
Abstract
Abstract
Even though the very thought of an injection into the eye may be frightening, an estimated 6 million intravitreal (IVT) injections were made in the USA during 2016. With the introduction of new therapeutic agents, this number is expected to increase. In addition, drug products that are injectable in ocular compartments other than the vitreous humor are expected to enter the back of the eye market in the not so distant future. Besides the IVT route, some of the most actively investigated routes of invasive administration to the eye include periocular, subretinal, and suprachoroidal (SC) routes. While clinical efficacy is the driving force behind new injectable drug product development for the eye, safety is also being improved with time. In the case of IVT injections, the procedural guidelines have evolved over the years to improve patient comfort and reduce injection-related injury and infection. Similar advances are anticipated for other routes of administration of injectable products to the eye. In addition to procedural improvements, the design of needles, particularly those with smaller diameters, length, and controlled bevel angles are expected to improve overall safety and acceptance of injected ophthalmic drug products. A key development in this area is the introduction of microneedles of a length less than a millimeter that can target the SC space. In the future, needles with smaller diameters and lengths, potentially approaching nanodimensions, are expected to revolutionize ophthalmic disease management.
S
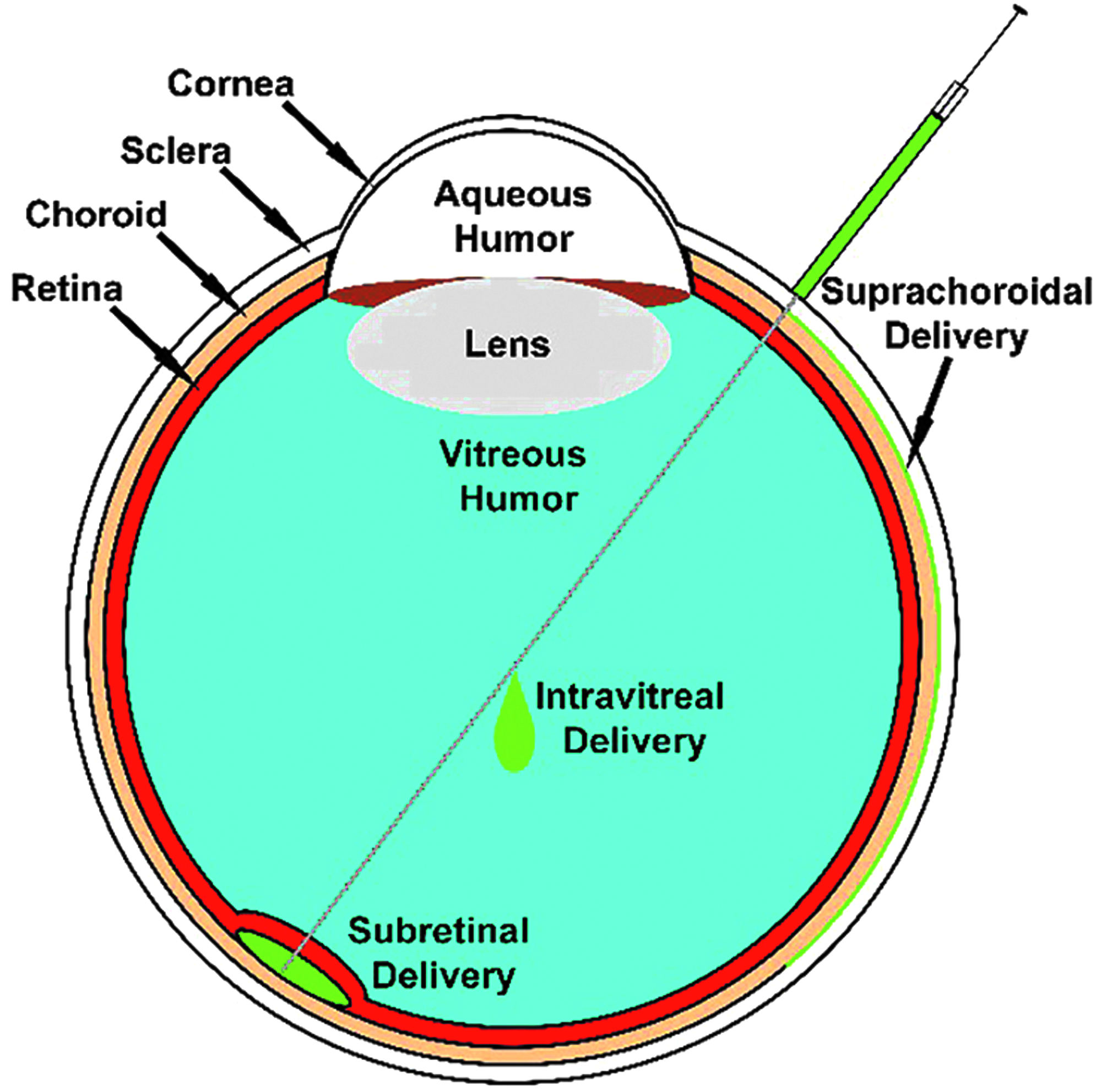
Typical approaches to IVT, SR, and SC injections. IVT, intravitreal; SC, suprachoroidal; SR, subretinal.
Growth of IVT Injections
The first IVT injections, which were described in 1911, used an air bubble to repair retinal detachments. 2 Before 2001, an estimated 3,000–4,500 IVT injections were performed in the United States per year, based on Medicare procedure codes and the American Medical Association (AMA)/Specialty Society Relative Value Scale (RVS) Update Committee Database (RUC).3–5 Currently, it is estimated that ∼6 million IVT injections were performed during 2016 in the United States alone, with the number of injections being considerably larger if worldwide estimates are included.3–5 Besides active ingredient and vehicle composition, 2 key elements that determine the