
Abstract
Abstract
Purpose:
To determine the frequency and economic impact of changing initial glaucoma therapy for patients with newly diagnosed open-angle glaucoma (OAG) or ocular hypertension (OHT).
Methods:
This retrospective longitudinal cohort study identified individuals within a large managed care network in the United States, who were newly diagnosed with OAG or OHT from 2001 to 2012 and were prescribed either a topical beta blocker (BB) or a prostaglandin analog (PGA). Claims data were analyzed over the 12-month period following their index prescription to determine physician prescribing habits, healthcare resource utilization patterns, and sociodemographic factors which may have contributed to changing the initial treatment strategy.
Results:
A total of 15,019 beneficiaries were identified with newly diagnosed OAG or OHT and whose index therapy was either a topical BB or PGA. Among these enrollees 80.9% were started on PGAs, while 19.1% were started on BBs. Of these beneficiaries, 29.2% of those started on PGAs and 39.5% of those started on BBs underwent a change in therapy within 12 months of their index prescription. Those in the topical BB treatment group had a 38% increased odds of changing glaucoma therapy relative to those started on PGAs (odds ratio [OR] 0.61, 95% CI:0.56–0.68). Patients who changed therapy required more frequent office visits (P < 0.0001) and incurred higher median eye care related charges (P < 0.0001) compared to those who remained on the index therapy unchanged.
Conclusions:
Changing initial ocular hypotensive therapy is common. Individuals who undergo a change in therapy required more frequent face-to-face monitoring and incurred higher healthcare related costs. Identifying strategies capable of optimizing the process of initiating ocular hypotensive therapy are appealing and possess the potential to improve patient outcomes and reduce healthcare costs.
Introduction
O
Although a variety of medical and surgical treatment options are available, topical IOP lowering medications remain the most common initial therapy for patients with OAG or OHT. Two of the most commonly prescribed classes of topical ocular hypotensives include beta blockers (BB) and prostaglandin analogs (PGA). Currently the initiation of ocular hypotensive therapy requires a trial-and-error approach because there are no recognized clinical markers which are capable of predicting an efficacious medication response or an undesirable side effect profile. Consequently, newly diagnosed OAG or OHT patients frequently require changes to their initial topical ocular hypotensive therapy. PGA induced hyperemia is a frequently reported adverse event, affecting 1 out of every 2.21 people. 7 Because PGA induced hyperemia was often cited as cause for changing a patient's medication, the estimated cost associated with changing therapy due to hyperemia resulted in nearly twice the annual medication cost to the patient ($73.67 hyperemia free patients vs. $140.02 for patients who changed therapy due to hyperemia).
However, clinical experience suggests that the impetus for changing the initially prescribed medication encompasses a wide range of reasons, including unbearable side effects, inadequate IOP control, mediation noncompliance, exorbitant medication costs, as well as many others. Although other studies have attempted to quantify the cost of changing therapy in relationship to a single side effect, such as hyperemia, we are unaware of a study which attempts to quantify the all-cause rate of changing initial therapy for newly diagnosed patients with OAG or OHT. In this study, we developed a claims based model to more completely evaluate how frequently medication changes occur, if these changes altered healthcare resource utilization patterns, and the cost associated with changing the initially prescribed therapy. We hypothesized that a significant percentage of individuals with newly diagnosed OAG or OHT who are started on either a topical BB or PGA will undergo a change in their index therapy within 12 months of starting the medication.
Methods
Data source, subject identification, procedure, and pharmacy tracking
The Clinformatics Data Mart dataset (Optum, Eden Prairie, MN) captures patient billing records from within a large managed care network located in the United States. Using International Classification of Diseases, Ninth Revision Clinical Modification (ICD-9-CM) codes for eye-related diagnoses (360–379.9), and Current Procedural Terminology (CPT-4) codes (65091–68899 or 92002–92499), as well as any other claim submitted by an ophthalmologist or optometrist, we identified individuals who had eye-related visits, diagnoses, and therapeutic procedures between January 1, 2001 and December 31, 2012. We also had access to sociodemographic data (age, sex, race/ethnicity, education level, household income, and region of residence) and outpatient prescriptions. Patient records were deidentified, thus this study met exemption criteria from the University of Michigan's Institutional Review Board and the work was approved as a nonregulated study. This research project adhered to the tenets set forth by the Declaration of Helsinki.
