
Abstract
Abstract
Purpose:
To investigate the change of serum IgG4 concentrations correlated with clinical evolution in patients with ocular adnexal marginal zone B cell lymphoma associated with IgG4-related ophthalmic disease (IgG4-ROD).
Methods:
Three consecutive patients with histopathologically confirmed ocular adnexal marginal zone B cell lymphoma associated with IgG4-ROD were evaluated. Two patients received radiotherapy and 1 patient received steroid therapy. Treatment outcome was evaluated by clinical symptoms, radiologic examination, and change of serum IgG4 level in these patients.
Results:
All patients had elevated serum IgG4 before treatment (462, 338, and 780 mg/dL respectively.) The 2 patients who received radiotherapy achieved complete remission and the serum IgG4 decreased to 345 and 92 mg/dL, respectively. The patient who underwent systemic steroid achieved partial remission and the serum IgG4 decrease to 161 mg/dL.
Conclusion:
Our study showed elevated serum IgG4 in all patients with ocular adnexal marginal zone B cell lymphoma associated with IgG4-ROD. In addition, the elevated serum IgG4 may decrease or keep stable after treatment, accompanied by improvement in clinical symptoms and reduction of lesions.
Introduction
I
Methods
We investigated 3 consecutive patients with biopsy-proven ocular adnexal marginal zone B cell lymphoma associated with IgG4-ROD, who were treated in Taipei Veterans General Hospital between 2011 and 2014. The inclusion criteria included a confirmed histopathological diagnosis of marginal zone B cell lymphoma by histological character, immunohistochemical light chain restriction or molecular heavy chain rearrangements of the IgG4-positive plasma cells, as well as a ratio of IgG4-positive/IgG-positive plasma cells more than 40% in a high-power