
Abstract
Abstract
Purpose:
Retinoblastoma is a childhood malignancy of the retina. To increase the exposures of systemic chemotherapy, high-dose cyclosporine, as a P-glycoprotein modulating agent, has been combined with a standard chemotherapy. However, the effective and safe dose of cyclosporine has not been well evaluated. This study is to optimize cyclosporine dose using population pharmacokinetic modeling.
Methods:
Clinical data were obtained from 161 systemic chemotherapy cycles of 34 pediatric retinoblastoma patients between December 2006 and April 2015. Total 15 scenarios were simulated by 5 different doses (12, 14, 15, 17, and 20 mg/kg) of cyclosporine in 3 different weight groups (5–10, 10–15, and 15–20 kg). Numerical success ratio was obtained after assessing the simulated target cyclosporine concentration in the range of 2,000–2,500 ng/mL using NONMEM version 7.3 software.
Results:
A final model was built based on a 1-compartment model with weight-normalized allometric scaling to minimize the variability of pediatric size. In simulations, numeric success ratio with 15 mg/kg/day and the above were higher than that of traditional doses in all of the scenario groups. No significant adverse responses were reported.
Conclusion and Relevance:
High-dose cyclosporine regimen as a P-gp modulator is required to improve the efficacy of systemic chemotherapy with caution in pediatric patients with retinoblastoma. Clearance, volume of distribution, and body weight are important parameters to consider in selecting adequate dosing regimen.
Introduction
R
Intravenous chemotherapy has been recognized as the most important eye-sparing treatment for intraocular retinoblastoma after the growing awareness of the second tumor risks with external radiation therapy. 2 However, chemotherapy had to be combined with focal treatment approaches for adequate tumor control since the mid 1990s, because it was rare for a tumor to be cured with chemotherapy alone even after number of treatment cycles. 3 The current trend of chemotherapy for the treatment of patients with retinoblastoma is focal therapies, which directly deliver chemotherapeutic agents to the eye or through regional arteries to improve cure rates and reduce the morbidity of less selective modalities. Nonetheless, intravenous chemotherapy is still commonly used to treat tumors that are too large or widespread to treat with focal modalities, such as cryotherapy, thermotherapy, or brachytherapy. For these reasons, intravenous chemotherapy is common primary, eye conservation approach for treating intraocular retinoblastoma. Often, extensive tumors in the posterior pole will shrink enough with chemotherapy to allow treatment with focal modalities in an attempt to preserve at least a portion of central vision.4,5 The first-line chemotherapy is a combination of vincristine, etoposide, and carboplatin in 3–6 cycles.6,7 However, that maximizing the concentration of chemotherapy agents in cancer cells has been a clinical challenge. By the review of Thomas et al., one of the methods to overcome this limitation is to inhibit P-glycoprotein (P-gp) efflux transporters in the blood–brain barrier and the ocular region8,9 by a P-gp inhibitor, such as high-dose cyclosporine suggested by Chan et al. 10 In addition, they found that the success rate in their patients tended to correlate with higher doses of cyclosporine. But, high serum concentrations of cyclosporine (Cpcyclosporine) have not been incorporated into their chemotherapy regimens in clinical practice owing to high variations in therapeutic range between individuals and it has not yet been validated. 11 The effective target levels of Cpcyclosporine are still controversial due to lack of clinical evidence on retinoblastoma.
In this study, we aimed to determine the optimal dose of cyclosporine using a population pharmacokinetic model in pediatric patients receiving systemic combination chemotherapy for retinoblastoma.
Methods
Study design
This retrospective study abstracted clinical data from electronic medical records of pediatric patients diagnosed with retinoblastoma and treated with high doses of cyclosporine at the Retinoblastoma Center of a 1,800-bed tertiary university hospital from December 1, 2006 to April 30, 2015.