Inclusion and exclusion criteria
We identified enrollees diagnosed with OAG (primary, pigmentary, and exfoliation) or OHT within 3 years before the initial prescription of either a topical BB or a PGA (Fig. 1). Additional inclusion criterion required that the enrollee was continuously enrolled in the plan for 3 years before the patient's index prescription of either a topical BB or PGA. During the 3 year “look-back” period, individuals were excluded if they were started on any IOP lowering medication, had laser or incisional glaucoma surgery, or had refractive surgery. In addition, individuals were excluded from analysis if any nonglaucoma related laser or incisional surgery was performed during the first year after the initial prescription.
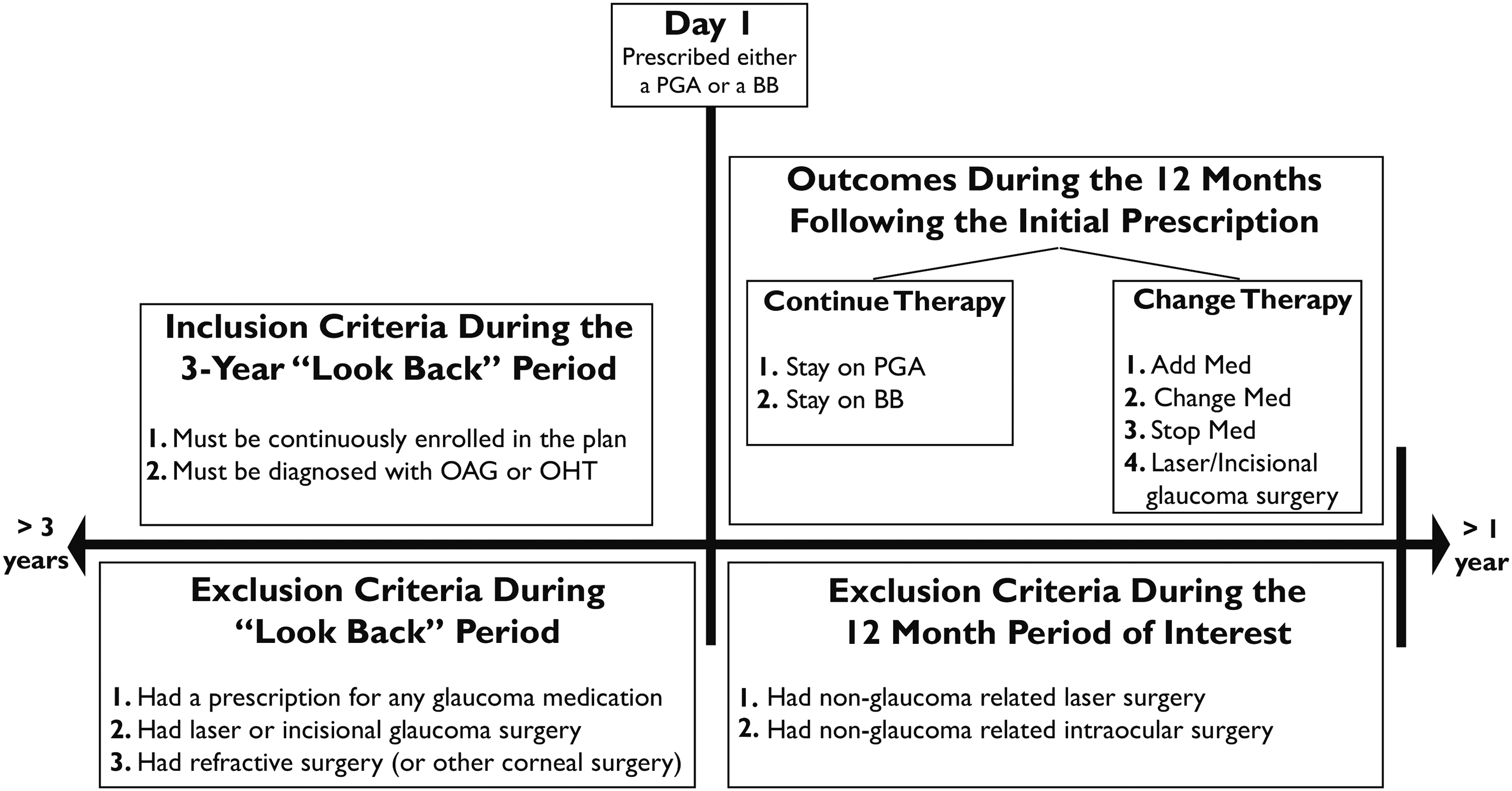
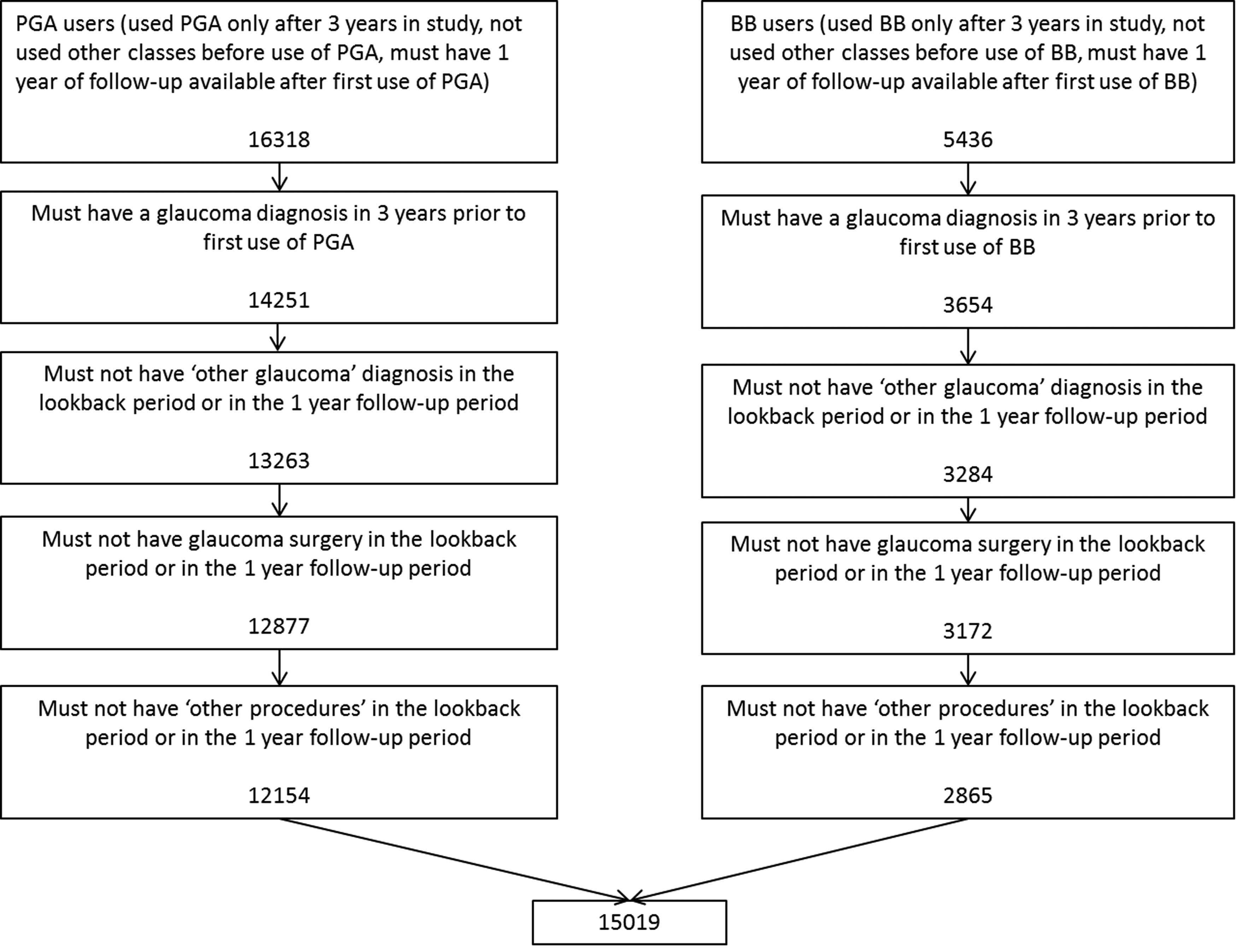
Schematic of Clinformatics Data Mart Dataset Query. The schematic depicts how the cohort of enrollees was selected from within the Clinformatics dataset.
