
Abstract
Abstract
Purpose:
We aimed to evaluate the effect of the topical application of a strong corticosteroid, difluprednate, on the levels of inflammatory and angiogenic cytokine in the vitreous and aqueous humor after laser photocoagulation.
Methods:
Pigmented rabbits were treated with retinal laser photocoagulation and divided into 4 groups, namely control (no additional treatment), topical application of difluprednate 0.05%, betamethasone sodium phosphate 0.1%, and sub-Tenon injection of triamcinolone acetonide (STTA). Samples of vitreous and aqueous humor were collected on posttreatment days 0, 1, 7, and 14. The levels of intraocular vascular endothelial growth factor (VEGF), interleukin-6 (IL-6), intercellular adhesion molecule-1 (ICAM-1), and monocyte chemotactic protein-1 (MCP-1) were measured using an immunoassay. Intraocular pressure (IOP) was monitored in each group.
Results:
VEGF, IL-6, ICAM-1, and MCP-1 were significantly elevated on day 1 and were reduced in both the vitreous and aqueous humor following topical application of difluprednate and STTA. Topical betamethasone reduced their levels in the aqueous humor but not in the vitreous. A significant increase of IOP induced by difluprednate returned to control levels after withdrawal of administration.
Conclusion:
Although the elevation of IOP was an expected, manageable side effect, topical application of difluprednate was more effective than STTA and betamethasone for reducing inflammatory cytokine levels after laser treatment.
Introduction
L
In the retina, choroid, and vitreous humor after laser treatment, increased proinflammatory cytokine levels indicate the involvement of inflammation in the pathogenesis or getting worse of DME treated by PRP.2,3 Shimura et al. reported that increased proinflammatory cytokine levels in the vitreous humor and transient worsening of macular edema in PRP-treated eyes of high-risk PDR patients compared with those in nontreated eyes. 4
The therapeutic effect of triamcinolone acetonide (TA), a long-acting corticosteroid, depends on its strong anti-inflammatory activity that reduces permeability of the capillary, fibrin deposition, endothelial tight junction loss, and intraocular cytokine levels. 5 Intravitreal injection (IVTA) or sub-Tenon capsule administration (STTA) of TA can prevent macular swelling and visual dysfunction induced by PRP;6–11 however, these are related to the complications of the eyes such as a rise in intraocular pressure (IOP) endophthalmitis, the progression of cataract, and the conjunctival scar.
Difluprednate is an ophthalmic steroid with high glucocorticoid receptor-binding affinity and superior tissue penetration. Previous studies have shown that difluprednate is effective for reducing inflammation after cataract surgery and uveitis.12–14 It was approved in 2008 by the U.S. Food and Drug Administration (FDA) and is used for the treatment of inflammation of postoperative eyes and the pain. 13 In Japan, difluprednate ophthalmic solution 0.05% (difluroprednisolone butyrate acetate; STEROP®; Senju Pharmaceutical Co., Ltd., Osaka, Japan) is used for the treatment of uveitis in dogs. Nakano et al. reported that instillation of difluprednate was effective in reducing refractory DME. 15 Case report of 2 patients with PDR showed that the use of difluprednate was effective to reduce the macular thickness after PRP. 16 Thus, the topical difluprednate may be one of the possible choices to treat the progression of macular edema after PRP. To investigate the underlying mechanisms, the present study compared the effect of difluprednate ophthalmic emulsion with STTA and betamethasone sodium phosphate 0.1% (Rinderon® Ophthalmic Solution Shionogi Pharmaceutical Co., Ltd., Osaka, Japan) on inflammatory cytokine levels in the vitreous humor of rabbit eyes after laser photocoagulation.
Methods
Animals
We prepared for the pigmented male Rex rabbits weighing 2.0 to 2.5 kg (Japan SLC Co., Ltd., Shizuoka, Japan) and let new environment acclimatize it for at least 1 week. They were able to obtain water and food freely (RC4; Oriental Yeast Co., Ltd., Tokyo, Japan). Animals care and experimentation followed the guidelines of the Association for Research in Vision and Ophthalmology Statement for the Use of Animals in Ophthalmic and Vision Research. Before photocoagulation and a medication, we anesthetized rabbits by an intramuscular injection of hydrochloric acid ketamine (3.5 mg/kg) and hydrochloric acid xylazine (5 mg/kg).
