
Abstract
Abstract
Purpose:
The objective was to provide preliminary information about the efficacy and safety of immunologically safe plasma rich in growth factor (immunosafe PRGF) eye drops in the treatment of moderate to severe dry eye in patients with primary and secondary Sjögren's syndrome (SS) and to analyze the influence of several variables on treatment outcomes.
Methods:
This retrospective study included patients with SS. All patients were treated with previously immunosafe PRGF eye drops to reduce the immunologic component contents. Ocular Surface Disease Index (OSDI) scale, best-corrected visual acuity (BCVA), visual analog scale (VAS) frequency, and VAS severity outcome measures were evaluated before and after treatment with immunosafe PRGF. The potential influence of some patient clinical variables on results was also assessed. Safety assessment was also performed reporting all adverse events.
Results:
Twenty-six patients (12 patients with primary SS, and 14 patients suffering secondary SS) with a total of 52 affected eyes were included and evaluated. Immunosafe PRGF treatment showed a significant reduction (P < 0.05) in OSDI scale (41.86%), in BCVA (62.97%), in VAS frequency (34.75%), and in VAS severity (41.50%). BCVA and VAS frequency scores improved significantly (P < 0.05) after concomitant treatment of PRGF with corticosteroids. Only 2 adverse events were reported in 2 patients (7.7% of patients).
Conclusions:
Signs and symptoms of dry eye syndrome in patients with SS were reduced after treatment with PRGF-Endoret eye drops. Immunosafe PRGF-Endoret is safe and effective for treating patients with primary and secondary SS.
Introduction
S
Autoimmune lacrimal gland destruction mediated by T lymphocytes leads to the development of dry eye syndrome (DES), a disorder that is often more severe in patients with SS than with non-SS. DES is clinically characterized by eye irritation, tear film instability, increased tear osmolarity, and ocular surface epithelial disease.3–5 It also has an inflammatory component since changes in the tear film composition caused by gland destruction of the lacrimal functional unit can stimulate the production of the proinflammatory cytokines on the ocular surface tissues. 6 Several proinflammatory molecules (IL-1α, IL-6, IL-17, TNF-α) and the transforming growth factor-β1 have been increased in the conjunctival epithelium of patients with SS. 7 Furthermore, the interferon-γ could be used as a biomarker for DES and SS due to its involvement in the loss of goblet cells and epithelial apoptosis, and finding high concentrations of its RNA in the conjunctiva, tears, and blood.8–10 Tear film hyperosmolarity is also a trigger factor of proinflammatory process in DES through the activation of the mitogen-activated protein kinases and nuclear factor-kB, which leads to the production of proinflammatory cytokines and matrix metalloproteinases.6,11
Improper handling of DES inflammatory process can lead to chronic ocular surface disease (OSD), which could even reach to corneal blindness in the cases of untreated patients. 5 DES has a great impact on the life quality of patients, affecting the fulfillment of several daily tasks such as reading, computer use, or driving. 12
Preservative-free artificial eye drops are the main conventional treatment for dry eye providing ocular surface lubrication. However, they lack the complex composition of natural tears such as water, salts, lipids, proteins, and growth factors. 13 Furthermore, taking into consideration that inflammation plays a main role in the pathogenesis of dry eye, other therapeutic alternatives such as topical corticosteroids and cyclosporine are used as a second-line treatment in severe dry eye.14,15 However, their use is limited due to several side effects, including ocular burns, strong irritation, increase of intraocular pressure, and glaucoma.16,17
The autologous serum (AS) eye drops are considered to be a safe and efficient treatment for patients with dry eye due to its ocular surface essential protein and growth factor contents.18,19 However, several studies show controversial results after using AS in patients with DES.20–22 AS eye drops might not be effective on ocular surface wound healing if circulating antibodies and proinflammatory cytokines are present, especially in patients with severe OSD linked to inflammation.23,24 A clinical study in patients with secondary SS shows unsuccessful results for DES after AS treatment. 19
Recently, autologous platelet enrichment technologies have been developed with the purpose of increasing protein and growth factor levels involved in tissue regeneration and stored into the α-granules of platelets. 25 Plasma rich in growth factors (PRGF) is one of those technologies, which is highly characterized due to its protein and growth factor content, as well as its biological stability over time.26–28 Other important features of PRGF formulations are their antimicrobial, antifibrotic, and anti-inflammatory properties.29–31 All of these characteristics exalt PRGF as an appropriate treatment for ocular surface disorders. PRGF eye drops have been successfully used for the treatment of several OSD such as DES from different etiologies, persistent epithelial defects, and corneal ulcers.32–35 However, no specific studies have been previously carried out with PRGF reduced in inflammatory components. 36 PRGF eye drops have demonstrated to be effective in the treatment of DES, including those patients previously treated with AS or cyclosporine. 34
The purpose of the present retrospective study is to show preliminary information about the safety and efficacy of immunologically safe (immunosafe) PRGF eye drops in the treatment of patients with SS (primary and secondary) and also to analyze the influence of several variables on treatment outcomes.
