
Abstract
Abstract
Purpose:
To evaluate the effects of dexamethasone intravitreal implant (Ozurdex) and identify risk factors for repeated treatment in patients with macula edema due to branch retinal vein occlusion (BRVO) or central retinal vein occlusion (CRVO).
Methods:
Patients followed up for at least 6 months were enrolled from 2013 to 2016. Dexamethasone intravitreal implant was given as the baseline treatment. For evaluation of dexamethasone intravitreal implant effects and complications, the demographics, medical history, best-corrected visual acuity (BCVA), intraocular pressure, and central retinal thickness (CRT) were recorded. Multivariate Cox proportional hazard model and logistic regression were used to identify factors for repeated treatment.
Results:
Twenty-three BRVO and 11 CRVO patients were enrolled. There were 15 males and 19 females. Fifteen (44.12%) patients needed only one dexamethasone intravitreal implant. The peak CRT and BCVA significantly improved. Comparing single-injection with multiple-injection group, age and initial CRT more than 400 μm were significantly higher in the multiple-injection group. From multivariate logistic regression and Cox proportional hazards analysis, patients with age older than 55 years and initial CRT more than 400 μm had higher risk for multiple injections.
Conclusions:
Patients receiving as-needed schedule of dexamethasone intravitreal implant had significant peak CRT and BCVA improvement. Age older than 55 years and initial CRT more than 400 μm were significant risk factors associated with repeated dexamethasone intravitreal implant treatment.
Introduction
R
Intravitreal injections are the most direct method to deliver medication into the posterior segment. Recently, intravitreal medications, including corticosteroids8–11 and anti-vascular endothelial growth factor (anti-VEGF) agents,12–19 have changed the treatment paradigm for many sight-threatening retinal diseases such as wet age-related macular degeneration, diabetic ME, and RVO.
Currently, 3 treatment options have been approved by the US Food and Drug Administration for the treatment of ME secondary to CRVO and BRVO, including a dexamethasone intravitreal implant (Ozurdex; Allergan, Irvine, CA),8–11 ranibizumab (Lucentis; Genentech, Inc., South San Francisco, CA),12–15 and aflibercept (EYLEA-Regeneron Pharmaceuticals, Inc., Tarrytown, New York, NY, and Bayer Healthcare Pharmaceuticals, Berlin, Germany).16–18 Intravitreal bevacizumab (Avastin; Genentech, Inc.) has also been used off label to treat RVO. 19
Repeated intravitreal anti-VEGF injections when recurrent ME results in worsening vision are a burden on medical care systems. 11 Among these drugs, Ozurdex has the longest duration of action of up to 4–6 months. Macular ischemia might affect results in patients after treatment with Ozurdex. Indeed, there's post hoc analysis of pooled data from 2 randomized, controlled trials about the effect of the duration of ME on clinical outcomes in RVO treated with Ozurdex. 20 They concluded longer ME duration (6 weeks' duration or more) at the time of first treatment with Ozurdex was associated with a significantly lower likelihood of achieving clinically meaningful improvements in vision or central retinal thickness (CRT) after treatment.
Therefore, we conducted this retrospective case series study to evaluate the effects, duration of action, and safety of injections of Ozurdex. In addition, we tried to identify possible risk factors for repeated treatment with regards to ophthalmological outcomes based on an as-needed schedule according to evidence of disease flare-ups on spectral-domain optical coherence tomography (OCT; Heidelberg Engineering, Heidelberg, Germany) in patients with ME due to CRVO or BRVO.
Methods
This is a retrospective, interventional case series study. From 2013 to 2016, many patients with a diagnosis of ME due to CRVO or BRVO received the treatment of intravitreal implants of Ozurdex at China Medical University Hospital. For analysis of this study, we scrutinized all the medical records related to this topic with final selection of cases with the following strict criteria: (1) a diagnosis of ME with a baseline CRT of more than 300 μm due to CRVO or BRVO, (2) vision loss resulting from ME after RVO were of less than 6 weeks' duration, (3) the diagnosis of ME secondary to CRVO or BRVO confirmed by 3 senior retinal subspecialists (C.J.L., J.M.L., and W.L.C.), (4) OCT graders were blinded to treatment, (5) implants of Ozurdex were given as the baseline treatment, and (6) patients of RVO receiving at least one treatment of Ozurdex and following up for at least 6 months.
Postvitrectomy, glaucoma, diabetic retinopathy, or diabetic ME patients were excluded. History of use of steroids via other ways, laser treatment or intravitreal anti-VEGF injection for RVO before Ozurdex, was also excluded. Not all diabetic patients have diabetic retinopathy; however, diabetic patients may have a chance to get RVO. The Institutional Review Board approved the study protocol. The study was performed in accordance with the World Medical Association's Declaration of Helsinki. Written informed consent was obtained from all patients.
Pupils were dilated with 0.5% tropicamide/0.5% phenylephrine (Mydrin-P; Santen OY, Finland), and the topical antibiotic levofloxacin (Cravit; Santen Pharmaceutical Co., Osaka, Japan) was applied before the intravitreal injections. Topical anesthesia was achieved using 0.5% proparacaine hydrochloride (Alcaine; Alcon Pharmaceuticals), given 3 times with 2-min intervals before the intravitreal injections. Each eye was prepared in a sterile manner using 5% povidone/iodine. The medication was injected intravitreally via the pars plana (3.5 mm away from the limbus). After the injection, the intraocular pressure (IOP) and retinal artery perfusion were checked, and the patients received topical levofloxacin 4 times daily for 7 days.
All cases were followed up in monthly schedule. Best-corrected visual acuity (BCVA), IOP, and OCT were recorded every month during the follow-up period. The demographic data, medical history, including diabetes and hypertension, ocular diagnosis (BRVO or CRVO), BCVA (approximate Early Treatment Diabetic Retinopathy Study [ETDRS] letter scores), 21 IOP, and CRT by OCT, were recorded for each patient throughout the study period from medical records, as well as the occurrence of any complications. Patients whose IOP exceeded 25 mmHg at any visit were evaluated and treated accordingly. Patients were eligible for retreatment with Ozurdex if their retinal thickness increased by 50 μm from the lowest recorded level. Further doses of Ozurdex were given if ME recurred as identified by OCT.
As for the statistical methods, the time to additional Ozurdex treatment was analyzed using Kaplan–Meier analysis and risk factors were identified using Cox proportional hazard analysis. Multivariate logistic regression analysis was used to identify possible risk factors for repeated treatment.
