
Abstract
Abstract
Purpose:
To evaluate the efficacy and primary safety of treatment with artesunate in reducing ocular neovascularization in humans.
Methods:
Five patients with corneal, iris, and retinal neovascularization and no light perception were treated with intravitreal injections of artesunate 80 μg. Visual acuity, anterior segment photography, fundus fluorescein angiography, and optical coherence tomography were used to evaluate efficacy, while intraocular pressure (IOP) and lens opacity degree were employed to evaluate safety. The primary endpoint was attenuation of neovascularization as determined at 24 weeks, with the last posttreatment follow-up at 52 weeks.
Results:
Corneal and iris neovascularization, which were secondary to fundus ischemic diseases and retinal neovascularization in all 5 patients, were attenuated after 1 or 2 injections by the 52-week follow-up. Retinal neovascularization was also attenuated, and papilledema was alleviated. The average IOP fell from 25.5 mmHg to 17.66 mmHg.
Conclusions:
This pilot study determined that intravitreal artesunate injection is efficacious for reducing corneal, iris, and retinal neovascularization. These results indicate that this drug may be a novel alternative to the currently popular antivascular endothelial growth factor drugs used to suppress ocular neovascularization and improve visual function.
Introduction
Ocular neovascular diseases are common worldwide. They affect nearly all ocular tissue and cause severe vision loss, sometimes even irreversible blindness. 1 These diseases can be primarily categorized as corneal neovascularization, rubeosis iridis or iris neovascularization, retinal neovascularization, or choroidal neovascularization depending on the location in which they are observed. 2 Although they occur at different anatomic sites, they have similar pathogeneses. Multiple factors regulate endothelial cell proliferation, migration, and angiogenesis through a series of molecular mediators, and vascular endothelial growth factor (VEGF) plays a key role in some of them.1,3 At present, the most widely used therapies for ocular neovascular diseases are anti-VEGF protein drugs, such as bevacizumab, ranibizumab, aflibercept, and conbercept, all of which produce sustained improvements in vision. 4 However, these protein drugs share the same limitations and drawbacks. For example, their target sites are essentially limited to VEGF and placental growth factor, which may be the reason these drugs are ineffective for some patients.1,5 Furthermore, compromised systemic vascular health, 6 high price, and the need for cold chain management limit their application. Therefore, a drug that is easier to synthesize and more effective for treating ocular neovascular diseases is needed.
Artemisinin is extracted from the Chinese herb qinghao, and it has remarkable antimalarial 7 and antitumor properties. 8 Youyou Tu, who discovered the antimalarial effects of artemisinin, received the Lasker Award and the Nobel Prize for her contribution to the medical field. As a member of the artemisinin family, artesunate has been demonstrated to inhibit angiogenesis by downregulating VEGF, platelet-derived growth factor, and protein kinase C alpha (PKCα). In addition, we have proved that artesunate can inhibit iris and retinal neovascularization in rabbits and iris neovascularization and macular edema in monkeys with no obvious side effects on the lens, retinal blood vessels, or retinal function. 9 Additionally, the ease of synthesis and storage and safety in systemic applications make artesunate more advantageous than current protein drugs.
However, so far, there has been no report on the application of artesunate to patients with ocular neovascularization diseases. The efficacy of treating ocular neovascularization in different areas and its safety in the eye have not been validated. So, we designed this pilot clinical study to evaluate the efficacy and safety of artesunate in human patients. As the current treatment for ocular neovascularization diseases has a relatively clear curative effect, in the interest of the patients, we recruited only patients with extremely serious ocular neovascularization for whom current therapy does not make much sense to determine the inhibitory effects of artesunate on corneal, iris, and retinal neovascularization and its safety in the eye.
Methods
The study protocol was reviewed and approved by the medical ethics committee of Zhongshan Ophthalmic Center, Sun Yat-sen University, China (No. 2014MEK064) and adhered strictly to the principles of the World Medical Association Declaration of Helsinki. All patients were provided with an explanation of the purpose and plan of the study, and they were informed that the product is not currently labeled for intravitreal injection. They provided written informed consent before participating in this study (ClinicalTrials.gov Identifier: NCT02448732).
