
Abstract
Abstract
Purpose:
To investigate PTSgels (Pentablock copolymers) as an injectable formulation technology for sustained ocular drug delivery. Drug release profile, tolerability, and polymer degradation for one of the thermosensitive, biodegradable, and biocompatible compositions were investigated through intracameral (IC) injection in rabbits.
Methods:
New Zealand White rabbit eyes were injected IC (50 μL) with 100 μg near-infrared-immunoglobulin G (NIR-IgG) in balanced salt solution (BSS) or 20% PTSgel; or with PTSgel or BSS alone. Ocular irritation scoring, intraocular pressure (IOP), and corneal thickness (CT) measurement, as well as color and infrared photography, were performed for up to 28 days postinjection. Upon euthanasia at 7, 14, or 28 days, eyes underwent ex vivo imaging (Xenogen IVIS) followed by tissue fixation and histopathology.
Results:
IC injection of PTSgel (liquid at room temperature) was performed without difficulty using a 31G needle. The polymer quickly gelled in the IC space resulting in an inferior anterior chamber deposit. The tested PTSgel was well tolerated, with no significant changes in IOP or CT. Eyes injected with NIR-IgG in PTSgel had visible NIR-IgG through 9 days postinjection, and ex vivo imaging detected a strong NIR-IgG signal in the anterior chamber through day 28. The gel deposit steadily decreased in size over time and was nearly eliminated by 28 days.
Conclusions:
The PTSgel released IgG for 28 days and was well tolerated. The polymer degraded in parallel with drug release. These results demonstrate the potential of intracameral PTSgel formulations for sustained delivery of biologic therapies to the ocular anterior segment.
Introduction
M
Several ocular-sustained drug delivery systems have been investigated, but most often require surgical implantation or do not have a predictable and controlled rate of drug delivery, limiting their clinical use. 6 Therefore, products that provide sustained release of ocular therapeutics with controlled release without the need for surgery would be highly beneficial.
Recent advancements in hydrogels appear to have overcome some of the aforementioned challenges. Hydrogels are aqueous solutions, which when exposed to certain external stimuli such as pH or temperature, form a deformable gel depot, from which a therapeutic concentration of drug is released over time into the surrounding tissue.
7
However, such gels have had issues regarding biocompatibility and protein degradation. One commonly used copolymer, poly (
A variety of thermosensitive gels have been developed using different block copolymers such as poly ethylene glycol (PEG), PLGA, poly (
Recently, we have obtained promising results for the sustained release of immunoglobulin G (IgG) as a model drug molecule from PTSgel compositions following subcutaneous injection. 14 PTSgels are thermosensitive gels consisting of mPEG, PCL, and PLA biodegradable polymer blocks. PTSgels can be easily injected through a small-gauge needle (31G), form a gel depot in situ, are biocompatible, and provide sustained release of IgG in vitro and in vivo while maintaining the chemical and biological integrity of the protein. In addition, PTSgels have the added benefit of allowing 100% drug loading without use of an organic solvent, thus avoiding loss of drug and ensuring a therapeutic concentration over an extended period of time even if required doses are high.14,15 PTSgels, therefore, can be used to create thermosensitive, biodegradable, and biocompatible formulations for sustained ocular delivery of biologic agents and other hydrophobic and hydrophilic molecules, for which the data are not included in this study.
PTSgels have been evaluated for release of IgG in vivo and in vitro. 14 By tailoring the PTSgel block composition and aqueous gel percentage, IgG can be released in a controlled manner from several days to several months in vitro. 14 The in vitro release parameters also have been correlated to in vivo release. A PTSgel (10GH) in a previous study provided a 10–14-day release of IgG in vitro, and also following subcutaneous injection in mice, released near-infrared (NIR)-IgG for up to 12 days. 14 The same PTSgel (10GH) has been tested in the current investigation.
The purpose of this study was to evaluate ocular tolerability and sustained antibody delivery of the model drug IgG, using pentablock thermosensitive gel (PTSgel), injected intracamerally (IC) in normal New Zealand White (NZW) rabbits.
Methods
PTSgel synthesis and characterization
PTSgels with PEG-PCL-PLA-PCL-PEG block arrangements were synthesized and characterized as previously described.14–16
In brief, a diblock copolymer was synthesized by ring-opening copolymeriziation of ɛ-caprolactone with monomethoxy PEG in the presence of tin octoate as a catalyst. The resulting diblock copolymer was similarly converted to triblock with
Sol–gel testing at 37°C
The sol (flow)–gel (no flow) of PTSgel was examined by following a previously published protocol. 14 In brief, the polymers were dissolved in PBS buffer (pH 7.4) at 25 wt% concentration. A 0.5 mL of aqueous polymeric solution was transferred into an 8 mL glass vial and placed in water bath maintained at 37°C. Vials were incubated for 5 min at 37°C. Gel formation was observed visually by inverting the tubes, immediately after removal from the water bath. In addition, temperature of soluble gel transition was determined for 25% 10GH PTSgel. The polymer solutions were gently vortexed and 200 μL of each sample was added to a microwell plate (costar) in triplicate. The plate was put into the plate reader (Synergy 2; Biotek) and the absorbance of each sample read at 550 nm. The plate was then read after a 15-min incubation at each of the following temperatures: 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, and 40°C. The average absorbance of each polymer at each temperature was plotted.
