
Abstract
Abstract
Purpose:
Evaluation of 0.3% cortisol phosphate eye drops in hyaluronic acid vehicle in the treatment of dry eye in Sjogren Syndrome.
Methods:
This prospective, single-center, masked (single blind), randomized controlled study included 40 female patients divided into 2 groups, group 1 treated with Idracemi, 0.3% cortisol phosphate eye drops twice a day, and group 2 treated with Cortivis, 0.3% cortisol phosphate in hyaluronic acid vehicle, with the same posology. Screening (day −7), randomization (day 0), follow-up (day 7), and termination (day 28) visits were conducted. Symptoms (VAS) questionnaire, tear film breakup time, corneo-conjunctival stain, intraocular pressure (IOP) measurement, and fundus examination were performed at each visit. Conjunctival impression cytology for human leukocyte antigen-DR (HLA-DR) expression at visit 1 and 4 was also performed.
Results:
No changes in IOP or fundus examination were observed in either group at each time point. Group 1 showed at day 28 a statistically significant amelioration of symptoms and reduction of HLA-DR expression. Group 2 showed at day 7 statistically significant improvement of corneal and conjunctival stain versus baseline and versus group 1; the symptom score was statistically significantly better than baseline and versus group 1 after 28 days too. The HLA-DR expression and the epithelial cell area were statistically significantly reduced versus baseline and versus group 1 at the same time.
Conclusions:
Cortisol phosphate proved to be safe and effective in treating dry eye in Sjogren Syndrome patients in both formulations. However, the formula with hyaluronic acid vehicle proved to be more effective. Both formulations were very well tolerated.
Introduction
I
Topical steroids constitute the first-choice therapy in noninfective acute inflammation of the ocular surface as well as in severe ocular dryness, postoperative inflammation, and in the prevention of corneal graft rejection.2–8
However, therapeutic index of prolonged steroid treatment is generally low due to their potential induction of subcapsular posterior cataract, of infection, of ocular hypertension, and glaucoma.9–11
Cortisol is a natural fast-acting corticosteroid of relative lower potency compared with synthetic steroids, whose topical use as an eye drop is generally considered to have a low prevalence of ocular side effects and a good safety profile. Cortivis (Medivis, Italy) formulation is characterized by the presence of cortisol phosphate in a water solution with sodium hyaluronate, a well-known natural vehicle that allows a prolonged permanence of the drug on the ocular surface. 12
Since dry eye is a chronic inflammatory disease, it would be useful to have an effective and safe drug that can be used with few daily applications to reduce the treatment burden. In fact, a safe and fast anti-inflammatory treatment would rapidly cure inflammatory episodes without worsening the patients' quality of life.
The aim of the present work was to evaluate the safety and clinical efficacy of cortisol phosphate 0.3% eye drops with and without hyaluronic acid vehicle in the treatment of ocular surface inflammation in moderate to severe dry eye in Sjogren Syndrome (SS) patients.
Methods
This prospective, masked, randomized controlled study was carried out at the University of Genoa, ltaly. Ethical approval was granted by the Ethics Committee of the University Hospital of Genoa and the study was conducted in concordance with the Declaration of Helsinki. Informed consent was obtained from all the participants after explanation of the nature and possible consequences of the study.
Patient population
Forty female patients with SS with moderate to severe dry eye grade 2–3 according to Berens et al. 3 were included in the study. The diagnosis of SS was carried out according to the classification criteria proposed by the American European Consensus Group. 13
Inclusion criteria were
1. Dry eye syndrome (either hyposecretive or hyperevaporative type) for at least 2 months.
2. Schirmer l test ≤8 mm/5 min.
3. Positivity to vital corneal staining, score 2 on a scale from 0 (absent) to 3 (severe), in at least 2 of 5 corneal areas as described by Lemp. 14
4. BUT <10 s.
5. Symptomatology of dry eye, with at least 2 positive symptoms (VAS >30 mm of 100 mm for each symptom) in the preceding 72 h, of the following:
- burning/stinging sensation
- ocular discomfort while blinking
- foreign body sensation
- sensation of ocular fatigue/heaviness of the lid
- preference to keep eyes closed
- itching
- photophobia
- sticky eye
- blurred vision
- dryness
6. Willingness to participate in the study while following the indications.
Exclusion criteria were
1. Age <18 years.
2. Pregnant or lactating women.
3. Women of childbearing potential who are not using adequate contraception methods.
4. Ocular surgery within the last 3 months.
5. Presence or onset of eye infections or of other acute pathologies, which could be resolved or modified during the course of the study independently from the treatment with study drugs.