Next, the eligible enrollees were divided into 2 groups based upon their index prescription (Group 1- started on a topical BB; Group 2- started on a topical PGA). The outcome measure within these 2 groups was a change in the index therapy within 12 months after starting either a topical BB or a PGA (Fig. 2). Importantly, a change in therapy was defined as the addition of another class of ocular hypotensive, a change in medication, cessation of all therapy, or if the enrollee required laser or incisional glaucoma surgery.
Schematic of our sample selection based on inclusion and exclusion criteria.
Statistical analysis
Analysis was performed using SAS 9.4 (SAS Institute, Cary, NC). Demographic characteristics were summarized using frequencies and percentage for categorical variables and means and standard deviations for continuous variables. Mean and median values were calculated for number of office visits and the charges submitted for those office visits during the 12 months after starting therapy. Multivariable logistic regression analysis was used to explore whether the odds of continuing initial treatment were associated with age, sex, race/ethnicity, education level, household income, or region of residence of the enrollees.
Results
Among the 15,019 beneficiaries who met our study criteria, the mean age (±standard deviation) was 61.2 (±12.6) years, with 75% identified as white and 53.6% identified as female. In this cohort, 12,154 (80.9%) patients were started on PGAs, while 2,865 (19.1%) were started on topical BBs. Of the 12,154 enrollees started on PGAs, 29.2% had a change in therapy within 12 months of initiating therapy. Among those started on topical BBs, 39.5% of the 2,865 enrollees changed therapy within the 12 month period of interest.
Individuals who had a change in initial PGA therapy were seen on average 0.7 more times per year (P < 0.0001) and incurred $54 more in median charges per year than those who remained on the initial PGA therapy unchanged. This finding was consistent in the topical BB group, where individuals who had a change in therapy were seen 0.9 times more often per year (P < 0.0001) and accrued $67 more in median charges than those who did not require a change in their initial therapy (Fig. 3).
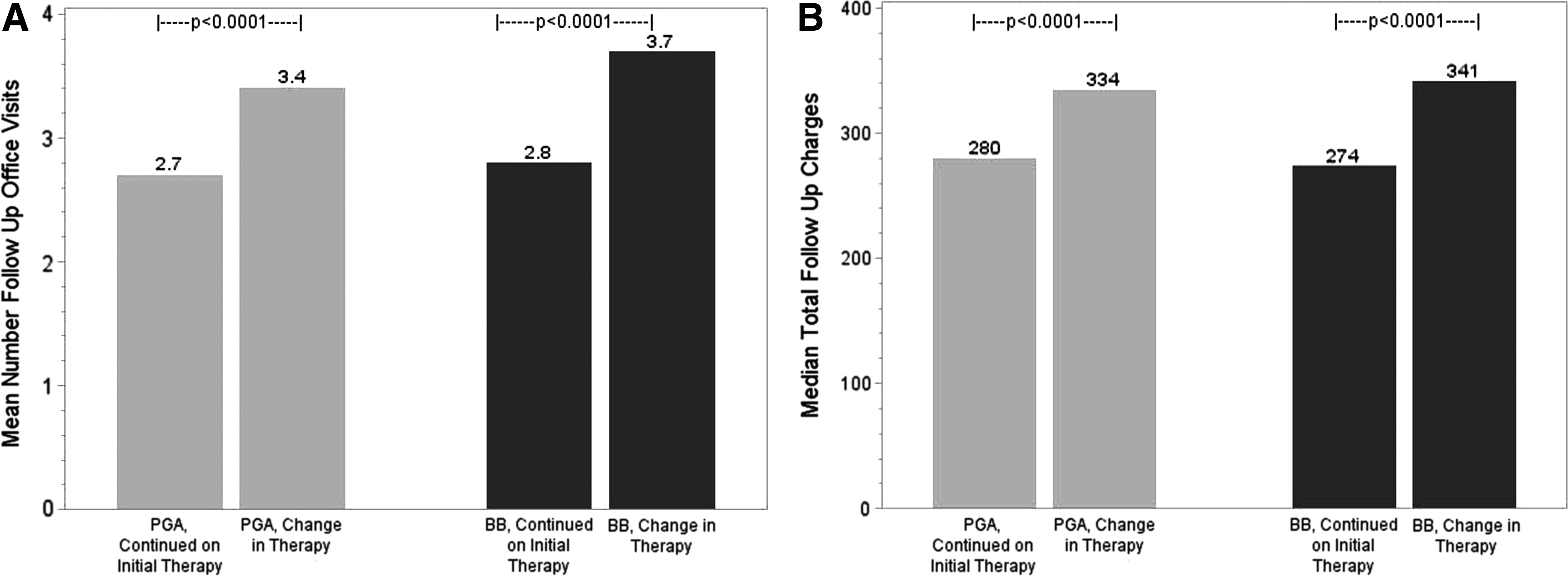
Change in initial therapy results in more frequent office visits and higher costs to the patient.