safety of IVT (as well as other intraocular injections) are the needle type and the method of injection. This is evidenced by emerging innovations in needle design for injectable ophthalmic drug products. The experience obtained with IVT and SR injections is expected to shape future technologies, including those intended for other emerging routes of invasive administration to the eye, including the SC injections.
Currently Approved IVT Injectable Products and Recommended Needles
Intravitreally injectable products are currently approved for branched or central retinal vein occlusion, diabetic macular edema, uveitis, and wet age-related macular degeneration, along with others. Table 1 summarizes the United States Food and Drug Administration (US FDA)-approved intravitreally injectable drug products along with the recommended needle sizes for human use. Based on Table 1, it is evident that in recent years, there has been a rapidly growing list of drug products for treatment of the back of the eye diseases. The growth experienced using this procedure and drug products is mainly due to the identification of new validated drug targets for various eye diseases and continuous development of IVT procedures, materials, drugs, and dosage forms that are safe for human use.
FDA, Food and Drug Administration; N/A, not available; TA, triamcinolone acetonide.
In 1998, Vitravene® (fomivirsen sodium), became the first intravitreally injected therapeutic agent that was approved by the US FDA. Even so, it was Kenalog® (triamcinolone acetonide [TA]) that was the first IVT drug with universal application for the treatment of macular edema associated with a number of etiologies. 6 To date, there are at least 9 intravitreally injected products approved by the US FDA (Table 1), with several in clinical trials. The injected therapeutic agents can be immediate release or controlled release products that maintain efficacy for up to around 3 years (ILUVIEN®). In addition, several drugs, including amikacin, amphotericin B, bevacizumab, cefazolin, ceftazidime, clindamycin, dexamethasone, foscarnet, ganciclovir, methotrexate, tobramycin, vancomycin, and voriconazole, are also compounded for IVT injections. 7 Over the years, the adverse events related to IVT injections have declined both due to procedural improvements and enhancement of the needle devices for the ocular drug delivery.
