
Abstract
Abstract
Purpose:
To assess the sensitivity of corneal cold receptors to a known transient receptor potential melastatin 8 (TRPM8) agonist, menthol, in dry eye and normals, and to determine whether factors such as disease duration or age affect responses.
Methods:
Dry eye disease (DED) (N = 33) and normal (N = 15) subjects were randomly assigned to receive Rohto® Hydra (0.01% menthol) or Systane® Ultra treatments (OU) in a prospective, double-blind, crossover study. DED subjects had documented disease and symptom response scores >2 on a 0- to 5-point scale. Normals had no history of DED and scores <2 on the same scale. Endpoints included mean cooling score (0 = not cool and 10 = very cool) evaluated at 0, 0.5, 1, 2, 3, and 4 min post-instillation, sum cooling scores (5 time points, range 0–60), and ocular signs and symptoms.
Results:
Mean (±SD) ages were similar, 62.2 ± 8.6-year (DED) versus 53.5 ± 7.6-year (normal). Corneal sensitivity scores were not different between groups. Mean cooling scores at 0.5–4 min post-menthol instillation were significantly higher in DED subjects (P ≤ 0.03). Sum cooling scores were significantly higher (P = 0.04) in DED subjects with a disease duration <10 years (N = 18, 28.3 ± 2.58) versus ≥10 years (N = 15, 20.2 ± 2.76). Age did not affect cooling response in either group.
Conclusion:
DED subjects had greater sensitivity to cold than normal subjects. DED duration, and not age, was critical to cooling sensitivity. The finding that cooling scores were higher in subjects with DED for less than 10 years compared to more than 10 years suggests that corneal cold receptor sensitivity decreases as the duration of DED increases.
Introduction
T
Maintaining a stable tear film during the interblink interval is critical to ocular surface health and is regulated, in part, by intact primary afferent sensory mechanoreceptors, cold receptors, and polymodal nociceptor nerve fibers innervating the ocular surface. The peripheral terminals of these nerves are located between the superficial corneal epithelial cells. Any damage caused by inflammation, desiccating stress, or abnormal gland secretions associated with DED may disrupt transmission of critical sensory information, including changes in pressure, temperature, and pain from the cornea to higher regulatory centers.6,9–11 Cold receptors express the transient receptor potential melastatin 8 (TRPM8), a nonselective cation channel that is believed to be a key transducer of ocular cooling (∼15–28°C), as well as cool sensation-producing ligands such as menthol.12,13
Corneal sensitivity is an indicator of ocular health and has been demonstrated to decrease with age.14–16 Confocal microscopy studies have reported that subbasal nerve density is either reduced or unchanged in DED patients. 17 In a similar manner, corneal sensitivity associated with DED has shown mixed results, with reports indicating both a decrease18–20 and an increase6,21,22 in sensitivity.
Much of the research exploring the relationship of TRPM8 to corneal cooling sensitivity was conducted in studies involving ex vivo corneas or in animal models.23–25 Parra et al. 26 explored the association between corneal temperature, neuronal activity, and reflex tearing in mammals. Their results demonstrated that a cold thermoreceptor impulse activity in response to decreased corneal temperature is suppressed after abolition of TRPM8 receptors in mice. Basal tearing has also been shown to be reduced in response to corneal warming in humans and mice. Kovacs et al. more recently 24 demonstrated, in multiple animal experiments with excised lacrimal glands, the changing thresholds for sensitivity of thermoreceptors, accompanied by changes in blink rate and tearing. Kovacs et al. also did preliminary work in humans using menthol strips on the cheek instead of directly in the eye, demonstrating significant effects of menthol on blinking, ocular discomfort, and cooling sensation, but not tearing. 24 Given that DED may result in enhanced corneal nerve sensitization6,21,22,24–26 and menthol elicits a neuronal response similar to mild cooling temperatures,10,23–29 we hypothesized that DED patients would display an enhanced corneal cooling response compared to healthy subjects. The objective of this study was to assess the sensitivity of corneal cold receptors to a known TRPM8 agonist, menthol (Rohto® Hydra), in dry eye and normal subjects. Results were compared to the cooling response triggered by nonmenthol containing artificial tears in the same subjects. In addition, this study sought to determine whether any factors such as age or disease duration contributed to potential differences in cooling responses in patients with DED.