Next we used multivariable logistic regression analysis to determine the impact of sociodemographic factors on medication persistence within the first year of starting either a BB or PGA. We found that patients started on topical BB had 38% lower odds of continuing treatment unchanged (odds ratio [OR] 0.617, 95% CI:0.563–0.676) compared to a patient started on a PGA (Fig. 4). Enrollees of Black race (OR 0.821, 95% CI:0.732–0.921) and Latino ethnicity (OR 0.800, 95% CI:0.687–0.931) had 18% and 20% lower odds, respectively, of continuing treatment unchanged compared to White enrollees. In contrast, patients in 3 (out of 4) of the highest income categories had an increased odds of remaining on the initial medication unchanged over the 12-month period of interest compared to those in the lowest income category. Finally, if we held other covariates equal, we found that for each additional year of age at first medication, the odds of continuing treatment unchanged went up by 0.6% (OR 1.006, 95% CI:1.003–1.009).
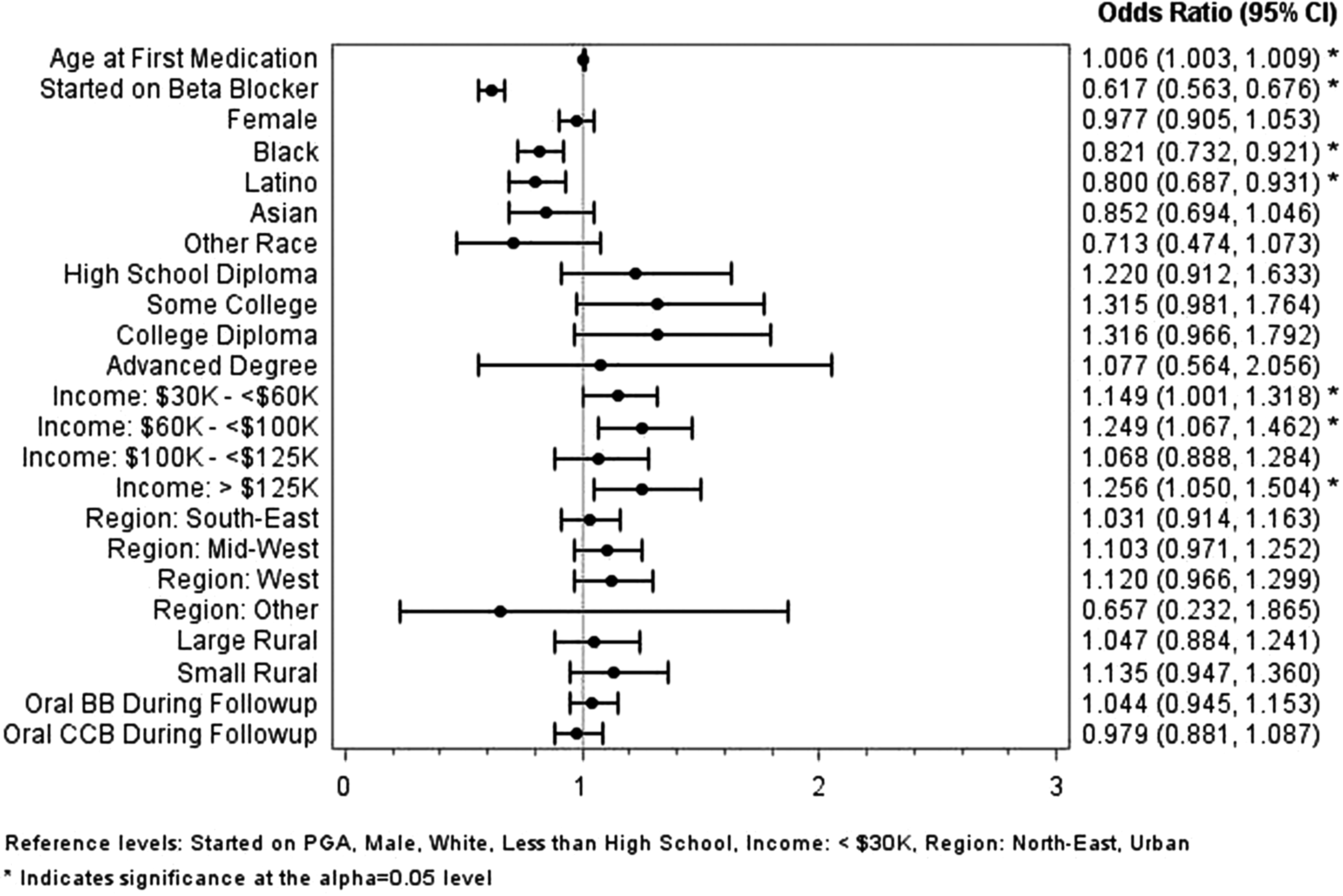
Forest plot of sociodemographic covariates. Above are sociodemographic factors that increase or decrease the odds of requiring a change in therapy within the first of initiating topical intraocular pressure lowering therapy.
