
Abstract
Abstract
Purpose:
To evaluate the effect of intravitreal dexamethasone implant (Ozurdex) treatment on serous macular detachment (SMD) in patients with nonischemic central retinal vein occlusion (CRVO).
Methods:
Retrospective, interventional, noncomparative case series was conducted. Twenty-four eyes of 24 patients with macular edema (ME) and SMD secondary to nonischemic CRVO made up the study population. Patients who had received intravitreal triamcinolone and/or antivascular endothelial growth factor treatment and/or had undergone retinal photocoagulation were excluded from the study. After Ozurdex injection, visual and anatomical responses were observed.
Results:
The mean follow-up time was 9.96 ± 2.44 months (minimum 7, maximum 14). After injection of Ozurdex, ME and SMD regressed except for 1 patient. Twenty cases showed relapse within a 5.45 ± 1.43 months mean time. Seventeen of them had SMD. Eight cases revealed a second relapse and 1 case revealed a third relapse after retreatments. The mean time for the second relapse was 5.50 ± 1.19 months. The height of SMD was found to be lower in all follow-up examinations—including relapses—than baseline measurements. The median SMD value decreased from 247.5 μm (minimum 80, maximum 745) at baseline to 0 μm (minimum 0, maximum 426) at the final examination (P < 0.001). No eyes lost vision at any control visit. The mean best corrected visual acuity increased from 0.89 ± 0.31 logMAR at baseline to 0.62 ± 0.31 logMAR at the final examination (P < 0.01). No local or systemic complication was observed.
Conclusion:
In this case series, Ozurdex was found as a safe and effective treatment for SMD and ME associated with nonischemic CRVO.
Introduction
R
Meanwhile, a number of clinical features such as the site of obstruction, status of macular perfusion, integrity of the ellipsoid zone, initial visual acuity, time to initial treatment, and previously applied treatments were found to influence treatment outcomes.10–12 Furthermore, optical coherence tomography (OCT) images showed that RVO did not create a uniform lesion in the macula. One of the most frequent lesions in RVO is the serous macular detachment (SMD). 13
SMD, which is associated with several ischemic, inflammatory, and neoplastic diseases, was described in patients with central retinal vein occlusion (CRVO) first by Weinberg et al. 14 Ozdemir et al. 15 showed that SMD is present on OCT more commonly than often recognized clinically. In their study, 81.8% of eyes with CRVO had SMD. The presence of SMD has been found to indicate poor visual prognosis in retinal vascular diseases and >1 pathogenetic mechanisms are suggested for this.16–19 However, there are a limited number of studies that assess treatment outcomes in eyes with SMD.20,21
The aim of this study was to evaluate the effects of intravitreal Ozurdex implant on treatment-naive SMD secondary to nonischemic CRVO.
Methods
A retrospective review was conducted on all patients who underwent intravitreal Ozurdex injection for ME secondary to CRVO at Bezmialem Vakif University, Istanbul, from September 2014 to October 2015. The patients matching the following criteria were included in the study: the presence of ME and SMD secondary to nonischemic CRVO during fundus examination and confirmed with fluorescein angiography or OCT; the presence of SMD detected by OCT; no evidence of ocular diseases that may cause ME or SMD, such as diabetic retinopathy, uveitis, macular pucker, or vitreomacular traction; and no evidence of glaucoma or ocular hypertension.
After obtaining a detailed ophthalmic and medical history, all patients underwent a comprehensive ophthalmic examination, including best corrected visual acuity (BCVA) measurement with Snellen chart, slit lamp biomicroscopy, indirect ophthalmoscopy with a 90-diopter precorneal lens, and a Goldmann 3-mirror contact lens. The patients suspected with the presence of CRVO underwent color fundus photography, fluorescein angiography, and spectral domain optical coherence tomography (SD-OCT).
Fundus photographs and fluorescein angiograms were obtained with a Zeiss VISUCAM 500 fundus camera (Carl Zeiss Meditec AG, Jena, Germany). OCT examinations were performed using a spectral domain-OCT (Heidelberg Engineering, Heidelberg, Germany) with standard SD-OCT scans (512 A-scans, 20 × 15°). The primary criterion for ischemic and nonischemic differentiation was the presence of at least 10 disk areas of retinal capillary obliteration, in accordance with the central vein occlusion study. 22
Central foveal thickness (CFT) was defined as the length between the inner retinal surface and the outer retinal surface. SMD was evident if the posterior surface of the retina was elevated over a nonreflective cavity with minimal shadowing of the underlying tissues. The distance between the outer retinal and the pigment epithelial surface at the fovea was measured for the height of the SMD.