Methods
This single-center, 2-visit, double-masked crossover study compared the sensitivity of corneal cold receptors to Rohto Hydra (The Mentholatum Company, Orchard Park, NY) with those of Systane® Ultra (Alcon Laboratories, Inc., Fort Worth, TX) in DED and normal subjects. Systane Ultra was selected as the control drop because it contains the same excipients as the Rohto Hydra, excluding menthol. Drops were stored at room temperature in the same location.
The study was approved by an Institutional Review Board (Alpha IRB, San Clemente, CA) and conducted in accordance with the Tenets of the Declaration of Helsinki. It was registered with clintrials.gov as NCT02985827.
All subjects provided written informed consent and were at least 18 years of age of any gender or race. At Visit 1, subjects underwent baseline slit-lamp examination and ETDRS best-corrected visual acuity (BCVA) and provided ocular medical/surgical history. DED subjects had a history of DED symptoms for at least 6 months with a symptom response >2 (0–5 point scale) on the Ora Calibra™ Ocular Discomfort and 4-Symptom Questionnaire,30,31 had a tear film breakup time (TFBUT) of ≤5 s in at least 1 eye, and total (sum of superior, inferior, and central) staining score ≥4 (0–12 Ora Calibra scale). Normal subjects had no prior diagnosis of DED or history of dry eye symptoms, reported scores <2 on the Ora Calibra Ocular Discomfort and 4-Symptom questionnaire, and had not used artificial tears for the previous month for ocular dryness. Subjects were excluded from the study if they had contraindications, allergies, or sensitivities to Rohto Hydra or Systane Ultra, any active ocular infection or inflammation (excluding DED), or punctal plugs in either eye. Subjects with a history of refractive surgery in either eye, a history of any ocular surgery within the previous 12 months, or any uncontrolled systemic disease were excluded. Contact lens wear was prohibited for 30 days before and during the study. Subjects who had participated in another investigational drug or device trial within 30 days of the study were excluded. Women of child-bearing potential could not be pregnant, planning to become pregnant, or nursing during the study. All subjects were required to avoid prescription ophthalmic medications and over-the-counter solutions, including artificial tears, for 24 h before the study visit.
A baseline cooling assessment was performed using the Ora Drop Cooling Scale (0–10 scale: 0 = not cool and 10 = very cool). Bilateral corneal sensitivity was assessed using a Cochet-Bonnet esthesiometer. Rohto Hydra or Systane Ultra eye drops (15 μL) were instilled bilaterally by pipette and sterile tip in a double-masked, randomized manner. Following instillation, ocular coolness was assessed in each eye at 0, 0.5, 1, 2, 3, and 4 min postdose. The sum of the 6 time points generated a sum cooling score (0–60), which was averaged across subjects to generate a mean sum cooling score. At 10 min postdose, bilateral corneal sensitivity was again assessed.
After 1 h, the crossover treatment was instilled in a randomized double-masked manner and ocular coolness assessed as described. Following all cooling assessments, a bilateral anesthetized Schirmer's test was performed.
At Visit 2, signs and symptoms of dry eye, including symptomatology, OSDI (Ocular Surface Disease Index), TFBUT, corneal fluorescein staining, and lissamine green staining, were assessed in all subjects. Subjective symptoms of ocular discomfort, burning, dryness, grittiness, and stinging were scored separately and as a sum score using the standardized Ora Calibra Ocular Discomfort and 4-Symptom Questionnaire.30,31 TFBUT was assessed by instilling 5 μL of fluorescein dye into the tear film and measuring the time between the last complete blink to the first appearance of tear film breakup. 32 Corneal fluorescein (inferior, superior, and central regions) and conjunctival lissamine staining (nasal and temporal regions) were scored on the standardized Ora Calibra Corneal and Conjunctival Staining Scale (0 to 4 scale, 0 = none to 4 = confluent staining, half-point units allowed).30,31 Each region was graded separately; the sum of the 3 corneal regions generated a corneal sum score (0–12), and the sum of the 2 conjunctival regions generated a lissamine sum score (0–8). Safety analyses included slit lamp biomicroscopy, BCVA, and adverse event query.
Statistical analyses
Descriptive statistics were calculated for all variables. Left and right eyes within a subject were averaged to obtain one measure per subject at each time point for cooling scores. 33 For population comparisons, 2-way analysis of variance was used to compare mean differences in ocular cooling scores between DED and non-DED subjects. To examine potential relationships to other dry eye assessments, the correlation of mean cooling scores and sum cooling scores to Schirmer's score, age, duration of disease, corneal staining, and OSDI was calculated for DED and non-DED groups using the sample Pearson correlation coefficient, r. For all statistical comparisons, P-values less than 0.05 were considered statistically significant.