field, and a minimum follow-up of 12 months to observe response to treatment. Clinical outcome was assessed by clinical symptoms, serial change of serum IgG4, and computed tomography (CT) imaging. This study was approved by institutional review board and conducted in accordance to the Declaration of Helsinki. Informed consent was obtained from the patients.
Result
Case 1
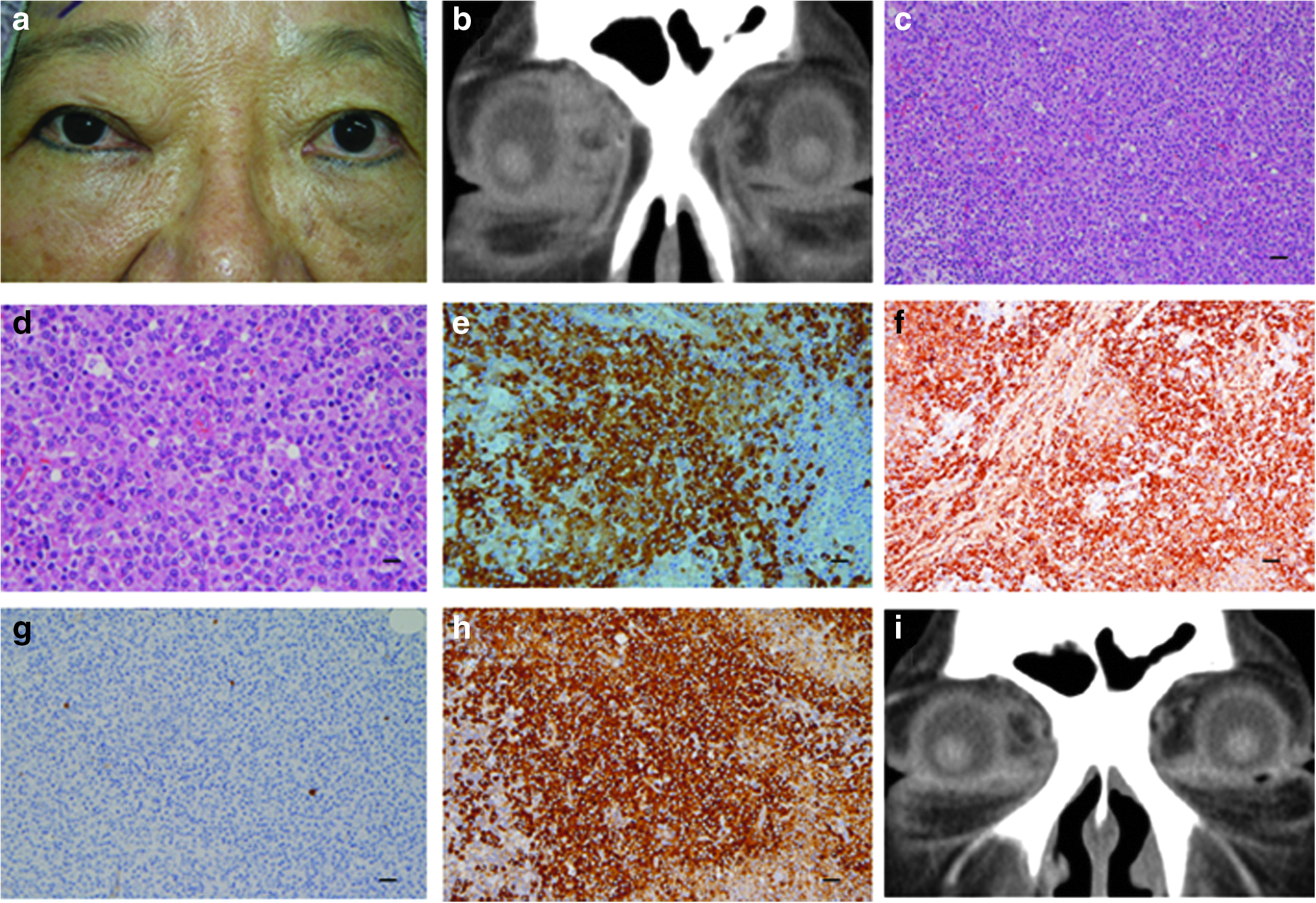
A 67-year-old female presented with progressive swelling of the right eye within 2 months (Fig. 1a). She had IgG4-RD in the left ocular adnexa 2 years ago and achieved complete remission after oral steroid and adjunctive radiotherapy. Ocular examination at this time revealed a palpable mass in the right eye and CT showed a soft tissue mass with a diameter of 17 mm at superonasal orbit of the right eye (Fig. 1b). Laboratory data at diagnosis showed that serum IgG4 was 462md/dL and the IgG4/IgG ratio was 39%. The patient underwent orbital biopsy and the pathology revealed a mature B cell neoplasm (Fig. 1c, d). Immunostaining revealed IgG4-positive plasma cells in the lesion with the IgG4/IgG ratio >90% and immunoglobulin light chain restriction of lambda (Fig. 1e–h). The histologic and immunophenotypic findings confirmed the diagnosis of an ocular adnexal marginal zone B cell lymphoma associated with IgG4-ROD. Positron emission tomography–computed tomography (PET-CT) scan showed no evidence of systemic involvement. She received radiotherapy 24 Gy in 12 fractions to right orbit fossa and 30 Gy in 15 fractions to the right orbital tumor. Radiotherapy resulted in significant clinical and radiological improvement (Fig. 1 i). No tumor recurrence was noted and her serum IgG4 concentration decreased to 345 mg/dL and the IgG4/IgG ratio decreased to 25% during the 48-month follow-up period.