The disease duration should have been <8 weeks for study entry. Patients who had received IVTA and/or anti-VEGF treatment and/or had undergone retinal photocoagulation and patients with visually significant cataracts or other disturbances of the eye that prevented a detailed fundus examination and tests were excluded from the study.
Ozurdex implant was injected with a customized, single-use 22-gauge applicator, through the pars plana into the vitreous cavity of all patients. All injections were performed under sterile conditions in an operating room. After the treatment, ofloxacin 0.3% eye drops were prescribed 4 times a day for 1 week.
Baseline parameters included visual acuity, intraocular pressure (IOP), and macular and SMD thickness at the central fovea. Patients were examined on days 1 and 7. Thereafter patients were followed monthly. The change of BCVA, CFT, height of SMD, and the resolution of the SMD was evaluated. Potential corticosteroid-induced and injection-related complications were also observed.
Retreatment with Ozurdex was performed for relapses on a pro re nata basis. Relapse was defined as a recurrence of ME on OCT scanning associated with a loss of BCVA of at least 1 line.
All procedures were conducted in accordance with the Declaration of Helsinki and a written informed consent was obtained from all participants in the study. The data analysis was done after the approval of the local university ethics committee (approval number and date: 4/17–February 24, 2016).
Statistical analyses were performed using the Statistical Package for Social Sciences version 20.0 (SPSS, Inc., Chicago, IL). All numerical data are expressed either as the median (minimum–maximum) or as the mean ± standard deviation. All categorical variables are expressed as number and percentage (n, %). An assessment of normality was done with Kolmogorov–Smirnov test initially. A paired t-test or one-way analysis of variance test was used for normally distributed data, whereas Wilcoxon signed rank test or Friedman test for non-normally distributed data, to compare the BCVA, CFT, and height of SMD values before the treatment and at follow-ups after treatment, was used.
Results
A total of 24 consecutive eyes of 24 patients (14 women and 10 men; mean age: 67.66 ± 8.67 years) with SMD secondary to nonischemic CRVO were examined in this series. The right eye was involved in 14 patients (58.3%) and the left eye in 10 patients (41.7%). A history of hypertension was present in 20 patients (83.3%), and a history of smoking was present in 17 patients (70.8%). No patient had diabetes mellitus (Table 1). All patients were classified as perfused. No patient had an afferent pupillary defect, cotton-wool spots, angiographic areas of capillary nonperfusion, iris neovascularization, or vessels in the angle. ME and height of SMD were documented as a mean ± standard deviation (SD) of 4.1 ± 1.1 days before intravitreal Ozurdex injection. Before Ozurdex injection, no eyes had been treated with systemic or local medication and laser photocoagulation. The follow-up period ranged from 7 to 14 months (mean ± SD, 9.96 ± 2.44 months).
SD, standard deviation.
At baseline, all eyes in the study had ME and SMD. ME and SMD regressed in all eyes except for 1 patient after Ozurdex injection. One eye that had not responded to Ozurdex received IVR treatment twice but it did not respond to ranibizumab either, and the patient discontinued the treatment at the 7-month follow-up. Three eyes (12.5%) remained relapse free over the entire follow-up (7, 8, and 12 months) after a single Ozurdex injection and required no additional treatments.
Seven cases showed first relapse at the 4-month follow-up. Six of them had SMD. At the 5-, 6-, 7-, and 8-month follow-ups, the other 13 cases showed a first relapse and 11 of them had SMD. Retreatment was performed for these patients, and ME and SMD regressed in all eyes. The mean time for the first relapse was 5.45 ± 1.43 months. Eight cases revealed second relapse and 1 case revealed third relapse after retreatments (Fig. 1). The mean time for the second relapse was 5.50 ± 1.19 months.