6. Presence or onset of glaucoma.
7. Use of any topical ophthalmic medication with the exception of tear substitutes and/or eye cleaning solutions for the treatment of dry eye.
8. Patients being treated with topical ocular, cyclosporine, steroidal, or nonsteroidal anti-inflammatory medications within the last month.
9. Occlusion therapy with lachrymal or punctum plugs within the last 2 months.
10. Change in systemic treatment within the last 2 months.
11. Contact lens wearers.
12. Patients who have participated in any clinical investigation within the last 30 days or are currently participating in a clinical study.
13. Patients who are unlikely to comply with the requirements of the study protocol or who are at risk of moving or being lost to follow-up.
14. Expected change in treatment of concomitant disease.
15. Patients with a history of recurrent ocular herpes and/or recurrent uveitis.
16. Inadequate lid closure.
Study population
Treatment of 50% and 5% of the control treatment for an α value of 0.05, using a 2-tailed analysis, and a power of 90%, which gave a population of 38 patients in total (19 per arm), was considered to be an assumed efficacy of the study to achieve statistically significant results.
Treatment protocol
On day 0, the patients were divided into 2 groups by randomized computer sorting.
Group 1 patients were treated with idracemi eye drops (0.3% hydrocortisone phosphate; Farmigea), 2 drops/eye twice a day, instilled in the conjunctival sac.
Group 2 patients were treated with cortivis monodose (0.3% hydrocortisone sodium phosphate in hyaluronic acid vehicle, Medivis), 2 drops/eye twice a day, instilled in the conjunctival sac.
The treatment was carried out for 28 days. Patients underwent visits at enrollment (T-7), baseline (T0), follow-up (T7), and termination visit (day 28); Table 1.
Ocular tests performed
At each visit, symptom evaluation, TBUT, fluorescein, and lissamine green staining examinations of the ocular surface and IOP measurement were performed on both eyes of all patients. At T0 and T28, the patients underwent fundus examination on both eyes and conjunctival impression cytology only in the right eye.
A symptom severity score was obtained by means of a VAS (from 0 = symptom absent to 100 = maximum discomfort) for the following symptoms: burning, itching, foreign body sensation, photophobia, sticky eye, blurred vision, and dryness. The total score was obtained by adding up the results of each symptom; this parameter was considered for statistical analysis. The IOP was determined using a Goldmann applanation tonometer (Haag-Streit). For fluorescein and lissamine green staining, a previously described scoring system was used. 14 For conjunctival impression cytology specimens, Supor 200 polyether sulfone membranes (Supor® Pall Life Science) were used. The membranes were cut into strips of approximately 3 × 5 mm, which were pressed on the temporal bulbar conjunctiva for 5 seconds and then removed. The samples were transferred to polylysinated slides with slight pressure and fixed in a 4% paraformaldehyde solution. The slides were then processed for human leukocyte antigen-DR (HLA-DR) expression using a mouse monoclonal antibody anti-HLA-DR (Abcam). Specimens were rinsed 3 times in phosphate-buffered saline (PBS), incubated for 2 min in 0.3% H2O2 to inhibit endogenous peroxidase, and then incubated overnight at 4°C with the primary antibody against HLA-DR. After rinsing 3 times in PBS, the specimens were incubated for 1 h at room temperature with antimouse immunoglobulin G peroxidase conjugate (Sigma-Aldrich Srl) secondary antibody. The specimens were rinsed 3 times in PBS, stained with 3,3'-diaminobenzidine (Sigma-Aldrich Srl), and dehydrated with graded alcohols and xylene. The slides were coverslipped using DPX resin. Negative controls were treated identically to all other slides, omitting the primary antibody.