We performed laser photocoagulation with a PASCAL® Streamline photocoagulator (Topcon Medical Laser systems, Santa Clara, CA), a 577 nm yellow wavelength, and Super Quad 160 contact lens. The laser settings were 200 mW, a spot size of 200 μm, exposure duration of 200 ms, and a spot number of 500.5,17 After the photocoagulation of both eyes, we assigned 36 rabbits to 4 crowds of 9 at random. These were controls (PRP only), a difluprednate group, a betamethasone group, and an STTA group. Three rabbits in each group were sacrificed on days 1, 7, and 14. Another group of 3 rabbits with no photocoagulation treatment were included with the evaluations conducted on day 0.
STTA and topical steroid treatment
STTA was performed following photocoagulation. The eyes were prepared with 5% povidone iodine and 0.4% oxybuprocaine hydrochloride topical anesthesia (benoxyl ophthalmic solution; Santen Co., Ltd., Osaka, Japan). We used an eyelid retractor to stabilize eyelids. We dissolved TA (MaQaid Wakamoto Pharmaceutical Co., Ltd., Tokyo, Japan) in a saline (40 mg/mL) and injected TA weighing 20 mg of 0.5 mL from the capsule space under sub-Tenon and let it arrive at the posterior pole using the needle of 20 gauges (Hurricane Medical Bradenton, FL).
Difluprednate 0.5% or betamethasone sodium phosphate 0.1% drops were administered topically immediately after laser treatment at 20:00 h on day 0. On day 1 and thereafter, eye drops were administered 4 times daily, at 9:00, 13:00, and 17:00 h for 14 days, and then stopped in the morning of day 15. IOP was measured using an Icare TONOVET tonometer (M.E. Technica Co., Ltd, Japan) on days 1, 7, 14, 21, and 28. The average of 6 successive measurements was recorded.
Assay of cytokines in the vitreous and aqueous humor
Vascular endothelial growth factor (VEGF), interleukin-6 (IL-6), intercellular adhesion molecule-1 (ICAM-1), and monocyte chemotactic protein-1 (MCP-1) levels in the vitreous and aqueous humor were assayed on days 1, 7, and 14 in both eyes of 3 rabbits in each study group. We anesthetized rabbits by intravenous injection of 10 mL pentobarbital sodium euthanized. We collected 500 μL aqueous humor from anterior chamber of each eye with a 30 gauge needle and 1.0 mL syringe. We enucleated the eyes and stored at −20°C for 2 days. The vitreous humor was removed while frozen and was centrifuged at 3,000 g for 10 min after thawing. The supernatant was vortexed and centrifuged again before collecting the supernatant.
The cytokine levels were measured by a sandwich enzyme-linked immunosorbent assay using a commercially available kit (VEGF and IL-6; Cusabio Biotech Co., Ltd., Hubei, China, ICAM-1; Cloud-Clone Corp., TX, MCP-1; NEO Group, Inc., MA) following the manufacturers' instructions. The assays used microtiter plates precoated with monoclonal primary antibodies and polyclonal secondary antibodies. The optical density of each sample was compared to a standard curve of recombinant protein. The assays were performed as previously described by Arimura et al. 5
Statistical analyses
We performed a statistical analysis using JMP® (SAS institute, Inc., Tokyo, Japan). Data are shown as means ± standard deviation. Bartlett's test was used to determine whether the variance was equal across samples. After confirming a normal distribution, the statistical significances between the groups were assessed by Mann–Whitney test. Statistical analyses were performed with the Wilcoxon signed-rank test (pretreatment and posttreatment data in the same group). P values <0.05 were considered significant.