Case 1:
Case 2
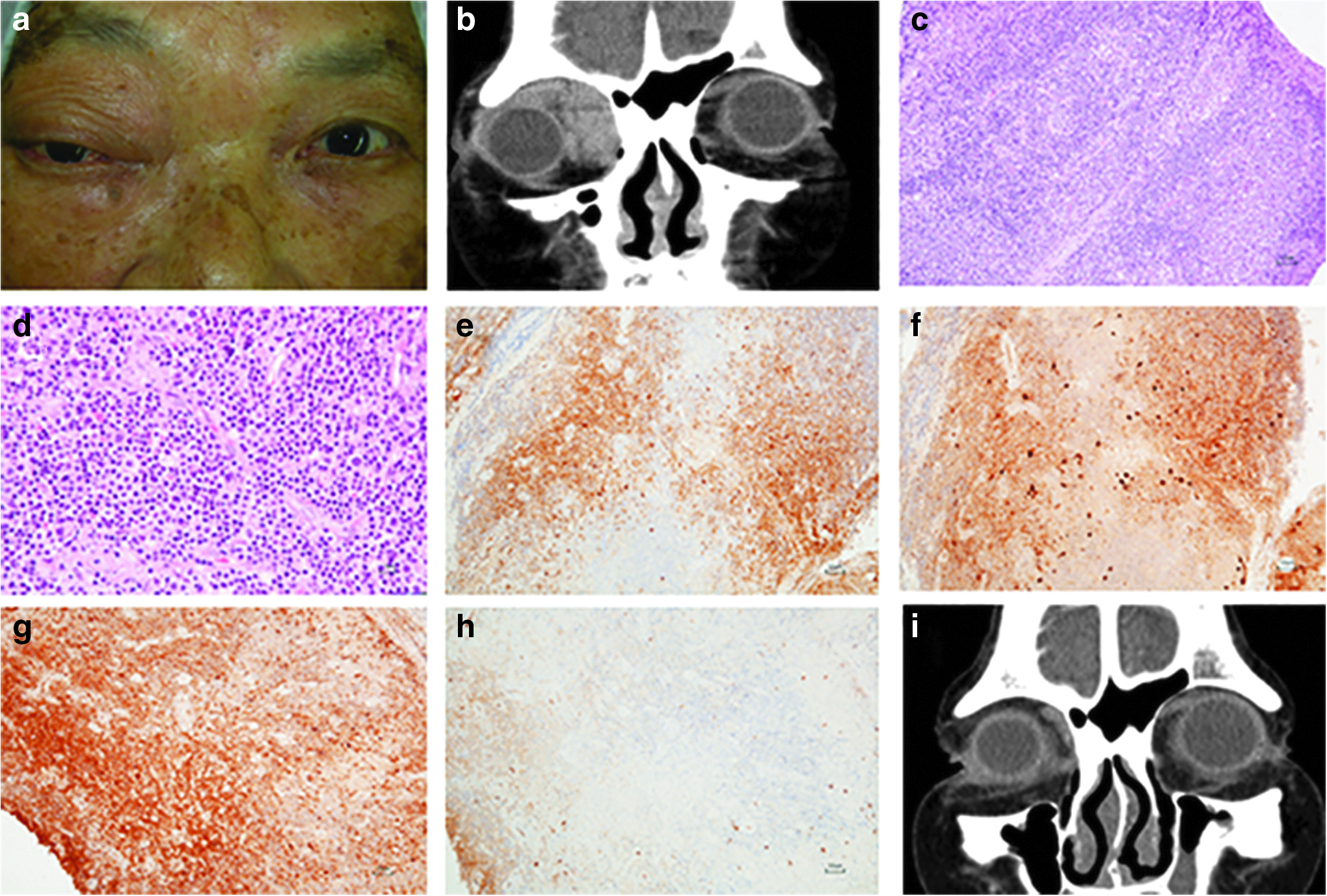
A 78-year-old female presented with proptosis and ptosis of right eye for 1 year and a palpable mass at medial orbit for 2 weeks (Fig. 2a). Ocular examination showed 3 mm of right proptosis with hypoglobus and generalized restriction of ocular motility in all gaze positions except abduction in the right eye. Orbital CT disclosed an infiltrative lesion in the right superonasal orbit with medial rectus muscle involvement (Fig. 2b). Laboratory data at diagnosis disclosed that serum IgG4 was 338 mg/dL and the IgG4/IgG ratio was 21%. The patient underwent orbital biopsy, which showed diffuse lymphoid proliferation with plasmacytic differentiation, and immunoglobulin light chain restriction of kappa, as well as abundant IgG4-positive plasma cells with the IgG4/IgG ratio >40% (Fig. 2c, –h). The diagnosis was compatible with ocular adnexal marginal zone B cell lymphoma associated with IgG4-ROD. PET-CT scan showed no evidence of systemic involvement. She then received radiotherapy 30 Gy in 15 fractions to right orbit tumor. After radiotherapy, she had experienced a marked clinical recovery on proptosis and ocular movement. A follow-up CT showed significant regression of the orbital lesion (Fig. 2i). No evidence of recurrence was noted and her serum IgG4 concentration decreased to 92 mg/dL and the IgG4/IgG ratio decreased to 5% during the 28-month follow-up period.