Most medical professionals and academics would generally credit the Irish physician, Dr. Francis Rynd, with perfecting the hollow needle as early as 1845. At that time he used his device to inject the drug morphine into nerve tissue. 8 Since that time, extensive research has been conducted to improve and enhance materials and methods to deliver therapeutic agents to specific areas of diseased tissue at the most effective treatment levels. Hollow needles are among the most widely used medical devices because they can be utilized in a number of different procedures, including biopsy, blood or fluid sampling, and drug product dosing and delivery. Regardless of the application, all procedures depend on the ability of the needle to effectively apply an adequate force that pierces the tissue, without causing significant pain, discomfort, and/or damage. Needle geometry is key to addressing these characteristics and most of the commercially available IVT injection procedural kits contain 27G and 30G needles of half-inch (1.27 cm) length (Table 1). The force required for human skin tissue insertion using 27G needles is significantly higher than those required for 30G needles. 9 Also, with a larger diameter needle, the level of patient discomfort is expected to increase. For instance, it is reported that 53% of insertions with 27G needles caused pain and some bleeding, whereas only 39% of insertions with 30G needles caused similar pain and some bleeding during injections into human skin tissue.10,11 Because of the complex anatomy of the eye, associated needle complications for IVT injections include intraocular infection, subconjunctival or vitreous hemorrhage, vitreous incarceration, fluid reflux, scleral damage, endophthalmitis (EO), and pain. 12
To minimize patient inconvenience and tissue damage, efforts are continuously being focused on miniaturization of needle devices both in diameter and length. It was stated by Hilt and Peppas in 200513 that the smallest needles commercially available were 30G for conventional syringes and 31G for pen injectors, with outside diameters (ODs) for these needles typically being 305 and 254 μm, respectively. Since then, several suppliers have reduced needle lengths and diameters, but mainly for research use. For instance, some commercial needle manufacturers like Japan Bio-Products Co. Ltd. supply 34G needles. World Precision Instruments (WPI), typically a supplier for researchers, has made available 36G needles with an OD around 110 μm, inside diameters range of 25–50 μm, and length of 2.5–3 mm, which is described in their “Sub-microliter Injection System Brochure.” But there is a limit to the decrease in diameter and length of traditional hollow needles because of the ductile nature of small metal needles and their tendency to bend. Also, it should be emphasized that unlike some of the other needles mentioned in the previous text, the WPI needles are not currently approved for human use. More research on novel materials will probably be needed to solve these mechanical limitations. To date, immediate release dosage forms such as drug solutions and slow release preparations, including drug suspensions and polymeric nano- and microparticles, have been assessed in the SCS. It is anticipated that a variety of dosage forms that can be either injected or surgically placed in this location will be viable options in future.
Guidelines for IVT Injections
Most professionals would agree that the reasons that IVT injections have revolutionized the field of ophthalmology are due to procedure guidelines and persistent adherence to them. In 2004, Aiello et al. 14 published a consensus guidelines document for the practice of IVT injections. Since then, there has been a dramatic increase in the use of this procedure because of effective drug development, which increased the possibilities for treatment. The above guidelines form the basis for the current best practice guidelines for IVT injections, including those that have been recently elaborated.7,15,16 Although guidelines are being published and revised for IVT injections, the routine practice is expected to widely deviate from the published guidelines. Indeed, some reports indicated high intraocular pressure (IOP) elevation after IOP injections. Such elevations may be attributed to procedural differences as well as formulation effects.
IVT Injection procedural guidelines focus on 8 areas of concern: (1) Lid Retraction Technique—which can prevent endophthalmis (EO), (2) Anesthesia—which increases patient comfort and prevents movement and involuntary eye lid closure, (3) Topical Antiseptics—which can prevent the growth of microorganisms, (4) Doctor and Patient Respiratory Masking—which can also prevent microorganism growth, (5) Injection Technique—angle and length of the needle can affect reflux and the technique can reduce hemorrhage, (6) IOP—IOP changes after the procedure normally only last for 5 s to 30 min, (7) Post-IVT Injection Antibiotics—which remains controversial, and (8) Safety of Bilateral Injections—best practice is to treat each eye as an individual patient. 16 As evidenced by the literature on this topic, there is a continued debate with regard to a number of these concerns and effectiveness or the lack thereof on procedural success. Although an oversimplification, the above list could be condensed to patient comfort, infection prevention, and needle placement angle and geometry (diameter and length) as the key parameters that influence the appropriate procedures. These criteria are expected to be relevant to other modes of injection, including SR and SC injections.