Inclusion criteria
Pediatric patients diagnosed with retinoblastoma and treated with systemic chemotherapy (vincristine, carboplatin, and etoposide) in combination with high-dose cyclosporine were included. High dose of cyclosporine was defined as cyclosporine administered in the range of 10–20 mg/kg. The target steady state Cpcyclosporine was 2,000–2,500 ng/mL on day 2.
Exclusion criteria
The exclusion criteria were as follows: (1) failure to receive the total dose of cyclosporine, with exception of dose adjustments or changes on days 1 and 2, and (2) incomplete documentation on Cpcyclosporine, infusion duration, or sampling time of cyclosporine.
Protocol of systemic chemotherapy with cyclosporine
Systemic chemotherapy (vincristine, carboplatin, and etoposide) with an adjuvant cyclosporine was administered as every 3-week cycle. These protocols contained vincristine 1.5 mg/m 2 intravenous on day 1, etoposide 150 mg/m 2 infusion over 3 h on day 1 and 2, and carboplatin 200 mg/m 2 infusion over 3 h on day 1 and 2. Cyclosporine was infused over 24 h and started 3 h before the first dose of chemotherapy on day 1 and 2. Cpcyclosporine was sampled 20 h after administration of cyclosporine on days 1 and 2.
Patient characteristics
Patients' age, height, weight, sex, age at diagnosis, and stages of retinoblastoma, which were determined using the Children's Oncology Group version of the International Classification of Intraocular Retinoblastoma, were collected as baseline patient characteristics. 12 Tumor characteristics, such as the extent of tumor as determined by experienced oncologists. 12 Patients' serum creatinine, aspartate transaminase (AST), alanine transaminase (ALT), total bilirubin, serum albumin, hematocrit, and total cholesterol were measured at the beginning of each cycle. The cycle number, weight-based dose (mg/kg), dose changes (%), Cpcyclosporine, administration duration, plasma sampling time, and concomitant medications were assessed. A chemotherapy-free interval of more than 1 year was considered new treatment. Dose adjustments were expressed as percentage changes by original weight-based dosing (%). Concomitant medications taken from 1 day before cyclosporine administration to the last day of cyclosporine treatment were reviewed to determine whether the drug interaction category falls to “consider therapy modification” through “avoid combination” from 5 categories: unknown, no action needed, monitor therapy, consider therapy modification, and avoid combination by using UpToDate® database. 13
Population pharmacokinetic modeling analyses
Population pharmacokinetic modeling was developed using NONMEM (version 7.3; Icon Development Solutions, Hanover, MD) assisted by Perl-speaks-NONMEM (PsN version 4.2.0). The first-order conditional estimation with eta-epsilon interaction option (FOCE+I) method was used, and 1-, 2-, and 3-compartmental open models with first-order absorption were tested as a base model. In addition, lag time and transit compartment models were compared to describe delayed absorption of drugs during the base model-building step Interindividual variability represented by η was evaluated with additive, proportional, and exponential models. Residual variability represented by ɛ was assessed with a combined (additive and proportional) model.
In this study, the clearance (CL) and volume of distribution (Vd) were tested because of the theoretical relationship between them. To express the relationship betweenpharmacokinetic parameters and covariates, allometric scaling equation normalized by standard body weight was used for body weight, and sigmoid hyperbolic model was used for organ maturation.14,15 Before quantifying effects of covariates that were not related to patient size and age, covariate reduction steps were performed with correlation among covariates. If the value of correlation coefficient between covariates was over 0.5, those covariates were unified with other summary variable or one of the weighted covariates was fixed to remove correlations. 14 After the covariate reduction step, stepwise covariate modeling was performed to derive the final model. Covariates, including sex, AST, total bilirubin, serum albumin, estimated glomerular filtration rates, hematocrit, total cholesterol, cycle number for chemotherapy, and concomitant medications with potential drug interactions were tested using forward selection–backward elimination processes with the likelihood ratio test to determine whether the potential covariates affected the pharmacokinetic parameters of cyclosporine. The effect of covariates on pharmacokinetic parameters was tested by linear, exponential, and power function models. Covariates were centralized with their own median values, and significance levels of P < 0.05 [ΔOBFV (objective function value) >3.84] and P < 0.01 (ΔOBFV >6.64) were used in the forward and backward selection processes. As additional model selection criteria, the precision of parameter estimates, goodness-of-fit (GOF) plots, and prediction-corrected visual predictive check plots were considered. Bootstrap (n = 1,000) was performed as an internal validation method to calculate bias, standard errors, and confidence intervals of the parameter estimates.