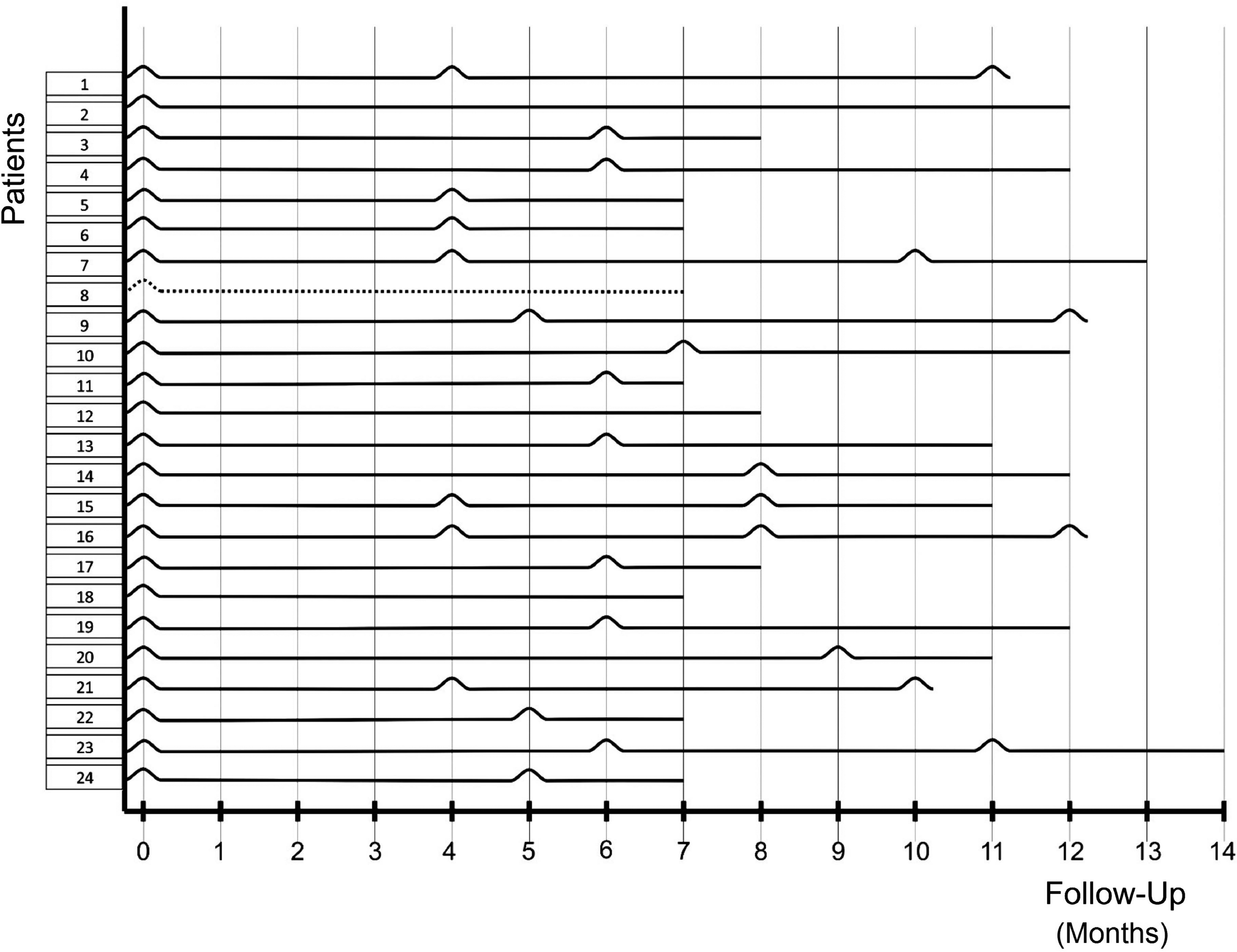
Post-treatment relapses of cases. Horizontal lines represent months of follow-ups and peaks show relapses. Case number 8 did not respond to Ozurdex and ranibizumab.
At baseline, the mean BCVA was 0.89 ± 0.31 logMAR. It was measured as 0.54 ± 0.29 logMAR (P < 0.01) and 0.64 ± 0.32 logMAR (P < 0.01) at the 3- and 6-month follow-ups, respectively. At the final visit, the mean BCVA was 0.62 ± 0.31 (P < 0.01). Compared with the baseline levels, loss of vision did not occur in any control visits.
The mean CFT decreased from 630.08 ± 133.07 μm at baseline to 313.21 ± 72.32 μm at the 3-month follow-up (P < 0.001). It was detected as 403.62 ± 178.45 μm (P < 0.001) at the 6-month follow-up and 335.46 ± 142.84 μm (P < 0.001) at the final examination.
The median height of SMD was 247.50 μm (minimum 80 μm, maximum 745 μm) before treatment. It was measured as 0 μm (minimum 0 μm, maximum 442 μm) (P < 0.001), 0 μm (minimum 0 μm, maximum 453 μm) (P < 0.001), and 0 μm (minimum 0 μm, maximum 426 μm) (P < 0.001) at the 3-month, 6-month, and final examinations, respectively.