Patient comfort is a real concern for procedural success and is affected by anesthesia and needle diameter. There are a number of lidocaine-based anesthetics available for use by ophthalmologists, with no evidence that one technique is better than another.16,17 However, EO can result from various sources of microorganisms attached to areas around the eye such as lids, lashes, tear film, and conjunctiva, or even from air exhaled from the doctor and patient.17–21 It is recommended that povidine–iodine (PI) at concentrations between 5% and 10% be applied to the IVT injection site right before the injection. 7 It may also be applied to surrounding structures such as eyelids and eyelashes, but application pressures that could cause the release of meibomian material should be avoided. If a gel anesthesia is being used for the procedure, it is recommended that PI be applied before and after gel application. After the final application of PI, any contact with the injection site by eyelashes and eyelid margin should be avoided. Injection needle diameter data show that pain and/or tissue damage can be reduced with 30G or even smaller gauge needles.9,16,17 Reduction in diameter, however, can limit the type and concentration of a formulation that can be injected. For instance, an increase in resistance to injection is anticipated as the particle size or particle concentration increases in an ophthalmic suspension formulation.
Infection with any medical procedure is always a major concern. Great care should be taken to maintain a sterile procedure environment for IVT injections. Literature suggests that EO is mainly caused by various Staphylococcus organisms and can result in severe vision loss or blindness. 22 Preinjection application of PI seems to be the best active agent to prevent infection as long as it is applied properly and allowed sufficient time to work. Some suggest that corticosteroids might actively suppress the patient immune responses, thereby increasing the chance for infection. 4 Some literature suggests that most of the postprocedural antibiotics may cause more harm than good and that lidocaine-based anesthesia might provide some antibacterial effect.22–25
It is also anticipated that the angle of entry of the needle into the eye will be further optimized to improve patient safety and procedural success. For instance, for IVT injections, scleral tunnel injection at an acute angle reduces vitreous reflux without compromising patient comfort. 26 In this approach, the needle is initially injected at an angle of 15°–30° followed by reorientation of the needle within sclera to a 45°–60° angle before needle entry into vitreous. 26 This creates needle tracks at 2 angles within the sclera, thereby minimizing hemorrhage as well as potential exposure to the atmosphere. It can be envisioned that a similar approach may be useful in reducing any potential blood leakage beyond sclera following SC injection, a procedure further discussed later.
SR Injections
SR injections are being evaluated in animal models and in human subjects, primarily for gene therapies and cell transplants for the treatment of previously incurable, inherited retinal diseases such as Leber congenital amaurosis, retinitis pigmentosa (RP), and the most common form of inherited juvenile macular degeneration known as Stargardt's disease (Table 2). The field of optogenetics is also contributing significantly toward the advancement and use of SR delivery. Early surgical interventions into the SR space used anterior transvitreal, posterior transscleral, and open sky approaches.27–29
In 1992, Wongpichedchai et al. described in great detail their comparison of the internal anterior transvitreal (internal access to SR space via the vitreous) and posterior transscleral transplantation (external access to SR space without passing through the vitreous) approaches to penetrate the SR space in a rabbit model for the purpose of retinal pigment epithellum (RPE) disruption and cell transplantation. 30 The internal approach was performed under direct observation as follows; in the superior quadrant of the eye, a peritomy was made, the superior rectus muscle was grabbed and sutured to rotate the eye. A sclerotomy (an operation for the relief of increased intraocular tension) was performed on an area 3–6 mm behind the corneal limbus once the sclera was exposed. 30 A micropipette connected to a 250 μL syringe, positioned on an electronic injector, was inserted anterior to the equator at an angle away from the lens. The micropipette was advanced until it penetrated the retina to around 200 μm. A localized bleb of the labeled cell suspension was then slowly injected, with 30–40 μL being the appropriate amount to produce the localized detachment of the retina and dislodge RPE cells. 30