Subjects
The screening criteria for corneal, iris, or retinal neovascularization was: 18–75 years of age with no light perception in the target eye and best corrected visual acuity of contralateral eye above 0.05. Corneal and iris neovascularization were secondary to fundus ischemic diseases. Patients with systemic diseases and those receiving systemic antineovascular therapy were excluded. All the patients were diagnosed by the same ophthalmologist. Neovascularization was verified according to the patients' medical histories, fluorescein angiography images, and optical coherence tomography (OCT) results. All the patients received injections from the same surgeon at the Zhongshan Ophthalmic Center, Guangzhou, China.
Artesunate injections
Artesunate was obtained from Guilin Pharmaceutical Co., Ltd. (Guangxi, China), dissolved in a sodium bicarbonate solution, then diluted to 1.6 mg/mL with intraocular perfusion fluid. As the effective concentration of artesunate is 20 μg/mL, 9 and the human eye vitreous volume is 4 mL, 10 the injection aliquot contained artesunate 80 μg per 50 μL.
After instillation of 1 or 2 drops of 5% povidone iodine in the conjunctival cul-de-sac for corneal anesthesia and mydriasis, the intravitreal injection was administered after corneal anesthesia and mydriasis. Under direct visualization, an ophthalmologist injected artesunate 80 μg in the superior temporal quadrant located 3 mm behind the limbus. After withdrawing the needle, the scleral entrance site was compressed with a cotton tip for 1 min, and a topical antibiotic ointment was instilled in the fornix.
Posttreatment follow-up
The posttreatment follow-up times were 1 day (P1D), 3 days (P3D), 1 week (P1W), 4 weeks (P4W), 12 weeks (P12W), 24 weeks (P24W), and 52 weeks (P52W). At each follow-up, best corrected visual acuity was assessed, and noncontact tonometer or Goldmann applanation tonometer, slit lamp, and funduscopic examinations were conducted. At P4W, a different ophthalmologist evaluated whether the treatment was effective and decided if the patient should receive a second injection. The criteria for a second injection was no obvious therapeutic result and the patient continued to have an elevated high intraocular pressure (IOP) or other painful complications. Corneal neovascularization was scored on a scale of 0–3 (0 = no vessel; 1 = vessels detectable under a surgical microscope; 2 = vessels easily seen under a surgical microscope; and 3 = vessels easily seen near the center of the cornea under a surgical microscope).11,12
The grading criteria for iris neovascularization were as follows: (1) fine surface neovascularization of the pupillary zone of the iris, involving 2 or fewer quadrants; (2) surface neovascularization of the pupillary zone of the iris, involving more than 2 quadrants; (3) in addition to the pupillary zone, neovascularization of the ciliary zone of the iris and/or ectropion uveae involving 1 or 2 quadrants; and (4) neovascularization of the ciliary zone of the iris and/or ectropion uveae involving 3 or more quadrants. 13 The primary endpoint was attenuation of neovascularization determined at 24 weeks, and the last posttreatment follow-up was performed at 52 weeks. To evaluate the efficacy of the treatment, corneal and iris neovascularization were assessed in anterior segment photographs. The safety of the treatment was evaluated based on the occurrence of endophthalmitis, cataracts, and elevated IOP.
Results
Five patients were recruited to participate in this pilot study. One participant (Patient 1) had corneal neovascularization, 3 (Patients 2–4) had iris neovascularization, and 1 (Patient 5) had retinal neovascularization. Their basic information, etiology, and previous treatments are summarized in Table 1.
Basic Information of the Study Subjects Is Provided
IOP, intraocular pressure; PPV, pars plana vitrectomy; CRVO, central retinal vein occlusion; PRP, panretinal photocoagulation; BRVO, branch retinal vein occlusion; NLP, no light perception.
Attenuation of corneal neovascularization with retinal detachment
We recruited a 65-year-old man (Patient 1) with retinal detachment in the right eye to treat his corneal neovascularization with intravitreal artesunate injections. This patient had undergone surgery and received a silicone oil injection in another hospital 1 year earlier but developed severe corneal opacification and neovascularization in his right eye, and the IOP was 6 mmHg before injection.