Pretreatment and post-treatment visual acuity and OCT findings are summarized in Table 2. Visual acuity and OCT values before treatment and during relapse points are displayed in Table 3. Although changes in mean BCVA and mean CFT were not statistically significant, decrease in SMD height was statistically significant.
As Kolmogorov–Smirnov test revealed a non-normally distributed SMD data for 3-month, 6-month, and final examination, median SMD is also shown in the table.
One-way ANOVA test.
Friedman test.
ANOVA, analysis of variance; BCVA, best corrected visual acuity; CFT, central foveal thickness; SD, standard deviation; SMD, height of serous macular detachment.
Paired t-test.
One-way ANOVA test.
ANOVA, analysis of variance; BCVA, best corrected visual acuity; CFT, central foveal thickness; SD, standard deviation; SMD, height of serous macular detachment.
Horizontal cross-sectional OCT images of a case before treatment and follow-up period are shown in Fig. 2. In the overall population, 8 eyes were pseudophakic and 16 eyes were phakic. No serious systemic or ophthalmic adverse events including injection-related complications, endophthalmitis, or cataract progression were observed.
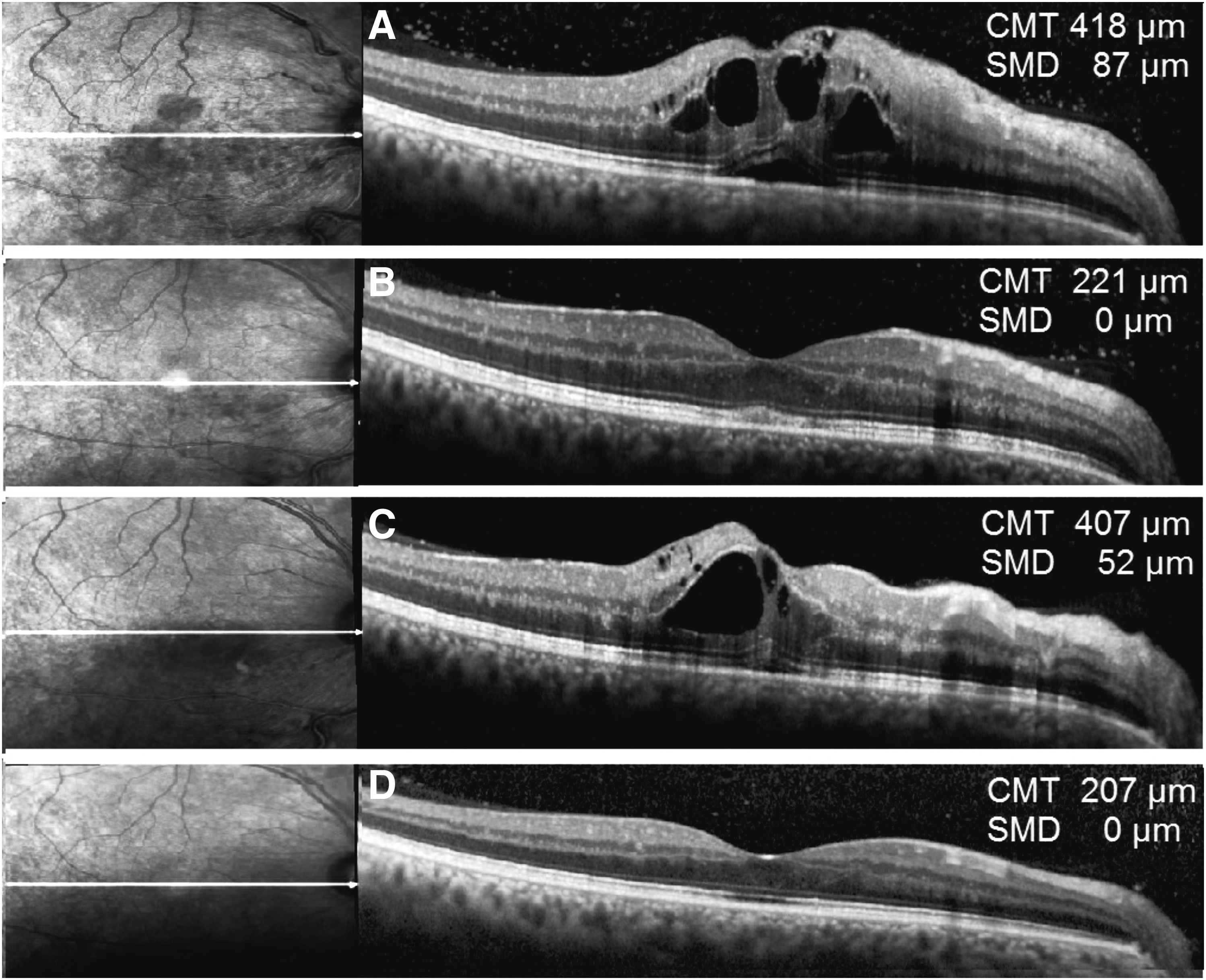
Horizontal cross-sectional OCT images of case 1 before treatment
The mean IOP was 16.0 ± 2.1 mmHg at baseline. Five eyes with increased IOP after single or repeated Ozurdex injection required a topical IOP-lowering medication. At the final visit the mean IOP was measured as 18.2 ± 2.9 mmHg.
