
Abstract
Abstract
Purpose:
To evaluate the efficacy and tolerance of a new matrix-regenerating agent (RGTA), Cacicol®, a polymer that mimics heparan sulfates bound to extracellular matrix proteins, avoiding its proteolysis, to treat neurotrophic keratopathy (NK).
Methods:
Uncontrolled prospective clinical study performed between January 2014 and May 2016. Twenty-five patients (25 eyes) with corneal neurotrophic ulcers, nonresponsive to at least 2 weeks of conservative therapy, were treated with Cacicol, instilled once/twice a week. During follow-up, slit-lamp examination, anterior segment photography, fluorescein-dye testing, and best-corrected visual acuity were analyzed. Ulcer evolution was evaluated using image analysis software (ImageJ®) and healing defined as decrease of the corneal ulcer area. An independent observer measured ulcer area.
Results:
All patients had complete corneal healing within an average of 4.13 ± 2.32 weeks. Mean ulcer area decreased significantly (P = 0.001) from 16.51% ± 18.56% (1st day) to 8.68% ± 11.25% at the 7th day and to 4.73% ± 10.75% at the 14th day. Compared with day 1, mean ulcer area decreased 60.24% after 7 days (P = 0.001), 54.92% after 14 days (P = 0.059), and 83.00% after 21 days (P = 0.003). Two cases of recurrence (8.0%) were registered. No systemic or local side effects were noticed.
Conclusions:
The new regenerating agent, Cacicol, represents an effective and safe therapy to treat NK.
Introduction
T
Neurotrophic keratopathy (NK) is a rare degenerative corneal disease, potentially sight threatening, characterized by reduced or absent corneal sensitivity, spontaneous epithelial breakdown, and impairment of corneal healing. 2 NK results from localized or systemic conditions affecting nerve function along its course and is frequently associated to herpes keratitis, chemical burns, long-term use of contact lenses, corneal surgery, or ablative procedures for trigeminal neuralgia. 3
According to Mackie, 4 clinical severity of NK is classified in 3 stages that guide the therapeutic approaches (Table 1). Treatment of corneal epithelial injuries with vitamins, collagenase inhibitors, anti-inflammatory agents, prophylactic topical antibiotic, artificial tears, or bandage contact lenses is frequently of poor or transient efficacy. In severe cases, oral doxycycline, autologous serum, amniotic membrane transplantation, tarsorrhaphy, or a conjunctival flap are used alone or in combination. 5 However, successful modulation of the healing response in these patients is rarely accomplished.
PK, penetrating keratoplasty; TCL, therapeutic contact lenses.
New topical treatments using growth factors such as epidermal growth factor (EGF), nerve growth factor (NGF), insulin-like growth factor (IGF), and matrix proteins were demonstrated effective in animal models.6–8 Recent studies with NGF have shown promising results in human corneal surgical wound healing.9,10
Clinical studies with a new matrix regenerating agent (RGTA) performed in animals 11 and humans12–14 have shown encouraging results in the treatment of corneal ulcers and dystrophies of various etiologies. RGTA is a biopolymer designed to mimic heparan sulfates bound to corneal extracellular matrix proteins, protecting them from proteolysis and enabling growth factors and cytokines to act on the injured site. It restores the physiological matrix organization and cellular microenvironment, stimulating the regeneration process. 12
The aim of this study was to evaluate the efficacy and tolerance of a new matrix RGTA, Cacicol®, in the treatment of NK.
Methods
This is a prospective clinical study performed at Centro Hospitalar e Universitário de Coimbra, between January 2014 and May 2016. Written informed consent was obtained from all subjects, and the study was conducted in accordance with the tenets of the Declaration of Helsinki.
Twenty-five patients (25 eyes) >18 years of age with persistent corneal neurotrophic ulcers despite 2 weeks of occlusion therapy, preservative-free eye lubricants, and autologous serum instillation were included. All presented corneal anesthesia, subjectively demonstrated by cotton tip test.