Case 2:
Case 3
A 67-year-old male presented with proptosis of left eye for more than 10 years with recent exacerbation (Fig. 3a). He had past history of squamous cell carcinoma of tongue after operation 11 years ago. On follow-up CT, a retrobulbar soft tissue mass, sized 25 mm in diameter, along the left optic nerve was incidentally found 9 years ago. The patient chose conservative observation for years. However, the proptosis continued to progress and a palpable mass over left superior orbit was noted recently. Hertel exophthalmometry showed left 4 mm proptosis. Orbital CT revealed a progressive enlargement of superonasal soft tissue component in the left orbit with involvement of the medial rectus muscle (Fig. 3b). Laboratory data at diagnosis showed that serum IgG4 was 780 mg/dL and the IgG4/IgG ratio was 52%. Incision biopsy revealed a diffuse monoclonal plasmacytic lymphoid proliferation and abundant IgG4-positive plasma cells (the IgG4:IgG ratio >50%) (Fig. 3c–f). The B cell clonality assay, which interrogates the immunoglobulin kappa light chain gene (IGK) and the immunoglobulin heavy (IGH) chain by a polymerase chain reaction method, showed monoclonal B cells (Biomed II commercial kit, including 3 IgH and 2 IgK) (Fig. 3 g, h). Therefore, the orbital lesion was diagnosed as ocular adnexal marginal zone B cell lymphoma associated with IgG4-ROD. PET-CT scan showed no evidence of systemic involvement. Because the patient refused to receive radiotherapy or chemotherapy, oral prednisone (30 mg/day) was started and gradually tapered based on his symptoms. Follow-up CT revealed moderate regression of left orbital lesion (Fig. 3i), and his serum IgG4 concentration decreased to 161 mg/dL and the IgG4/IgG ratio decreased to 15% during the 18-month follow-up period.

Case 3:
Discussion
IgG4 is the rarest subtype of serum IgG, which accounts for about 3–6% of total IgG in normal subjects. Elevated levels of serum IgG4 (>135 mg/dL) are commonly seen in patients with IgG4-RD, which are noted in 60% to 70% of patients with IgG4-RD and in 91% to 100% of patients with ocular adnexal IgG4-RD.6–11 However, other conditions have also been associated with high serum IgG4 levels, such as pemphigoid diseases, Churg–Strauss syndrome, multicentric Castleman's disease, and eosinophilic disorders.12–15 Although the diagnostic value of serum IgG4 levels in IgG4-RD remains uncertain, monitoring of serum IgG4 has been demonstrated to determine the disease activity of IgG4-RD and to be a useful parameter to follow the therapeutic effects and recurrence in these patients after treatment. 16 Furthermore, our prior study revealed that lower serum IgG4 and IgG4/IgG ratio at diagnosis were associated with poor response to systemic steroid in patients with ocular adnexal IgG4-RD. 11 This is the first study to report the change of serum IgG4 concentrations associated with clinical evolution in patients with ocular adnexal marginal zone B cell lymphoma associated with IgG4-ROD after treatment.
In this study, the serum IgG4 levels before treatment were significantly elevated in all patients. Kubota et al. have also disclosed that the serum IgG4 in ocular adnexal marginal zone B cell lymphoma with IgG4-positive plasma cells was significantly higher than those in the IgG4-unrelated ocular adnexal marginal zone B cell lymphoma, and similar to those of IgG4-RD. 5 Therefore, it is important to differentiate the diagnosis between IgG4-related marginal zone B cell lymphoma and IgG4-RD not only by increased serum levels of Ig-G4 and histological IgG4-immunostaining but also by immunoglobulin light chain restriction or molecular heavy chain rearrangements.