Discussion
The pathogenesis of SMD in retinal vascular diseases is not clearly understood. However, it is believed that the leakage from retinal circulation into the subretinal space exceeding its drainage capacity is the main cause of SMD. 14 The occlusion of retinal venous outflow in RVO leads to an increase in intravascular pressure, particularly in postcapillary venules and capillaries. Venous obstruction also leads to capillary nonperfusion and tissue ischemia, which causes generation of chemical intermediates that enhance vascular permeability. Thus, it is well known that increased intravascular pressure and vascular permeability in CRVO and branch retinal vein occlusion (BRVO) have important roles in the development of ME and SMD. 23 Laser photocoagulation, intravitreal steroids, and intravitreal anti-VEGF drugs were tried in the management of these complications.6–9,24,25
Laser photocoagulation was not found to be effective in the treatment of ME secondary to CRVO. 24 However, grid laser photocoagulation yielded partial success in the treatment of ME secondary to BRVO. 25 The possible mechanisms through which laser photocoagulation is beneficial are ablation of the ischemic retina and consequent decrease in vascular permeability factors, the closure of incompetent capillaries, and the stimulation of retinal pigment epithelium facilitating fluid resorption. 26 By contrast, in eyes with SMD and BRVO, it is reported that absorption of ME was delayed after grid laser and that no visual and anatomic success was obtained. 27 In contrast, only a limited number of studies examined their effect on SMD associated with RVO.21,28,29 Cinal et al. 21 have studied the effect of IVB on 19 eyes with SMD related to CRVO over a mean follow-up period of 21.6 months. In their study in which 15 cases were reported as being nonischemic, the mean BCVA increased, the mean CFT decreased, and SMD was resorbed in 16 patients with an average number of 5.9 injections. In another study including 34 eyes with BRVO and 14 eyes with CRVO, Dolz-Marco et al. 28 have found that IVR was not effective in improving visual acuity in 7 eyes with SMD. Gallego-Pinazo et al. 29 reported improvement in BCVA and all SD-OCT parameters in 22 patients with SMD secondary to BRVO with a mean number of 5.0 IVR injections over a follow-up period of 12.5 months. None of the mentioned studies had a statement about the time when complete resorption of SMD was first observed.
Intravitreal anti-VEGF drugs have a relatively short duration of effect against ME and hence the need for repeated injections is a major drawback of this treatment option. In contrast, numerous studies revealed that the pathogenesis of SMD is not solely linked to congestion of the draining vascular system but also related to the dysfunction in various retinal and choroidal structures,29–31 and particularly to inflammation.18–32 Therefore, anti-VEGF injections that are effective in diffuse retinal thickening (DRT) might be insufficient in eyes with SMD.16,17,33
The inflammatory cytokines were more often found to be correlated with morphological changes assessed by SD-OCT, whereas VEGF-A did not correlate with CRVO-associated changes in SD-OCT. In a study conducted by Dacheva et al., 33 inflammatory cytokines such as IL-6 and MCP-1 in CRVO cases were found to be correlated with morphological changes such as central macular thickness, thickness of neurosensory retina, extent of SMD, and disintegrity of the IS/OS, in contrast to VEGF-A level that did not yield any correlation. In another study, VEGF, IL-6, and IL-8 levels were examined in vitreous samples of patients with DM, and only IL-6 had a significant correlation with the presence of SMD. Thereby authors have concluded that inflammation might have an important role in SMD development in eyes with diabetic ME. 18 In a study that included diabetic eyes grouped according to their predominant patterns of ME as DRT, cystoid macular edema (CME), or SMD, inflammatory cytokines were found higher in CME and SMD groups than in the DRT group, whereas no difference was found between groups in terms of angiogenic cytokines such as VEGF. 32
Another mechanism suggested for the development of SMD is external limiting membrane (ELM) damage. As lipids and proteins that are extravasated because of the blood–retinal barrier destruction cannot pass through the ELM, they draw fluid to the outer retina through an osmotic effect. When there is damage in the ELM, the excess fluid accumulated in the outer retina freely moves to the subretinal space along with lipids, proteins, and inflammatory cells. 31 The presence of IL-6 promotes the inflammation in the outer retina 34 and may further damage the ELM. There are also considerations about defects in the choroidal vascular bed secondary to RVO and disruptions in the outer blood–retinal barrier that might have important roles in the pathogenesis of SMD. 29
As SMDs are presumably linked to a multifactorial process, its treatment necessitates a multidirectional therapeutic effect. To have a maximum potency against SMD, an ideal drug should prevent new vessel formation, reduce the vascular permeability, inhibit the inflammatory cascade, promote the retinal pigment epithelium (RPE) function, and prevent or better heal the ELM damage.