Intracameral injection
All protocols were conducted according to the ARVO Statement for the Use of Animals in Ophthalmic and Vision Research. In addition, use of animals in this study was approved and monitored by the North Carolina State University Institutional Animal Care and Use Committee (IACUC).
NIR dye labeled IgG (IRDye800CW) was purchased from LICOR Biosciences, Lincoln, NE. NIR-IgG in PTSgel (10GH) or balanced salt solution (BSS) was prepared by adding 500 μL of cold PTSgel (20% final polymer concentration in aqueous solution) or BSS to 1 mg of lyophilized NIR-IgG, resulting in a 0.2% final NIR-IgG concentration. The prepared solutions were gently vortexed and stored at 4°C until use. The solutions were used within 24 h of preparation. After general anesthesia and aseptic surgical preparation, 50 μL of solution using a 31-gauge needle was injected through the temporal limbus into the anterior chamber of normal, adult NZW rabbits. The rabbits were injected with either BSS, 100 μg of NIR-IgG in BSS, 20% PTSgel, or 100 μg of NIR-IgG in 20% PTSgel. In vivo tolerability was evaluated by monitoring intraocular pressure (IOP), Hackett–McDonald ocular irritation scores (via slit lamp biomicroscopy), and central corneal thickness (CT). IOP was measured using a rebound tonometer (TonoVet®, icare, Tiolat, Helsinki, Finland) with a disposable probe held horizontally, 4–5 mm from the corneal surface. CT, an indirect