Subgroup analyses
The DED population was divided into 2 groups based on self-reported duration of disease: fewer than 10 years or 10 years or more.
The DED group was also categorized by age: <55 and ≥55 years, <60 and ≥60 years, <65 and ≥65 years, and <70 and ≥70 years. Mean sum cooling responses were calculated comparing the DED and normal groups for each age-subgroup separately (</≥55, 60, 65, and 70, respectively).
Two-tailed, unequal variance t-tests were used to compare sum cooling scores (0–60) to both Rohto Hydra and Systane Ultra, age, staining, symptom severity, and anesthetized Schirmer's scores between the subgroups of DED patients based on both disease duration and age.
Results
Thirty-three DED subjects (25 females and 8 males) and 15 normal subjects (8 females and 7 males) participated in this study. The mean age in the DED subjects was 62.2 ± 8.6 years (range 33–76 years) and the mean age in the normal subjects was 53.5 ± 7.6 years (range 36–63 years, significantly different from dry eye subjects, P < 0.05). The mean Schirmer's score with anesthesia was 5.5 ± 5.7 mm in the DED group and 12.8 ± 11.8 mm in normal subjects. The mean OSDI score was 15.5 ± 8.9 in the DED group and 1.4 ± 1.7 in normal subjects.
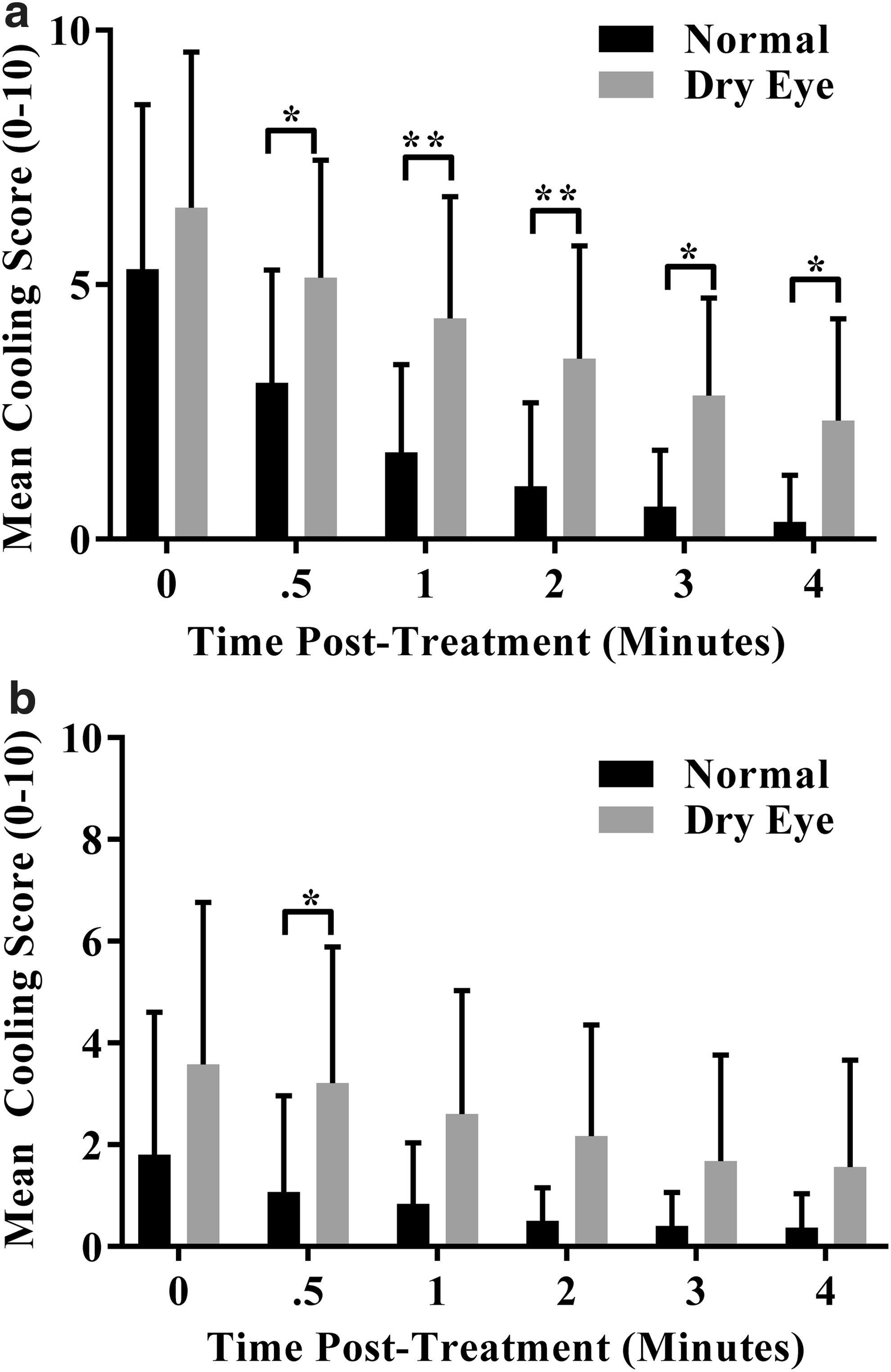