In addition, we also noted that the mean concentrations of serum IgG4 decreased from 527 to 199 mg/dL (Table 1), accompanied by a partial or complete resolution on clinical symptoms and radiological images in all patients with ocular adnexal marginal zone B cell lymphoma associated with IgG4-ROD after treatment. These findings are similar to the study of serial change of serum IgG4 on ocular adnexal IgG4-RD by Lin et al., 17 indicating a possible relationship between IgG4-related ocular adnexal marginal zone B cell lymphoma and IgG4-RD. The serum IgG4 levels were not normalized completely in case 1 and case 3. In case 1, she had a prior diagnosis of IgG4-ROD in the left eye before she developed an IgG4-related marginal zone B cell lymphoma in the right eye. Both her ocular lesions responded well to systemic steroid and adjunctive radiotherapy with no evidence of systemic involvement or local recurrence noted during a follow-up period of 48 months. However, her serum IgG4 remained to be 345 mg/dL and the IgG4/IgG ratio was about 25%. Tabata et al. also noted that serum IgG4 was not normalized among half of patients with IgG4-RD after treatment. 16 The persistent elevated serum IgG4 levels may be due to a prior or subclinical IgG4-RD with infiltration of IgG4-positive plasma cells in various organs, but did not show symptoms. In case 3, the persistent elevated serum level of IgG4 (161 mg/dL) and IgG4/IgG ratio (15%) may be due, in part, to the fact that case 3 only achieved partial response with residual ocular lesion after steroid therapy. In case 2, with good response to radiotherapy, her serum IgG4 concentration decreased to 92 mg/dL and the IgG4/IgG ratio decreased to 5%. Because of limited cases of IgG4-related marginal zone B cell lymphoma in this study and literatures, whether the persistent elevated serum IgG4 levels in these patients mean the presence of subclinical tumor lesion or inflammation required further large prospective studies.
Currently, there still remain many unknowns on the relationship between IgG4-related lymphoma and IgG4-RD. IgG4-ROD appears to have a particular association with nonHodgkin lymphoma, especially the marginal zone B cell lymphoma. 18 Based on these findings and past reports, there have been 24 cases of ocular adnexal IgG4-related marginal zone B cell lymphoma with an IgG4/IgG ratio >0.4.3–5,8,9,19,20 Among them, 2 cases arose in the site of histologically confirmed ocular adnexal IgG4-RD. 4 Interestingly, our case 1 with a past history of ocular adnexal IgG4-RD developed IgG4-related marginal zone B cell lymphoma later in the other eye. Sato et al. have reported ocular adnexal marginal zone B cell lymphoma with detected clonal rearrangement of the IGH chain gene arising from IgG4-related disease of the ocular adnexa. It suggests that marginal zone B cell lymphoma could arise in a background of IgG4-related chronic inflammation by clonal expansion of IgG4+ plasma cells.3,18 Sato et al. also reported an IgG4-producing marginal zone B cell lymphoma of the lymph node, indicating that not only can malignant lymphomas occur in the setting of IgG4-RD but also IgG4-producing cells can be neoplastic. 21 Ohno et al.'s study found that a significant subset of ocular marginal zone B cell lymphoma (IgG4 associated) might raise IgG4-RD, and they both exhibited significantly higher expression ratios of similar inflammatory cytokines. 22 Nevertheless, whether ocular adnexal IgG4-related marginal zone B cell lymphoma arises from preexisting IgG4-ROD or IgG4-related marginal zone B cell lymphoma can initiate an immunologic response with subsequent infiltration of IgG4-positive plasma cells requires further investigation.
Because of limited cases of IgG4-related marginal zone B cell lymphoma in this study and literatures, the optimal treatment has not been well established. However, the management of patients with ocular adnexal marginal zone B cell lymphoma is often according to the disease stage. Patients with localized lymphoma are most commonly treated with radiotherapy. 23 Because 1 of our patients (case 3) refused to receive radiotherapy, oral prednisone was used, which achieved partial response in the patient. The effect of steroid in case 3 may be attributed partially to these findings consistent with both an autoimmune disorder and an allergic disorder in IgG4-RD.
In conclusion, we reported elevated serum levels of IgG4 in 3 patients with ocular adnexal marginal zone B cell lymphoma associated with IgG4-ROD. The elevated serum IgG4 in these patients could decrease or keep stable after radiotherapy or systemic steroid, along with improvement in clinical symptoms and reduction of the ocular lesions.
Footnotes
Acknowledgment
This study was partially supported by grants (V106C-008) from the Taipei Veterans General Hospital, Taiwan.
Author Disclosure Statement
No competing financial interests exist.