method of evaluation of corneal endothelial cell toxicity,17,18 was measured using a handheld ultrasound pachymeter (PachPen, Accutome, Lynwood, WA). Evaluation of tolerability as well as color (Nikon D7100; Nikon Corporation, Tokyo, Japan) and infrared photography (Nikon D300s; Nikon Corporation, Tokyo, Japan) were performed before the injections and then at 1, 2, 3, 4, 5, 7, 10, 14, 21, and 28 days after injection. The size of the gel deposit was measured over time using ImageJ software (National Institutes of Health, Bethesda, MD).
Rabbits were serially euthanized and eyes collected on 7, 14, and 28 days postinjection. Immediately after collection, each eye underwent ex vivo imaging (IVIS, Xenogen, Alameda, CA) using Indocyanine Green (ICG) settings, as previously described. 14 NIR-IgG fluorescence was quantified using the IVIS imaging software automatic region of interest setting to calculate the radiant efficiency of the NIR-IgG signal in the anterior chamber of each eye. Each eye was then fixed in 10% Davidson's solution, processed for histopathology, stained with hematoxylin and eosin, and examined using light microscopy.
Results
PTSgel synthesis and characterization
For the purposes of this study, a thermosensitive PTSgel polymer was synthesized and designated PTSgel 10GH. Other PTSgels with differing release parameters have been developed and reported elsewhere. 