He received intravitreal artesunate injections and eyedrops containing tobramycin dexamethasone, pranoprofen, and diclofenac for 1 week. At P24W, neovascularization had clearly improved from the center of the cornea, and the neovascularization score decreased from 3 to 1 as shown in Fig. 1. The patient's IOP was 7.7 mmHg, and these improvements were still evident at P52W.
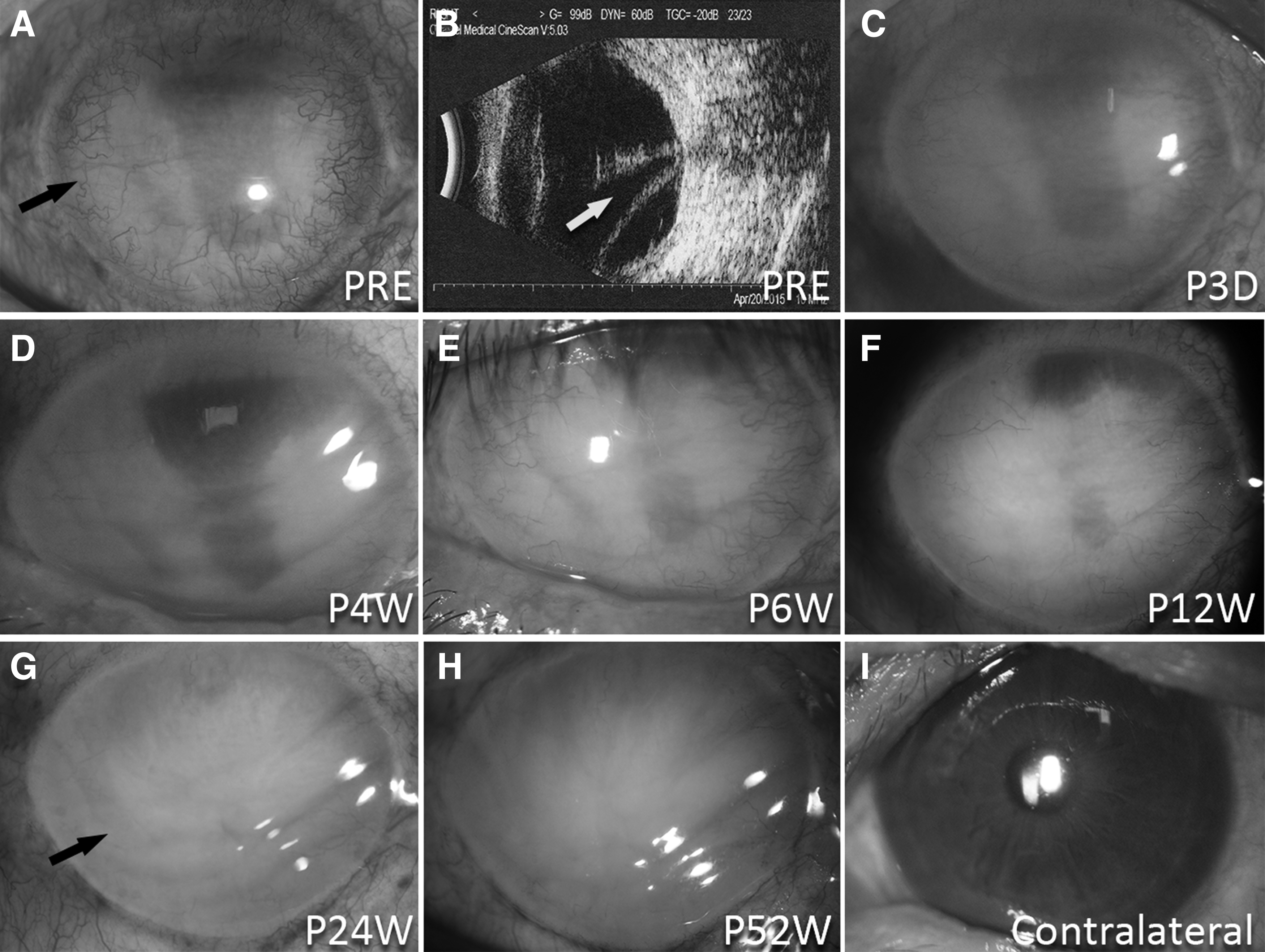
Attenuation of corneal neovascularization in Patient 1 with retinal detachment.