Simulation analyses
Three groups of body weight (5–10, 10–15, and 15–20 kg) were created based on random sampling with prior information about mean and standard deviation from 2007 Korean Growth Chart in Korean children and adolescents 2007, 16 which has been endorsed by the Korean government health to date, performed with R 3.1.1 and R studio. In each group, 1,000 samples were simulated for each dosing scenario: 12, 14, 15, 16, and 20 mg/kg of cyclosporine. Numerical predictive check, the success ratio of simulation scenario, was obtained to assess the simulated target Cpcyclosporine below the maximum tolerable range by visual inspection.
Safety analyses
Adverse event reports, including hypersensitivity reactions suspected to be related to the administration of cyclosporine, were reviewed. Addition of new medications, extension of length of hospitalization, and life-threatening incidences were outcomes of interest that were related to adverse event reports. Any causality categories were evaluated as probable, likely, or certain using the WHO-UMC criteria. 17
Results
Patient characteristics
The study enrolled 34 pediatric patients who received 161 chemotherapy cycles after excluding 61 cycles and 1 patient (Fig. 1). The stages of retinoblastoma are presented in Table 1. The mean number of chemotherapy cycles was 11.2 (range: 2–30). Patients received high-dose cyclosporine-combined chemotherapy at an average of 4.9 ± 3.3 cycles, and the average dose increased based on weight was 9.7% ± 14.8%. High-dose cyclosporine was administered at a mean dose of 13.0 mg/kg/day, and the average Cpcyclosporine was 1,331.0 ng/mL on day 1 and 1,300.8 ng/mL on day 2. The mean plasma value was 1,315.9 ng/mL during the full course of the first 2 days (Table 2).

Enrollment of study patient.
Patient Characteristics
Data are n (%) or median (range).
In bilateral retinoblastoma, the stage of each stage (the worse eyes) per patient was counted.
Characteristics and Clinical Information of Each Chemotherapy Cycle
The result is beyond or below the indicator range.
Estimated according to age using the equations of Schwartz et al.
AST, aspartate aminotransferase; ALT, alanine aminotransferase; BUN, blood urea nitrogen; SD, standard deviation.
Population pharmacokinetic model analysis
The final model equation is given below, where Vd: volume of distribution,
During stepwise covariate forward selection step (P = 0.05) and backward elimination step (P = 0.01), body weight was incorporated into Vd and CL as a power function model, with an exponent value of 0.859. The estimated pharmacokinetic parameters and the fundamental GOF plot of the final model are presented in Table 3 and Fig. 2, respectively. Visual predictive check showed that the observation data fit well within the 5th–95th percentiles of simulation and were symmetrically distributed in Fig. 3.
