
Abstract
Abstract
Purpose:
To evaluate the clinical findings and the efficacy of dexamethasone intravitreal implant in patients with postvitrectomy macular edema.
Methods:
The records of 14 patients diagnosed with postvitrectomy macular edema unresponsive to first-line treatment, treated with intravitreal dexamethazone implant injection and followed at least 6 months between October 2011 and May 2016 were retrospectively reviewed. All patients underwent standard ophtalmological examination, fluorescein angiography, and optical coherence tomography. Best-corrected visual acuity (BCVA), central macular thickness (CMT), and intraocular pressures (IOPs) were recorded at baseline, at first and sixth months after the injection.
Results:
The mean BCVA, which was 0.2 ± 0.14 logMAR at baseline significantly increased to 0.44 ± 0.2 logMAR at first month (P = 0.05) and to 0.4 ± 0.22 logMAR at sixth month of intravitreal dexamethazone implant injection (P = 0.01). CMT was also significantly decreased to 368.3 ± 90.4 μm at first month and to 323 ± 84.6 μm at sixth month from pre-injection value of 520.7 ± 90.3 μm (P = 0.001 and P = 0.002, respectively). IOP significantly increased from was 15 ± 2.1 mmHg at baseline to 20.6 ± 5.4 mmHg at first month of intravitreal dexamethazone implant injection (P = 0.01).
Conclusion:
Dexamethazone implant treatment may reduce CMT and improve BCVA in cases with postvitrectomy macular edema. IOP should be regularly screened in these cases.
Introduction
P
Despite the advantages of modern VRS, postoperative macular edema is a commonly encountered complication in vitrectomy cases. Parolini and Sartore detected postoperative macular edema in 10.8% of patients treated with epiretinal membrane surgery. 3 Kim et al. calculated the postvitrectomy macular edema as 47%. 4
Inflammatory mediators such as proinflammatory cytokines and vascular endothelial growth factor (VEGF) are released due to surgical trauma. These mediators cause liquid accumulation and cystic cavity formation in the outer plexiform and inner nuclear layers as a result of damage to the blood-retina barrier and increased vascular permeability. 5 Furthermore, light toxicity, vitreomacular traction, age, iris color, and the surgical technique are also thought to affect the development of macular edema.6–8
Oral acetazolamide and topical nonsteroidal anti-inflammatory drugs (NSAIDs) are used as first-line treatment for postoperative macular edema. As second-line treatment, intravitreal injection of steroids such as triamcinolone 9 and dexamethasone implants, 10 and injection of intravitreal VEGF inhibitors11,12 and subcutaneous interferone alpha-2 are considered. 13
Intravitreal dexamethasone implants (Ozurdex®; Allegran, Inc., Irvine, California) are bio-soluble intravitreal implants that release 0.7 mg dexamethasone over a period of 6 months into the vitreous and retina. 14
In this study, we aimed to evaluate the anatomical and functional outcomes of intravitreal dexamethasone implant for treatment of VRS-related macular edema.
Methods
Study design and population
The medical files of 14 patients (4 women, 10 men; mean age 62.8 ± 8.8 years; age range 39–74 years) who were diagnosed with postvitrectomy macular edema unresponsive to the first-line treatment with NSAIDs for 2 months, and received intravitreal dexamethasone implant injection between October 2011 and May 2016 were reviewed retrospectively. Other inclusion criteria were an increase in retinal thickness of more than 310 μm in parafoveal 3 mm diameter area on optical coherence tomography (OCT), leakage in macula and optic disc in fluorescein angiography (FA), and the follow-up duration of at least 6 months after intravitreal injection. Cases in which retinal pathology had been detected after VRS, those who had undergone cataract surgery and panretinal laser photo-coagulation combined with VRS, had macular edema due to other reasons, or had uncontrolled systemic diseases were excluded from the study.
The study was conducted according to the Helsinki Declaration and approved by the Institutional Ethics Commitee (no. 15, date 18.10.2016), and informed consent requirement was waived due to retrospective design of the study.
Study procedures
The data on the medical history and demographics were recorded for all patients. All cases were operated by the same surgeon with the 23-Gauge vitrectomy system. No epinephrine was added to the infusion fluid in any of the cases.
Before intravitreal dexamethasone implant injection, all patients underwent standard ophtalmological examination, FA, and OCT. OCT evaluations were performed by the same physician using the spectral domain OCT (Spectralis OCT, Heidelberg Engineering, Heidelberg, Germany).
Best-corrected visual acuity (BCVA), central macular thickness (CMT), and intraocular pressures (IOPs) were recorded at baseline, at first and sixth months after the injection.