Iris neovascularization regression with vitreous hemorrhage or retinal detachment
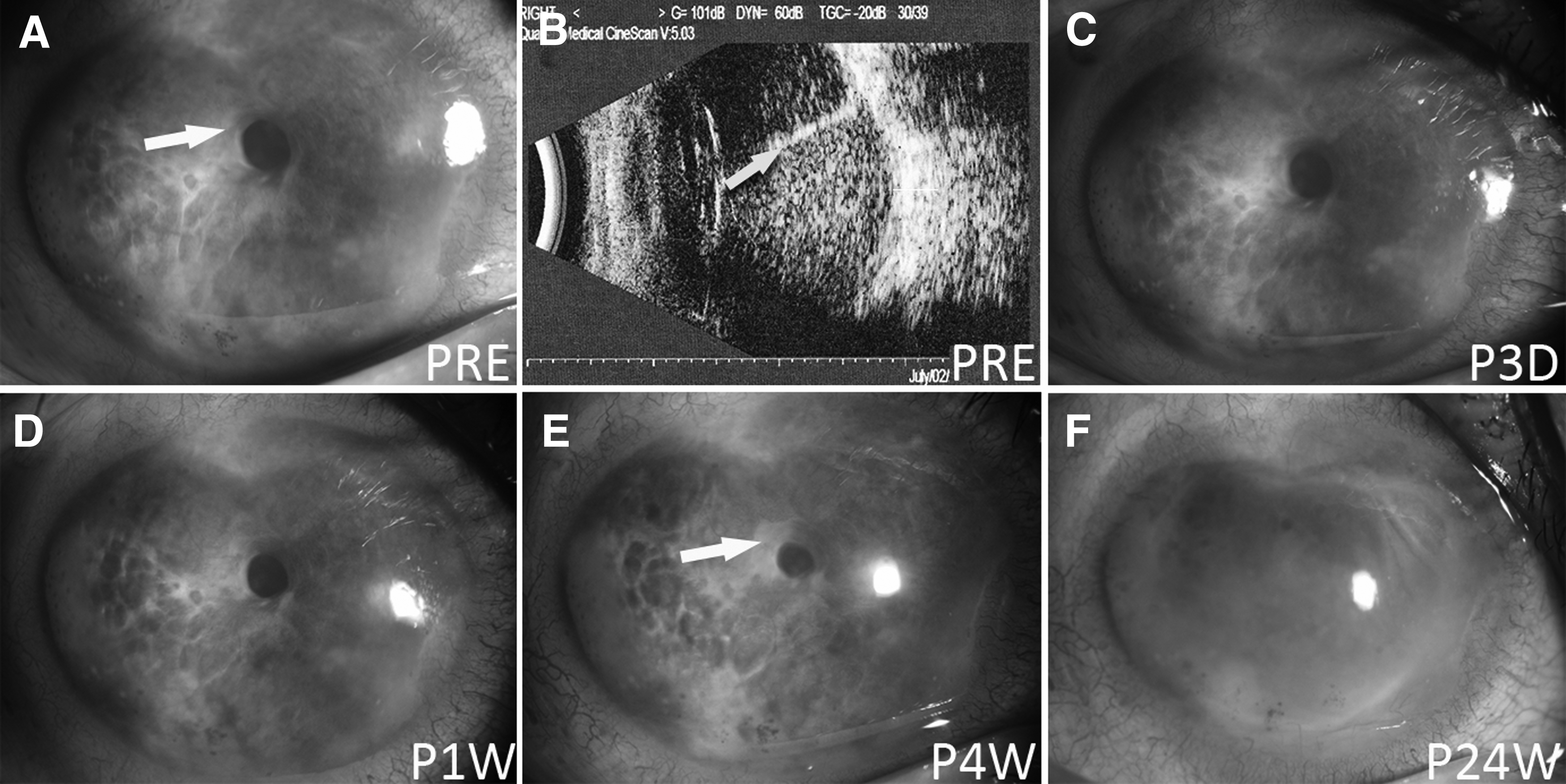
Three participants (Patients 2–4) with iris neovascularization were recruited. Patient 2 was a 65-year-old woman, and her left eye had undergone pars plana vitrectomy with silicone oil injection because of vitreous hemorrhage. Her initial IOP measured by noncontact tonometer (NCT) was 45 mmHg, even though she had taken methazolamide tablets and applied brinzolamide and timolol maleate eye drops. Conjunctival congestion, corneal edema, keratic precipitate, irregular pupil, clear anterior chamber, corneal and iris neovascularization, and mild obscure fundus were present on the first examination. After an artesunate intravitreal injection, she continued to take methazolamide tablets and apply both brinzolamide and brimonidine tartrate eye drops for 1 month to control IOP. She also received panretinal photocoagulation (PRP) at P12W. At P24W, the IOP had decreased to 24 mmHg (NCT), superior corneal and iris neovascularization were reduced, as was corneal edema. The iris neovascularization score decreased from 2 to 1. The images are shown in Fig. 2.

Iris neovascularization regression in Patient 2 with vitreous hemorrhage.
Patient 3 was a 37-year-old man who had lost vision in his right eye more than 10 years earlier, and the initial IOP was 7 mmHg (NCT). Examination revealed mixed congestion, corneal edema, clear anterior chamber, iris neovascularization, and iris