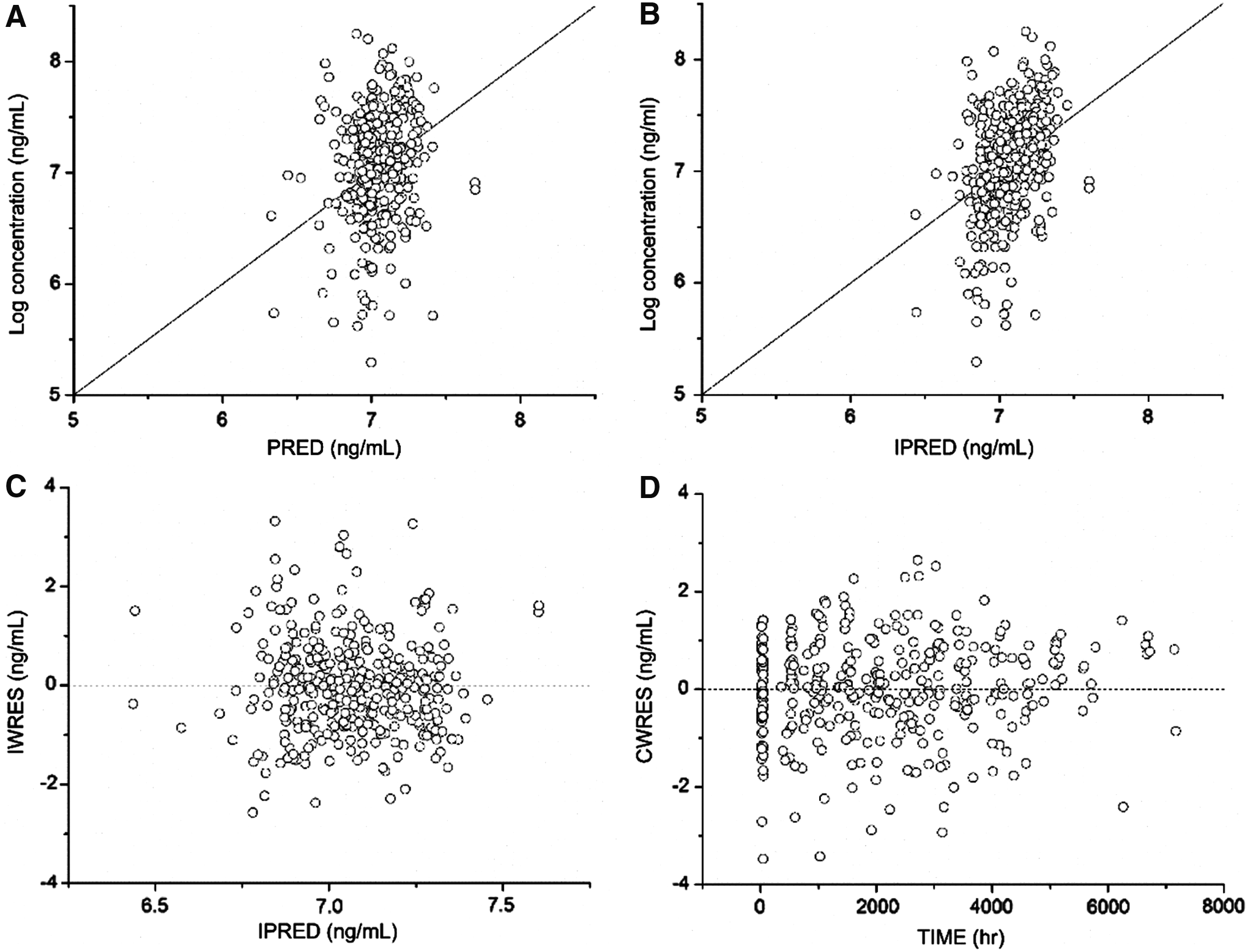
Fundamental goodness-of-fit plot of final model. Estimated cyclosporine concentrations at 44 h after first cyclosporine dose.

The visual predictive check plot. Open circle are observed plasma concentrations of cyclosporine. Upper, middle, and lower shade block are model-predicted 95th percentile, median, and 5th percentiles of model simulated data (n = 1,000).
Final Estimated Pharmacokinetic Parameters and Interindividual Variability Values of Final Model
CL, clearance of cyclosporine; CV, coefficient of variation; RSE, relative standard error; Vd, volume of distribution.
Simulation for individualized dosage prediction
Cpcyclosporine increased with increasing doses of cyclosporine (12, 14, 15, 17, and 20 mg/kg) in all 3 different weight groups. The highest increase was at 44 h after cyclosporine initiation, with prediction values of 5, 50, and 95th percentiles of simulation (Fig. 4).