Mean corneal sensitivity scores were equivalent and normal (60 mm) in both groups at baseline and 10 min after instillation of Rohto Hydra and Systane Ultra (P = 0.24). Mean cooling scores obtained immediately upon instillation, and 0.5, 1, 2, 3, and 4 min post-Rohto Hydra were significantly higher in the DED group compared to the normal group at all time points (Fig. 1a, P ≤ 0.03). Mean cooling scores post-Systane were also higher in the DED group at all time points; however, only at 0.5 min postdose was this difference significant (Fig. 1b).
Sum cooling scores (sum across all time points, range 0–60, Fig. 2) were significantly higher in DED than normal subjects after treatment with both Rohto Hydra (P < 0.003) and Systane Ultra (P < 0.032). However, a greater cooling response was observed with Rohto Hydra relative to Systane Ultra only in the DED group (DED: P = 0.004 and non-DED: P = 0.320).
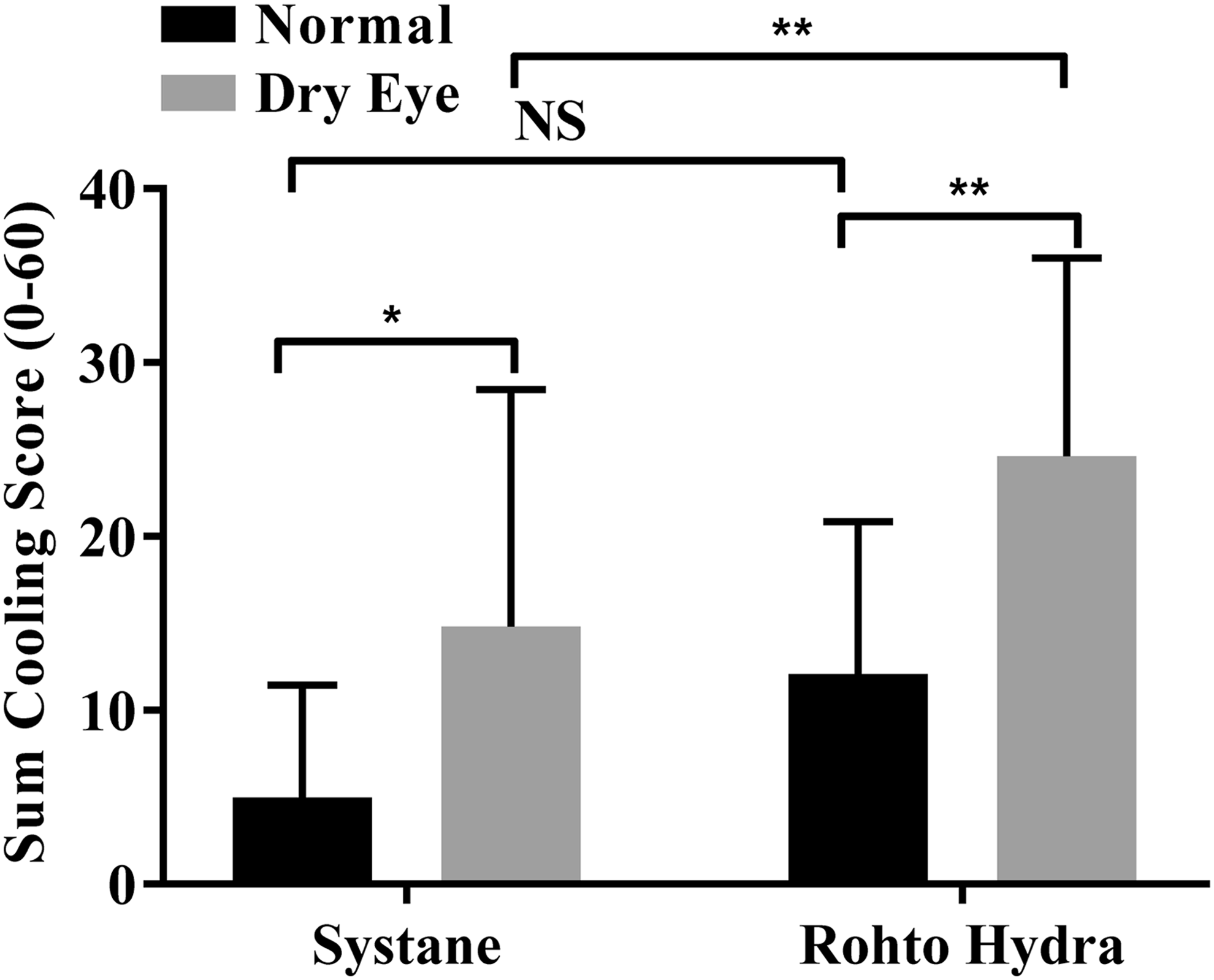
Mean (±SD) sum cooling scores (sum of 6 time points postdose, 0–10 point scale, range 0–60) after either Rohto Hydra or Systane Ultra treatment. Comparisons between DED and normal groups were calculated using a 2-way ANOVA (asterisk indicates statistical significance, P < 0.05).