Methods
A retrospective design study was performed, including 12 patients with primary SS (24 eyes) and 14 patients (28 eyes) with secondary SS (Table 1), treated between September 2011 and September 2013 at a single private center, Ocular Surface Unit of the Fernandez-Vega University Institute (Oviedo, Spain). All the Declaration of Helsinki principles were fulfilled to perform this study.
BCVA, best corrected visual acuity; OSDI, ocular surface disease index; PRGF, plasma rich in growth factors; RA, rheumatoid arthritis; SD, standard deviation; SLE, systemic lupus erythematosus; SS, Sjögren syndrome; VAS, visual analog scale.
All patients included in the study were diagnosed with SS following the classification principles from the American-European Consensus Group of rheumatologists and ophthalmologists. 37 Most of the SS patients included in this study showed meibomian gland dysfunction, being classified and diagnosed as evaporative dry eye. Patients included in the study must fulfill the following criteria: (1) symptoms of dry eye, (2) symptoms of dry mouth, (3) clinical tests for ocular signs such as Schirmer's test, tear break-up time (TBUT), and/or rose Bengal staining, (4) focal lymphocytic sialadenitis within minor salivary glands with quantification determined by histopathological evaluation, (5) signs of salivary gland involvement evaluated by parotid sialography, scintigraphy, and unstimulated salivary flow, and (6) presence of autoantibodies: anti-Ro(SSA) and anti-La(SSB). Those patients without associated autoimmune disease such as SLE, RA, and connectivopathies, and who presented 4 of 6 items mentioned above were diagnosed with primary SS. Secondary SS was defined in the presence of an associated connective tissue disease at the same time that patients fulfilled the first 3 criteria points described above. Forty patients (9 with RA and 5 with SLE) diagnosed as secondary SS were included in the study. 37 Patients diagnosed as SS with moderate to severe DES for at least 6 months of evolution were included in the study. DES criteria were established according to the DEWS 2007 classification. 38 All enrolled patients had Schirmer I test values of less than 5 mm, TBUT film values less than 5 s, and a poor or no response to previous treatments for DES (artificial tears, topical or systemic corticosteroids, therapeutic contact lenses, punctal occlusion plugs, AS, and/or topical cyclosporine).
Patients with lid structural abnormalities; with morphological changes in meibomian glands such as vascular dilation, acinar atrophy, or orifice metaplasia; with any inflammation or active structural change in the cornea, conjunctiva, iris, or anterior chamber; glaucoma; and with any active corneal infection were excluded from the study.
PRGF preparation
After informed consent was signed, patients' blood was collected into 9-mL tubes. Samples were centrifuged at 580 g for 8 min at room temperature in an Endoret System centrifuge (BTI Biotechnology Institute, S.L., Miñano, Álava, Spain). The whole column of PRGF was collected after centrifugation using the Endoret ophthalmology kit (BTI Biotechnology Institute) and avoiding the buffy coat that contains the leukocytes. PRGF eye drops were incubated at 37°C for 1 h. The obtained supernatant was then heat treated at 56°C for 60 min to reduce the immunologic components (immunosafe PRGF). Finally, plasma supernatants were filtered, aliquoted, and stored at −20°C until use.