Simulation plots for patients after administration of cyclosporine
The success ratio to reach the target Cpcyclosporine of 2,000–2,500 ng/mL was not higher than 7.27% with cyclosporine dose of 12 mg/kg in all the 3 body weight groups. For simulations with ≥15 mg/kg of cyclosporine, all of the body weights had a success ratio higher than 7.27%.
Safety
Of 161 chemotherapy cycles, 10 adverse cases related to cyclosporine were reported in 34 patients. Eight cases were mild rash and itching, and all of these were resolved with chlorpheniramine. When cyclosporine was rechallenged in 6 cases, no subsequent adverse events were observed. One case of seizure and hypernatremia without subsequent events was reported. There was one report of hypertension, which was stabilized with hydralazine injection.
There were 5 cases (3.1%) in “consider therapy modification” or “avoid combination” drug interaction categories, and 4 cases involved clarithromycin and 1 case reported seizure caused by phenytoin.
Discussion
Gallie and the colleagues reported that chemotherapy without a focal treatment did not control most intraocular retinoblastoma, perhaps because of the common high expression of multidrug resistance P-gp in retinoblastoma. 18 When the intravenous systemic therapy treating retinoblastoma combines short courses of high-dose chemoagents and simultaneous, high-dose but short-duration cyclosporine, it targets multidrug resistance without increased chemotoxicity occurring. 19 Cyclosporine as an adjuvant anticipates to inhibit P-gp transportation to block P-gp-induced efflux of vincristine and etoposide, and possibly modulates responses to carboplatin. 10 Thus, administration of cyclosporine as a P-gp inhibitor was expected to potentiate therapy by the increased concentration of chemotherapy agents even when long-term systemic chemotherapy alone could not be relied on controling intraocular retinoblastoma. 20 Therefore, it further potentially delays the invasive treatment and the enucleation, especially for the patients with bilateral retinoblastoma.
The majority (83%) of patients in the present study had advanced stage retinoblastoma (stage D or E) and 35% had bilateral retinoblastoma, therefore, aggressive treatment was indicated. However, only 7.27% of the pediatric patients reached the target cyclosporine concentration of 2,000–2,500 ng/mL. Several studies showed the efforts to improve the efficacy of systemic chemotherapy by increasing cyclosporine concentrations. In a study evaluating cyclosporine dose in combination with etoposide, it was observed that Cpcyclosporine had to be higher than >2,000 ng/mL to increase the area under the curve of etoposide. 8 A study on 13 pediatric patients showed that Cpcyclosporine of 1,359–4,835 ng/mL was obtained after 15 mg/kg/24 h cyclosporine was administered for 60 h in combination with etoposide.3,21 Generally, children below 5 years of age have higher cyclosporine clearance than patients older than 5 years of age. Therefore, administering a higher weight-based dosing in children below 5 years of age were also considered. 22 It was a challenge to reach the target steady-state Cpcyclosporine with the usual administered dose of 12 mg/kg in pediatric patients.
In our retinoblastoma clinic, it has been a challenge to prescribe the optimal dose of cyclosporine to achieve the target concentration since there is lack of available data with the dosing. Moreover, the dose of cyclosporine as P-gp inhibitor is much higher than that of other indications as an immunosuppressant, disease-modifying antirheumatic drug, immunomodulator, and calcineurin inhibitor, so that there are profound safety concerns among practitioners. Nonetheless, such a study to find the dose is too hard to perform in a format of prospective study or national claims data analysis due to ethical reasons and the rareness of the disease. The number of patients in our study was 34 pediatric patients who were rather small, but it was similar or of higher number than other studies.3,21
One-compartment pharmacokinetic modeling was found to be a reasonable model with our continuous administration of cyclosporine. The CL was 6.03 L/h, which was comparable with the CL of 5.9 L/h obtained in a previous study in hematopoietic stem cell transplant (HSCT) patients with a mean age of 10.5 years. Other studies reported higher clearances of 14.8 and 15.1 L/h for pediatric patients.21,23 The Vd in our study was 38.7 L. Ni et al. reported a Vd value of 89.1 L for pediatric patients with aplastic anemia. 24 Another study showed a Vd value of 192 L for adult leukemia patients. 25 The differences in CL and Vd could be due to different types of disease or physiological organ maturation of study population. Weight-based dosing, which was common in pediatric patients and comparable to doses based on body surface area, was used in the present study. 22 We found that creatinine clearance, blood urea nitrogen, ALT, AST, total bilirubin, and albumin values had no effects on the final model. This may be due to the minimal preexisting organ dysfunction in our pediatric patients.