14 The 10GH PTSgel was constructed with different block sizes of m-PEG, PCL, and PLA with PLA in the center of the molecule (PEG550-PCL500-PLA1000-PCL500-PEG550). The molecular weight of PTSgel 10GH was 3100 Da and transitioned from liquid phase to gel at 37°C (Fig. 1). As described before, 14 the NMR and FTIR data confirmed the structural composition and PDI of 1.08 indicated a good quality synthesis with little dispersity in the molecular weight.
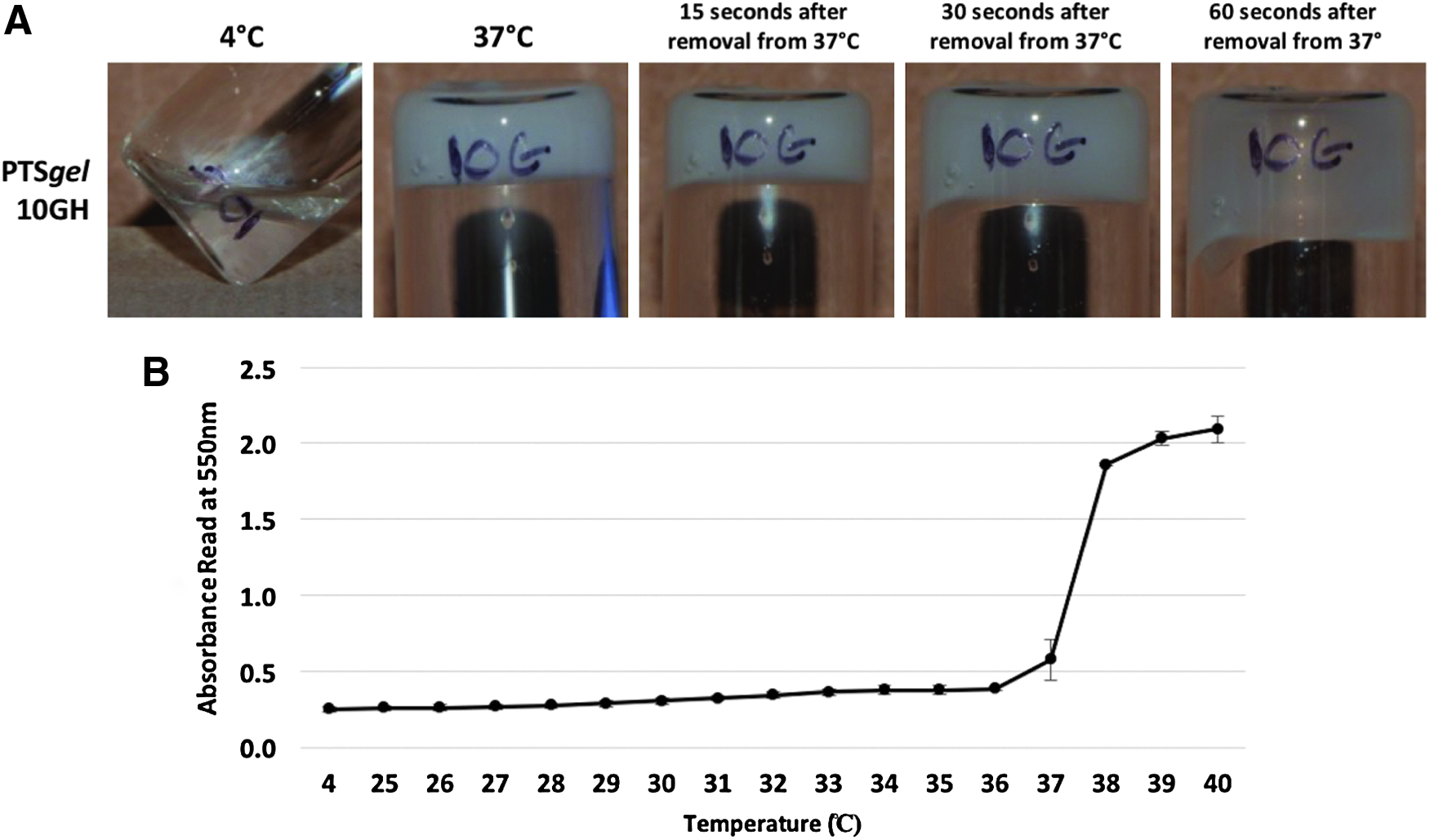
Sol–gel testing of 20% PTSgel 10GH.
Intracameral injection
Tolerability of PTSgel postintracameral injection
Five NZW rabbits were used in this study. Two eyes were injected with BSS alone, 1 eye with NIR-IgG in BSS, 4 eyes with PTSgel alone, and 3 eyes with NIR-IgG in PTSgel. Intracameral injection of PTSgel was performed without difficulty using a 31G needle and was well tolerated by the eye. No significant difference in IOP (Fig. 2) or CT (Fig. 3) was observed between treatments.
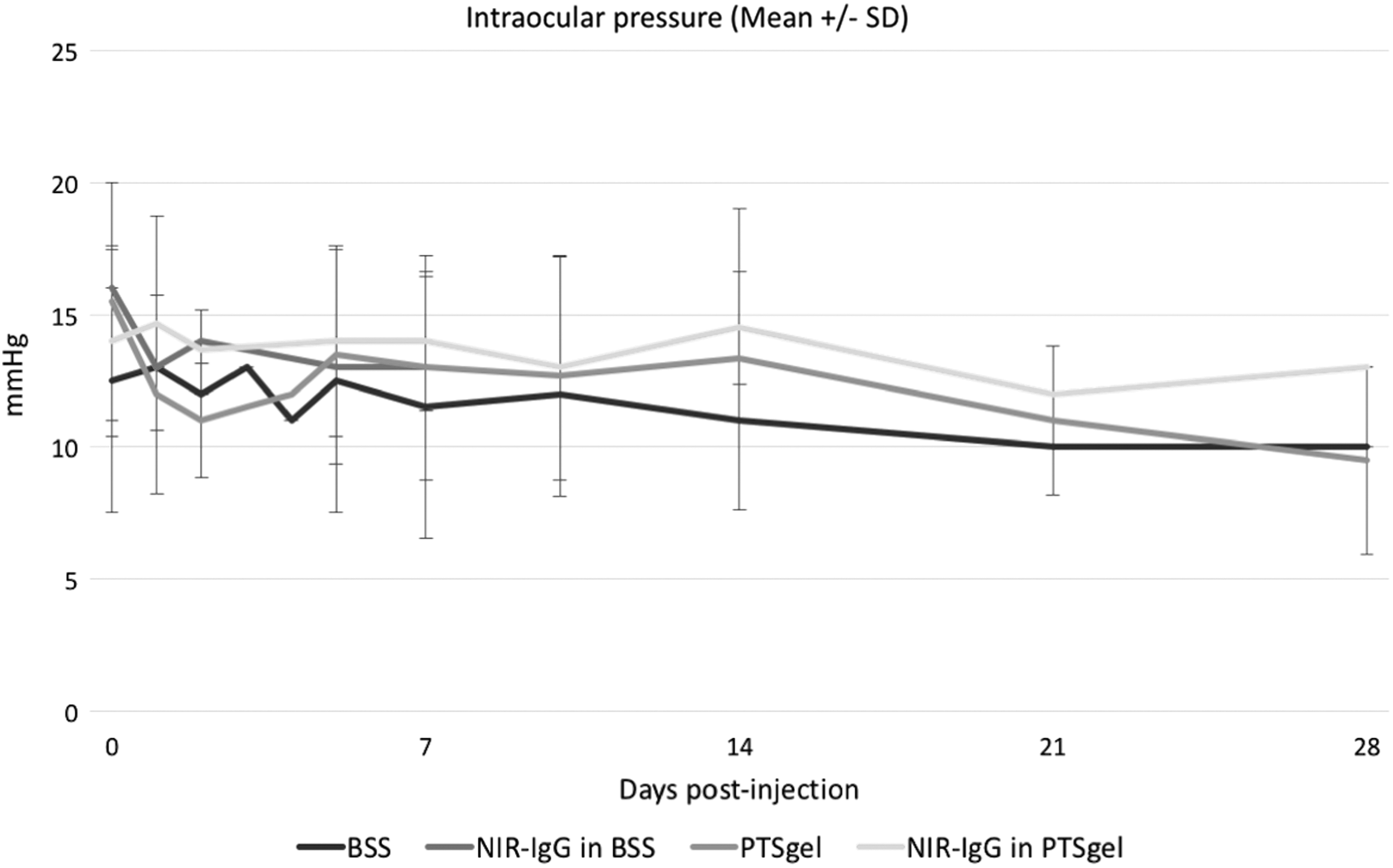
IOP (mean ± SD) after injection with 50 μL of BSS, 0.2% NIR-IgG in BSS, PTSgel, or 0.2% NIR-IgG in PTSgel. There was no significant difference in IOP between groups throughout the study. BSS, balanced salt solution; IOP, intraocular pressure; NIT-IgG, near-infrared-immunoglobulin G.

Central corneal thickness (mean ± SD) after injection with 50 μL of BSS, 0.2% NIR-IgG in BSS, PTSgel, or 0.2% NIR-IgG in PTSgel. There was no significant difference in central corneal thickness between groups throughout the study.
