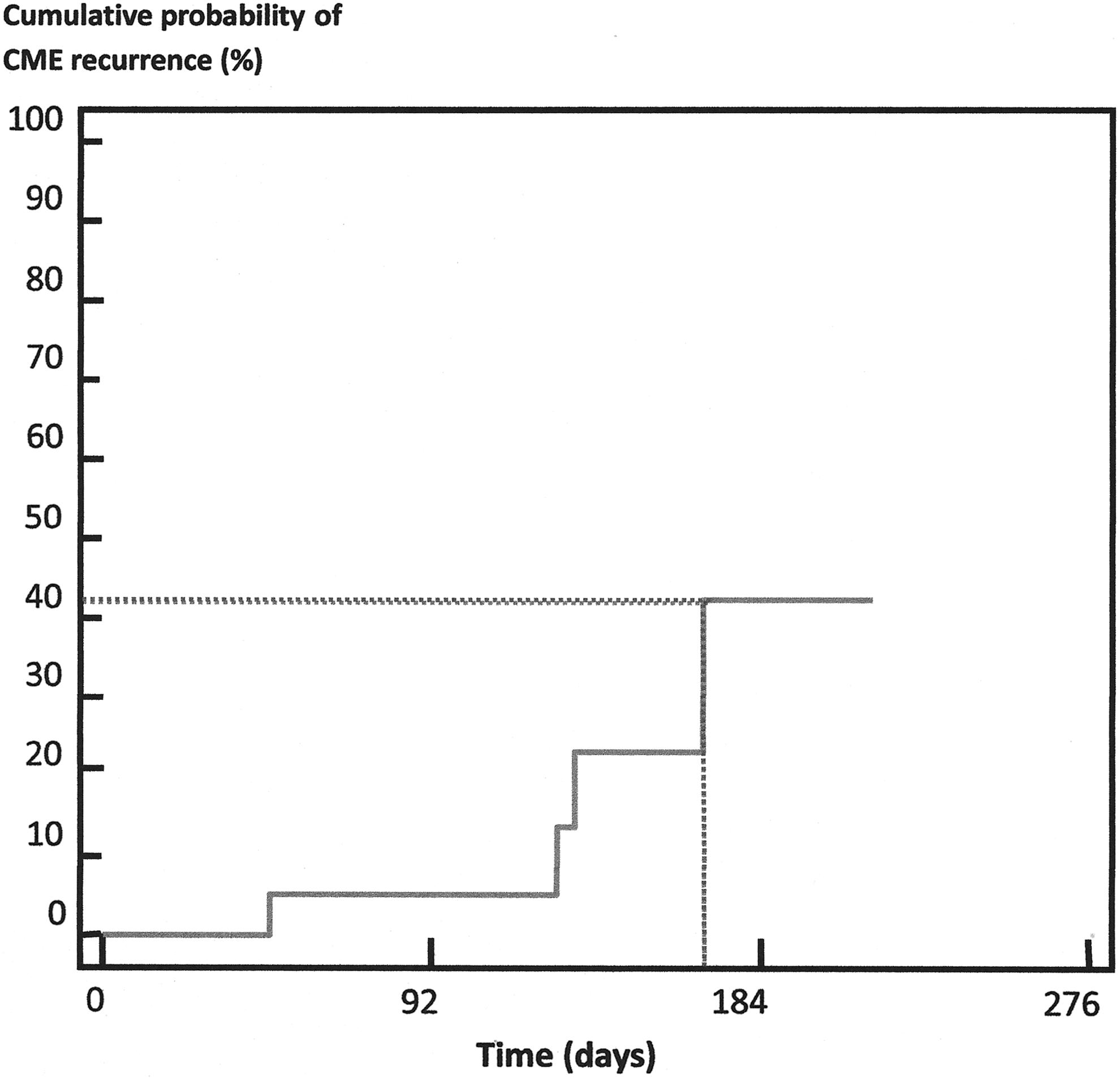
Kaplan–Meier survival curve of the time to CME recurrence after IVT-DI. At 6 months after the IVT-DI, 42% of the eyes present a CME recurrence expressed by an increase ≥20% of baseline CRT. CME, cystoid macular edema.
We found no statistically significant difference between the mean IOP before injection, early after injection (1.3 ± 0.7 months), and late after injection (4.4 ± 1 months). There is no increase in the number of patients using a triple antihypertensive therapy, and no glaucoma surgery, but 28% of the patients required a single or a double antihypertensive therapy in the later follow-up.
We did not note any adverse events because of the surgical intervention itself, such as subconjunctival hemorrhage, retinal detachment, vitreous hemorrhage, endophthalmitis, or implant migration.
Systemic and topical therapies were analyzed before and after IVT-DI (Table 2). Systemic steroids were used for 78.6% of the patients during the entire period before injection (Table 2), for 36% just before implant, and for 28.6% early and late after IVT-DI. Immunosuppressive treatment was used for 64.2% of the patients during all periods before injection (Table 2), for 43% just before implant, for 36% of the patients early after IVT-DI, and for 64.2% of patients late after IVT-DI.
From 7 years to 2 days before IVT-DI.