Order of treatment had no effect on mean cooling response in either group. Also, statistical analysis of right versus left eyes showed no significant difference in either group and with either treatment, suggesting that contralateral or extra-ocular neurological cross talk did not interfere with ocular sensitivity assessments.
Sum cooling scores after Rohto Hydra treatment were negatively correlated with Schirmer's scores in DED subjects only (r = −0.38, P = 0.03, Table 1). Sum cooling scores after Systane Ultra treatment were not correlated with Schirmer's scores in either group (DED: r = −0.17, P = 0.36; non-DED: r = 0.29, P = 0.29, Table 1). Mean cooling scores were not significantly correlated with any other dry eye variable.
Bold values indicate P < 0.05.
DED, dry eye disease; OSDI, Ocular Surface Disease Index.
The DED population was divided into 2 groups based on self-reported duration of disease: 10 years or more (≥10, N = 15) or fewer than 10 years (<10, N = 18). Mean age was similar in both groups (≥10: 61.73; <10: 62.88 years). No statistically significant differences in Schirmer's scores, corneal staining, TFBUT, or symptom severity were observed between the 2 disease duration subgroups (Table 2). Sum cooling scores after Rohto Hydra treatment, but not after Systane Ultra treatment, were significantly higher in patients with DED for <10 years (28.3 ± 2.58) compared to those with DED for >10 years (20.2 ± 2.76, P = 0.04, Fig. 3).