pigment loss. B-scan ultrasound examination showed retinal detachment from an earlier date. After injection, the iris neovascularization did not obviously decrease, and the score remained at 1. This patient did not return for his 12-week follow-up examination. He presented again at P24W, and his iris pigment loss was greater than on his previous visit. The IOP measured with Goldman applanation tonometer was 1 mmHg, and images are shown in Fig. 3.
Iris neovascularization in Patient 3 with retinal detachment.
Patient 4 was a 61-year-old woman whose IOP in the right eye was initially 28 mmHg. She complained of no vision in her right eye and severe pain for the past 10 years. Due to poor socioeconomic status, she had been unable to avail herself of surgical treatment. The ophthalmic exam revealed slight atrophy in her right eye, mixed congestion, bullous keratopathy, a clear anterior chamber, marked neovascularization of the iris, lens opacity, and an invisible fundus. The B-scan ultrasound examination showed long-standing retinal detachment. She received an artesunate injection and was prescribed methazolamide tablets, brinzolamide eyedrops, and brimonidine tartrate eyedrops to control her IOP. A nonsteroidal anti-inflammatory drug was prescribed to control inflammation. At P24W, her IOP was 28 mmHg, and the iris neovascularization score had decreased from 4 to 1 (Fig. 4). Unexpectedly, the bullous keratopathy had also decreased, and this improved condition remained at least until P52W.