A mild, transient inflammatory response following injection was observed in all eyes. The ocular irritation scores for the BSS group peaked at 1 day postinjection and the PTSgel at 5 days postinjection, with a mean (±SD) ocular irritation score of 0.5 (±0.7) and 3.25 (±0.5) in the BSS and PTSgel groups, respectively. Peak ocular irritation scores occurred 1–3 days postinjection in eyes receiving NIR-IgG in BSS [cumulative score of 8 (±0.5)] and NIR-IgG in PTSgel [cumulative score of 6.3 (±0.6)]. This suggests that the NIR-IgG resulted in a transient ocular inflammation as it was not observed with BSS or PTSgel alone (Fig. 4).
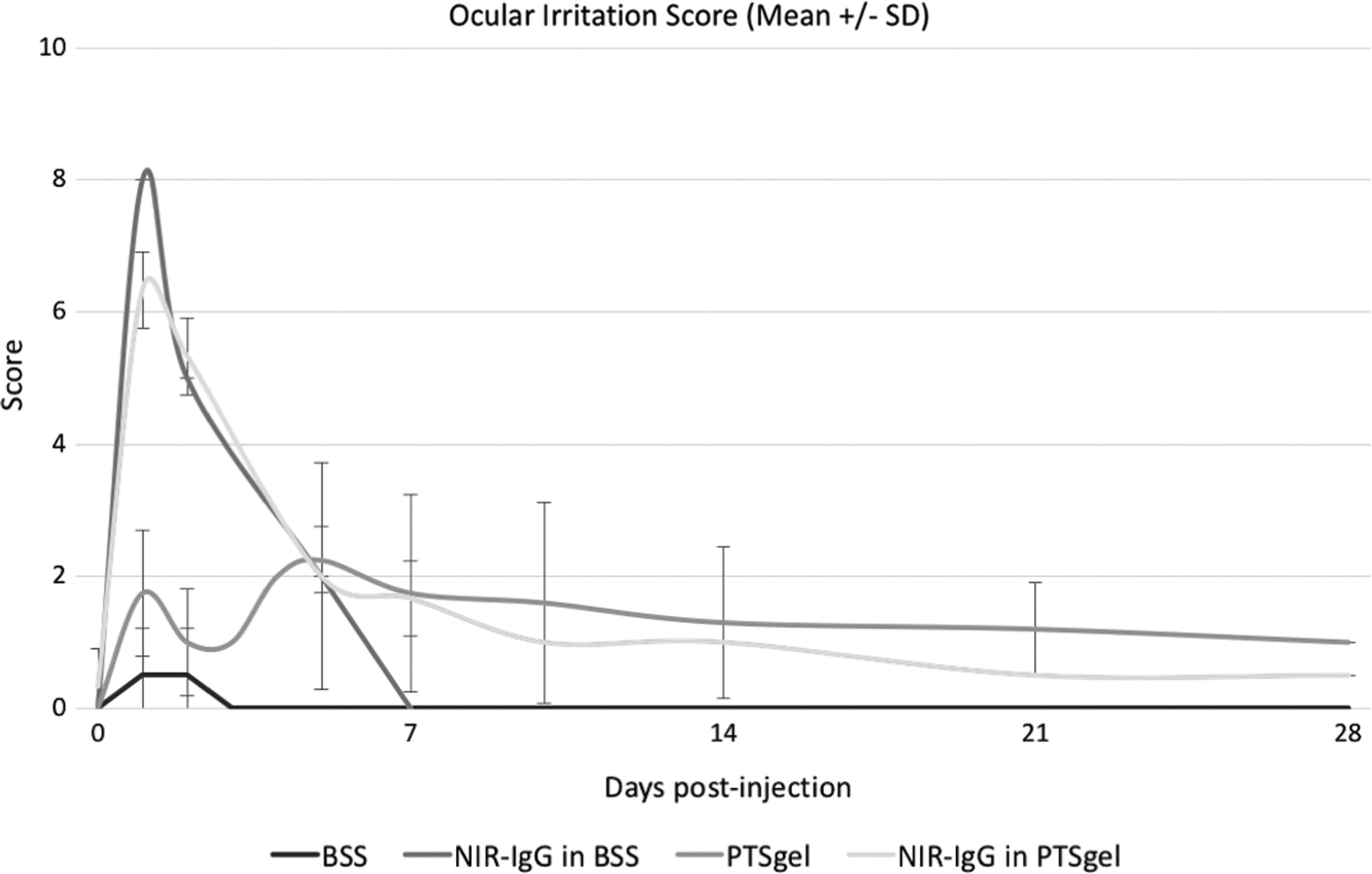
Mean cumulative ocular irritation scores (mean ± SD) after injection with 50 μL of BSS, 0.2% NIR-IgG in BSS, PTSgel, or 0.2% NIR-IgG in PTSgel. Peak ocular irritation scores occurred 1–3 days postinjection in eyes receiving NIR-IgG in BSS [cumulative score of 8 (±0.5)] and NIR-IgG in PTSgel [cumulative score of 6.3 (±0.6)]. This suggests that the NIR-IgG resulted in a transient ocular inflammation as it was not observed with BSS or PTSgel alone.
NIR-IgG visualization and polymer disintegration