All procedures were performed under highly sterile conditions, operating inside a laminar flow hood. 36 Before initiating the treatment, patients were instructed to keep the PRGF eye-drop dispensers at −20°C for a maximum of 3 months; each dispenser was used for 3 consecutive days.
All patients gave their informed consent before starting treatment. The PRGF-Endoret eye drops were applied topically (in conjunctival sac) 4 times daily for 6 weeks in the affected eye. In case of poor response, an additional cycle of 6 weeks with PRGF was added, up to 7 cycles. PRGF treatment did not exclude the use of other concomitant treatments (antibiotic agents, anti-inflammatory, artificial tears, etc.) when considered necessary.
Outcome measures
Several outcome variables were used to measure the efficacy of PRGF eye drop treatment. All these variables were measured before and after the treatment with PRGF for a follow-up period of 12 months.
Both demographic (gender, age) and clinical variables of patients (associated pathologies, previous and concomitant treatments, etc.) were collected. All necessary data were obtained from clinical records of patients.
Treatment response was determined by a combination of clinical examination (slit lamp) and evaluation of ocular surface symptoms [OSD index (OSDI), visual analog scale (VAS)], also the best corrected visual acuity (BCVA) was determined using Snellen optotype (conversion to logMAR scale logarithm of the minimum angle of resolution). The evaluation of ocular surface symptoms was done with the OSDI scale; OSDI scale estimated values ranging from 0 to 100 by severity of dry eye symptoms, and with the VAS (100-point scale; 0 = no discomfort, 100 = maximal discomfort, dryness, burning/stinging, photophobia, foreign body sensation, blurred vision, itching, and pain), both in frequency and severity of symptoms.
The positive response to continue with the treatment was defined as improvement in clinical signs associated with the improvement in subjective scales.
Safety assessment was performed by recording and evaluating any adverse events or complications that may appear during the time of therapy with PRGF.
Statistical analyses
Descriptive statistics were performed using absolute and relative frequency distributions for qualitative variables and mean values and standard deviations (SD) for quantitative variables. Different normality tests (Kolmogorov–Smirnov and Shapiro–Wilk) were performed on each variable sample.
Variables that showed differences among them in the baseline values and the variables with potential modified effect on outcome measures were identified by the statistical test required on each case. These variables were taken into account when analyzing the results before and after treatment with PRGF, stratifying them accordingly. Any potential difference observed between baseline (before) and after PRGF treatment was analyzed using the nonparametric Wilcoxon statistical test. Statistical significance level was set at P < 0.05. SPSS v15.0 for Windows statistical software package (SPSS, Inc., Chicago, IL) was used for all statistical analyses.
Results
Demographic and clinical results of patients with primary or secondary SS are shown in Table 1. Twenty-six patients with a total of 52 affected eyes were included and evaluated in the present study. All patients were women (100%). The mean age of the patients was 59.9 years (SD = 14.9, range between 35 and 87 years). Half of the patients (50%) were older than 60 years. All cases were bilateral since the pathology affected both eyes equally.
The 65.4% (17 patients) received 1 or 2 cycles of PRGF (1 cycle = 6 weeks of treatment), while 34.6% (9 cases) received 3 or 4 cycles of PRGF. Six patients (22.2%) had high blood pressure (HBP).
Of the 56 treated eyes, 18 of them were previously treated with corticosteroids (34.6%). A total of 6 cases (11.5%) were previously treated with AS, and 10 (19.2%) with cyclosporine eye drops (0.05% twice daily) without favorable results. In 4 cases (7.7%), a concomitant treatment with cyclosporine eye drops (0.05% twice daily) was maintained.
Results of primary outcome measures for the entire study population are summarized in Fig. 1. A significant reduction in the OSDI scale was observed from a baseline value of 55.13 (SD = 19.60) to a final post-treatment value of 32.74 (SD = 22.47). The latter represents a total reduction of 41.86%, which was statistically significant (P < 0.05) (Fig. 1A). The BCVA (conversion to logMAR scale logarithm of the minimum angle of resolution) was reduced from a baseline value of 0.17 (SD = 0.21) to a final post-treatment value of 0.06 (SD = 0.08), showing an improvement of 62.97% (P < 0.05) (Fig. 1B).