Statistical analysis
Study data were summarized using descriptive statistics (e.g., mean, standard deviation, range, frequency, and percentage). For analysis of repeated measurements, Friedman test was used. The paired data were compared by the Wilcoxon signed rank test. The limit for statistical significance was set as P < 0.05. All statistical analyses were performed with SPSS for Windows (Statistical Package for Social Sciences, ver. 15.0; SPSS, Inc., Chicago, Illinois) software.
Results
Baseline clinical and ophthalmological findings
Four of the cases had diabetes mellitus and hypertension, and 2 had hypertension. Ten of the cases (71.4%) underwent VRS due to regmatogen retinal detachment, 1 (7.1%) for epiretinal membrane, 1 for intraocular foreign body (7.1%), and 2 for complicated cataract surgery (14.2%) (Table 1). Eleven of the cases (78.5%) had pseudophakia and 3 had (21.5%) phakia. During follow-up, cataract was not observed in cases with phakia
OCT, optical coherence tomography.
On OCT images, diffuse retinal thickening was observed in 6 cases (42.8%), cysts besides retinal thickening in 8 cases (57.1%) (Fig. 1), and serous fovea detachment in 2 cases (Fig. 2). Leakage around the optic disc and macula was present on FA in all cases (Fig. 3).

OCT images before
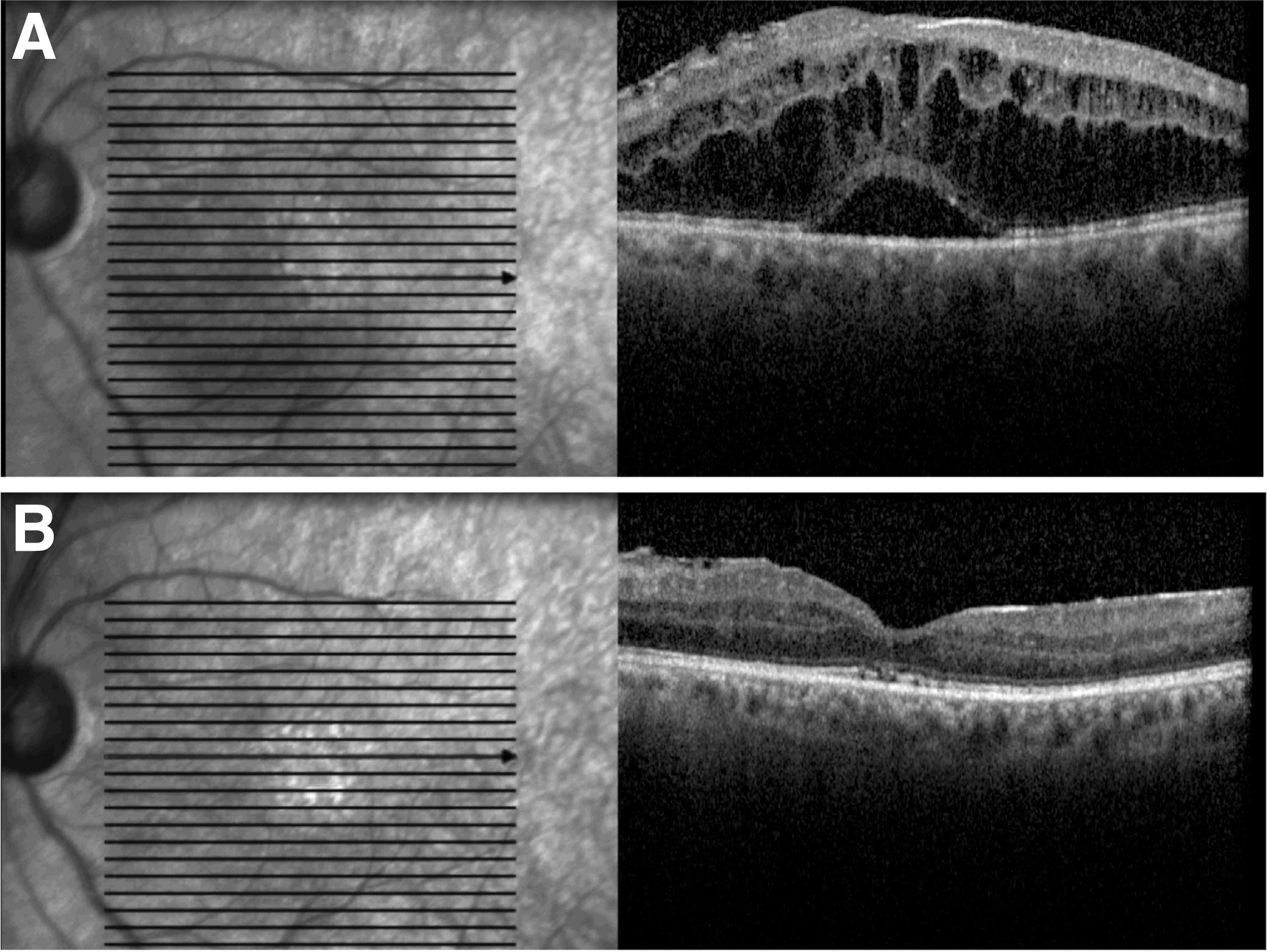
OCT images before
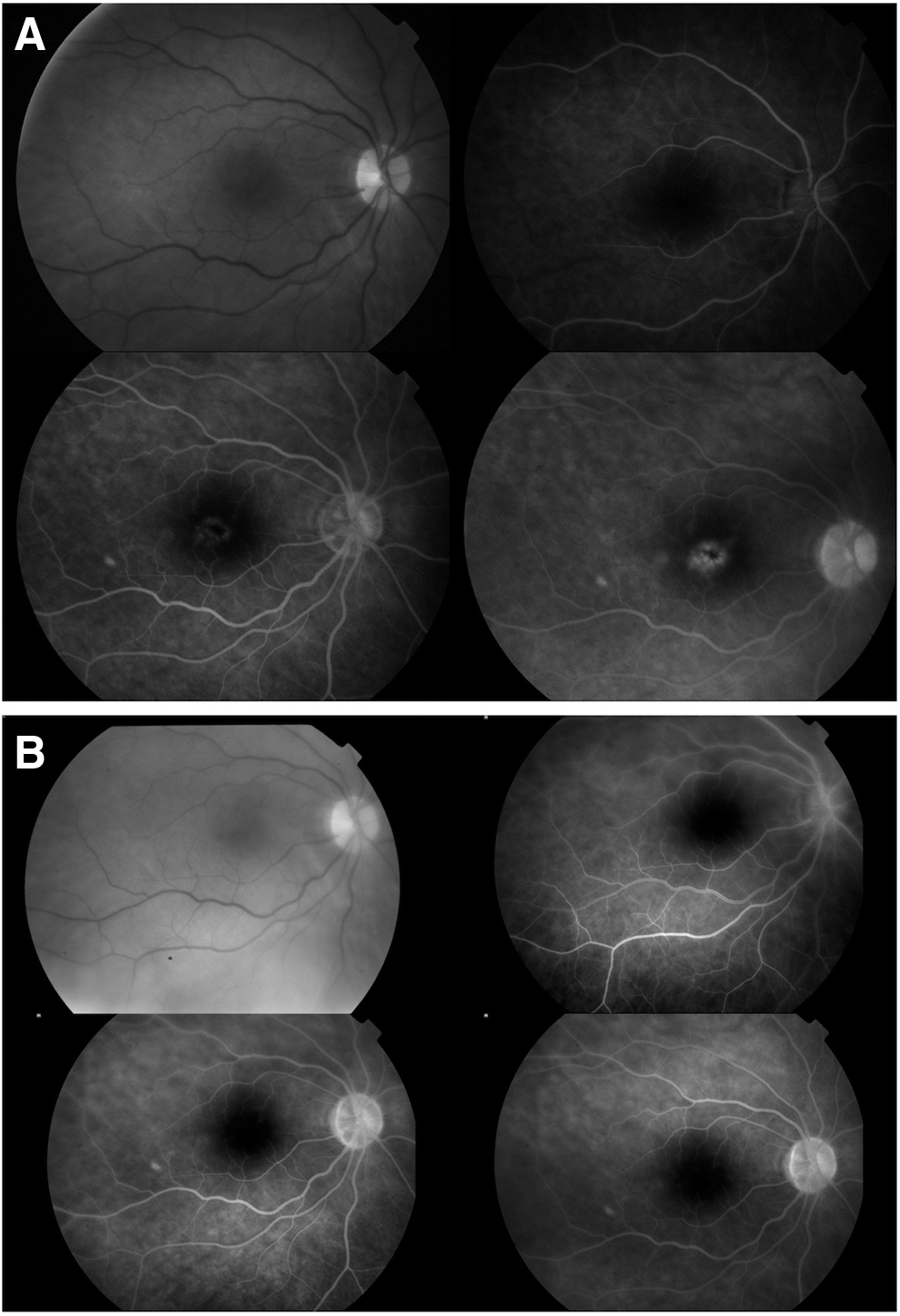
Fluorescein angiography images before
Efficacy of intravitreal dexamethasone implant injection
The mean duration of follow-up after intravitreal dexamethasone implant injection was 12.5 ± 5.3 months (range, 8–24 months), and the mean time interval between VRS and intravitreal injection was 16.5 ± 15.8 months (range, 3–55 months). No macular edema was observed in 9 cases at the end of 6 months. In 3 cases with recurrent edema, intravitreal dexamethasone implant injection was reperformed. For the other 2 cases, treatment continued with intravitreal ranibizumab due to an increase in IOP after dexamethasone implant injection. Two doses of intravitreal ranibizumab was injected in both cases. For all cases, the second intravitreal injection (intravitreal dexamethasone or ranibizumab injection) was administered at least 6 months after the first intravitreal dexamethasone implant injection. In one of the cases that had responded to treatment, but had developed an increase in intraretinal fluid, relapse was observed in the third month, while in 4 cases, relapse occurred in the fourth month.