Images were photographed at the same magnification of 40 × with a Zeiss Axiovert 10 light microscope and saved as TIFF. A morphometric study was carried out using the public domain ImageJ software to quantitatively assess the HLA-DR expression. The RGB color images were converted into 32-bit grayscale images, using the function Image>type >32-bit, and the epithelial cell area and the grayscale value (function: analyze>measure) were calculated, respectively, in μm2 and in optical units from 0 = black to 255 = white. In this way, a higher expression of HLA-DR corresponded to darker images and was reported as lower values in the 0–255 grayscale; a lower expression was indicated by lighter images, corresponding to higher values on the same scale.
Statistical analysis
The global symptom score, the corneal fluorescein staining score, the IOP values, the epithelial cell area, and the HLA-DR expression on the conjunctival epithelial cells were considered as primary efficacy variables. The statistical analysis of the results was carried out in a masked method by an investigator not involved in the study, using the software MedCalc (version 11.4.1.0). Only the results of right eyes were considered for statistical analysis. Student's t test and Mann–Whitney U test were used as appropriate. A value of P < 0.05 for 2-tailed tests was considered statistically significant.
Results
The 40 subjects included in the study (38 females and 2 males, mean age ± standard deviation 59.5 ± 5.9 years) were randomly divided into 2 groups: group 1, 20 subjects (1 male, 19 females, mean age 60.1 ± 5.1 years); group 2, 20 subjects (1 male, 19 females, mean age 58.8 ± 6.7 years). The results of the study treatments on symptoms and tests are reported in Table 2.
Group 1 treated with IDRACEMI; Group 2 treated with CORTIVIS.
Versus T0.
Versus group 1 at the same time.
IOP, intraocular pressure; T0, baseline; T7, day 7; T28, day 28; TBUT, tear breakup time; VAS, visual analog scale.
For the impression cytology study, the morphometric data regarding the mean epithelial cell area and the HLA-DR expression, reported as optical units, are summarized in Table 3 and Figs. 1 and 2.

Morphometric results of the mean conjunctival epithelial cell area expressed in μm2. The cortivis-treated group (group 2) showed a statistically significant lower value than baseline and idracemi-treated group (group 1) at the same time of observation (P < 0.001 vs. both baseline and idracemi-treated group at the same time of observation).

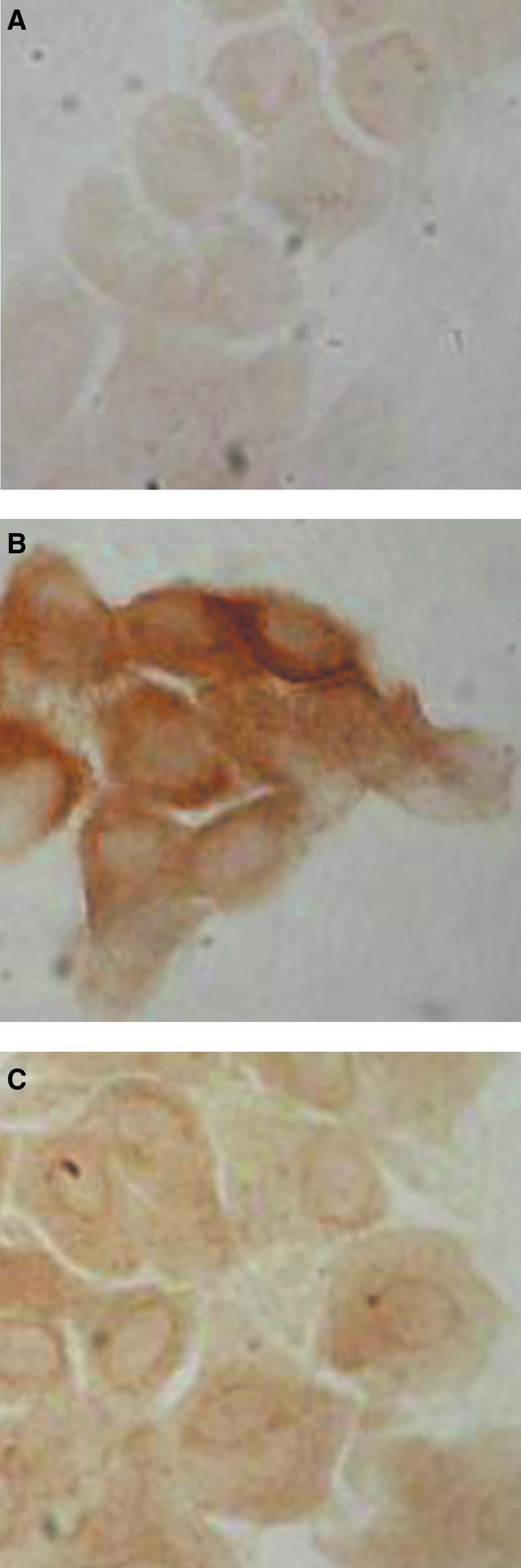