A corneal expert classified all cases according to Mackie's classification and performed corneal ulcer borders debridement. All patients were treated with RGTA eye drops (Cacicol; OTR3, Paris, France), instilled in the morning. All started with 1 instillation per week. In the absence of corneal ulcer area decrease, 2 weekly instillations were performed and maintained until complete corneal healing. RGTA treatment was interrupted as soon as complete healing was achieved. Aminoglycosides antibiotics were not used concomitantly.
Follow-up visits were scheduled to days 7, 14, 21, 28, and months 2 and 3 after initiating treatment. Each clinical evaluation included slit-lamp examination, anterior segment photography, fluorescein-dye testing and best-corrected visual acuity (BCVA, Snellen optotype). Ulcer evolution was evaluated using image analysis software (ImageJ®, version 1.47; Wayne Rasband Research Service Branch, National Institute of Mental Health, Bethesda, MD) and healing defined as decrease of the corneal ulcer area. Recurrence was considered when a new epithelial defect reappeared in the same area as the previous corneal ulcer within 3 months after complete corneal healing.
At each visit, neurotrophic ulcer area was calculated as proportion of the total corneal area by slit-lamp photography, using image analysis software ImageJ. Ulcer area was measured by an independent observer, with no access to patient's data or clinical stage.
Wilcoxon and Friedman tests were used to compare BCVA values and corneal ulcer area, respectively. Log-Rank Mantel-Cox test was used to identify corneal healing risk factors, and Kaplan–Meier analysis was performed to estimate time until cure. A P-value below 0.05 was considered statistically significant.
Results
Twenty-five eyes of 25 patients were included. The mean age at the beginning of the treatment was 61.68 ± 17.02 years (range: 27–90), and 16 (64.0%) patients were male. The mean follow-up time was 13.91 ± 7.27 months.
All corneal ulcers were grade 2 in Mackie's clinical classification, except for 1, which was grade 3. The most frequent cause of NK was surgical trauma (80.0%; n = 20). Eleven cases occurred after surgeries other than penetrating keratoplasty (cataract and vitreo-retina surgeries), one of these with familial amyloidosis polyneuropathy. Nine were after penetrating keratoplasty (PK) and 1 with a previous chemical burn. Causes of corneal ulcers are summarized in Fig. 1.
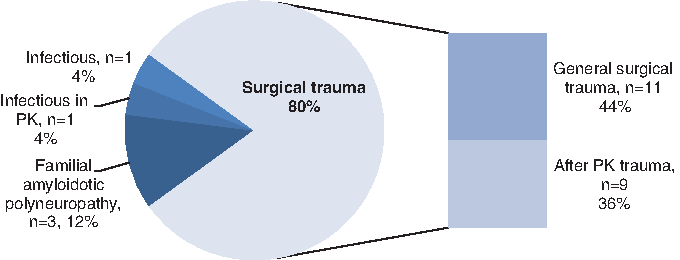
Causes of corneal ulcer. PK, penetrating keratoplasty.
The average number of instillations until complete corneal healing was 5.0 ± 2.64 (median = 5), with an average of 1.41 ± 0.46 instillations per week.
All patients had complete centripetal corneal ulcer healing within an average of 4.13 ± 2.32 weeks—ranging from 1 to 9.29 weeks (Figs. 2 and 3). After initiating treatment, the mean area of neurotrophic ulcers decreased significantly (Friedman test: P = 0.001) from 16.51% ± 18.56% (1st day) to 8.68% ± 11.25% in the 7th day and to 4.73% ± 10.75% in the 14th day (Fig. 4). When compared with day 1, mean ulcer area decreased 60.24% after 7 days of treatment (P = 0.001), 54.92% after 14 days of treatment (P = 0.059), and 83.00% after 21 days of treatment (P = 0.003).