Results
Thirty-four patients who have received Ozurdex for ME due to RVO and were followed up for at least 6 months were enrolled, with BRVO being the underlying etiology in 23 patients (67.65%) and CRVO in 11 patients (32.35%) (Table 1). There were 15 males (44.12%) and 19 females (55.88%) with a mean age of 57.94 ± 13.67 years. Twenty-nine patients (85.29%) were phakic, and 5 (14.71%) were pseudophakic at baseline. The mean follow-up period was 14.59 ± 8.05 months. The baseline data between BRVO and CRVO patients showed no significant difference (Table 1).
Comparing the BRVO and CRVO groups.
BCVA, best-corrected visual acuity; BRVO, branch retinal vein occlusion; CRT, central retinal thickness; CRVO, central retinal vein occlusion; DM, diabetes mellitus; IOP, intraocular pressure.
During the study period, 15 (44.12%) patients received only one dose of Ozurdex due to being in a stable condition, 15 (44.12%) received 2 doses, 2 (5.88%) received 3 doses, 1 (2.94%) received 4 doses, and 1 (2.94%) received 6 doses due to recurrent ME. Comparing single-injection with multiple-injection group, age, initial CRT, and proportion of diabetes mellitus were significantly higher in multiple-injection group (Table 2). For evaluation of possible factors which might influence the interval to second treatment, some initial conditions were analyzed among those 19 patients receiving more than one injection. We found that interval to second treatment was significantly shorter for patients with initial CRT ≥400 μm when compared with those with initial CRT <400 μm (Table 3). The mean duration between the first and second injections of Ozurdex in patients of initial CRT ≥400 μm was 4.24 months and in patients of baseline CRT <400 μm was 9.42 months (P = 0.0042, <0.05). There was no significant difference in risk between the BRVO and CRVO groups in analysis of the patients stratified by a diagnosis of RVO (P = 0.452).
Comparing single-injection with multiple-injection groups; * P < 0.05.
Comparing different status of each baseline data; *P < 0.05.
The peak change in CRT of all the 34 patients after the Ozurdex treatments were −220.6 ± 168.8 μm (459.15 ± 164.22 μm to 238.59 ± 56.39 μm, P < 0.001, Fig. 1). The final change in CRT after Ozurdex treatments were −156.3 ± 158.2 μm (459.15 ± 164.22 μm to 302.88 ± 91.21 μm, P < 0.001, Fig. 2). Overall, 20.59% of the patients had a CRT under 250 μm after Ozurdex treatments. The CRT showed a significantly more reduction in the BRVO than the CRVO group after the Ozurdex treatments (Fig. 3).
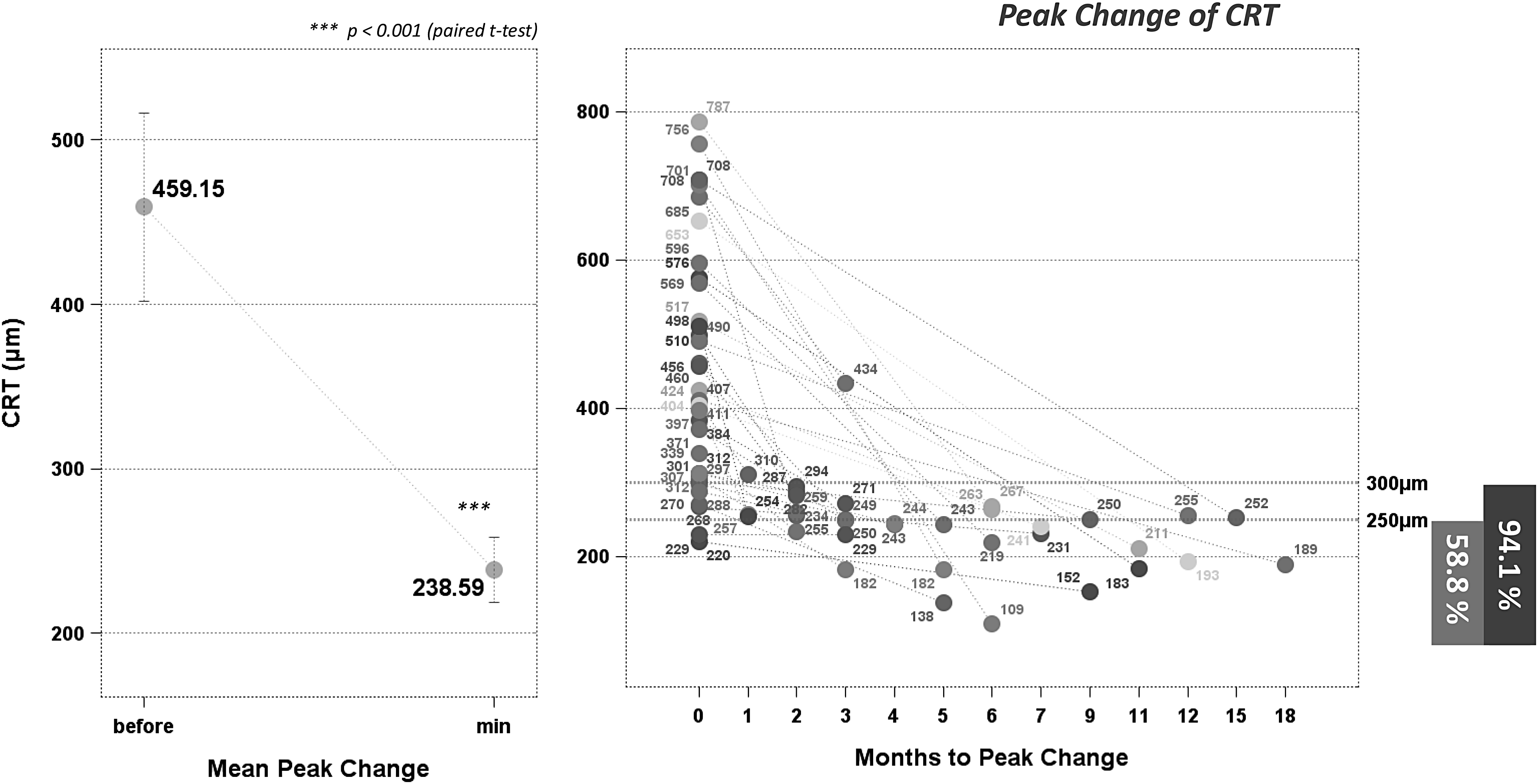
The peak change in CRT of all the 34 patients after the Ozurdex treatments was −220.6 ± 168.8 μm (459.15 ± 164.22 μm to 238.59 ± 56.39 μm, P < 0.001). The CRT in 58.8% patients could be achieved under 250 μm, and 94.1% could be achieved under 300 μm. CRT, central retinal thickness.