PTSgel was visible as a focal deposit in the inferior anterior chamber in eyes injected with PTSgel by day 1 postinjection (Fig. 5). The gel deposit steadily decreased in size over time and was nearly eliminated by 28 days postinjection (Fig. 6). Infrared photography revealed visible NIR-IgG as granular deposits in the anterior chamber. In eyes injected with NIR-IgG in BSS, the IgG was visible only immediately after injection and was negative by 24 h after injection. The NIR-IgG was visible through 9 days postinjection in eyes injected with NIR-IgG in PTSgel. No NIR-IgG was detected in eyes injected with only BSS or PTSgel (Fig. 7).

PTSgel 10GH in the anterior chamber. PTSgel was visible as a focal deposit in the inferior anterior chamber (arrow) at 1 day postinjection.
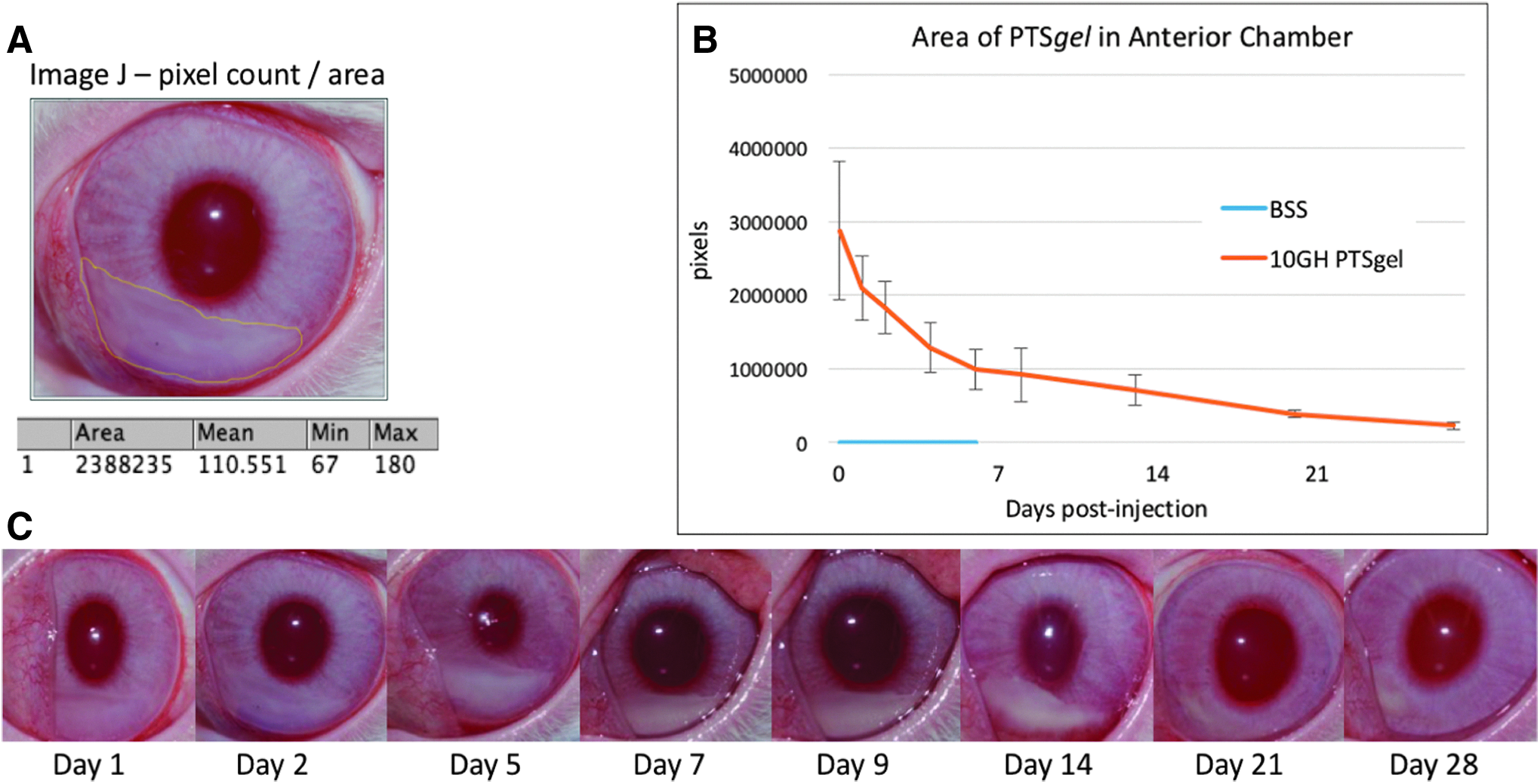
Degradation of PTSgel in the anterior chamber. The gel deposit steadily decreased in size over time and was nearly eliminated by 28 days postinjection.

Infrared photography of PTSgel 1 day after injection.
Ex vivo imaging for NIR-IgG sustained release
Ex vivo IVIS imaging revealed a strong signal of NIR-IgG in the anterior chamber of eyes injected with NIR-IgG in PTSgel. The signal gradually decreased over time through day 28, and no signal was detected in eyes receiving NIR-IgG in BSS or those receiving PTSgel or BSS alone. Quantification of the NIR-IgG fluorescence signal demonstrated a decrease in radiant efficiency at each time point, indicating steady release of IgG from the PTSgel over time (Fig. 8).
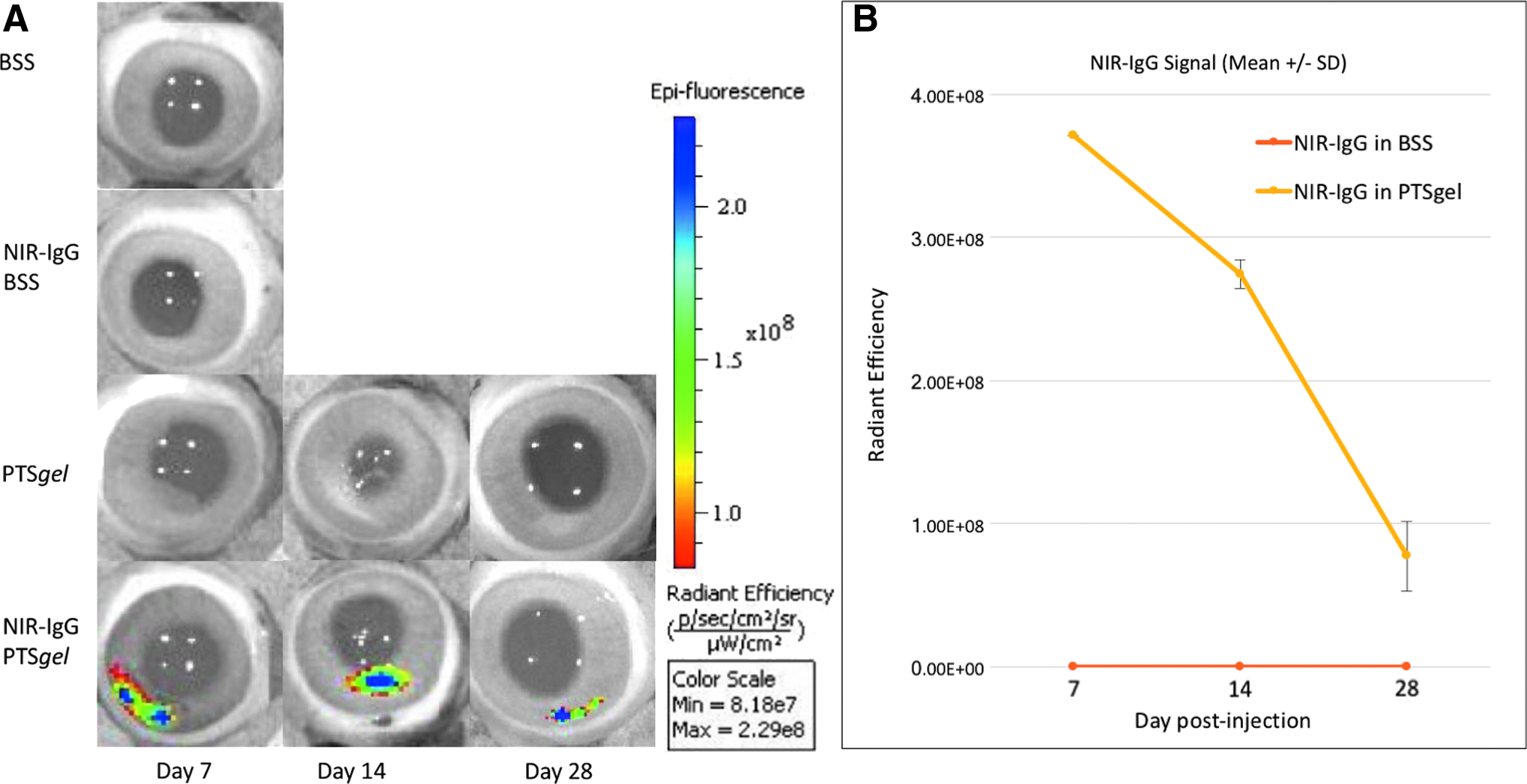
Ex vivo imaging of the anterior chamber after various treatments.