The anatomical improvement was recorded in both OCT and FA images after intravitreal dexamethasone implant injection (Figs. 1–3).
The mean BCVA scores were determined as 0.2 ± 0.14 before the intravitreal injection, 0.44 ± 0.2 in 1 month after injection, and 0.4 ± 0.22 in 6 months after injection. The mean BCVA scores at 1 and 6 months were significantly higher compared with the preinjection score (P = 0.05 and P = 0.01, respectively) (Table 2). However, there were no statistical differences between BCVA scores at 1 and 6 months (P = 0.07).
Data are given as mean ± standard deviation (min–max).
Friedman test was used for analysis of repeated measurements.
Pairwise comparisons with Wilcoxon signed rank test: P = 0.05 for preinjection versus first month, P = 0.01 for preinjection versus sixth month, P = 0.07 for first month versus sixth month.
Pairwise comparisons with Wilcoxon signed rank test: P = 0.001 for preinjection versus first month, P = 0.002 for preinjection versus sixth month, P = 0.15 for first month versus sixth month.
Pairwise comparisons with Wilcoxon signed rank test: P = 0.01 for preinjection versus first month, P = 0.27 for preinjection versus sixth month, P = 0.02 for first month versus sixth month.
BCVA, best-corrected visual acuity; IOP, intraocular pressures.
The mean CMT in the perifoveal 3 mm-diameter area, which was 520.7 ± 90.3 μm before the intravitreal injection decreased significantly to 368.3 ± 90.4 μm in 1 month after the injection, and 323 ± 84.6 μm in 6 months after the injection (P = 0.001 and P = 0.002, respectively) (Table 2).
The mean IOP significantly increased from 15 ± 2.1 mmHg to 20.6 ± 5.4 mmHg 1 month after intravitreal dexamethasone implant injection (P = 0.01) (Table 2). After intravitreal dexamethasone implantation, the IOP was determined to be higher than 25 mmHg in 7 cases (%50) and topical antiglaucomatous treatment was administered. IOP was measured to be high for the first time in 6 of these cases (42.8%) in the first month, and in one of the cases (7.1%) in the fourth month. In one of these cases brinzolamide, in 4 cases dorzolamide and timolol combination, and in 2 cases dorzolamide, timolol, and brinzolamide combination were administered as topical antiglaucomatous treatment. The IOP levels dropped below 20 mmHg with the treatment in all cases. At the sixth month of follow-up, the mean IOP levels were 14.9 ± 1.8 mmHg. Three cases currently continue with the antiglaucoma treatment. None of the cases required filtration surgery.
Discussion
In the present cohort of 14 patients, we showed that intravitreal dexamethazone implant provides anatomical and functional improvement in cases with postvitretomy macula edema resistant to first-line treatment.
Surgical trauma and prostaglandins and leukotrienes released as a result of arachidonic acid metabolism play a role in the pathophysiology of postoperative macular edema. Steroids and NSAIDs prevent the synthesis of prostaglandins by inhibiting the 2 arms of this pathway. NSAIDs act by inhibiting cyclooxygenase 1 and 2; corticosteroids act by inhibiting phospholipase A2. 15
Fluid accumulation in the extracellular space and formation of a cystic cavity in the outer plexiform and inner nuclear layers due to impairments of the blood-retina barrier are the main mechanisms. Pathological macular edema can be classified as clinical and angiographic. Angiographic macular edema is characterized by the presence of leakage in the perifoveal capillaries and accumulation of fluorescein around the fovea in platoid pattern on FA without any decrease in BCVA.16,17 Besides these findings, in clinical macular edema, BCVA is 20/40 or lower. The incidence of angiographic cystoid macular edema is higher than clinical macular edema. 17 In our study, clinical macular edema was present in all cases.