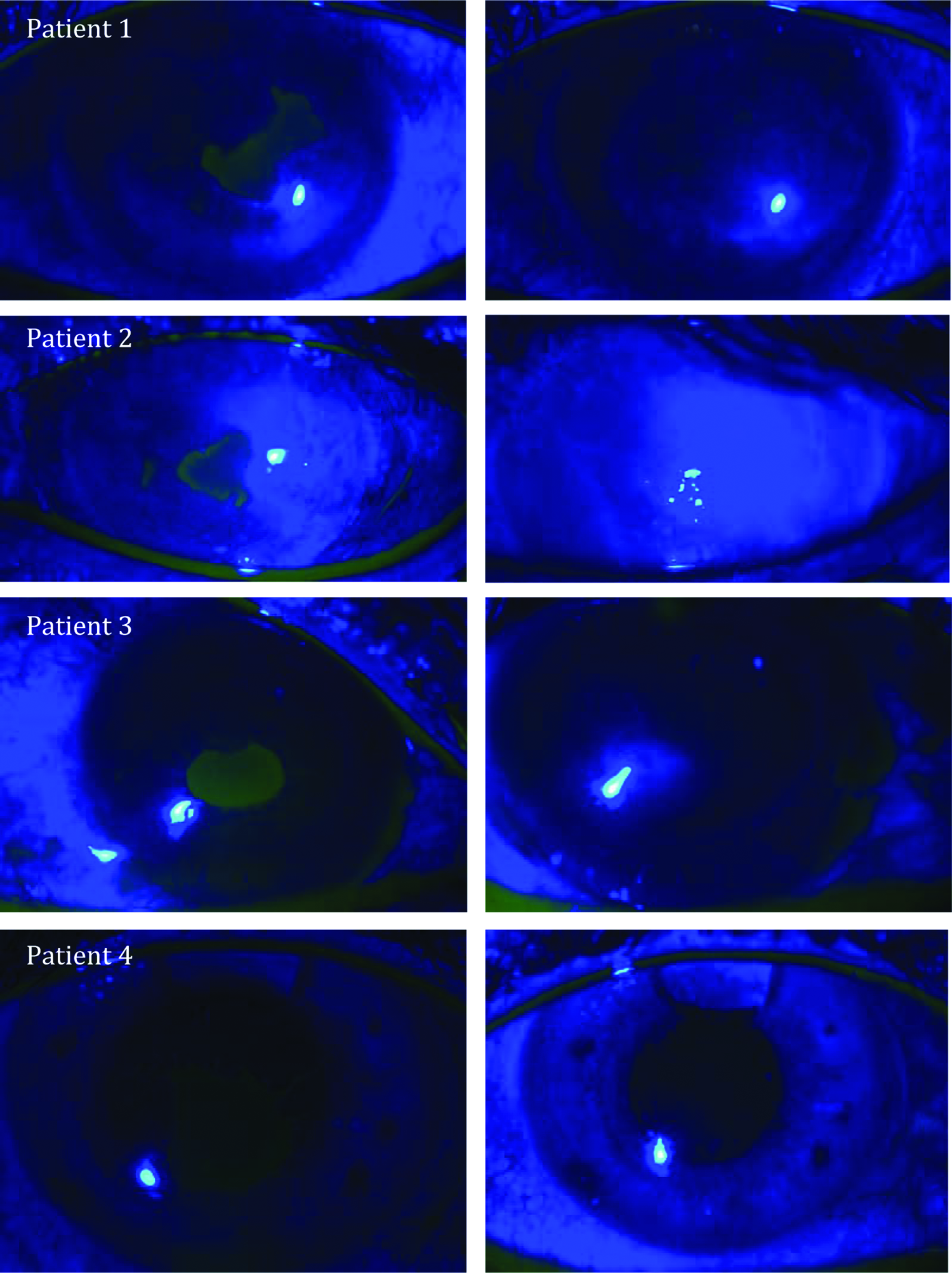
Corneal neurotrophic ulcers after RGTA treatment. Left column: before treatment; right column: after healing. Patient 1: FAP, complete corneal healing in 1 month; Patient 2, 3, and 4: surgical trauma, complete corneal healing in 1 month, 6 weeks and 2 weeks. FAP, familial amyloidotic polyneuropathy; RGTA, regenerating agent.