The external approach was performed with indirect observation using a 33G needle, the bevel of which was reduced to half the original length and covered with a glass sleeve of the micropipette, ultimately allowing only 4 mm of the needle tip to protrude. 30 After peritomy to expose the posterior sclera, a full-thickness scleral flap was dissected to provide a window of the desired size at the transplantation site. This allowed the needle tip to be visible as it penetrated the choroid. 30 With the needle shaft and tapered tip secured at 15° by 2 sutures 1 cm apart, the needle was advanced protruding 4 mm in length to penetrate the choroid tangentially into the SR space. An aliquot of 100 μL EDTA solution was manually injected using a 250 μL syringe. Cells dislodged from Bruch's membrane by EDTA were aspirated. The syringe was then removed at the hub and replaced with a second syringe containing 50 μL of labeled cultured RPE cell suspension. 30 These cells were then injected, needle removed, and the flap closed. The blebs were completely flat after 1 week for the internal and after 2 weeks for the external approach. Because of the direct observation, the internal approach was deemed more accurate.
Regardless of the approach used, none of the eyes experienced any further retinal detachment following the procedure. Retinal hole diameters were similar to the outer diameter size of the micropipette, around 27–30G needle size for the interior approach, whereas for the exterior approach, the hole diameter was similar to 33G needles. 30 Although complications vary slightly depending on the procedure performed, those common to both approaches were retinoschisis, SR hemorrhage, and retinal atrophy. Use of small gauge needles, careful selection of injection site, diathermy, and prior experience was deemed helpful in reducing occasional SR hemorrhages. While the internal transvitreal approach requires creation of a retinal hole, the external approach resulted in iatrogenic retinal holes in 20% or less of the cases.
The open-sky approach was used by researchers at Columbia University when they transplanted a culture of human RPE cells into the Bruch's membrane of an owl monkey. 29 The anterior segment was opened creating a retinal flap, then underlying RPE cells were removed using trypsinization and gentle rubbing, and labeled cultured cells were introduced into the treated area. The major drawback with this approach was the difficulty in replacing the retinal flap once the new cells were introduced. Even though encouraging results were obtained, it was determined that the pars plana approach was easier and less traumatic. 29
So far, the procedures described for retinal transplantations have involved approaches requiring surgically opening the eye and then suturing the incisions. These types of procedures carry with them the potential for surgical complications such as vitreous loss, retinal detachment, and ocular hemorrhage, which discourage multiple implantation sites. 31 Lazar and DelCerro et al. in 1992 developed a precise means of accessing the SR space in rats using an injection technique with a custom-made device.28,31 They reported that the method was consistent and allowed real-time photography or video to document the procedure. It comprised commercially available materials, a 27G butterfly needle with a 15° bevel, which was tightly sheathed with plastic tubing. The plastic tubing served 2 purposes—it covered the needle so that only 1.1–1.4 mm of the needle was left exposed and provided a stop to limit the depth of needle penetration into the eye tissue. This provided an effective means for preventing retinal holes and tears. A cell suspension was preloaded into a microsyringe, and then, colibri forceps were used to grab the sclera and rotate the eye anteriorly. A stereomicroscope fitted with a video camera was used for the direct visualization of the procedure. The needle with the bevel side up to allow for the best view for the operator was manually inserted through the sclera. Then, it was gently rotated without changing its angle until it could be viewed in the SR space, it was advanced slightly further to elevate the retina and the 2–4 μL of cells injected. This procedure was then repeated rotating the injection site by 180°.