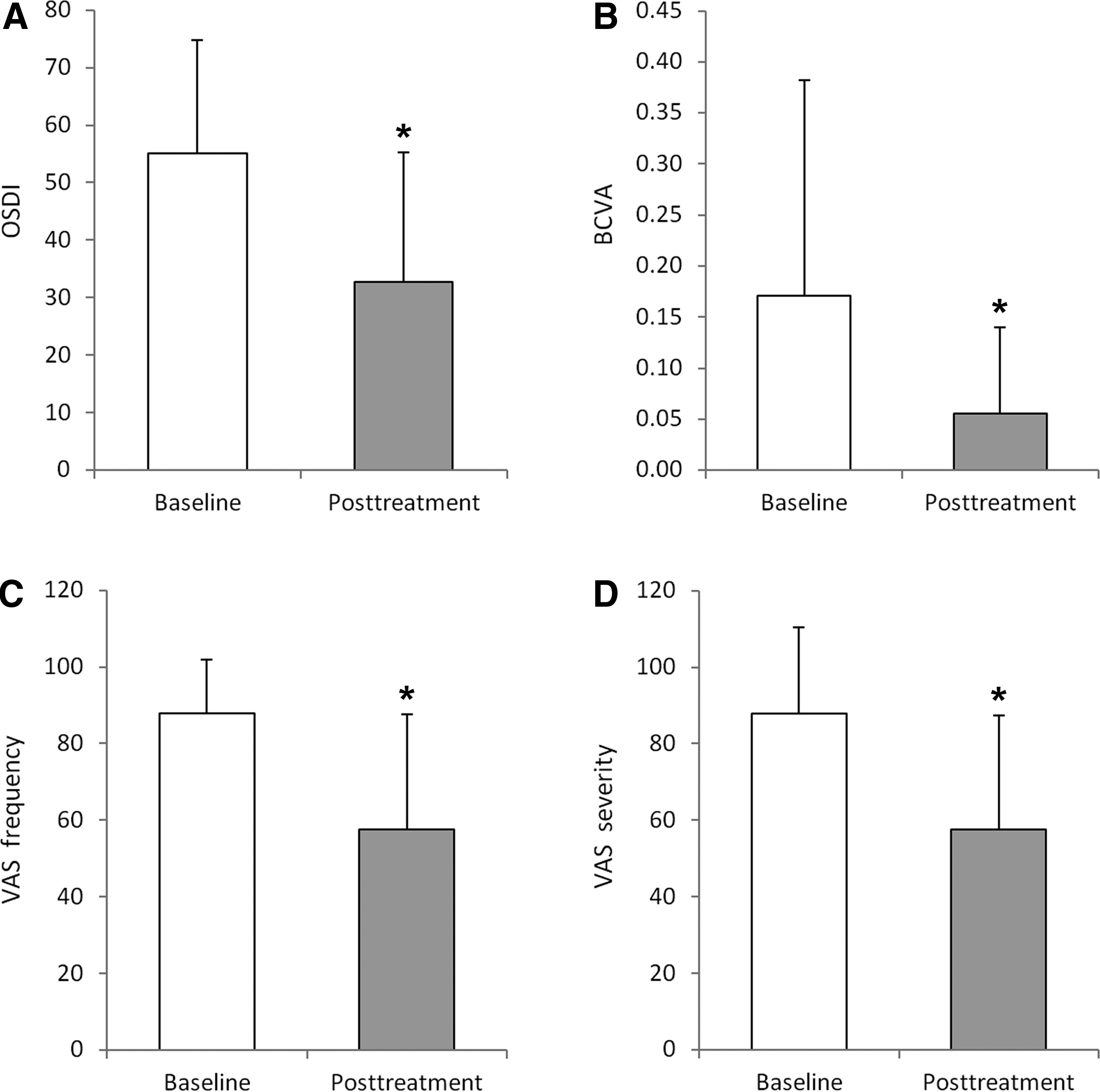
Outcome measures before and after plasma rich in growth factor eye drop treatments. Results obtained by OSDI
Regarding the ocular symptoms (discomfort, dryness, burning/stinging, photophobia, foreign body sensation, blurred vision, itching, and pain) measured by VAS score in frequency, a significant decrease was measured ranging from a baseline value of 87.98 (SD = 14.01) to a final post-treatment value of 57.69 (SD = 29.84). This represented a reduction of 34.75% being statistically significant (P < 0.05) (Fig. 1C). Finally, the VAS score of symptoms in severity resulted in a relevant and significant decrease of 41.50%, going from a baseline value of 81.15 (SD = 22.37) to a final post-treatment value of 47.69 (SD = 29.75), which was also statistically significant (P < 0.05) (Fig. 1D).