Discussion
Based on our analysis of claims data from a large US managed care network, the vast majority of eye care providers are initially prescribing patients PGAs (80.9%) rather than BBs (19.1%). Interestingly, 29.2% of patients started on a PGA and 39.5% of patients started on a topical BB required a change in therapy within 12 months of the index prescription. Enrollees who had a change in therapy were seen for office visits 0.7 and 0.9 more times per year in the PGA and topical BB groups, respectively. Not surprisingly, individuals had medication changes and were seen more frequently for office visits and incurred higher median charges per year; $54 more dollars per year in the initial PGA treatment group and $67 more dollars per year in the initial topical BB treatment group.
These results are consistent with previous studies that showed that ∼30% of patients started on glaucoma medications required a change in therapy with 12 months.8–10 In another health insurance claims dataset with 5,300 individuals with glaucoma or glaucoma suspect status, nearly 50% of patients on topical glaucoma therapy had discontinued their medication within 6 months of the index treatment. 11 These results for multiple studies highlight the significant and clinically relevant role that medication compliance and adherence plays in topical glaucoma therapy. Furthermore, Oostenbrink et al. 12 and Denis et al. 13 both reported that changes in glaucoma drug therapy resulted in (or predicted) significantly higher yearly costs. Both studies reported that changing medications and more frequent office visits were found to be major contributors to the annual cost of treatment for glaucoma patients.
Currently there are no predictive markers which can help eye care providers determine the appropriate initial medication for newly diagnosed OAG and OHT patients. To gain insight into this issue, we used multivariable logistic regression analysis to evaluate factors which increased or decreased the odds of remaining on the index medication unchanged. We found that being started on a BB was associated with a 38% increased odds of changing the initial therapy within 12 months. The exact reason for this increased odds cannot be determined from insurance claims data because it lacks clinical information, therefore we cannot clearly evaluate physician decision making. But it stands to reason that side effects and dosing regimens likely contributed to changes in therapy.
Supportive to this notion is the fact that topical BBs have a well-known association of serious side effects in patients with pulmonary and cardiac disease. In fact, estimates show that 50%–60% of patients on topical BB had a contraindication to their use.14,15 This suggests that the inadvertent use of topical BBs in patients with contraindications may occur more frequently than expected. While there remains controversy regarding the frequency of serious adverse events for patients started on topical BB, a recent study by Schmier et al. showed that patients who were started on topical BB therapy and then discontinued its use had more frequent hospitalizations and incurred higher yearly costs. 16 Given that roughly 40% of patients started on BB will undergo a change in therapy within 12 months, it is of paramount importance to develop ways to accurately initiate topical ocular hypotensive therapy and facilitate medication persistence.
Even if serious adverse events did not contribute to the increased odds of changing therapy after being started on a BB, previous research has shown that medication compliance and vision related quality of life are intimately associated with glaucoma medication regimens.17–19 Thus, practically speaking, the commonly used twice daily dosing schedule of many BBs versus the once daily dosing schedule of PGAs likely contributed to the increased odds of changing therapy in the topical BB cohort. However, without clinical data we were not able to ascertain with certainty if cost, efficacy, medication compliance, unbearable side effects, or other factors were responsible for the increased odds of changing therapy after being started on a topical BB.