In 2001, Verdugo et al., 28 modified their technique for use in a SR injection or cell transplantation of RPE cells in a canine model, which, once the technique was mastered, also provided consistent results. 28 They used a 29G needle with a 30° bevel covered with tubing exposing only about 3–4 mm that was adjusted accordingly, based on the dog's age and estimated scleral thickness. Injected cell volumes varied with the optimal injection volume described as 100–150 μL administered by injecting twice. Unlike the previous technique, the eye was rotated ventrally, and the superior rectus muscle was then sutured for stabilization. A focal conjunctival peritomy was made with bleeding control by pinpoint cautery. An incision was made in the form a scleral flap to provide a window at the transplantation site, which was sutured closed following the injection. 28 The above procedures, originally developed for experimental cell transplantations, can potentially be adapted for drug product dosing.
Through the years, other investigators have assessed the effects of additives incorporated into the SR injection formulations. In 2007, Maia et al. 32 in a rabbit model explored the effect of preservative-free, preserved TA suspensions (Kenalog; Bristol-Meyers-Squibb, Princeton, NY), or balanced salt solution (BSS) on the retina and found that the preservative-free solution induced less retinal damage. In this study, 16 rabbits were submitted to a vitrectomy. The surgical procedure was standardized by using laser marks and performed by the same individual. Using a 2-port 20G, supplied by Alcon, Inc. (Fort Worth, TX) the vitrectomy was performed. A 41G macular cannula was inserted through the nasal sclerotomy once the vitreous cutter was removed. Independent of the 200 μL aliquots of 1 of the 3 solutions with concentrations of 40 mg/mL injected, the resulting blebs created following the procedure were similar with regard to area diameters. The significance of research on the safety of TA provides important data for chorioretinal disease drug therapy and chromovitrectomy. In this article, the authors also discuss the controversial results between their finding and some other researchers. Key theories for their success were solution preparation, reducing the size of the supernatant TA crystals, concentration, and cannula size. They also raised questions with regard to the toxicity of the secondary agents normally present in the Kenalog suspension.
Then in 2009, Francis et al., 33 performed a study in which fluorescently-labeled human cortical neural progenitor (hNPCctx-GFP) cells were subretinally transplanted into nonhuman Primates (normal macaque monkeys). The cell introduction, 100,000 cells per eye, was performed using the pars plana transvitreal approach. In this case, the retina was approached with 39/22-G curved (Synergetics, O'Fallon, MO) SR cannula connected to a syringe. A BSS was injected slowly to create a small SR bleb, which was then increased once the cannula was introduced to expand the bleb. This minimized the trauma to the retina. The Synergetics cannula was then replaced with a 30G curved cannula (Hurricane Instruments, San Francisco, CA), connected to a piece of sterile tubing preloaded with cells. 33 The cells were slowly added under direct viewing to ensure correct placement. The authors indicated that this approach might be suitable for translation to humans. 33
Petersen-Jones et al. 34 confirmed in a large animal model (canine), some results previously reported in a murine model, that when comparing self-complementary and single strain AAV2/5, self-complementary AAV2/5 showed promise to treat conditions where rapid genetic alterations maybe desired. 34 The retinal injection was performed using an ophthalmic microscope, a vitrectomy lens, and the injection was delivered by using a RetinaJect Injector (SurModics, Inc., Irvine, CA). The injector was inserted using the pars plana approach with direct observation; it was advanced across the vitreal cavity to the retinal surface where a 39G cannula was extended to touch the retinal surface. Each left eye was injected with 250 μL of scAAV2/5-GFP vector at 0.5 × 1012 viral particles/mL, and each right eye was injected with the same amount of the ssAAV2/5-GFP vector. They report that reattachment was confirmed in all 4 eyes injected after only 2 days and also a mild surgically induced inflammatory reaction and retinal inflammation of retinal vasculature, which resolved by itself within a week after the procedure. The fluid injection pressure created a retinotomy, which allowed the fluid to pass through it to the SR space to induce retinal detachment. The first serotype, AAV2, was developed back in the 1980's and cloned from a wild-type virus. Since that time, many other AAV serotypes have been described and studied in the retina, and the general consensus reached by researchers has been that tropism, at the onset of transgene expression, and the specificity of transduction may vary when using different serotypes and host species. 35 However, with recent preparation advances, the AAV2 remains one of the most promising recombinant viral vectors for translational gene therapy. Some of the other serotypes investigated for instance, include AAV2/8, AAV2.sFlt-1, and AAV2-hRPE65v2. 36
Thus, while white papers are being written on the well-established IVT injections, SR injections are being assessed widely and progressed toward clinical studies. This method of injection is probably the most retina-invasive one mentioned in this article. Even so, the data generated by the ongoing clinical trials suggest that these SR injections have managed to provide successful treatment for several of the targeted eye diseases. As a result, gene therapy research continues to grow by leaps and bounds. In recent years, a number of new clinical trials (clinicaltrials.gov) have emerged, for instance, NCT02435940 and NCT03011541 (SCOTS2). A number of researchers have also expressed the opinion that the first therapeutic use of CRISP technology may be for the treatment of RP. The anticipation for the future is clear in that the expectations are focused on improving the active agents and administration techniques. This might even result in the publication of the well-tested guidelines for SR injections.