Results
Cytokine profiles in the vitreous humor
VEGF, IL-6, ICAM-1, and MCP-1 levels were assayed before PRP (baseline) and on days 1, 7, and 14 (Fig. 1). In the only PRP group (control group), all cytokine levels increased from basic line but decreased thereafter. Levels of VEGF were significantly lower on day 1 (P = 0.038) in the difluprednate group and on days 1 (P < 0.001) and 7 (P = 0.029) in the STTA group. Levels of IL-6 were significantly lower in the difluprednate group than in controls on days 1 (P = 0.018), 7 (P < 0.001), and 14 (P = 0.023), and were lower in the STTA group than in controls on days 1 (P < 0.001) and 7 (P = 0.001). Levels of MCP-1 were lower than in controls on day 1 (P = 0.023) in the STTA group and on days 1 (P = 0.001) and 7 (P = 0.038) in the difluprednate group. Levels of ICAM-1 in the control group were higher on day 7 than at baseline and levels in the difluprednate and STTA groups were significantly lower than in controls on days 1 (P = 0.029, and P = 0.031, respectively) and 7 (P = 0.024 and P = 0.033, respectively). No significant differences in cytokine levels were observed in the betamethasone group compared with controls.
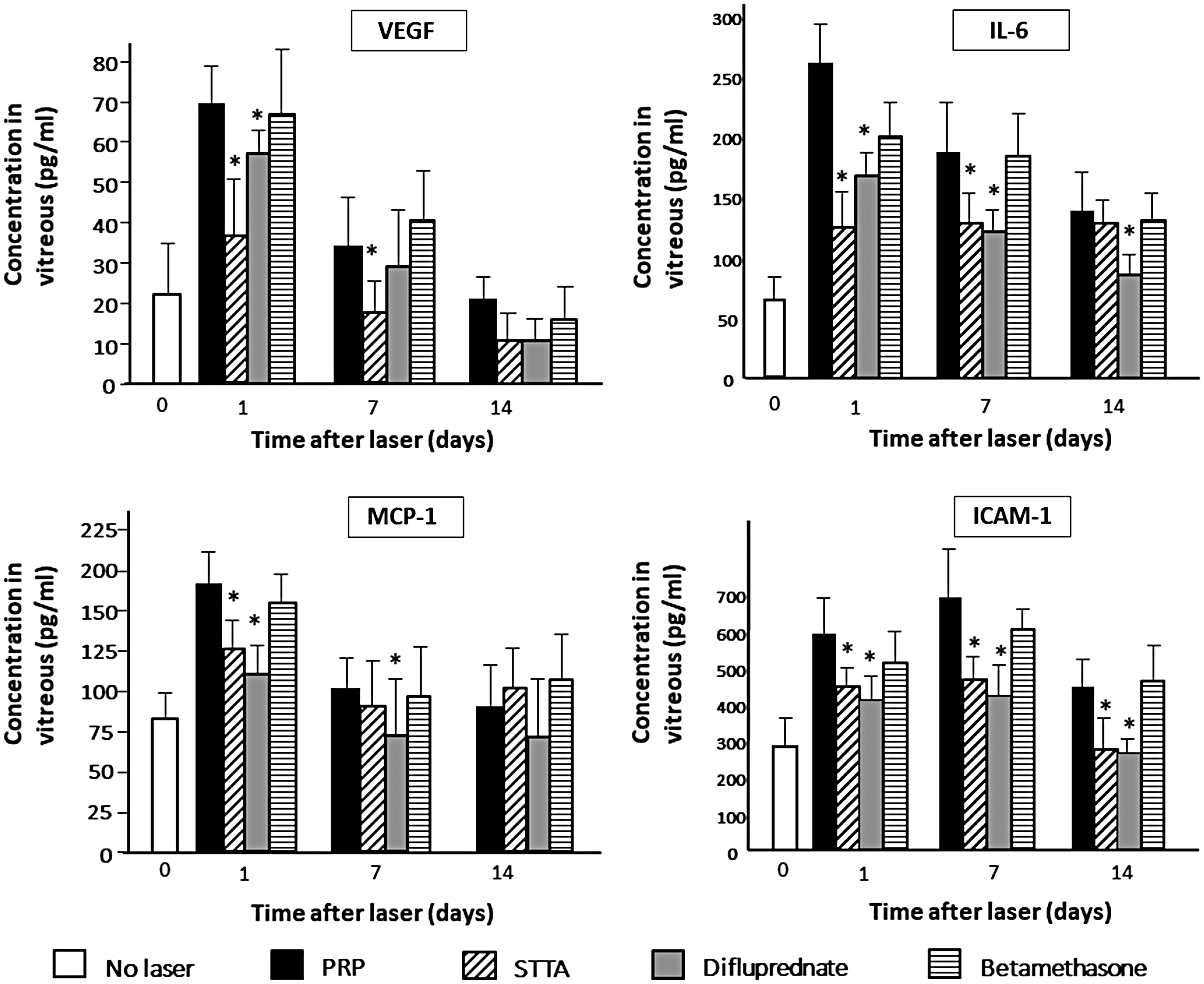
Inflammatory and angiogenic cytokine levels in the vitreous humor following the administration of difluprednate 0.05%, betamethasone sodium phosphate 0.1%, or STTA after PRP. *P < 0.05 vs. controls. Error bars show standard deviation (n = 8). VEGF, vascular endothelial growth factor; IL-6, interleukin-6; MCP-1, monocyte chemotactic protein-1; ICAM-1, intercellular adhesion molecule-1; PRP, panretinal photocoagulation; STTA, sub-Tenon injection of triamcinolone acetonide.