The final change in CRT after Ozurdex treatments was −156.3 ± 158.2 μm (459.15 ± 164.22 μm to 302.88 ± 91.21 μm, P < 0.001). The final CRT in 20.59% patients could be achieved under 250 μm, and 64.71% could be achieved under 300 μm.
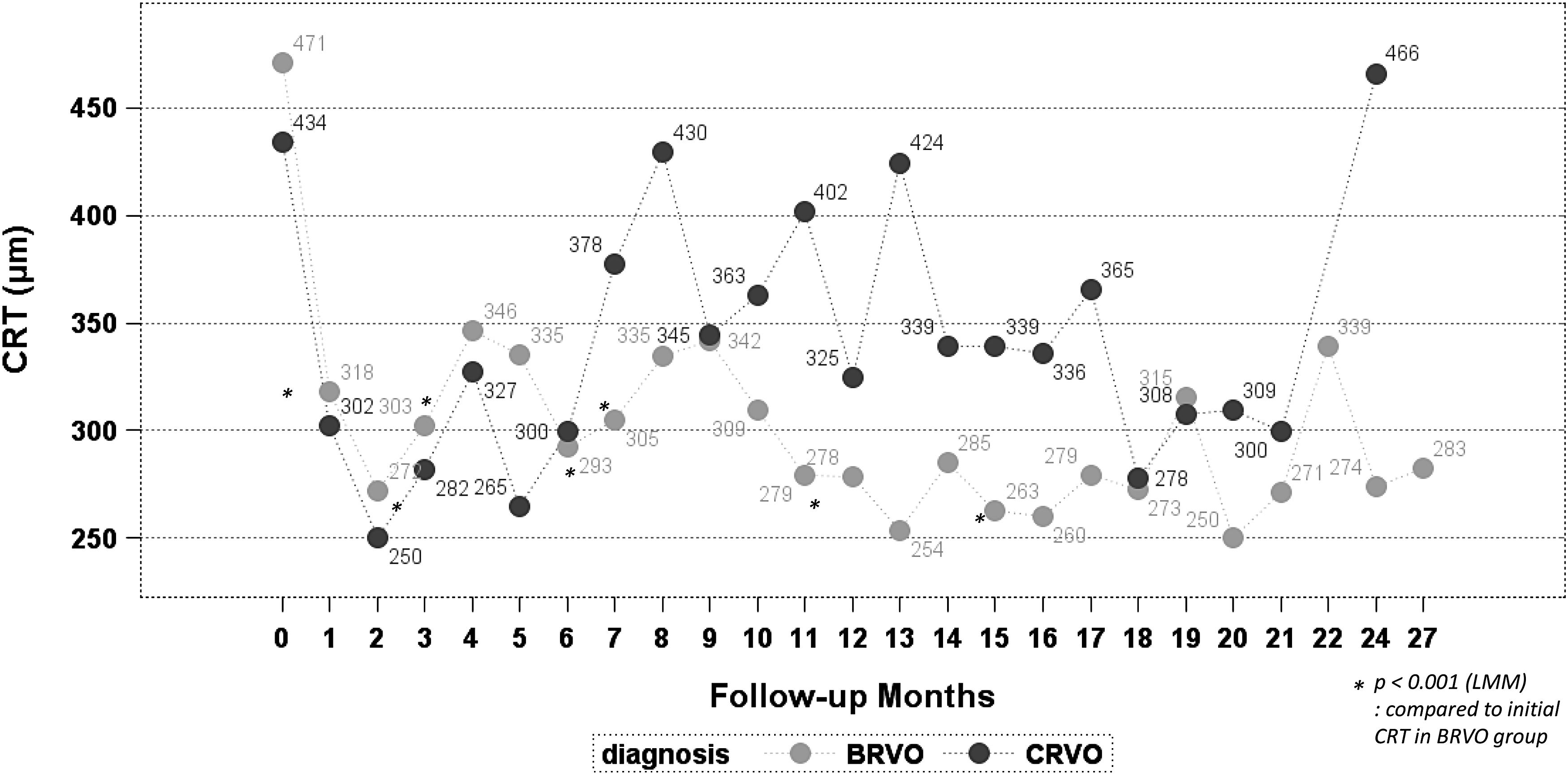
The CRT showed a significantly more reduction in the BRVO than the CRVO group after the Ozurdex treatments. BRVO, branch retinal vein occlusion.
The peak change in BCVA (approximate ETDRS letter scores) of all the 34 patients after the Ozurdex treatments were 21.76 ± 24.82 letters (37.38 ± 30.34 to 59.15 ± 28.46 letters, P < 0.001, Fig. 4). The final change in BCVA after Ozurdex treatments were 4.44 ± 38.11 letters (37.38 ± 30.34 to 41.82 ± 46.76 letters, Fig. 5).