Emergence of Microneedles and SC Drug Delivery
While IVT and SR needle development in recent years focused on decreasing diameter of the needle used, SC delivery has been primarily enabled by design of needles with micron size lengths (Table 3). Currently, IVT injections use 1.27 cm needles with OD of ∼305–410 μm, and there is a growing effort to reduce these needle dimensions. In terms of drug delivery, the driving force to develop smaller needles in either gauge or length has been mainly for transdermal applications. From this field, some very successful transdermal devices for injections have evolved that are painless and blood free. 11 This has been achieved by using fabrication methods and techniques from other industries to manufacture microneedles. 13
PDS, posterior drug delivery system; POE, poly (ortho) esters; IVT, intravitreal.
Microneedles are expected to offer a less invasive and more reliable means than conventional needles to access the SCS. Accurate placement of drug formulation in the SCS is expected to reduce injury to the underlying retinal layers. These microneedles have been manufactured from a number of materials in a variety of shapes and sizes, as required for different drug delivery systems. Currently, we are beginning to see some technological crossover for drug delivery systems from the skin to the eye. A key emerging area of ophthalmic research that can benefit from small needles is SC drug delivery. The SC drug delivery requires placement of drug product directly beneath the sclera and above the choroid in the virtual SCS. To not pierce the choroidal vasculature or underlying structures in any significant manner, needles used for this purpose are ideally of a length comparable to scleral thickness at less than 1 mm. Given this necessity, needle lengths have decreased to a micron size, that is, below 1 mm.
In initial experiments performed in the last 10 years, researchers have inserted hollow microneedles into the human cadaver sclera (intrascleral), with in vitro and in vivo experiments being performed on rabbit and pig eyes. 37 The primary effort of this group has been application of microneedles for SC drug delivery, although application of microneedles in other sites within the eye is readily feasible. During their experimentation, they infused microparticle and nanoparticle suspensions with particle diameters that included particles of diameters 20 nm, 100 nm, 500 nm, and 1 μm. 37 Because of this research, it was determined that microneedles may provide a minimally invasive approach to circumvent the eye's anatomic barriers to allow for precise placement of the needle to deliver drug molecules and particle suspensions to target treatment areas within the eye. One iteration for an optional ocular microneedle geometry could be described as a needle with a tip angle ≤20°, an adjustable length range between 800 and 1,000 μm, diameters similar to the smallest needle gauges that are capable of delivering drug volumes ranging from 15 to 35 μL, and insertion angles that are procedure-dependent from 75° to 105°.37–41 Another critical factor is the force required to deliver the drug, due to the size of the needle and back pressure from the tissue.37–41 Most physicians and nurse practitioners are uncomfortable applying the needed intraocular injection forces without some sort of aid. For this reason, some professionals have even gone so far as to design and manufacture syringe/needle supports to assist with positioning and injecting. Examples include the guarded injection device,42,43 InVitria® (manufactured by FCI), SCS microinjector (SCS™; Clearside Biomedical), and SpEye™ (Alyko Medicals candidate for the EURETINA Innovation Awards in 2014), to name a few.