Cytokine profiles in the aqueous humor
VEGF, IL-6, ICAM-1, and MCP-1 levels were assayed before PRP (baseline) and on days 1, 7, and 14 (Fig. 2). Levels of VEGF transiently increased on day 1 and decreased to baseline levels on day 7. The increase of VEGF levels on day 1 was significantly suppressed by difluprednate (P < 0.001), betamethasone (P = 0.021), and STTA (P < 0.001). Significant decreases in VEGF level was observed in the difluprednate group on days 7 and 14. The transient increase of the IL-6 level was significantly obstructed by STTA on days 1 (P = 0.001) and 7 (P = 0.035), difluprednate on days 1 (P = 0.001), 7 (P = 0.001), and 14 (P = 0.034), and betamethasone on days 1 (P = 0.022) and 7 (P = 0.028). No effects of betamethasone and STTA were seen on day 14. The transient increase in MCP-1 levels was significantly inhibited by STTA on day 1 (P = 0.029) or difluprednate on days 1 (P = 0.036) and 7 (P = 0.042), but not betamethasone. The rise in ICAM-1 level was significantly obstructed by STTA on day 1 (P = 0.021), difluprednate on days 1 (P = 0.037) and 14 (P = 0.020), or betamethasone on day 1 (P = 0.041).