Concomitant medications caused potential drug interactions in 3.1% (n = 5) of the study cycles. In 1 HSCT study, 4.1% of drugs concomitantly used with cyclosporine were in risk categories “consider therapy modification” or “avoid combination” (itraconazole, voriconazole, and phenytoin), and there were no clinically significant drug interactions.25,26 It was similar with our study. Some studies reported significant drug interactions between corticosteroids and cyclosporine. 14 However, interaction with corticosteroids was classified as category “monitor therapy”, and was therefore not analyzed.
Of the 10 adverse events reported (6.2%), 7 were very mild reactions without subsequent complications with rechallenge. So far, previous studies reported no serious adverse events with even higher doses of cyclosporine than those in our study.14,18,21,27 In a study where the loading dose of cyclosporine was 2–8 mg/kg for 2 h and 5–24 mg/kg/day in conjunction with etoposide for 3 continuous days, no serious adverse events were reported, despite the high cyclosporine plasma concentration of 4,800 ng/mL. 28 Nevertheless, in 3 of 8 patients who exhibited plasma concentrations >6,000 ng/mL, 2 serious cases of kidney damage were reported. In the same study, hyperbilirubinemia was observed when at least 14.6 mg/kg/day of cyclosporine was administered with the average Cpcyclosporine reaching above 2,354 ng/mL; however, it resolved in the following days. 28 Considering the adverse events reported at high target levels of ∼5,000 ng/mL and the above in other studies, a target steady-state Cpcyclosporine of 2,000–2,500 ng/mL at 44 h could be reasonable sugestions with the administration of systemic chemotherapy.
This study has several limitations. Although the study hospital runs one of the major retinoblastoma special clinics in Korea, only 34 pediatric patients were available over the study period because retinoblastoma is such a rare disease. It was a retrospective study that the data collected were based on the electronic chart review. However, we were able to perform a population pharmacokinetic modeling to suggest to elevate cyclosporine dose, a P-gp inhibitor, to enhance the effect of systemic chemotherapy.
In summary, in our simulation models with 3 different ranges of body weight, when cyclosporine doses were equal to or higher than 15 mg/kg, the success ratios reached the target concentration greater than 7.5% in the study. Thus, our result supports that increasing the dose of cyclosporine above 15 mg/kg would achieve the concentrations capable of reaching the target level. But, at the same time, the conservative approach with careful dose increase should be considered owing to inter- and intraindividual variability in cyclosporine pharmacokinetic as well as potential adverse effects. Further clinical research on the selection of cyclosporine dose as a P-gp inhibitor is warranted.
Conclusions
To the best of our knowledge, this is the first study to optimize high-dose cyclosporine as a P-gp inhibitor in combination with systemic chemotherapy using population pharmacokinetic modeling in pediatric patients. This result provides an evidence for the effective and safe use of cyclosporine in the pediatric population.
Footnotes
Acknowledgments
The authors wish to thank Ms. Caroline Kim at the School of Pharmacy, University of Maryland, Baltimore, MD who supported the medical writing of the article and the collaboration of the staff members of Pediatric Oncology unit in Yonsei University Medical Center. Authors did not receive any specific funding to conclude this article.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Review Board at the University Health System (IRB 4-2015-0372) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived for individual participants included in the study given the retrospective nature of this work.
Author Disclosure Statement
No competing financial interests exist.