The needles for ocular drug delivery in the clinic are currently at centimeter size for length and at micron size for diameters. Continued effort in the development of needles for safe and effective drug delivery is expected to introduce microneedles and even nanoneedles in length and/or diameter. In the recent past, microneedles with length under a millimeter and diameters similar to currently used IVT needles have been assessed in humans for SC delivery, efficacy, and safety (Table 3). In these clinical trials, a microinjector device from Clearside Biomedical, Inc. is being used to inject a TA drug suspension in a 100 μL volume. It is anticipated that nanoneedles can be enabled for intraocular injections eventually, provided that sufficiently strong needles with nanodimensions can be developed for piercing eye tissues. 44 Early results, from the first 6 months of the clinical trial showed excellent safety and promising efficiency performance. Complete trial results could be published sometime next year. An alternative approach for SC delivery developed by iScience Surgical Corporation (Menlo Park, CA) includes a needle piercing followed by 200 μm microcannula- or microcatheter-guided placement of medication within a particular region (eg, near macula) of the SCS. This approach is considerably more complex and invasive than the microneedles, usually involving more equipment, a 2–3 mm incision created in the superotemporal quadrant and performed in an operating room under monitored local anesthesia. Even so, results have been reported as successful.
In the study of Tetz et al. 45 2012, even though several patients had some complications after the SC procedure, none of the patients required secondary procedures during the 6-month follow-up period. There were 21 eyes in the study, only 1 eye experienced IOP, which was controlled, and only 1 required temporary treatment with glaucoma medications. From the eyes that were phakic, initially 2 experienced an increase in nuclear sclerosis. No patients experienced SC hemorrhages, and there was no visual evidence of retinal or choroidal tissue trauma. 45 Compared with IVT injections and SR injections, relatively few groups have working experience with SC injections. With the ongoing assessment of microneedles for SC delivery in clinical studies and wider acceptance of this procedure for drug delivery, guidelines for SC injections are expected to evolve.
Conclusions
In conclusion, IVT injections have been widely accepted over the last few decades for treating various intraocular diseases. Safety and effectiveness of this medical procedure has been studied extensively as evidenced by the number of published articles on this topic; however, there is still room for improvement. As with any medical procedure, protocols and guidelines for IVT injections need to be adhered to have successful outcomes. In addition to IVT injections, several other intraocular injections are feasible, for example, SR, SC, and periocular. A number of approaches have been developed for SR injections, with the transvitreal injections via pars plana area being the most common. In future, the availability of microneedles may further advance the use of transscleral approaches for SR delivery. SC delivery, a newer method of drug delivery, received considerable attention in the recent years. This is mainly because of the design of small microneedles and cannulas for drug deposition in the SCS. It can be envisioned that small diameter needles approaching nanodimensions may be useful for ocular drug delivery, especially for localized delivery of potent drugs. Nanoneedles are expected to reduce any tissue damage associated with IVT, SR, and SC injections with conventional needles. The smaller the diameter of the needle the lower is the vitreal efflux expected at the point of needle entry. However, nanoneedles will likely be viable for injecting clear, low viscosity liquids, including solutions, nanosuspensions, and nanoemulsions. With an increase in injection volume, particle size, and viscosity of the formulation, resistance to injection is expected to be higher for nanoneedles as opposed to conventional needles. In addition to the modes of administration discussed in this article, nanosize needles are expected to be safer for ocular surface injections. Development of miniature medical devices and needle geometries is likely to improve drug delivery as well as patient safety of intraocular injections. In the future, it is anticipated that smart and miniature needle baring devices will be used to advance multiple applications in various locations within the eye.
Footnotes
Acknowledgments
Author Disclosure Statement
No competing financial interests exist.