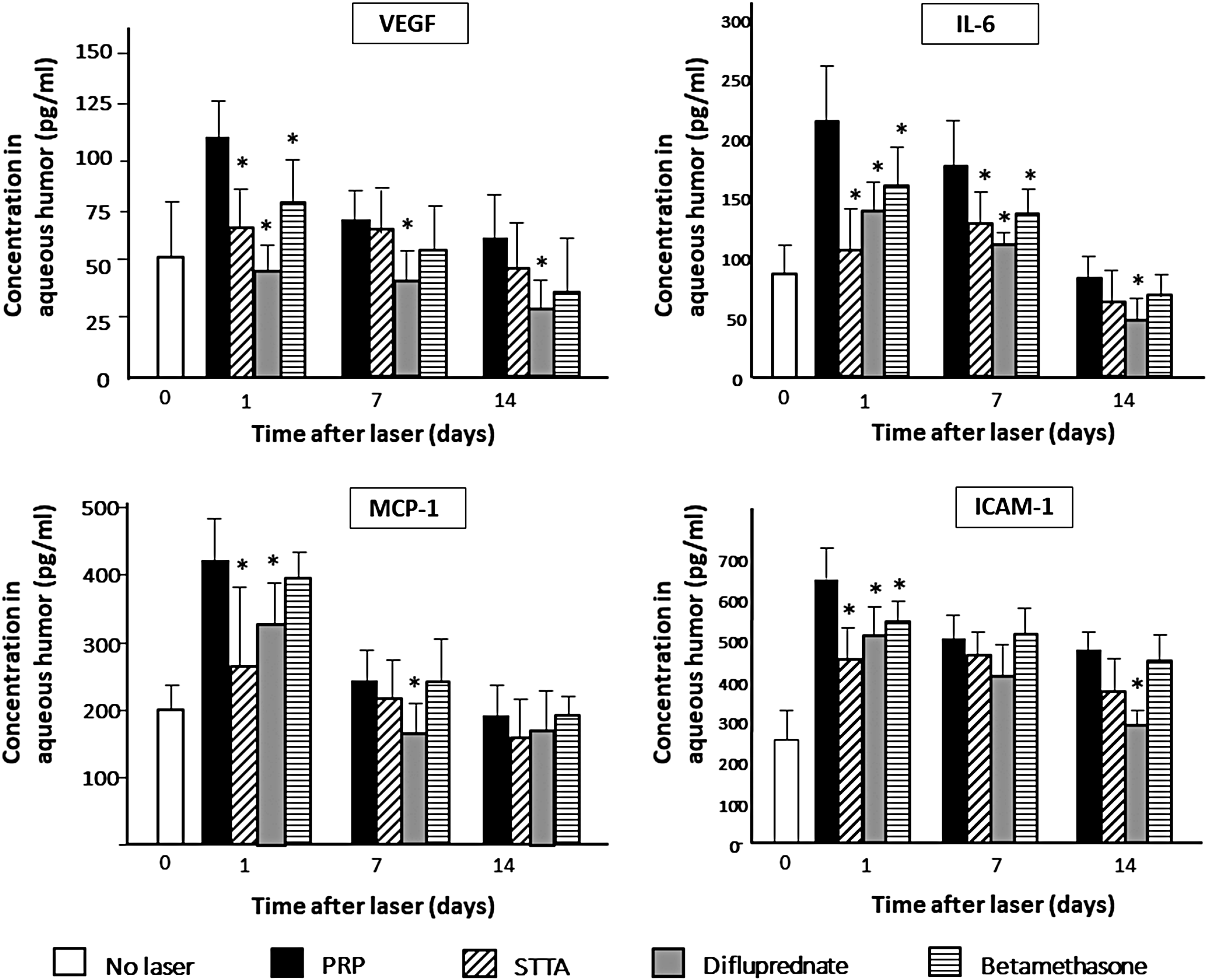
Inflammatory and angiogenic cytokine levels in the aqueous humor following administration of difluprednate 0.05%, betamethasone sodium phosphate 0.1%, or STTA after PRP. *P < 0.05 vs. controls. Error bars show standard deviation (n = 8).
Intraocular pressure
IOP was monitored (Fig. 3) because it is known to increase after treatment with ophthalmic steroids. IOP was significantly increased on days 7 (P = 0.001) and 14 (P = 0.0098) in the eyes treated with difluprednate compared with controls with PRP only. No significant IOP increase was observed in eyes treated with betamethasone. Daily administration of difluprednate and betamethasone drops was stopped on day 14, and IOP had returned to control levels on days 21 (P = 0.0059) and 28 (P = 0.041). A significant increase of IOP was observed on day 21 compared with controls. We found no significant correlation between the value of IOP and the cytokine levels in the aqueous humor or vitreous at each time point (simple regression analysis, P > 0.05).