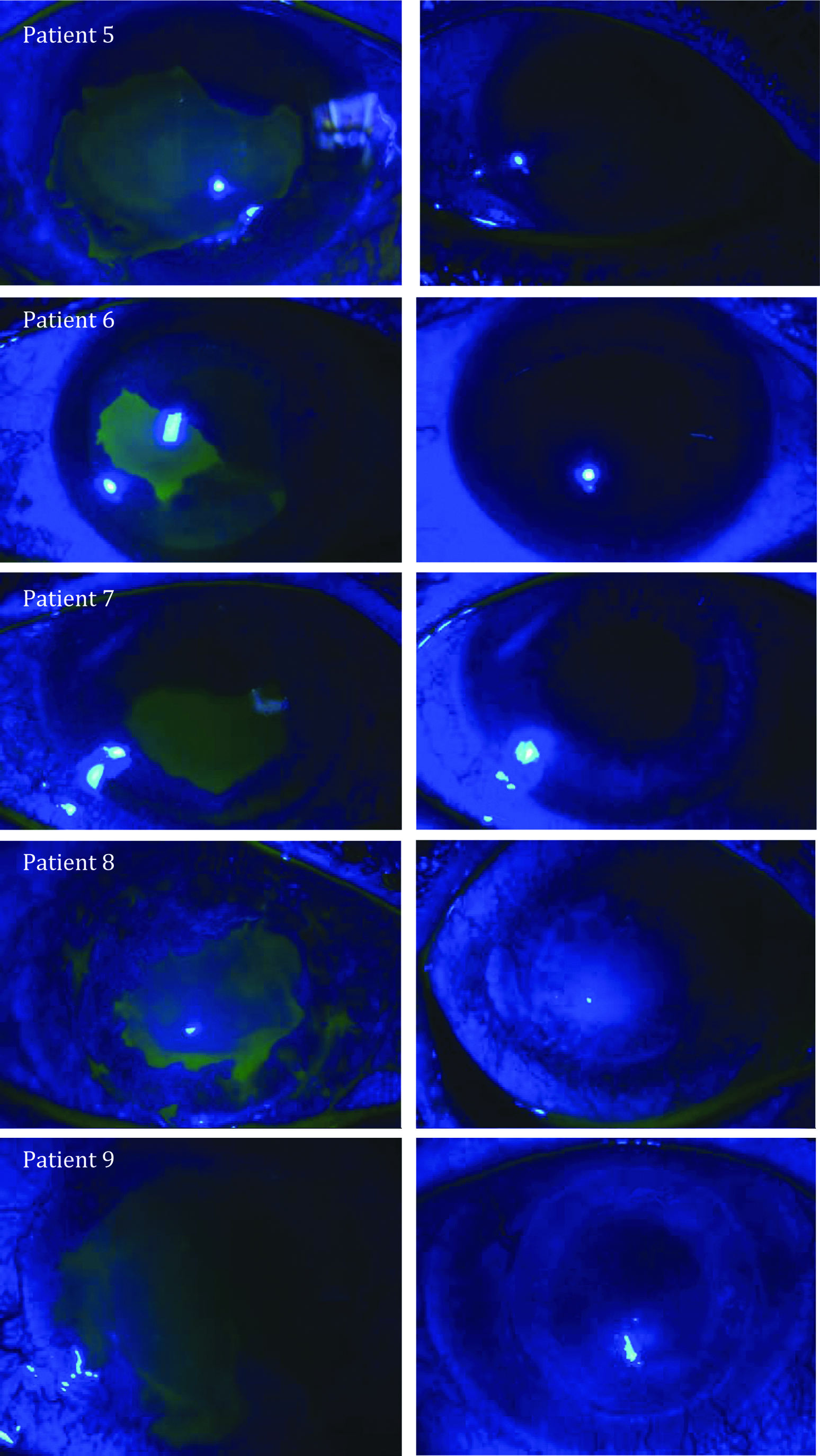
Corneal neurotrophic ulcers after RGTA treatment. Left column: before treatment; right column: after healing. Patients 5, 6, and 7: surgical trauma, complete corneal healing in 6, 2, and 2 weeks, respectively; Patient 8: after PK, complete corneal healing in 6 weeks; Patient 9: infectious in PK, complete healing in 3 weeks.