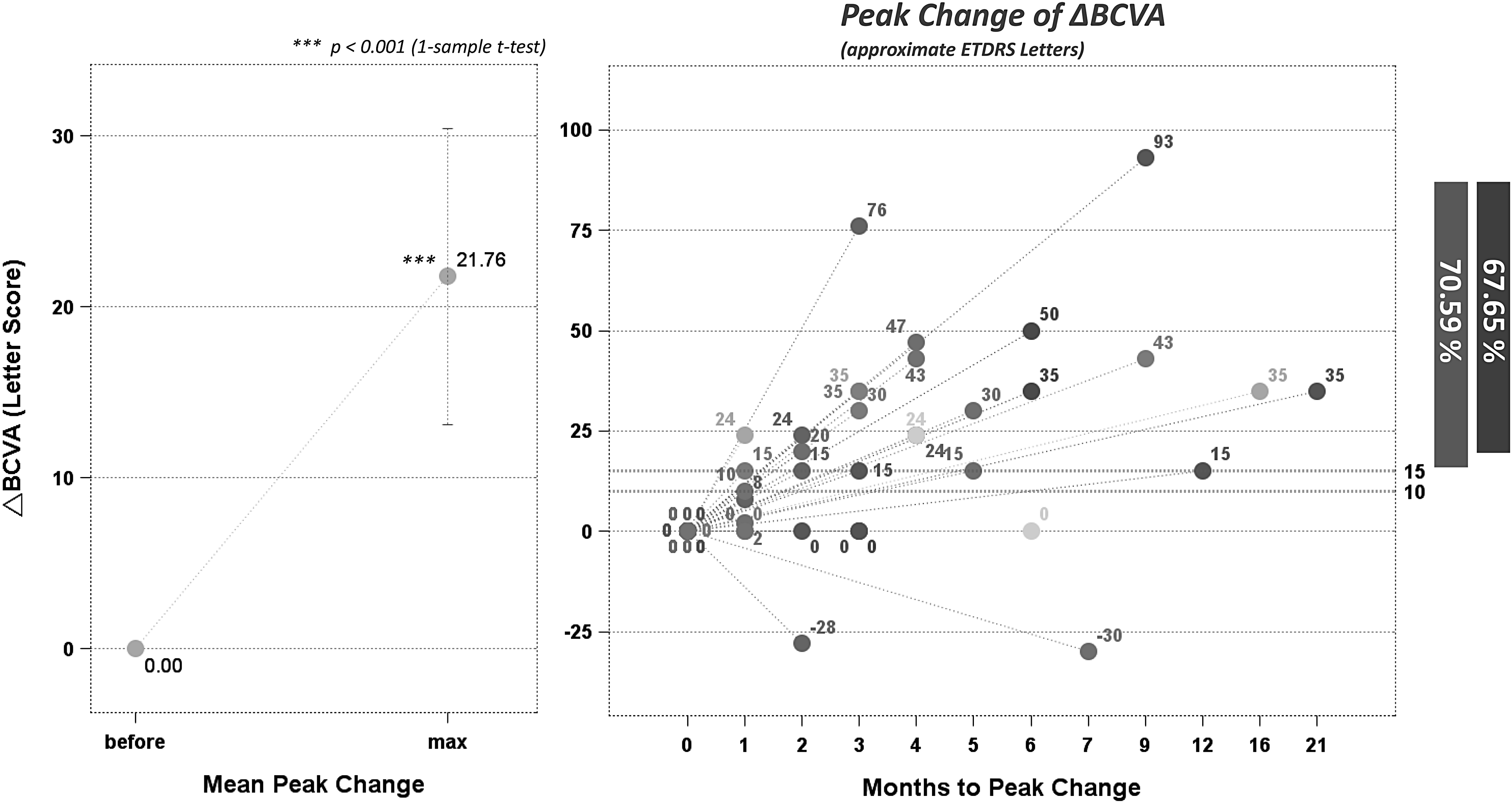
The peak change in BCVA (approximate ETDRS letter scores) of all the 34 patients after the Ozurdex treatments was 21.76 ± 24.82 letters (P < 0.001). The peak BCVA improvement in 70.59% patients could be achieved more than 10 letters, and 67.65% could be achieved more than 15 letters. BCVA, best-corrected visual acuity; ETDRS, Early Treatment Diabetic Retinopathy Study.
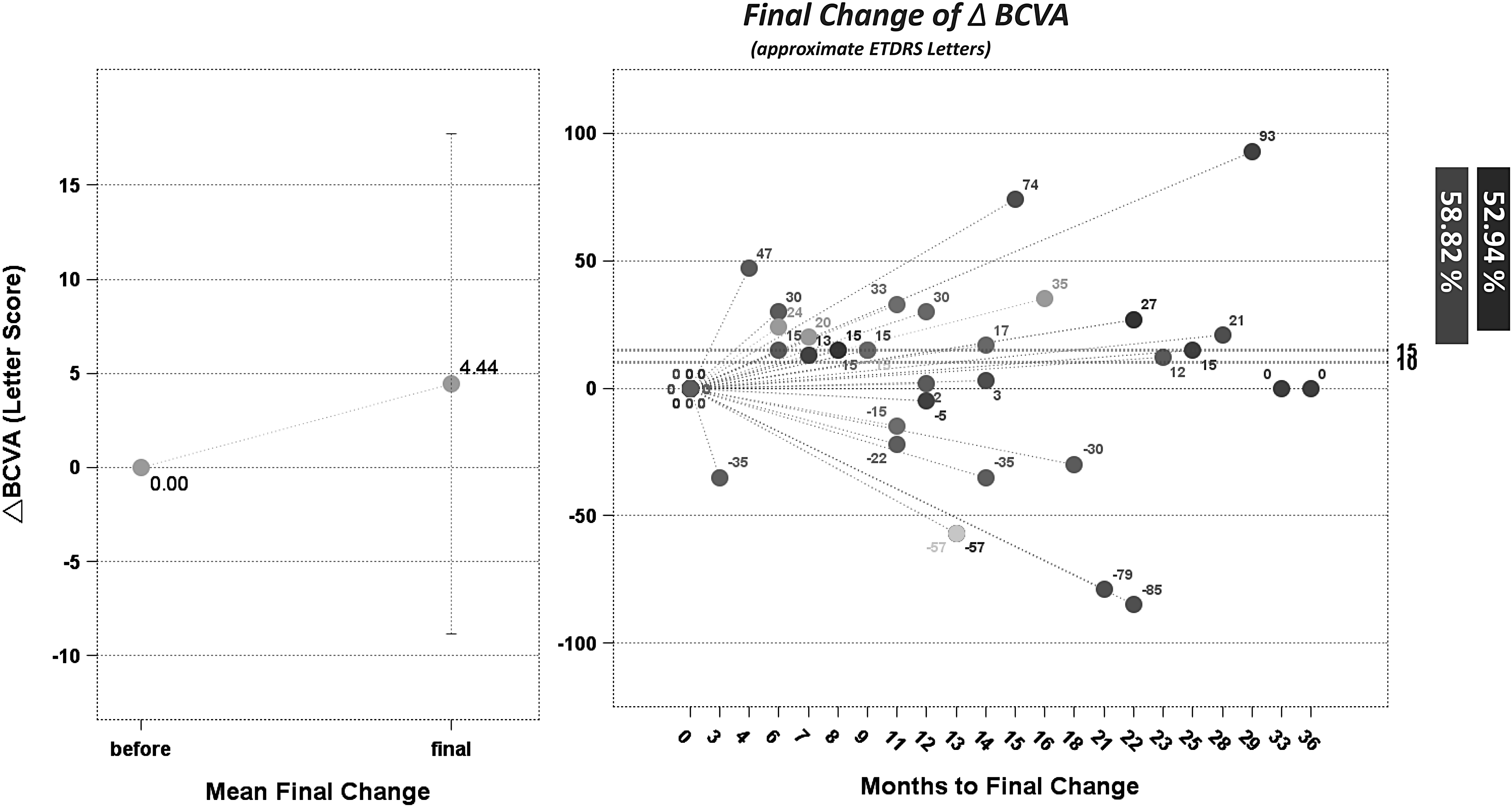
The final change in BCVA (approximate ETDRS letter scores) of all the 34 patients after Ozurdex treatments was 4.44 ± 38.11 letters. The final BCVA improvement in 58.82% patients could be achieved more than 10 letters, and 52.94% could be achieved more than 15 letters.