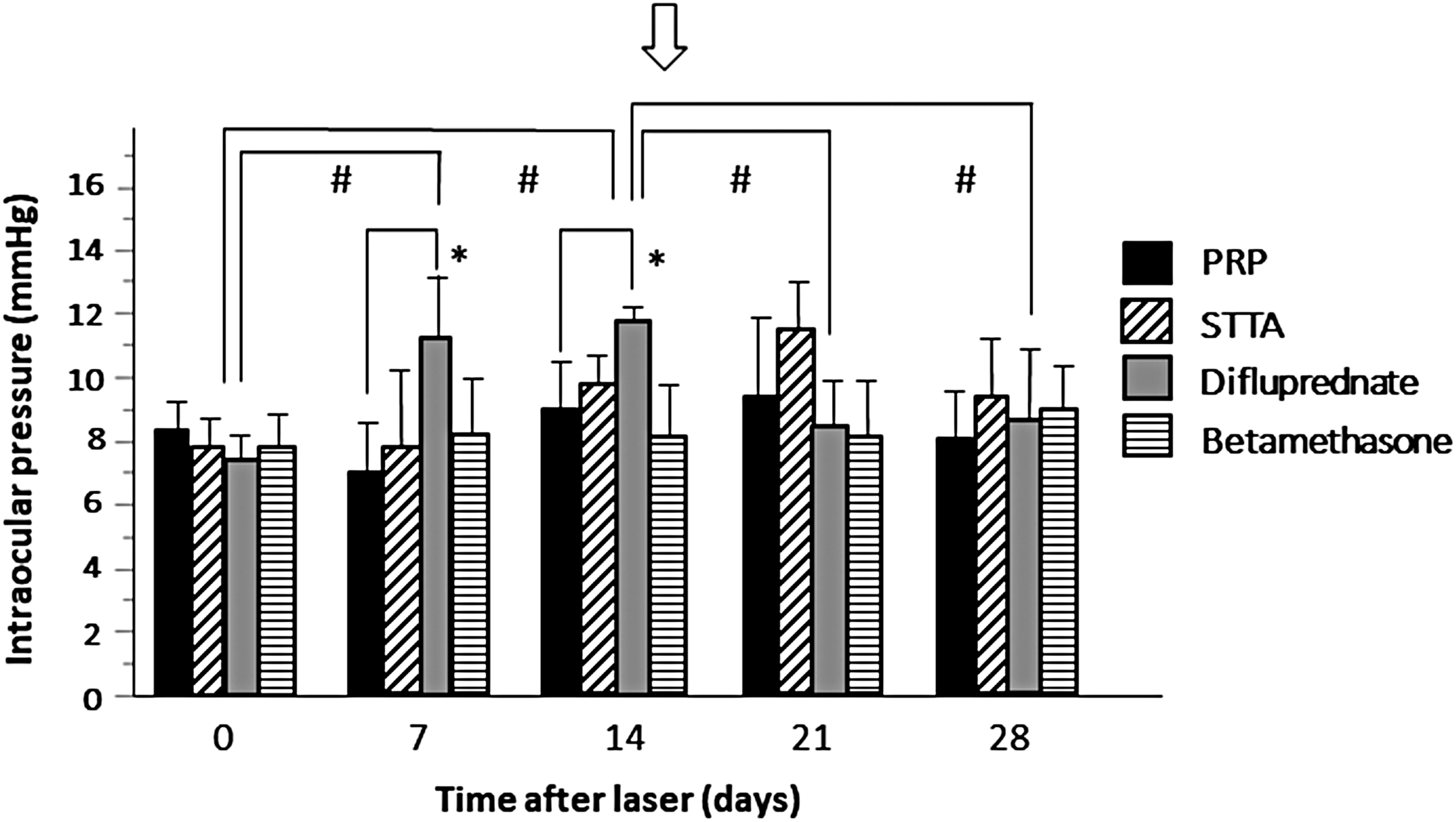
Intraocular pressure after the administration of difluprednate 0.05%, betamethasone sodium phosphate 0.1%, or STTA on days 0, 1, 7, 14, 21, and 28 after PRP. White arrow indicates the timing to stop the eye drops of difluprednate or betamethasone. *P < 0.05 vs. controls. #P < 0.05 vs. each time point, error bars show standard deviation (n = 8).
Discussion
We recently demonstrated that STTA and IVTA were effective in reducing the proinflammatory cytokine levels in the vitreous and aqueous humor of the eyes of pigmented rabbits after photocoagulation. 5 IVTA is a standard treatment and more widely used than STTA; however, STTA may be safer because of a lower incidence of endophthalmitis, progression of cataracts, and elevation of IOP.8,18 Although STTA may be useful to reduce inflammation associated with PRP, the procedure is not as simple as IVTA. Frequent conjunctival incision is associated with infectious complications risk of severe conjunctival scarring. Also, drug reflux of TA, which may occur from the conjunctival incision site, increases the risk of insufficient reduction of DME and the elevation of IOP. 19 These disadvantages can be avoided using steroid eye drops. In this study, cytokine levels in both vitreous and aqueous humor were significantly reduced on days 1 and 7 after laser photocoagulation in rabbits treated with difluprednate group and STTA. Difluprednate was effective as a noninvasive anti-inflammatory treatment.