Results from the primary outcome measures were stratified according to the variables identified as potential effect modifiers. These variables include age, HBP presence, number of PRGF cycles (1–2 or 3–4), previous treatment with AS or cyclosporine, and concomitant treatment with corticosteroids or with cyclosporine.
Regarding the stratified results observed in the OSDI scale (Table 2), the previous treatment with AS showed a clear influence on the baseline OSDI values and in the improvement after treatment with PRGF. In patients who previously were treated with AS, the improvement after treatment with PRGF eye drops was significantly greater (P < 0.05). In the case of BCVA, significantly better results were observed for the patients treated concomitantly with corticosteroids (P < 0.05) than for those ones who were not treated concomitantly (reduction of 73.1% vs. 43.8%) (Table 3). Interestingly, concomitant treatment with cyclosporine showed no significant improvement (P = 0.066) in BCVA despite a reduction of 72.7% from the baseline to the final post-treatment value.
Statistically significant difference (P < 0.05) between groups.
No statistically significant differences (P > 0.05) before versus after treatment with PRGF.
AS, autologous serum; HBP, high blood pressure.
Statistically significant difference (P < 0.05) between groups.
No statistically significant differences (P > 0.05) before versus after treatment with PRGF.
Stratification regarding VAS frequency scale also led to improved outcomes in those cases in which concomitant cyclosporine and corticosteroids were not used (P < 0.05) (Table 4). Furthermore, no significant differences were observed from baseline to final treatment when concomitant treatment was used (P = 0.066 in the case of corticosteroids and P = 0.157 in the case of cyclosporine). Regarding VAS severity scale, with the exception of using cyclosporine as concomitant treatment, all outcomes significantly improved after PRGF treatment (Table 5).
Statistically significant difference (P < 0.05) between groups.
No statistically significant differences (P > 0.05) before versus after treatment with PRGF.
No statistically significant differences (P > 0.05) before versus after treatment with PRGF.
Regarding safety, 2 adverse events (7.7%) were reported during the treatment with PRGF. Both patients showed eye irritation. The symptoms were satisfactorily resolved in a few days.
Discussion
The prevalence of SS in the global population has been reported to be from 0.2% to 3.0%, predominantly affecting women aged between 40 and 60 years, presenting a ratio (women vs. men) of 9:1.39,40 A retrospective study of 220 patients with DES showed that 25% (57 patients) had some type of rheumatic disease, where twelve of them were diagnosed with SS. Primary in the initial ophthalmologic visit, therefore it is important to take this into account facing DES symptoms. 41 The ocular involvement of SS is mainly due to the deterioration of the lacrimal functional unit by lymphocytic infiltration, which promotes destructive inflammatory mechanisms. 42 This situation could lead to chronic DES of difficult treatment, which if not properly controlled could then result in severe ocular complications (including corneal blindness) with significant impact on the quality of life of patients. 43
Topical lubricants would be the first choice of treatment of DES in patients with SS. If this would not work, AS therapy, topical applications of corticoids and/or cyclosporine would be then used. And finally, the last treatment of choice would be secretagogues (pilocarpine, cevimeline). Punctual plugs or biological drugs not licensed for ophthalmological use such as rituximab, belimumab, and epratuzumab are used if the above therapies are not effective. Finally, rescue treatment with corneal transplant or autograft limbal epithelial cells is the last opportunity so that these patients can be kept. 44 In addition, inflammatory mechanism should be controlled to avoid the inflammatory progression and tissue injury.