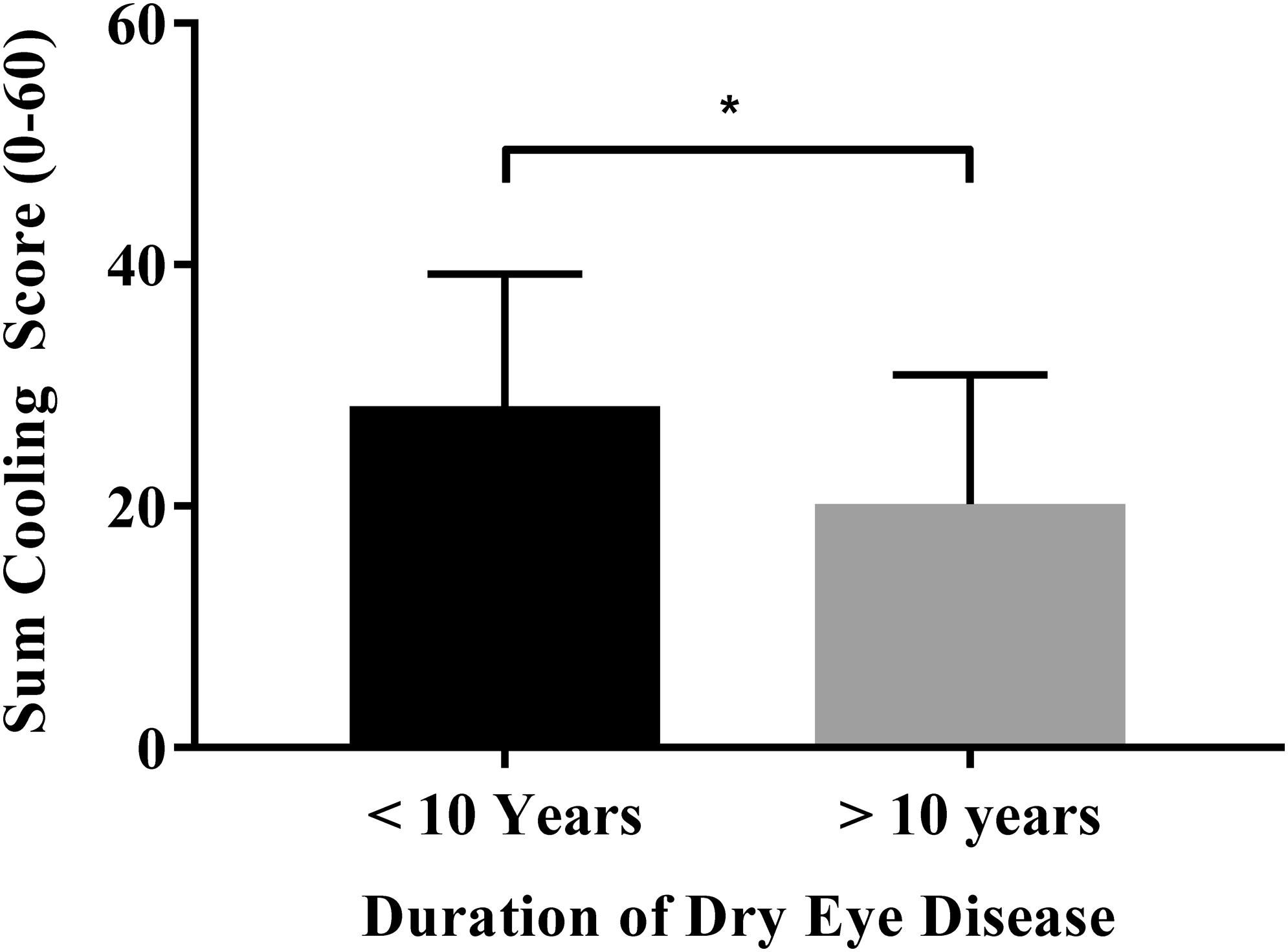
Mean (±SD) sum cooling scores (sum of 6 time points postdose, 0–10 point scale, range 0–60) after Rohto Hydra treatment. Comparisons between DED disease-duration subgroups were calculated using an unpaired, equal variance, t-test (asterisk indicates statistical significance <0.05).
Comparisons of mean differences were made using 2-tailed, equal variance t-tests (asterisk indicates statistical significance, P < 0.05).
TFBUT, tear film breakup time.
No statistically significant differences were demonstrated for cooling scores with either Rohto Hydra (P ≥ 0.42) or Systane Ultra (P ≥ 0.38) when DED subjects were categorized by age.
The correlations of cooling response to age were weak both in the DED group (R = −0.06) and in normal subjects (R = −0.09). Additional post hoc analyses were conducted by excluding the 5 youngest subjects in the normal group as well as excluding the 11 oldest subjects in the DED group to evaluate comparisons when the ages of the 2 groups were more closely matched (Table 3). In each of these subsets, the cooling response scores were similar to the total population and all P-values for every time point retained statistical significance.
This resulted in age-matched groups in both scenarios. The significance of the cooling response results was unchanged in these subgroups from what was found in the whole population.
Discussion
Signal transduction from corneal nerves begins with activation of transient potential receptor channels.11,34 Cold-sensitive neurons containing TRPM8 appear to be activated first when evaporation of the tear film causes cooling of the ocular surface.12,23–29,35 This cooling phenomenon has been shown to be accentuated in animal models of DED and can be triggered by application of menthol.10,23–26,36,37 Our study confirmed the presence of a greater sensitivity of cold receptors in DED subjects that was found in animal models of DED23–29,35,36 and in the application of menthol strips to the cheek in DED subjects. 24 Results did not appear to be affected by neurological cross talk, as the right and left eye data were not significantly different. Order of treatment also had no effect on the data, suggesting that the second instillation was not associated with any threshold change or memory response.