Overall, 72.22% of the patients had BCVA ≥15 approximate ETDRS letters improvement after Ozurdex treatments. For all 34 patients, the BCVA showed a significantly better final BCVA improvement in the BRVO (+18.00 letters) than the CRVO (−23.91 letters) group after the Ozurdex treatments. The improvement in BCVA occurred mainly in the patients with BRVO, but not CRVO.
Using the second treatment of Ozurdex as a final event, survival analysis was applied. Kaplan–Meier analysis revealed that the median time to the second Ozurdex treatment for all 34 patients was 9.76 months. We performed further analysis stratified by age and found that the median time to the second Ozurdex treatment in the group older than 55 years was 4.23 months, and in the group younger than 55 years, the median time to second treatment was greater than 30 months. The difference was statistically significant (P = 0.0009, Kaplan–Meier analysis) (Fig. 6). Actually, in the younger group, more than 80% only needed one injection during follow-up. This meant that the group of patients with age ≥55 years had a higher risk for second treatment when comparing with the patients with age <55.
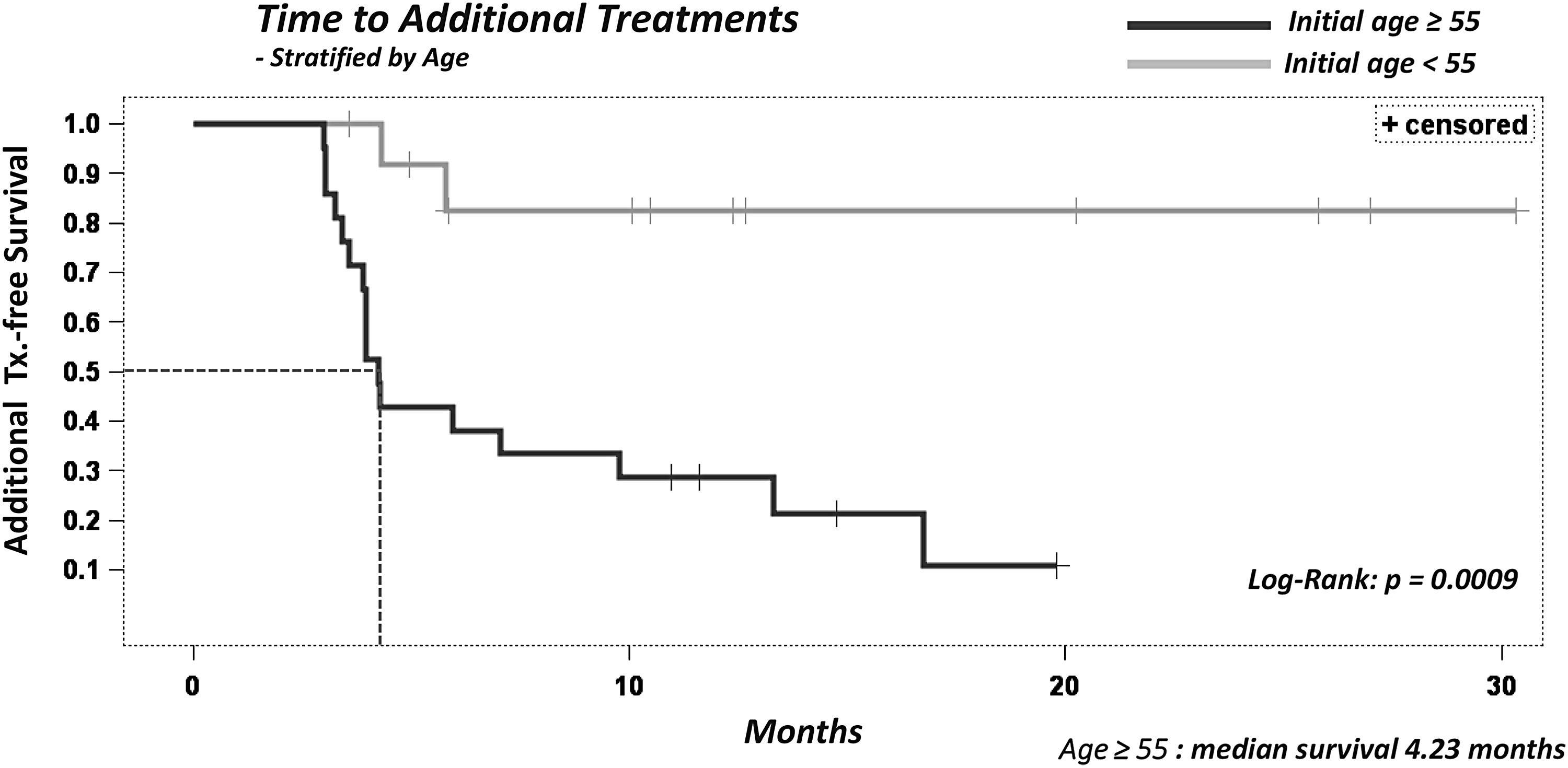
The median time to the second Ozurdex treatment in the group of age older than 55 years was 4.23 months. In the group of age younger than 55 years, more than 80% only needed one injection during follow-up. The difference was statistically significant (P = 0.0009, Kaplan–Meier analysis).