We also used multivariable logistic regression analysis to evaluate sociodemographic factors which influenced the odds of remaining on the index therapy unchanged. We found that being of either a Black race or Latino ethnicity was associated with a decreased odds (18% and 20%, respectively) of remaining on the medication unchanged during the first year of therapy. Previous studies have identified a relationship between medication adherence and race.18,20–22 These studies have shown that individuals of non-white race had higher rates of medication noncompliance. In both the African American and Latino populations, glaucoma remains a leading cause of blindness, suggesting that medication noncompliance may play a clandestine role in disease progression requiring patients to undergo a change in therapy shortly after starting IOP lowering medications.
In addition, it is well known that topical BB, specifically timolol, is readily bound by melanin which effectively reduced the ocular bioavailability of the medication,23,24 suggesting another potential reason why African Americans and Latinos, who generally speaking have a higher concentration of melanin in the eye, may have a decreased odds of remaining on the index therapy unchanged.
Multivariable logistic regression analysis also uncovered that enrollees in 3 out of 4 of the highest income groups had an increased odds of staying on the index therapy unchanged during the 12-month period of interest. Previous studies on medication compliance identified an association with education and socioeconomic status. 25 Again, medication noncompliance in the lower income level may have contributed to the frequency of changing initial therapy. Another factor to consider for medication persistence is the availability of generic glaucoma medications. During the 11-year data period the generic BBs were available. The generic forms of latanoprost were approved in 2011, but it is difficult to know when these became available in the retail market. As the potential time of available latanoprost generics is short compared to the 11-year study period, we are unable to assess the impact of lower cost generic alternatives for the PGAs.
Finally, clinical experience suggests that variation in IOP response to topical ocular hypotensives was almost certainly a contributing factor. 26 In fact, a recent meta-analysis from van der Valk et al. showed that PGAs had a higher rate of IOP reduction than topical BB. 27 Perhaps this contributed to the increased odds of changing therapy for enrollees started on a topical BB. But inconsistent IOP response is not solely linked to topical BBs; in fact, Schwartz et al reported that 43% of patients in the Glaucoma Adherence and Persistence Study (GAPS) switched medications because of lack of efficacy. 7 Other studies have indirectly addressed the issue of medication nonresponse by assessing the benefit of adjunctive IOP lowering therapy when topical monotherapy failed to control adequately IOP.28–30 Finally, in a retrospective analysis of the US Latanoprost Study Group, Cameras and Hedman reported that 20% of latanoprost treated and 31% of timolol treated patients failed to achieve IOP lowering greater than 15% from baseline after 2 weeks of treatment. 31
A direct comparison between clinical trial derived nonresponder rates and our “change in therapy” designation would be inappropriate. This is, in part, because our goal was to identify the all-cause rate of medication change for newly diagnosed OAG and OHT patients who were started on a topical BB or PGA. Thus our inclusive definition of “change in therapy” does not discriminate between individuals who had intolerable side effects, poor compliance, could not afford the medication, and those who did not have an adequate IOP response to the index therapy. In addition, we cannot determine from the information presented which medication should be started in a given patient; for the time being this decision remains up to the physician's discretion. However, a frank discussion regarding medication cost, dosing schedules, side effects, and IOP goals should help guide the process of medication initiation.
Yet, despite these limitations both our claims data and data from clinical trials have demonstrated a clear need to develop more targeted approaches to initiating glaucoma medical therapy. As there are no predictive clinical markers for medication treatment response, our future research will focus on quantitative trait analysis of IOP regulation using measures of aqueous humor dynamics, given the success of this approach for IOP.32–35 The potential benefits of this approach include expedited treatment optimization for patients and reduced healthcare associated costs both at the level of individual and that of society at large.
The trial-and-error approach to the medical management of patients with OAG and OHT results in a substantial number of patients who change therapy within 12 months of their initial prescription. This change in therapy results in more frequent office visits and higher yearly charges. Given the prevalence of OAG and OHT, the economic impact of changing the initial therapy for newly diagnosed OAG and OHT patients is tremendous. Future research that identifies biomarkers predictive of treatment response is an appealing strategy that may improve patient care and potentially reduce healthcare costs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.