Safety evaluation via histopathology
After the eyes were collected and imaged, they were processed for histopathology and evaluated via light microscopy. In 1 eye injected with PTSgel and collected on day 7 postinjection, a mild inflammatory response was observed infiltrating the iridocorneal angle with a focal neutrophilic infiltrate on the anterior iris, but a gel depot was not visible in this eye on histopathology. In eyes receiving PTSgel, a small depot of PTSgel could be visualized in the inferior anterior chamber up to 28 days postinjection. The gel depot was mildly infiltrated with mononuclear cells with mild inflammation surrounding the depot. A mild mixed population of inflammatory cells was noted in the inferior iridocorneal angle in eyes receiving BSS alone and collected on day 28 (Fig. 9).
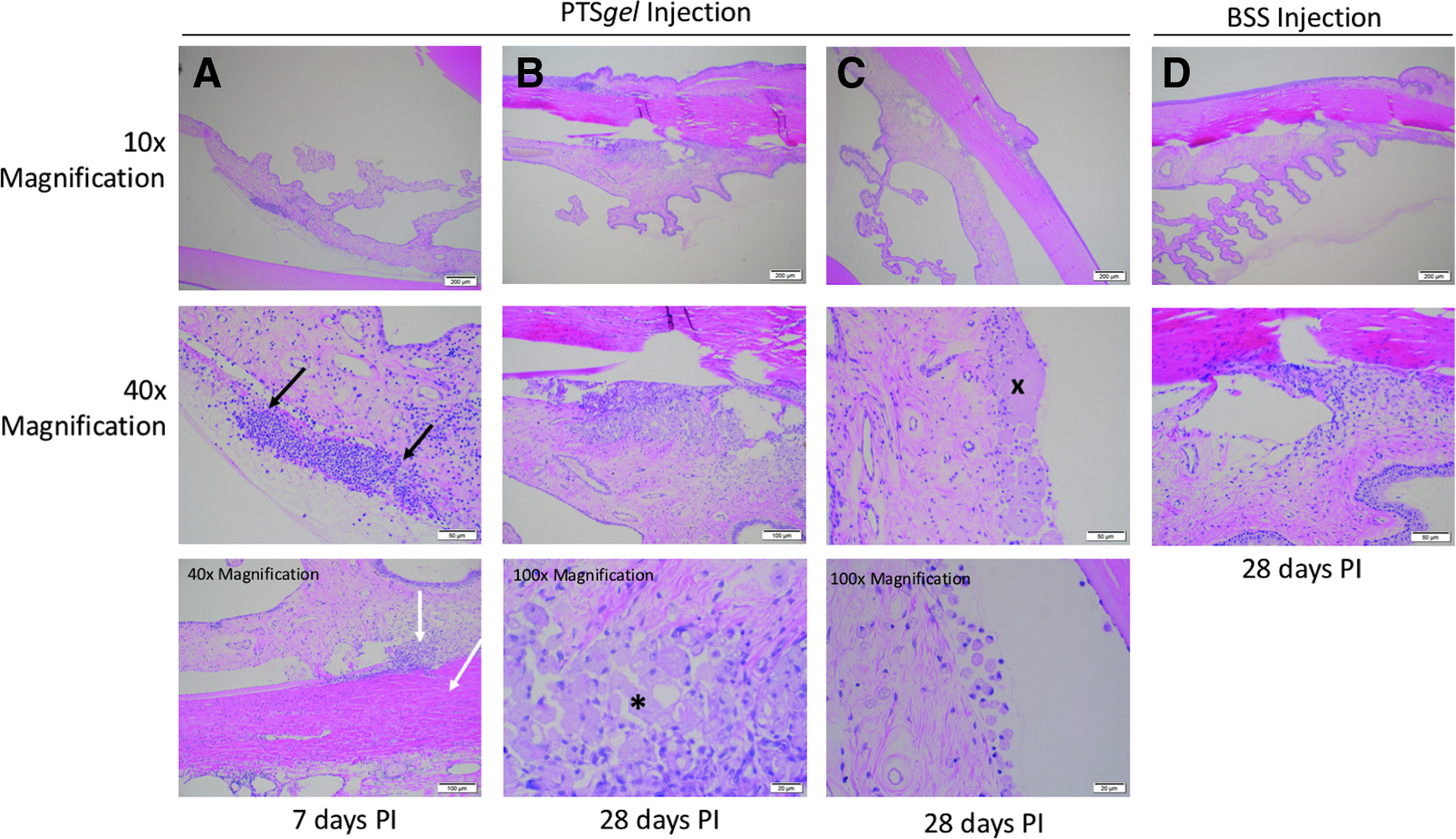
Ocular histopathology after intracameral injection of PTSgel. In 1 eye injected with PTSgel and collected on day 7 postinjection
Discussion
We have demonstrated that injection of PTSgel 10GH (while liquid at room temperature) into the anterior chamber of rabbits can be performed easily through a 31-gauge needle, forming a gel in the inferior anterior chamber that is well tolerated, and releases IgG for up to 28 days. For other thermosensitive gels, a documented disadvantage has been reported due to the possibility of solution–gelation (sol–gel) transition during handling or injection, making injection difficult or impossible. 6 This was not noted in the present study as the PTSgel was easily injected through a 31-gauge needle, despite handling of the syringe before injection, and a solid gel deposit was immediately created in the inferior anterior chamber after injection.