Also, we performed further analysis after stratifying the patients by initial CRT ≥400 μm or <400 μm and found that the median time to the second Ozurdex treatment in those with initial CRT ≥400 μm was significantly shorter compared with those <400 μm. The median time to the second Ozurdex treatment in the initial CRT ≥400 μm group was 4.12 months and in the initial CRT <400 μm group, the median time to second treatment was greater than 30 months. The difference was statistically significant (P = 0.008, Kaplan–Meier analysis) (Fig. 7). Actually, in the initial CRT <400 μm group, more than 50% only needed one injection during follow-up. This meant the group of patients with initial CRT ≥400 μm had a higher risk for second treatment when comparing to the patients with initial CRT <400 μm. The median time to the second Ozurdex treatment in diabetes group was 4.23 and 16.7 months in nondiabetes group by Kaplan–Meier analysis, which was statistically significant (P = 0.0017, Kaplan–Meier analysis) (Fig. 8). The median time to the second Ozurdex treatment in BRVO and CRVO group was not significantly different.
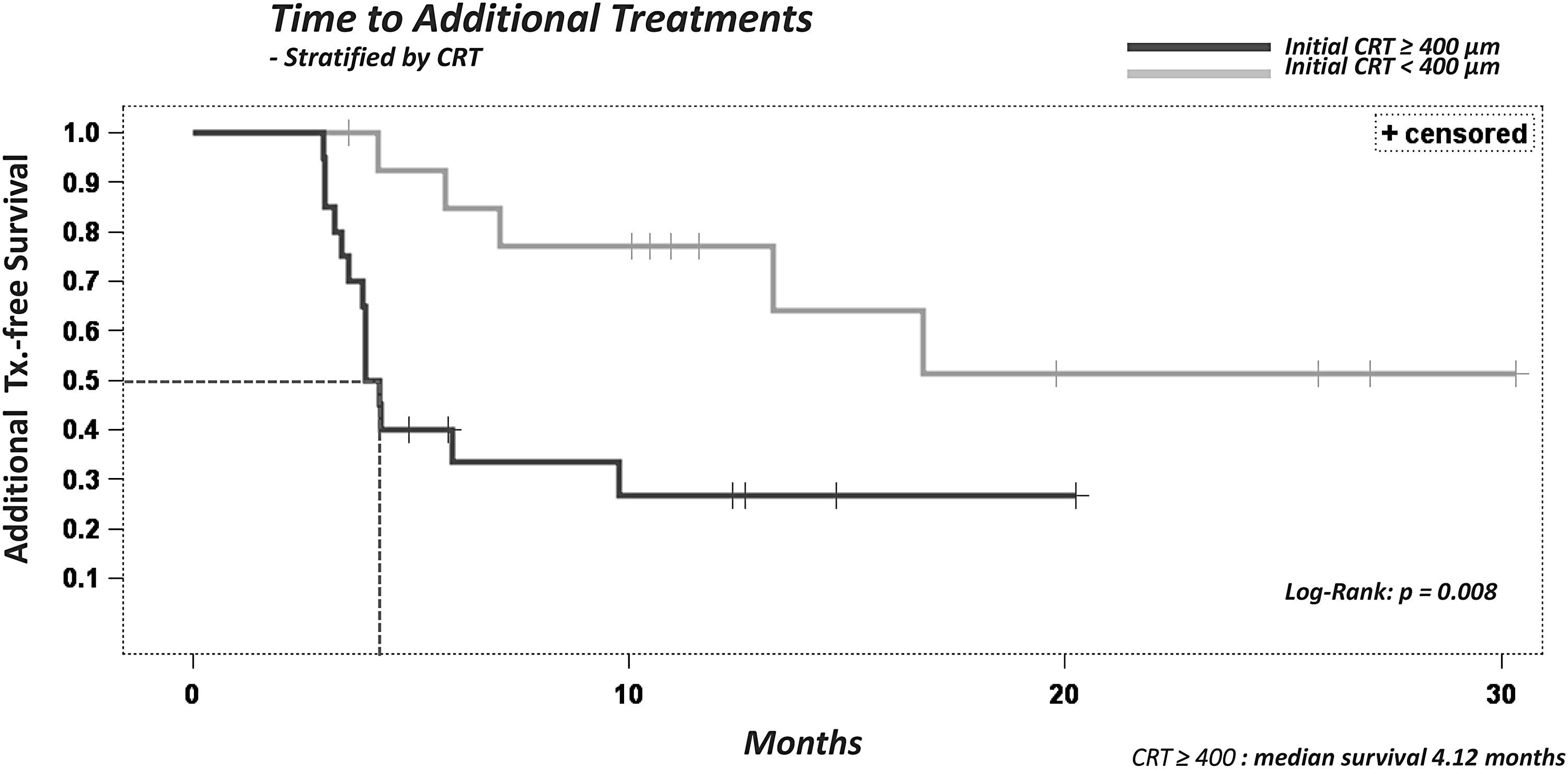
The median time to the second Ozurdex treatment in the initial CRT ≥400 μm group was 4.12 months. In the initial CRT <400 μm group, more than 50% only needed one injection during follow-up. The difference was statistically significant (P = 0.008, Kaplan–Meier analysis).