Morphometric results for the HLA-DR expression in conjunctival epithelial cells. The results were obtained converting the color images in optical units (from 0 = black to 255 = white). The higher the value, the clearer the cells and the lower the HLA-DR expression. HLA-DR, human leukocyte antigen-DR.
Versus baseline.
Versus group 1 at the same time.
HLA-DR, human leukocyte antigen-DR; T0, baseline; T28, day 28.
In group 1, after 28 days of treatment, there was a statistically significant improvement of the global symptom score from 316.9 ± 203.5 at baseline to 239.2 ± 97.5 (P = 0.032 vs. T0, mean difference −77.15; 95% confidence interval [CI] −147.1 to −7.2).
A statistically significant reduction of HLA-DR expression was present after 28 days of treatment (Fig. 2 and Table 3). No other statistically significant variations were found in group 1 for the other tests performed throughout the study.
In group 2, a statistically significant improvement of symptoms was observed at T28 (149.2 ± 126.5) versus both T0 (292.6 ± 177.5; P = 0.049; mean difference −89.7; 95% CI −179.3 to −0.11) and group 1 at the same time of observation (239.2 ± 97.5; P = 0.030; mean difference −88.4; 95% CI −167.6 to −9.3).
The TBUT in group 2 showed a statistically significant improvement versus T0 at T28 (from 2.5 ± 1.0 to 3.5 ± 1.3; P = 0.014; mean difference 1.0; 95% CI 0.22 to 1.77).
The lissamine green stain showed a statistically significant improvement of the conjunctival epithelium starting from T7 (from 4.3 ± 1.1 at T0 to 3.1 ± 1.5 at T7; P = 0.006; mean difference −1.05; 95% CI −1.76 to −0.33) and lasting throughout the study. A statistically significant difference was also observed versus group 1 patients at the same time of observation (4.4 ± 1.0) (P = 0.002; mean difference −1.3; 95% CI −2.10 to −0.49) and lasting for the duration of the study.
The corneal fluorescein stain showed a statistically significant improvement versus T0 starting from T7 (from 6.4 ± 2.9 at T0 to 3.7 ± 2.5 at T7; P = 0.0003; mean difference −2.7; 95% CI −3.97 to −1.42) and versus group 1 at the same time (5.5 ± 1.2 for group 1 and 3.7 ± 2.5 for group 2; P = 0.014; mean difference −1.8; 95% CI −3.22 to −0.37).
No statistically significant changes were found for IOP at all times in both groups compared with baseline values. No significant changes were found at fundus examination in both groups of patients at any time of the study.
A statistically significant reduction of the epithelial cell area was observed in group 2 after 28 days of treatment (T0 = 372.9 ± 132.9, T28 = 305.9 ± 129.0; P < 0.001; mean difference −97.9; 95% CI −132.1 to −63.7). There was also a statistically significant difference versus group 1 at the same time (group 1 = 405.6 ± 107.1) (P < 0.001; mean difference −67.3; 95% CI −103.9 to −30.7) (Fig. 1 and Table 3).