The antiedematous effect of corticosteroids depends on several mechanisms. It is well known that corticosteroids inhibit the cell-mediated inflammation by reducing leukocyte adhesion and extravasation. It is also proved that corticosteroids restore the function of the blood–retinal barrier, downregulate the synthesis of VEGF, which is also known as a vascular permeability factor, and trigger the RPE pump. 35 In addition, it was also found that triamcinolone, a corticosteroid, also induces Müller cell-mediated fluid resorption from retinal tissue. 36 Actually, triamcinolone acetonide is the first intravitreal drug reported to be effective in the treatment of ME and SMD secondary to CRVO. In the study conducted by Karacorlu et al., 37 IVTA was applied to 10 eyes with CRVO. ME and SMD were resorbed, central macular thickness (CMT) decreased, and visual acuity increased. On recurrence, IVTA injection was repeated in 4 of 5 patients in the third and sixth months, respectively.
Although triamcinolone acetonide was widely accepted to be effective in ME, high incidence of its side effects such as increased IOP and cataract formation limited the use of this drug and urged the research for alternative corticosteroids with lower incidence of side effects. A sustained-release dexamethasone intravitreal implant, Ozurdex, was used in the treatment of ME secondary to BRVO or CRVO. Several studies revealed that the mean BCVA improved and the mean CFT decreased in eyes with RVO treated with Ozurdex. However, the incidence and outcome of SMD were addressed in only 2 studies.12,20 In the study, which has a larger study group, Maggio et al. examined the factors affecting the prognosis in RVO. CRVO/hemicentral RVO was identified in 23 patients and Ozurdex injection provided a significant improvement in BCVA of 11 nonischemic eyes at the end of 12.5 months of the mean follow-up period; however, no gain in BCVA was obtained in the ischemic group despite the apparent regression of CMT.
Several coexisting factors that are influential on parameters measured in previous studies might have yielded confusion about the interpretation of the outcomes specific to treatment-naive SMD and ME secondary to recent onset nonischemic CRVO. We have found that injection of Ozurdex provided regression of ME and SMD in all eyes but in 1 eye. ME recurred in 20 eyes once, in 8 eyes twice, and in 1 eye thrice during the follow-up period. The mean time was 5.45 ± 1.43 months for the first relapse and 5.50 ± 1.19 months for the second relapse. Most of the recurring eyes had SMD. However, the mean height of SMD was barely lower than pretreatment (244.20 ± 129.26 at baseline and 59.05 ± 33.73 at first relapse points of cases). Ozurdex has a more prolonged duration of action than anti-VEGF drugs and a lower incidence of side effects than triamcinolone acetonide, which makes it a successful option for the treatment of ME secondary to RVO.
Our study group consisted of treatment-naive nonischemic CRVO cases with similar visual acuities, all of which received a standard initial treatment approach. This makes our study results more refined for a specific clinical trait. Our study, in contrast, has some limitations with its small sample size, short follow-up time, and retrospective nature. Besides, as this study includes only a specific subset of CRVO, it is difficult to generalize these results to all CRVO patients.
In conclusion, in our study population, intravitreal Ozurdex was found as an effective and reliable therapeutic option for the treatment of SMD and ME in nonischemic treatment-naive CRVO. To better assess the effectivity and reliability of Ozurdex in similar case groups, more randomized controlled studies comparing Ozurdex and alternative drugs are needed. Also, to evaluate the effect of SMD in the prognosis of CRVO, additional studies should compare the effects of Ozurdex for eyes with and without SMD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.