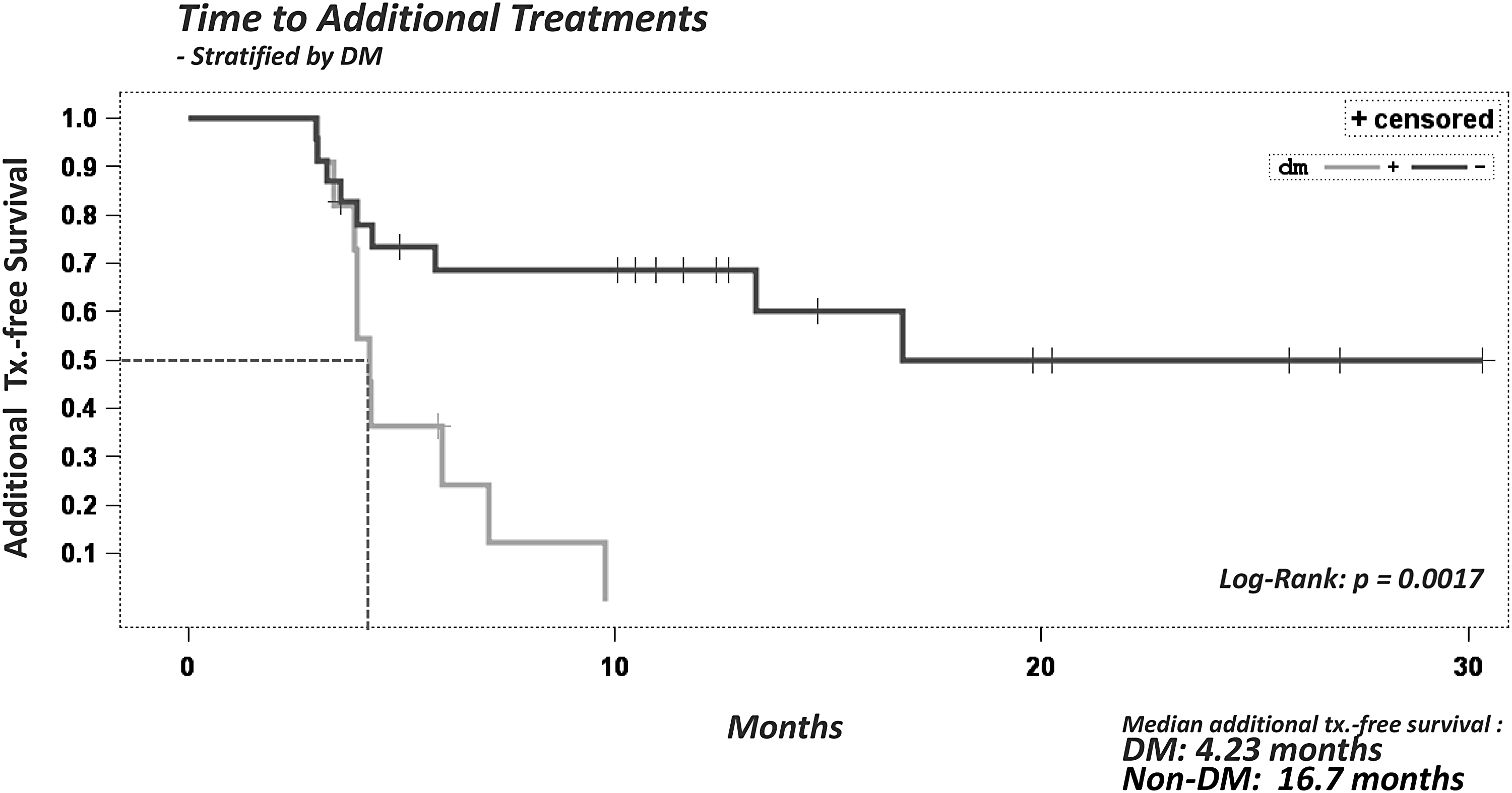
The median time to the second Ozurdex treatment in diabetes group was 4.23 and 16.7 months in nondiabetes group by Kaplan–Meier analysis which was statistically significant (P = 0.0017, Kaplan–Meier analysis).
In multivariate analysis, Cox proportional hazard model revealed that age older than 55 years and initial CRT ≥400 μm were significantly high risk factors for additional treatment, with a hazard ratio up to 8.853 (95% CI: 1.826–42.915) and 3.826 (95% CI: 1.175–12.460), respectively (Table 4). Multivariate logistic regression also verified that age older than 55 years and initial CRT ≥400 μm are the risk factors of multiple injections (Table 5).
Bold values signify P < 0.05.
Dependent variable: single injection versus multiple injections (event).
Bold values signify P < 0.05.
At any visit, 35.3% of the patients had a change in IOP ≥10 mmHg. Of these patients, 41.2% had a peak IOP ≥25 mmHg and 17.7% had a peak IOP ≥35 mmHg. The mean elevation of peak IOP was 9.53 ± 4.75 mmHg (from 15.41 ± 3.40 to 24.94 ± 8.15 mmHg). The mean elevation of final IOP was 0.24 ± 3.51 mmHg (from 15.41 ± 3.40 to 15.65 ± 3.30 mmHg). At the final visit, only one patient (2.9%) had a change in IOP ≥10 mmHg. Although 41.2% of the patients had an IOP ≥25 mmHg at any visit, the IOP eventually returned to the normal range.
Complications included 3 CRVO patients with a persistently elevated IOP (which was controlled with antiglaucomatous medication) and 4 CRVO patients with retinal neovascularization who were managed by panretinal photocoagulation. Some elderly patients had some degree of lens opacity at baseline. Vision-impairing cataract was not observed in the patients who only received one Ozurdex injection. Cataract progression was found in about 29% patients after the second Ozurdex injection. However, none underwent cataract extraction during the study period.
Discussion
RVO is a serious retinopathy that causes vessel obstruction in the retina, thus severely impairing vision. RVO is mainly classified as CRVO and BRVO, both of which can cause ME that then induce loss of vision. The Branch Vein Occlusion Study showed that macular photocoagulation is superior in improving vision compared with observation alone, and it has been the standard of care for patients with ME secondary to BRVO since 1984. 6 The Central Vein Occlusion Study demonstrated that grid photocoagulation of ME was of no visual benefit despite the resolution of ME in the treated eyes and recommended observation for ME secondary to CRVO. 7
Long-standing ME can result in progressive retinal changes and loss of photoreceptor function. It is therefore reasonable to assume that the timely reduction of ME can reduce the risk of losing retinal function. 20 Recently developed pharmacologic agents have changed the treatment protocol for ME secondary to RVO. Intravitreal anti-VEGF agents, including ranibizumab12–15 and aflibercept,16–18 have been approved for the treatment of ME in patients with BRVO and CRVO. It has also been suggested that the off-label use of intravitreal bevacizumab is effective in reducing ME and improving vision in eyes with RVO. 19
Several systemic factors have been identified as being associated with RVO, including diabetes, hypertension, and heart diseases. 4 Therefore, concerns have been raised that anti-VEGF agents may induce local and systemic adverse events. However, even though none of the trials with ranibizumab12–15 or aflibercept16–18 has shown increases in thromboembolic events in this population of patients, intravitreal steroid treatment may be preferable in patients comorbid with RVO and recent thromboembolic events.