As to the HLA-DR expression in the specimens obtained from both groups, at T0, it was mainly localized in the cellular membrane and in the cytoplasm. At T28, in group 1, the conjunctival cells showed a milder irregular positivity, while in group 2, the expression was significantly reduced and it was localized only along the cellular membrane.
A morphometric study was carried out on the images converted from color to grayscale. In group 1, the expression of HLA-DR changed in a statistically significant manner at T28 when compared with T0 values (from 60.8 ± 18 at T0 to 78.0 ± 18.9 at T28; P = 0.02; mean difference 8.62; 95% CI 1.43 to 18.81). In group 2, a marked statistically significant reduction of the HLA-DR expression was observed at T28, both versus T0 (109.9 ± 18.0 and 58.9 ± 19.0, respectively; P = 0.0001; mean difference 50.99; 95% CI 46.61 to 55.37) and group 1 (109.9 ± 18.0 and 78.0 ± 18.9, respectively; P = 0.0001; mean difference 32.89; 95% CI 27.96 to 37.83) (Figs. 2–3A–C and Table 3).
Discussion
Dry eye is a common ocular surface disease with various clinical manifestations. Some mild or episodic symptoms are easily controlled with ocular lubricants. However, long-term application of artificial tears is not effective for some patients, especially those with moderate to severe symptoms. It has been confirmed that dry eye is related to the inflammation of ocular surface and it is based on immune response. Corticosteroids are effective anti-inflammatory drugs widely used to control eye inflammation.15–19
Hyaluronic acid (HA) eye drops have been used in several trials for the treatment of dry eye.20–27 HA is able to increase precorneal tear film stability and corneal wettability; it reduces the tear evaporation rate as well as the healing time of corneal epithelium in any eye patients.24,25,28–31 Furthermore, data in literature suggest a positive effect of HA on conjunctival cells in Sjogren Syndrome patients. 32
The results of the present study showed that the treatment with both formulations of 0.3% cortisol phosphate was able to determine a clinical amelioration of ocular discomfort, as demonstrated by the statistically significant improvement in clinical tests and symptoms. However, the formulation of cortisol with hyaluronic acid showed better results and a potentiated anti-inflammatory activity (as confirmed by the higher reduction of HLA-DR markers) probably due to the increase of ocular surface residence time due to the use of hyaluronic acid as the vehicle.
It should be noted that the presence of preservatives in the idracemi formulation in group one, even if with demonstrated low levels of direct toxicity on histology of the tissues in specifically addressed studies,33,34 could be a confounding factor and could have had some role in the difference of results obtained from the 2 preparations.
No adverse events were recorded, since IOP and fundus examinations were not modified by either treatment during the 28 days of therapy. Due to the well-known possible complications linked to prolonged steroid treatment, long-term effects even of small concentrations of a mild steroid with short metabolism such as topical hydrocortisone on intraocular pressure (IOP) and cataract formation are not known and should be monitored with caution.
Cortisol phosphate in hyaluronic acid vehicle is an innovative formulation, which guarantees double efficacy: in both hydrophilic environment (tear film) and lipid environment (cornea). It also guarantees double safety because it ensures good tolerability during instillation because of the aqueous solution as well as a negligible effect on the IOP increase. Cortivis is 0.3% cortisol phosphate associated with hyaluronic acid (a natural drug delivery system). This differentiates the product from all other topical steroids. The association of cortisol and hyaluronic acid creates a compound between the steroid and the polymer, which is a hydrophilic mucoadhesive drug in which cortisol and hyaluronic acid are linked through hydrogen bonds and which is able to bind the epithelial corneal mucin. This leads to a long permanence of the cortisol on the ocular surface. Light scattering experiments have shown that the cortisol chemically interacts with hyaluronic acid by forming mucoadhesive micrometric aggregates, which are characterized by a weak negative charge. 12 This confirms that the ability to be mucoadhesive is transferred from hyaluronic acid to the cortisol through molecular chemical interactions. That is the mechanism that allows the long-term maintenance of cortivis on the ocular surface. Therefore, cortivis is highly indicated for the treatment of inflammation of ocular surface. Some note should be taken that all the results have been obtained in females who may have different behavior in response to steroids than males.