Mean and median area of corneal neurotrophic ulcer (%) during RGTA treatment; n = 25.
The healing rate after 7 days of treatment was 12% (n = 3), followed by 28% (n = 7) by the end of the 14th day, 44% (n = 11) after 21 days, and 68% (n = 17) within the first month. By the end of the second month of treatment, all corneal ulcers had healed.
Healing occurred without neovascularization in all patients. However, moderate corneal scarring was noticed at slit-lamp examination. No patient experienced a decrease in visual acuity, 7 patients presented with an improvement in visual acuity at the last follow-up available. Mean visual acuity significantly improved from 1.40 ± 0.67 to 1.2 ± 0.63 logMAR (Wilcoxon test: P = 0.027).
Using Kaplan–Meier survival analysis, the mean complete corneal healing time was 28.76 ± 3.21 days, with an expected mean time of 22.46–35.05 days within a confidence interval of 95%. This interval of time until cure is not correlated to gender (Log-Rank Mantel-Cox test: P = 0.853) or corneal ulcer cause (P = 0.101). Cox regression also showed that age (P = 0.819), initial corneal ulcer area (P = 0.408), initial visual acuity (P = 0.162), gender (P = 0.631), and corneal ulcer cause (P = 0.892) are not risk factors for delayed corneal healing.
Two cases of recurrence (8.0%) were recorded. The first case occurred 1 month after complete corneal healing (Fig. 5). Despite 5 more RGTA instillations, retreatment failed and RGTA application was discontinued. This patient had history of oral mucosa allotransplant and 2 PK after a chemical burn. The last clinical evaluation revealed diffuse decrease of corneal transparency without corneal ulcer and visual acuity of light perception. Topical treatment with autologous serum was maintained and cyclosporine introduced. The second recurrence occurred in a patient with PK, 6 weeks after complete corneal healing. Two weeks of occlusion and topical treatment with preservative-free eye lubricants and autologous serum instillation led to successful corneal healing.
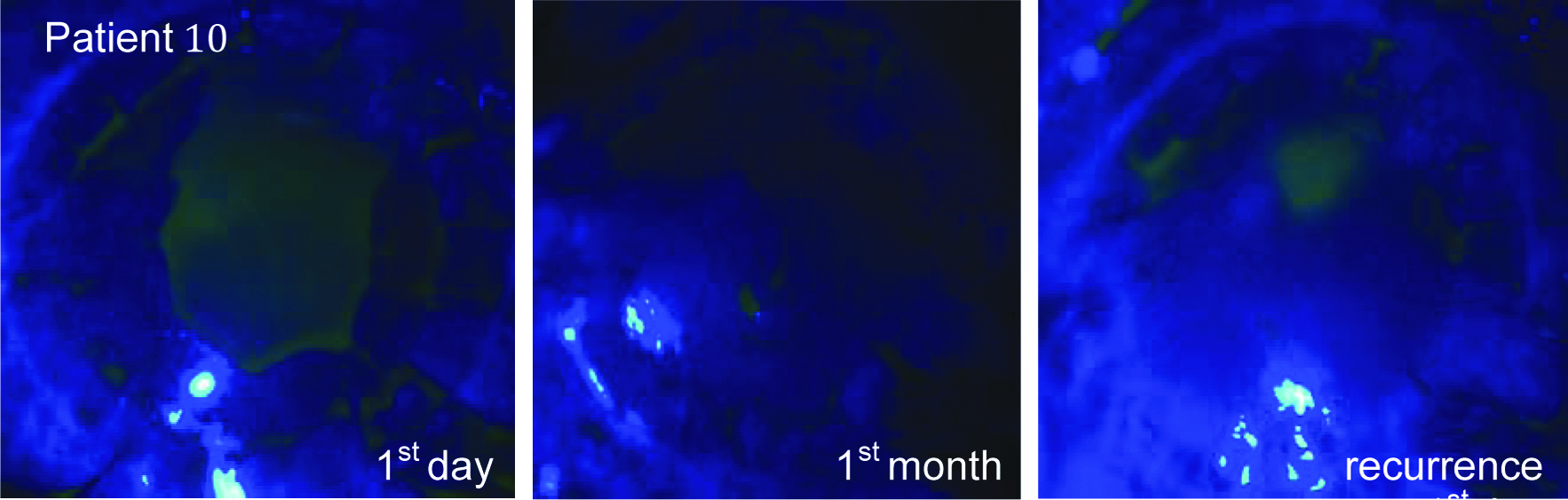
Patient 10: after PK with history of chemical burn, complete corneal healing in 1 month; recurrence 1 month after RGTA interruption.