PRGF eye drops have been developed to provide a therapeutic alternative to the SS and DES patients, being approved by the local regulatory agency in the category of human-use medicinal products. 45 The heated PRGF eye drops used in the present study maintain their regenerative, bacteriostatic, and anti-inflammatory properties, reducing the content in inflammatory components.36,46 In light of the foregoing, heat-inactivation treatment of platelet-rich plasma is suggested for treating patients with autoimmune diseases thus minimizing the risk to enhance ocular inflammation. Otherwise, AS eye drops have been shown to be of no effect in the treatment of secondary SS probably due to high levels of serum proinflammatory cytokine. 19
In a recent study, PRGF eye drops showed their effectiveness in the ocular surface wound healing, reducing corneal haze formation in mice subjected to PRK surgery. 47 The success of PRGF eye drops was also observed in the treatment of different OSD, showing a significant reduction (P < 0.05) in OSDI and a significant improvement (P < 0.05) in BCVA and in frequency and severity of VAS scores.35,48 In addition, patients suffering from moderate to severe DES who were previously treated with AS or cyclosporine with unsatisfactorily results showed a significant improvement in dry eye symptoms after treatment with PRGF eye drops. 34
Results from the present retrospective 12-month follow-up study suggest that the use of immunologically safe PRGF eye drops improved significantly (P < 0.05) the BCVA in 62.97% of patients suffering primary (24 eyes) or secondary (28 eyes) SS. Furthermore, dry eye symptoms measured by the OSDI test were significantly reduced (P < 0.05) after treatment with immunosafe PRGF eye drops, showing a reduction of 41.86%; additionally, the quality of life of SS patients was also improved (P < 0.05), showing a decrease of 34.75% and 41.50% in the frequency and severity VAS, respectively. A total of 65.4% of patients received between 1 and 2 cycles of immunosafe PRGF eye drops.
In our study, 34.6% of patients were previously treated with corticoids, 11.5% with AS and 19.2% with cyclosporine with unfavorable results. These patients showed a significant clinical improvement (P < 0.05) of BCVA, OSDI, and VAS after treatment with immunosafe PRGF eye drops. These results suggest that PRGF eye drops are a good treatment and should be thought of as an initial therapy option for DES in patients with SS. Analyzing the results observed in this study and taking into account the modifying effects identified in certain variables, it is noteworthy that concomitant treatment with cyclosporine did not improve (P > 0.05) BCVA and VAS scores in comparison to the patients treated with heated PRGF eye drops alone. However, concomitant treatment of PRGF eye drops with corticosteroids improves BCVA and VAS frequency scores in patients with SS.
Two adverse events were reported along the study. These 2 events (eye irritation) were registered as mild and were related to the use of PRGF eye drops, no hampering to complete the treatment period.
Cyclosporine treatment has been published in several studies in patients with DES with encouraging results 49 ; however, most of these studies are retrospective and with a follow-up period between 1 and 6 months being necessary to carry out more comparative and prospective studies. 50
The present study has some limitations. First, this is a noncomparative study without the control group. Second, it is necessary to increase the number of patients treated with this method to verify and clarify the results obtained in this study. Third, in future studies, it would be interesting to include some more clinical variables such as corneal and conjunctival staining, Schirmer's test, and tear film osmolarity analysis. However, despite the potential limitations, the data observed in this study suggest that the use of immunologically safe PRGF-Endoret eye drops is safe and effective in reducing the signs and symptoms of DES in patients with SS. PRGF treatment reduces significantly the OSDI score in those patients who were previously treated with AS, improving BCVA and VAS for the 12-month follow-up period. Although future controlled prospective studies are needed to further strengthen this hypothesis, immunologically safe PRGF-Endoret eye drops should be considered as a possible effective therapeutic alternative for these cases of DES from SS patients.
Footnotes
Acknowledgments
The authors thank Virginia Cuadrado for her support with the English grammar. This study received funding from the Ministry of Economy and Competitiveness of the Spanish Government, within the project denominated SURFEYE (reference RTC-2014-2375-1).
Proprietary Interests
E.A. reports that he has a licensed patent for Plasma Rich in Growth Factors.
Author Disclosure Statement
The authors declare the following competing financial interest(s): E.A. is the Scientific Director of and G.O. and F.M. are scientists at BTI Biotechnology Institute, a dental implant company that investigates in the fields of oral implantology and PRGF-Endoret technology. For all other authors, no competing financial interests exist.