Antibiotics, antiviral, antituberculosis, and anticoagulant.
IVT-DI, intravitreal dexamethasone implant; anti-VEGF, anti-vascular endothelial growth factor; NSAID, nonsteroidal anti-inflammatory drugs; SLT, selective laser trabeculoplasty.
Discussion
Corticosteroids are the first-line treatment for noninfectious uveitis.10,22,23 There are different forms of administration of corticosteroids: topical, systemic, or local.
Topical steroids penetrate directly into the anterior chamber with minimal systemic absorption, reducing systemic side effects. It can be given at frequent intervals easily. However, topical administration increases the risk of local side effects, including cataract and increased IOP; moreover, it does not penetrate posterior structures of the eye. 24
Systemic steroids (oral or intravenous) are generally the first-line therapy for posterior noninfectious uveitis, especially if the ocular disease is bilateral. However, they induce many systemic side effects. 25
Local corticosteroid injections (periocular or intravitreal) are used for the treatment of both intermediate and posterior uveitis. Injections provide higher concentration of corticosteroids near the posterior pole for a better treatment of the posterior inflammation than oral treatment and topical drops.4,23,24 They allow limited systemic absorption and are particularly used when the pathology is unilateral. However, the half-life of local corticosteroid injections is a few months and the patients require repeated injections.4,13 Periocular injections present risks and side effects (ptosis, extraocular muscle injury, globe penetration, or skin depigmentation), but intravitreal injection also presents side effects (intravitreal hemorrhage, endophthalmitis, and retinal detachment). 26 Subconjunctival injections also cause cataract formation and elevated IOP. 25 One study found that the IOP of patients who had received ≥1 periocular triamcinolone acetonide 40 mg was ≥24 and ≥30 mmHg in 34.0% and 15%, respectively; glaucoma surgery was performed in 2.4% of eyes. Cataract surgery was performed within 12 months in 13.8% of the initially phakic eyes. 27
The IVT-DI releases corticosteroids slowly into the eye, providing a control of the posterior inflammation.4,13 We can speculate, as suggested in one of the MUST studies, 28 that good candidates for local treatment are unilateral or asymmetric uveitis or those with absolute contraindications to immunosuppressive therapy or temporary contraindications (i.e., pregnancy).11,12 Yet, one other part of the MUST study 29 did not demonstrate a clear benefit of the local approach over the systemic approach.
In our retrospective study, our results suggest that a single injection of IVT-DI for the treatment of noninfectious uveitis improves visual acuity and decreases macular thickness. All the positive effects were obtained without uncontrolled IOP or glaucoma surgery during the follow-up.
The effect of the IVT-DI on noninfectious uveitis has been investigated in several studies30–39 (Table 3); importantly, most studies are retrospective and included only few patients. All studies found a positive effect of the IVT-DI on both visual acuity and macular thickness. In terms of effectiveness, an important issue is the duration of the effect that seems to be around 4 to 6 months. This range has generally been obtained by Kaplan–Meier analysis,30,31 and our results are in accordance with these data. A few of the mentioned studies have analyzed the effect on the decrease of the dose of the immunosuppressive treatment. Unfortunately, owing to the design of our study, we are also unable to conclude about a possible effect of the injection on the dose of systemic immunosuppressive treatment. Concerning the safety profile, only 3 patients presented an IOP >25 mmHg at 1.3 ± 0.7 months. They were treated with antihypertensive drops and only 1 with an additional selective laser trabeculoplasty whereas no one required a glaucoma surgery. However, 21.4% and 14% of the patients had a triple antihypertensive therapy previously and just before IVT-DI, respectively. A detailed evaluation of the development of cataract was not performed in our retrospective study but none of the eyes needed a cataract surgery during our follow-up. There were no other serious adverse effects. However, this study is not designed to address the effects on cataract and glaucoma, as it typically takes longer than 4–5 months to develop.
All the studies are retrospective except 1 randomized sham-controlled phase 3 trial to determinate the dose of dexamethasone in the intravitreal implant.
IOP, intraocular pressure.
This study has several weaknesses. It is a retrospective study and few data were missing. In addition, there are multiple etiologies of noninfectious uveitis and the macular thickness is measured by 2 different OCT machines. Indeed, as mentioned in the Methods section, all measurements were not performed on the same OCT. However, it has been demonstrated that OCT Optovue RTVue both in normal and pathological edema underestimates the CRT as compared with Spectralis Plus OCT.20,21 Since OCT Optovue RTVue measurements were mostly performed at baseline, our findings of a macular thickness decrease are thus at most underestimated but not false.
In addition, follow-up time of each patient slightly differed, which induced some variability in between patients and in the mean evaluation time of visual acuity, macular thickness, and IOP.
In conclusion, in our group of patients with active noninfectious uveitis, the evaluation of a first single dexamethasone implant was found to improve visual acuity and decrease macular thickness without significant increase of IOP, although the effect seems limited in time. It seems to be an interesting adjuvant treatment in noninfectious uveitis already treated by systemic therapies.
Footnotes
Author Disclosure Statement
F.W., L.C., L.P., and X.J. have worked as consultants in advisory board for Allergan. X.J. has received travel refund.