No systemic or local side effects were noticed, and no pain or discomfort during drop instillation was reported.
Discussion
NK is one of the most difficult and challenging ocular diseases that lacks a specific treatment. Corneal healing is a complex process that involves a diversity of growth factors, cytokines, and cellular interactions. 15 The inability to correctly modulate this process leads to persistent epithelial corneal defects, corneal ulcers, inflammation, melting, and finally perforation. 5 Prompt aggressive treatment based on clinical evidence is essential to avoid final stages of NK.
Conservative treatments are frequently ineffective and the need to find new substances to favor and improve corneal healing emerges. Molecules such as collagenase inhibitors, fibronectin, heparin, EGF, IGF, and NGF 12 proved efficacy in in vitro and animal studies. Medical treatments include autologous serum and neurotrophin eye drops, 16 but only autologous serum and plasma rich in growth factor are currently being used in clinical practice with effectiveness.17–19
Autologous serum includes components such as substance P (SP), IGF-1, and NGF, which improve proliferation, migration, and differentiation of the corneal surface epithelium and can be useful to restore its integrity in patients with NK.20–23 Clinical studies showed complete corneal healing in 60%–100% of the patients with NK treated with autologous serum within a mean time period ranging from 17.1 to 22.4 days.22–24 However, it requires weekly blood sampling and a preparation protocol. The risk of contamination for patients and health professionals, instability of the product, and the absence of a legal framework associated to its high cost are other disadvantages. 19 On the contrary, Cacicol is a purely engineered product, free of contamination risk. The association of topical SP and IGF was also used in an open study in 25 patients with NK, with complete healing of persistent epithelial defect (PED) in 73% of patients within 4 weeks. 8
Encouraging results with topical NGF were obtained in patients with moderate to severe NK. Uncontrolled studies reported complete corneal healing within 12 days to 6 weeks of treatment.20,21 Recently, a recombinant human NGF eye drop formulation has been developed for clinical use, and Phase 2 studies have shown safety and good tolerance. 25 However, none of these new agents is yet available. Another phase 2 randomized study was evaluating the safety and effectiveness of topical Nexagon®, CODA001, a natural oligonucleotide that downregulates connexin43, reducing inflammatory response and enhancing healing. Patients with PED resulting from diabetic vitrectomy surgery, herpes simplex virus (HSV) keratitis, herpes zoster virus (HZV) keratitis, corneal burns, postphotorefractive keratectomy, or postcorneal transplant surgery were included. However, the study was not completed. 26
An alternative topical treatment for NK has been recently commercialized, the ReGeneraTing Agent OTR4120® of extracellular matrix Cacicol. It is provided as a sterile single-dose solution of polycarboxymethyl glucose sulfate with dextran T40 and 0.9% sodium chloride as excipients. It belongs to the polysaccharides' family, derived from dextran by chemical substitutions with carboxymethyl, sulfate and hydrophobic groups.27,28 The therapeutic interest of this regenerator agent was first described by Papy-Garcia et al. 29 in 2005 and initially used to treat skin healing after burns. 30 This biopolymer is engineered to replace the heparan-sulfates destroyed upon tissue injury and to specifically bind extracellular matrix proteins and growth factors, protecting them from proteolysis. 27 In vitro, it improves extracellular matrix remodeling and formation by enhancing collagen I and III31–33 and glycosaminoglycan synthesis. 34 It additionally contributes to matrix protection by inhibiting proteolytic enzymes such as elastases, plasmines, and cathepsin. 12