Intracameral injection of sustained drug delivery of high drug load (100 μg IgG) with a low injection volume, injectability through a 31-gauge needle, and biodegradability to obviate the need for surgical removal were all achieved with the PTSgel. The PTSgel provided a sustained ocular delivery of IgG for ∼28 days in normal rabbits. It has been shown in the literature that copolymers containing PCL have a faster release of protein biologics than the rate of gel degradation, leaving behind a shell of nondissolved gel.19,20 However, in this study, in vivo observation of only a small remnant of gel remaining in the anterior chamber after 28 days at the time of euthanasia correlated with the presence of a strong NIR-IgG signal visible on ex vivo IVIS imaging, indicating that the steady degradation of PTSgel paralleled the release of IgG in vivo. This is advantageous because at repeated dosing at the time of drug exhaustion, there would not be accumulation of drug-depleted gel within the anterior chamber.
PTSgels have previously been evaluated for release of IgG subcutaneously and in vitro. 14 The PTSgel (10GH) used in that study resulted in a 10–14-day release of IgG in vitro and a 12-day release of NIR-IgG following subcutaneous injection in mice. The ocular in vivo IC drug release appears to be slower than in vitro or after subcutaneous injection, possibly due to slower diffusion and/or metabolic turnover in the eye. However, after IC injection, IgG release paralleled the in vivo degradation in situ. Furthermore, different polymer concentrations and compositions other than 10GH of PTSgel can be developed to modulate the release of proteins or small hydrophobic and hydrophilic molecules. In an earlier publication, we demonstrated release from days to several weeks using PTSgels in vivo, injected subcutaneously. 14
While the current study focused on antibody protein, it is likely that suitably tailored PTSgels can also provide sustained release for small-molecule ocular therapies. In our laboratory, we have obtained promising results for the sustained delivery of pazopanib, brinzolamide, cyclosporine, and difluprednate from various compositions of PTSgels for release in vitro (unpublished data). Of note, these molecules could be dissolved or suspended in PTSgels in relatively high concentration (up to 4%), despite their hydrophobic nature. Thus, one might hypothesize that these drugs would provide a sustained in vivo release profile and thus allow for a large variety of ocular drugs to be used with PTSgels. Sustained delivery of drugs to the anterior chamber of the eye may have benefit for treatment of glaucoma, through direct delivery to the trabecular meshwork or ciliary epithelium, uveitis, through direct tissue exposure to the iris or ciliary body, or for treatment of posterior corneal diseases (i.e., corneal endothelial disease).
The PTSgel used in this study was well tolerated with only a mild and transient inflammatory reaction noted in all eyes regardless of treatment group. The Hackett–McDonald ocular irritation scores were temporarily higher in eyes receiving NIR-IgG in BSS or in PTSgel compared with eyes receiving BSS or PTSgel alone, suggesting that the NIR-IgG or a component of the dye was the cause of the irritation observed rather than the PTSgel itself.
IgG, a full-length antibody with a molecular weight of 150 kDa, is commonly used as a model for sustained delivery of protein therapeutics. It is reasonable to hypothesize that biologics similar to the model IgG used in this study, such as bevacizumab (149 kDa), would behave similarly in vivo. 21 Although we demonstrated that IgG remained in the PTSgel in vivo for the duration of the study, we did not evaluate in vivo pharmacokinetics of the release of IgG from the gel. Further studies are needed to determine the pharmacokinetics and pharmacodynamics of specific ocular therapeutics using PTSgel. Ocular tissue distribution needs to be performed separately for each drug that is to be delivered using this drug delivery system.
Conclusions
The PTSgel composition (10GH) used in the in vivo testing was well tolerated, provided sustained release of IgG, and was largely eliminated from the anterior chamber by 28 days. These results support continuing investigations on using PTSgel for sustained delivery of therapies (biologics and small molecules) for ocular anterior and posterior segment diseases.
Authors' Contribution
E.S., S.S., J.S., and S.A. have no proprietary interest; R.A. and B.G. have financial interest in i-novion, Inc.; S.W., U.G., and P.V. are the cofounders of i-novion, Inc.
Footnotes
Author Disclosure Statement
No competing financial interests exist.