Although Cochet-Bonnet assessments are recognized to not be as sensitive at low thresholds of stimuli, 38 no differences in mechanoreceptor-mediated sensitivity were found between dry eye and normal subjects. This suggests that activation of TRPM8 receptors rather than corneal mechanoreceptors might have been the source of heightened sensitivity observed in this study. Heightened cooling responses to menthol may be caused by enhanced sensitivity of afferent cold thermoreceptors and/or upregulation of TRMP8 receptors, as is seen with chronic injury in polymodal nociceptors in the cornea and other body tissues.35–37,39–43 Normal subjects displayed a lesser, but still detectable cooling response, possibly due to normal basal firing of low-threshold thermoreceptors.
Although the literature suggests that age is the primary cause of decreased corneal sensitivity in DED patients,41–43 mean cooling scores were not correlated with age, corneal staining, or OSDI in either the DED or normal groups (Table 1). Cooling response to menthol did correlate with Schirmer's scores in DED subjects whose Schirmer's scores were reduced from normal. No similar correlation was observed in normal subjects. It is possible that this finding only in subjects with reduced tear production was more related to the confounding factor of a reduced tear volume not effectively diluting the menthol-containing eye drops, and as a consequence, the TRPM8 agonist may have had a longer residence time, and exaggerated the effects of the menthol drops.
Results of this study substantiate those of a previous study that showed a diminished and delayed reflex tearing response in dry eye subjects challenged with a controlled adverse environment (CAE). 44 The response continuum from normal subjects, to mild, moderate, and severe dry eye revealed an increasing delay in time to compensation within the CAE, and this phenomenon might relate to changes in TRPM8-mediated corneal sensitivity, as seen in this study.
In contrast to the limited effect of age on cooling sensitivity, the duration of DED appeared to significantly impact cooling responses. The decreased cooling sensitivity observed in subjects who had DED for an extended period of time (at least 10 years) may have been due to the prolonged effects of inflammation, decreased density of epithelial corneal cells, impairment of sensory nerves and/or TRPM8 downregulation, accessory gland dysfunction, and other disease-specific factors associated with prolonged DED. Interestingly, symptoms and all other signs, Schirmer's scores, TFBUT, and staining, were similar between the 2 disease-duration subgroups. Only the cooling response to the menthol-containing solution was significantly different and correlated with DED duration. This may point to a specific pathology associated with permanent anatomical changes to corneal nerves that is pathognomonic to DED of long duration.
This pilot study was limited by sample size, strict inclusion criteria for age range, and stratification of self-reported duration of duration of disease a priori, as well as unequal gender representation. Furthermore, while no subject spontaneously reported nasal cooling with menthol drops, activation of highly sensitive nasal mucosa might have occurred, and an effect on nearby tissues might have contributed to the overall perception of cooling, as well as provided insight to subjects on whom masked drops were administered. In addition, the comparison of commercially prepared drops, Rohto Hydra and Systane Ultra, is a weakness of this study since excipients may have influenced the results. Systane was selected for comparison based on a similar excipient list to that of Rohto Hydra. Confirmation of these findings with a menthol solution of similar concentration is warranted. Nevertheless, our analyses possessed the sensitivity to distinguish statistical differences between the DED and normal subjects, as well as the impact of disease duration on cooling responses.
In conclusion, results from this study confirmed our hypothesis and met our objectives by demonstrating that instillation of menthol-containing eye drops resulted in enhanced cooling sensations in DED subjects compared to normal subjects. This cooling sensation in response to menthol was diminished as the duration of DED progressed. These findings reveal new possibilities for future study of the role TRPM8-mediated sensory dysfunction plays in ineffective compensatory mechanisms like reflex tearing in dry eye, and how targeting these aspects of pathophysiology might benefit patients and simplify their dry eye diagnosis.
Footnotes
Acknowledgment
This study was 100% privately funded by Ora, Inc.
Author Disclosure Statement
All authors are employees of Ora, Inc. and have no conflicts of interest. M.B.A. is the Founder and Chief Scientific Officer of Ora, Inc. Ora, Inc. has received or is receiving financial consideration in connection with certain ocular allergy and dry eye therapeutics. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the article apart from those disclosed.