A noncontrolled French pilot study showed the efficacy of RGTA instilled once a week in the treatment of both chronic corneal dystrophies and resistant corneal ulcers, with complete corneal healing achieved in 4 of the 5 patients included and no side effects reported. 12 However, 2 ulcers recurred after treatment interruption, suggesting that a higher dose could be more effective. Aifa et al. reported complete corneal healing in 8 (72.7%) of 11 patients with severe NK after 8.7 weeks of treatment with RGTA on alternate days. 13 Despite the higher dose used, recurrence occurred in 1 patient and treatment failed in 3 patients. Two patients presented ulcer area expansion and 1 deep ulcer evolved to microperforation. Three more clinical cases are reported in the literature, 1 after herpes zoster ophthalmicus 14 and 2 after fungal keratitis. 35 In these cases 2 or 3 administrations per week lead to complete corneal healing within 4–8 weeks. These encouraging results were investigated in an alkali-burned rabbit cornea model with a single dose of RGTA-OTR4120 (50 μL, 5 μg) and compared with a control group treated with sodium chloride. 11 RGTA treatment appeared effective in reducing clinical signs of inflammation, enhancing reepithelialization, and improving histological patterns, without in vivo toxicity even at high doses. Moreover, Cacicol has no components of animal or biological origin, being not only safer than other topical agents developed to date but also effective in penetrating the cornea without crossing the Descemet's membrane.
One or 2 weekly instillations of 0.33 mL sterile dose are the producer's recommended dosage, due to the limited sites for heparan binding available in the healing tissue. Once all these sites are RGTA bound, excess RGTA may compete with heparan-binding growth factors for sites on the matrix-bound RGTA, reducing the amount of growth factor available and its healing efficacy.
Our series, the largest described in the literature, showed promising results: total reepithelialization achieved in all 25 patients within 1–9 weeks after initiating Cacicol once or twice a week. These results are similar to or even better than those reported in the literature.12,13 A shorter period until healing was described, using similar RGTA doses, with statistically significant decrease of ulcer area. Despite antioxidant and antifibroblast proliferation effects of RGTA, moderate corneal scarring was noticed. However, visual acuity improved significantly after complete corneal healing. Since RGTA is capable of binding growth factors to the extracellular matrix and prevents proteolysis, combined treatment with autologous serum complements its actions, leading to rearrangement of the extracellular microenvironment, which becomes suitable for proliferation, migration, and differentiation of the ocular surface epithelium.
Statistically analyzing the interval of time until cure, we conclude that age, initial corneal area, initial visual acuity, gender, and corneal ulcer cause are not risk factors for delayed corneal healing. However, larger randomized studies are required to ascertain associated risk factors.
After a mean follow-up period of 13.91 ± 7.27 months, recurrence rate was low (8.0%, 2 patients).
Conclusions
Despite its limitations, absence of randomization or controlled groups and small population, our study represents the largest series reported in the literature showing that RGTA Cacicol is effective and very well tolerated in corneal wound healing. It is not only a stable molecule that can be synthesized with reproducibility and no contamination risk but also an easy and comfortable topical treatment. A Phase 3 randomized clinical trial is ongoing to evaluate the safety and efficacy of RGTA-T4020 instilled 4 times per week in the treatment of chronic neurotrophic keratitis or corneal ulcer. 36 In the future, more randomized studies should be performed to define inclusion criteria and the most appropriate therapeutic dosage.
Footnotes
Author Disclosure Statement
The authors have no commercial or proprietary interest in any concept or product described in this article. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.