The conventional betamethasone and prednisolone steroid eye drops helps to relieve inflammation, redness, and irritation. Difluprednate ophthalmic emulsion is a novel formulation including a more powerful steroid, and glucocorticoid that links the affinity of difluprednate for active metabolites was found to be 56 times stronger than that of prednisolone. 20 Furthermore, organization penetration is promoted by adding ester acetate in C-21 difluprednate digit, and an active ingredient can arrive at the uvea. 13 A single instillation of radiolabeled difluprednate was found to result in detectable posterior segment levels. 20 The study data demonstrated that difluprednate inhibited cytokine levels in both the vitreous and aqueous humor, and that betamethasone had an effect on cytokines only in the aqueous humor. These findings suggest that difluprednate may be a more effective anti-inflammatory treatment in the posterior segment.
VEGF promotes retinal neovascularization and blood vessel permeability leading to macula edema, and MCP-1 is known to influence attraction and activation of monocytes and macrophages.21,22 Itaya et al. showed that VEGF and MCP-1 strongly developed with retina pigmented layer after laser damage. IL-6 is multifunctional cytokine participating in inflammation and immunoresponse. 2 IL-6 production is promoted by hypoxidosis and hyperglycosemia, and its impact on blood vessel permeability and a vascularization is shared with VEGF.23–25 ICAM-1 is an endothelium- and leukocyte-associated transmembrane protein. 26 Increases of these proinflammatory cytokines have been associated with the etiology of DME. 24 After laser photocoagulation, these cytokine levels in the aqueous and vitreous humor were significantly decreased in the difluprednate group, which contributes to reduction of the inflammation after photocoagulation that could exacerbate macula edema.
Inhibitory effects on the cytokine levels following difluprednate treatment were observed for a relatively long period. On day 14, the reduction of IL-6 in the vitreous and aqueous humor and VEGF and ICAM-1 in the aqueous humor was maintained with difluprednate but not STTA. This difference might result from the continuing daily application of difluprednate drops compared with the single STTA administration. Daily topical application of difluprednate is a very convenient, functional way of taking medication.
Although difluprednate was effective as a topical corticosteroid, a significant elevation of IOP was observed. All ophthalmic corticosteroids, either topical or systemic, may elevate IOP. Because of its strong steroidal activity, increased IOP would be more prevalent with difluprednate than other ophthalmic steroids. Previous clinical studies reported increased IOP in 20%–40% DME and uveitis patients.15,27 In those series, most patients were controlled by topical hypotensive medications or selective laser trabeculoplasty. Alternatively, our data demonstrated that the withdrawal of difluprednate is effective to reduce IOP. Using this agent as an anti-inflammatory treatment after laser photocoagulation is recommended with close monitoring of IOP. In human, it is reported that the increase of IOP and the therapeutic effect for DME have correlation after the treatment of TA. 19 However, it seems that the cytokine levels were not linked to the elevation of IOP, since we could find no significant relationship between them.
Our and previous reports based on animal models showed the elevation of inflammatory cytokines levels were transient and returned baseline within 14 days after laser photocoagulation.5,17 Also, clinical data showed that progression of macular edema and the increase of anterior flare intensity, which are inflammation markers, were temporal events within ∼6 months after PRP.17,28,29 This finding indicates that the necessity to inhibit the inflammatory reaction using difluprednate may be limited in the early stage after photocoagulation. The limited use of difluprednate would contribute to decrease the risk of IOP elevation.
Although our data are limited to the results of ELISA assay, we conclude that the topical application of difluprednate has a potential to reduce the levels of inflammatory cytokines in the vitreous and aqueous humor after PRP. IOP increase is a promising side effect of difluprednate, however, that can be normalized after the withdrawal of the eye drop. Based on our data, the administration of difluprednate may be effective to inhibit the laser-induced inflammation as well as STTA.
Footnotes
Author Disclosure Statement
No competing financial interests exist.