This new formulation can be considered an ideal choice for the treatment of severe ocular dryness, with inflammatory component. In fact, it guarantees high efficacy due to the intrinsic characteristics of the molecule and ensures minimal risk of complications due to the presence of hyaluronic acid and the absence of both surfactants and preservatives in its formulation.
Cortivis was shown to exert anti-inflammatory activity powerful enough to reduce the expression of HLA-DR in conjunctival epithelial cells. The evaluation of HLA-DR as an inflammatory marker has been previously reported as an objective and quantitative method for the assessment of inflammation on the ocular surface.35–37 HLA-DR is an immune-related marker, normally expressed by immunocompetent cells, which is upregulated in epithelial cells in case of autoimmune and inflammatory disorders. In dry eye, conjunctival cells overexpress this marker,36–40 probably in response to tear film alterations capable of inducing inflammation-driven epithelial damage. The cortivis treatment induced a more profound suppression of marker expression, corresponding to a significantly better improvement of clinical conditions versus cortisol alone. While immunohistochemistry usually provides only a topographical description of the cellular structures positive for the stain, morphometric analysis of the specimens permitted obtaining of accurate quantitative data on the molecular expression and the changes determined by the treatment.41,42
The conjunctival epithelial cells, during chronic illness, show peculiar changes defined as squamous metaplasia.2,43–46 This is characterized by the presence of enlarged keratinized cells with reduced nucleus/cytoplasm ratio, associated with decreased goblet cell density, so that it can be considered a characteristic feature of ocular surface damage. These conjunctival alterations determine the production of a malfunctioning tear film, as demonstrated by the reduced TBUT, resulting in a dry eye condition. A treatment that is able to revert the conjunctival metaplastic changes will help considerably to restore a healthier ocular surface, with an improvement of symptoms and signs of ocular discomfort. From this point of view, the reduced area of the epithelial cells indicates a significant improvement of the ocular surface conditions. The inflammatory status occurring in SS requires a therapy, which may be accompanied by complications, such as IOP increase, capable of greatly interfering with the final outcome of the treatment. However, no IOP rise was observed throughout the study in both groups.
With regard to corticosteroid therapy, the use of a molecule designed to address its therapeutic efficacy mainly on the ocular surface without penetrating into the eye can be considered an important tool in dry eye treatment in patients with SS and should provide considerable advantages. Cortivis could be suggested among the molecules pertaining to this specific group.
Our results showed that it was possible to obtain a significant improvement of corneo-conjunctival epithelium already after 7 days, with further improvement after 28 days. The symptoms showed a significant improvement in both groups at 28 days, but it was more evident in the cortivis patients. Breakup time showed in the cortivis-treated group, a statistically significant improvement after 28 days, although it remained in the abnormal range, thus demonstrating that ocular surface impairment in SS would probably need a more complex and longer therapeutic approach.
Considering the results of the tests performed, together with significant reduction of the conjunctival HLA-DR expression and the improvement of cytologic features of the epithelium, it can be concluded that the treatment with cortisol phosphate in hyaluronic acid vehicle was able to induce a significant clinical amelioration of the ocular surface in patients with SS, with administration only twice a day. This gives a reduced treatment-related burden to the patients and provides for a good therapeutic tool designed to obtain rapid reduction of inflammation with a lower number of administrations compared with less potent corticosteroids. In fact, cortivis eye drops proved to be a safe and effective first-line treatment in the management of ocular surface inflammation in moderate to severe dry eye. Having obtained the objective of a significant reduction of inflammation, this treatment could be switched to less potent corticosteroids at lower dosage and with fewer administrations as a maintenance therapy.
In summary, cortivis showed better performance compared with a similar active formula without the viscoelastic polymer. Statistically significant differences were found after 28 days of treatment for each parameter evaluated and already after 7 days of treatment for corneo-conjunctival staining between the 2 groups of treatment.
Footnotes
Acknowledgments
Cortivis and idracemi used in the trial were provided by Medivis (Italy) and Farmigea (Italy), respectively.
Author Disclosure Statement
No competing financial interest exists