Mc Donald et al. detected FA leakage following vitrectomy in 70% of epiretinal membrane cases and 80% of macular hole cases. 18 Frisina et al. determined the incidence of macular edema as 12.8% in vitrectomy patients who had undergone epiretinal membrane peeling, and they stated that postoperative macular edema was an important posterior segment problem seen after VRS. 19
In cases without vascular leakage, the mechanism of cyst formation is thought to be iatrogenic Müller cell damage that occurs during internal limiting membrane and epiretinal membrane peeling. Cystic formations develop due to retinal structural injury without damage to the blood-retina barrier in these cases. 19 Similar to Irvine-Gass syndrome, in cases with damage to the blood-retina barrier due to inflammation, vascular leakage, and fluorescein leak are observed on FA. In our study, internal limiting membrane-epiretinal membrane peeling was performed in 6 cases, and optic disc and macular leakage were seen in all. Therefore, the persistent macular edema seen in our cases was thought to be caused by inflammation.
Kim et al. stated that macular edema seen after vitrectomy was a commonly seen complication affecting visual rehabilitation and emphasized the importance of primary retinal pathologies in edema formation. Increase in retinal thickness is seen to be higher in VRS for epiretinal membrane and intravitreal hemorrhage compared to macular hole operations. Researchers have found that inflammation plays an important role in the development of persistent macular edema and addition of epinephrine to the infusion solution leads to macular edema by increasing the prostaglandin levels. 4 In our study, no epinephrine was added to the infusion solution during VRS; therefore, this mechanism is considered inapplicable in our cases.
Dexamethasone is a potent corticosteroid that acts by long-term suppression of various inflammatory cytokines. Georgalas et al. observed a decrease in central retinal thickness and an increase in visual acuity by dexamethasone implant in a vitrectomy case with macular edema resistant to topical sub-tenon and intravitreous steroid administrations. 10 Karaçorlu et al. administered intravitreal triamcinolone treatment to 6 cases (42.8%) for postoperative macular edema and established that this treatment was effective and safe for pseudo phakic macular edema. 9 Bellocq et al. detected anatomical and functional improvement in 48.7% of the cases in their study involving 50 patients who had undergone intravitreal dexamethasone implant with the diagnosis of postoperative macular edema. Researchers observed anatomical and functional recovery at 3 months postinjection. However, they found that the sixth month BCVA was statistically significantly higher than the pretreatment BCVA. The highest mean IOP levels in the study were measured at the first month after treatment. 14 Similarly, in our study, there was a statistically significant difference in retinal thickness measurements and BCVA scores after dexamethasone implant injection in the first and sixth months compared to pretreatment, and the highest mean IOP was determined at the first month. IOP regulation with topical treatment was observed in all cases. None of the cases required filtration surgery. In 9 cases (64%), remission was seen with single dose implantation, while in 5 cases, a second injection was necessary.
Koutsandrea et al. reported that 3 cases out of 14 single-dose intravitreal triamcinolone injection cases required antiglaucoma treatment in the first 3 months and only 1 case received antiglaucoma treatment at the end of the 12th month during the 12-month follow-up. 20 In our study, topical antiglaucoma treatment was administered to only 3 of the cases at the end of the 6-month follow-up.
The 2 most important side effects of corticosteroid treatment are cataract development and IOP increase. 21 Only 3 of our cases were phakic. In these cases, cataract development was not observed on the follow-ups.
The limitations of the study include the low number of cases, the absence of a control group and short follow-up duration. Nevertheless, this is the first study on the efficacy and safety of clinical practice of intravitreal injection of dexamethasone implant in cases postvitrectomy macular edema resistant to first-line treatment in a tertiary single center. Further controlled studies with a large number of cases would demonstrate the effect of dexamethasone implant in postvitrectomy macular edema treatment more precisely and reliably.
In conclusion, intravitreal injection of dexamethasone implant provides anatomical and functional improvement in the treatment of postvitrectomy macular edema resistant to first-line treatment. IOP follow-up is important after intravitreal injection of dexamethasone implant.
Authors' Contributions
Each of the authors has participated in the study and takes public responsibility for the content and the integrity of the work.
Footnotes
Author Disclosure Statement
No competing financial interests exist