Ozurdex is an intravitreal implant containing 700 μg of dexamethasone, and it has also been approved for the treatment of RVO. The GENEVA trial included 2 identical 6-month, randomized, prospective, multicenter, masked, sham-controlled, and parallel-group studies, using Ozurdex for the treatment of ME following BRVO or CRVO. 8 The results from 1,267 randomized patients were pooled and evenly divided into 3 groups. The second stage was an open-label extension, and all patients received 700 μg Ozurdex. The authors of the trial concluded that in patients with ME associated with BRVO or CRVO, Ozurdex produced significantly greater and more rapid improvements in vision than sham treatment. 9 In addition, patients treated with Ozurdex were also significantly less likely to experience worsening of BCVA than the sham-treated patients. Furthermore, Ozurdex was well tolerated and most patients had no significant increase in IOP 180 days posttreatment, and 21% of the patients with BRVO and 17% of those with CRVO only required a single dose over a 12-month period. 9 Although the study design was based on a therapeutic level of Ozurdex lasting for 6 months, BCVA actually peaked between 3 and 4 months.8,9
The SHASTA study was a retrospective chart review of patients receiving 2 or more Ozurdex injections for RVO. 11 Data were collected from the charts of 289 patients after the first Ozurdex injection and each subsequent visit through a minimum of 3 months up to 6 months after the last Ozurdex injection. Overall, the patients received a mean of 3.2 injections of Ozurdex as either monotherapy (29.1%) or combination therapy, with a mean interval between injections of 5.6 months. After the first 6 Ozurdex injections, 59.7% of the patients with BRVO and 66.7% of those with CRVO achieved a gain of 2 or more lines. The authors concluded that the clinical use of 2 or more injections of Ozurdex, either alone or in combination with adjunctive RVO treatment was safe and effective in the treatment of ME following RVO. Furthermore, decreases in ME and improvements in BCVA continued to be seen after each subsequent Ozurdex injection, and no new safety concerns developed after the use of multiple implants. 11
In the current study, CRT and BCVA improved significantly after one or more intravitreal Ozurdex injections. After the initial Ozurdex injection, 15 (44.12%) of the patients did not require adjunctive treatment during the study period. The relatively long treatment-free period (the median time to the second Ozurdex treatment was 9.76 months) in this study is consistent with previous findings, and suggests that this treatment is more beneficial than other short-duration therapies.
Published reports in which reinjections have been made after shorter intervals on an “as needed” basis are already available.22,23 To achieve satisfactory visual and anatomic outcomes after the intravitreal administration of Ozurdex, the reinjection interval has been proposed to be considerably less than 6 months in many instances. 24 Mayer et al. also provoked a criteria for a retreatment included an increase in CFT in OCT of >100 μm. 25 In this study, we wanted to set up a more aggressive criteria to achieve better outcome, so “as needed” basis with an increase in CFT in OCT of >50 μm from the lowest recorded level was chosen.
Further analysis revealed that the median time to the second Ozurdex treatment in those older than 55 years or initial CRT ≥400 μm was significantly shorter in those younger than 55 years or initial CRT <400 μm. The effectiveness of Ozurdex in ME secondary to BRVO decreases with aging has been reported recently. 26 Ages were also negatively correlated with the mean reduction of CRT for the whole study group. Altunel et al. supposed the solubility and release of dexamethasone in the vitreous might change with aging. 26
Age as a high risk factor for repeated treatment was an additional finding, when we analyzed our data. The negative effect of aging on the Ozurdex treatment in RVO may result from the involutional changes of retinal pigment epithelium and impaired function of retina cells. Besides, the thicker internal limiting membrane and vitreous degeneration due to aging might also affect the effectiveness of ozurdex.27,28 We analyzed the results that aging lowered the effectiveness of Ozurdex in treatment of ME in RVO. With the support from the finding of Altunel et al., we opine that age might be an important clinical determinant, which will influence the treatment of Ozurdex therapy. Nevertheless, more studies with prospective design are mandatory to pursue the underlying mechanism.
Although not supported in the multivariate analysis, we found that higher risk of receiving a second dose of Ozurdex in those with diabetes was significantly higher compared with those without diabetes in univariate Kaplan–Meier analysis. Several biochemical mechanisms in diabetic patients, including protein kinase C–β activation, increased VEGF production, oxidative stress, accumulation of intracellular sorbitol, and advanced glycosylation end products, may contribute to the overexpression of a range of cytokines, altered vascular permeability and damaged capillary endothelial cells that aggravate ME in RVO.29–31 In addition, hemodynamic pathways are activated in patients with diabetes, and these may be amplified by comorbid systemic hypertension. 29 Under hyperglycemic conditions, which are frequently seen in patients with diabetes, impairment of retinal blood flow, increased inflammatory cell adhesion to retinal blood vessels, capillary blockage, and hypercoagubility32–34 can result in more severe hypoxia and damage to the retina, which may then deplete Ozurdex more rapidly. Thus, the true influence of diabetes on the effect of Ozurdex should be further confirmed in future studies.
In the conditions of RVO, a rise in intravenous and capillary pressure leads to stagnation of blood, hypoxia of the affected structures, and damage to the capillary endothelial cells, with extravasation of plasma constituents. The pathophysiology of ME after RVO is a breakdown of the blood–retinal barrier, which normally prevents water movement in the retina, thus allowing fluid to accumulate in the retinal tissue. Inflammatory processes and an increase in vascular permeability are an integral part of the pathological process. Macular fluid accumulation alters cell function in the retina as well as provoking an inflammatory reparative response in a vicious cycle. 35
In patients with initial higher CRT, there might be more inflammatory activities to induce more severe ME. Therefore, higher initial CRT was a significant risk factor for additional Ozurdex treatment and the shorter median time to the second treatment.
The limitations of this study include its retrospective nature, a small sample size, and the lack of a concomitant control group. BRVO and CRVO have different pathogenesis. Also, nonischemic and ischemic CRVO have different pathogenesis, clinical features, prognosis, and management. They should be evaluated separately. Nevertheless, our results showed that the clinical use of 1–6 Ozurdex implants was safe and effective in the treatment of ME following RVO. Resolution of ME and improvements in BCVA were noted after each subsequent Ozurdex injection. Although BCVA remained relatively stable in the group with repeated injections for recurrent ME, more aggressive strategies should be attempted to maximize the beneficial effect on BCVA as seen in the group that received a single injection because of the detrimental disease process in the repeated-treatment group. The factors associated with challenging outcomes, including CRVO, age older than 55 years, initial CRT ≥400 μm, and diabetes, necessitate more frequent follow-up visits. Further research is required to establish the optimal retreatment schedule for Ozurdex, especially in these high-risk patients.
Disclaimer
The authors have no proprietary or commercial interest in any materials mentioned in this article.
Footnotes
Authors' Contributions
The authors were involved in the design and conduct of the study, data collection, analysis, management, and interpretation of data, and preparation, review, and approval of the article.
Author Disclosure Statement
No competing financial interests exist.