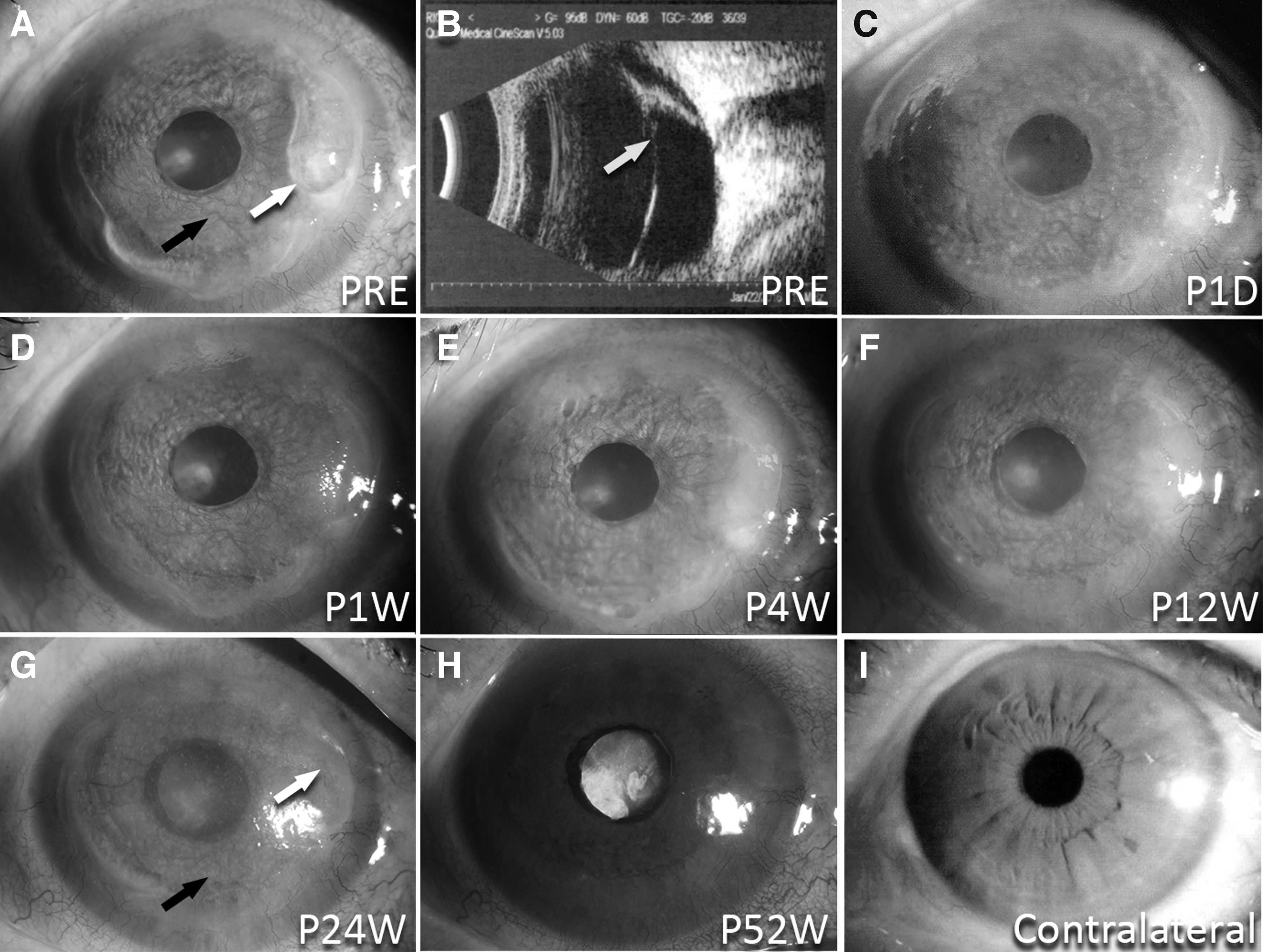
Attenuation of iris neovascularization in Patient 4 with retinal detachment.
In 2 of these 3 patients, iris neovascularization obviously decreased, and the change was very slight only in Patient 3. Considering iris neovascularization was severe in these patients, and they received only 1 injection without alleviation of their etiology, it is tenable that artesunate reduced iris neovascularization.
Attenuation of retinal neovascularization secondary to central retinal vein occlusion
Patient 5 was a 26-year-old woman with central retinal vein occlusion of the right eye, optic atrophy, and neovascularized glaucoma. Her initial IOP was 40 mmHg. Before artesunate injection, she received PRP and methazolamide tablets, brinzolamide eyedrops, and brimonidine tartrate eyedrops to decrease her IOP.
This patient received 2 artesunate intravitreal injections, 1 of which was administered 1 week after her first visit and another 1 month later, as the ophthalmologist found that the therapeutic effect was inadequate. At P24W, OCT revealed obvious papilledema shrinkage, fundus fluorescein angiography showed a decrease in papilledema hyperfluorescence (Fig. 5), and these results remained at P52W. Although she was prescribed IOP-lowering medications, her IOP readings still fluctuated.
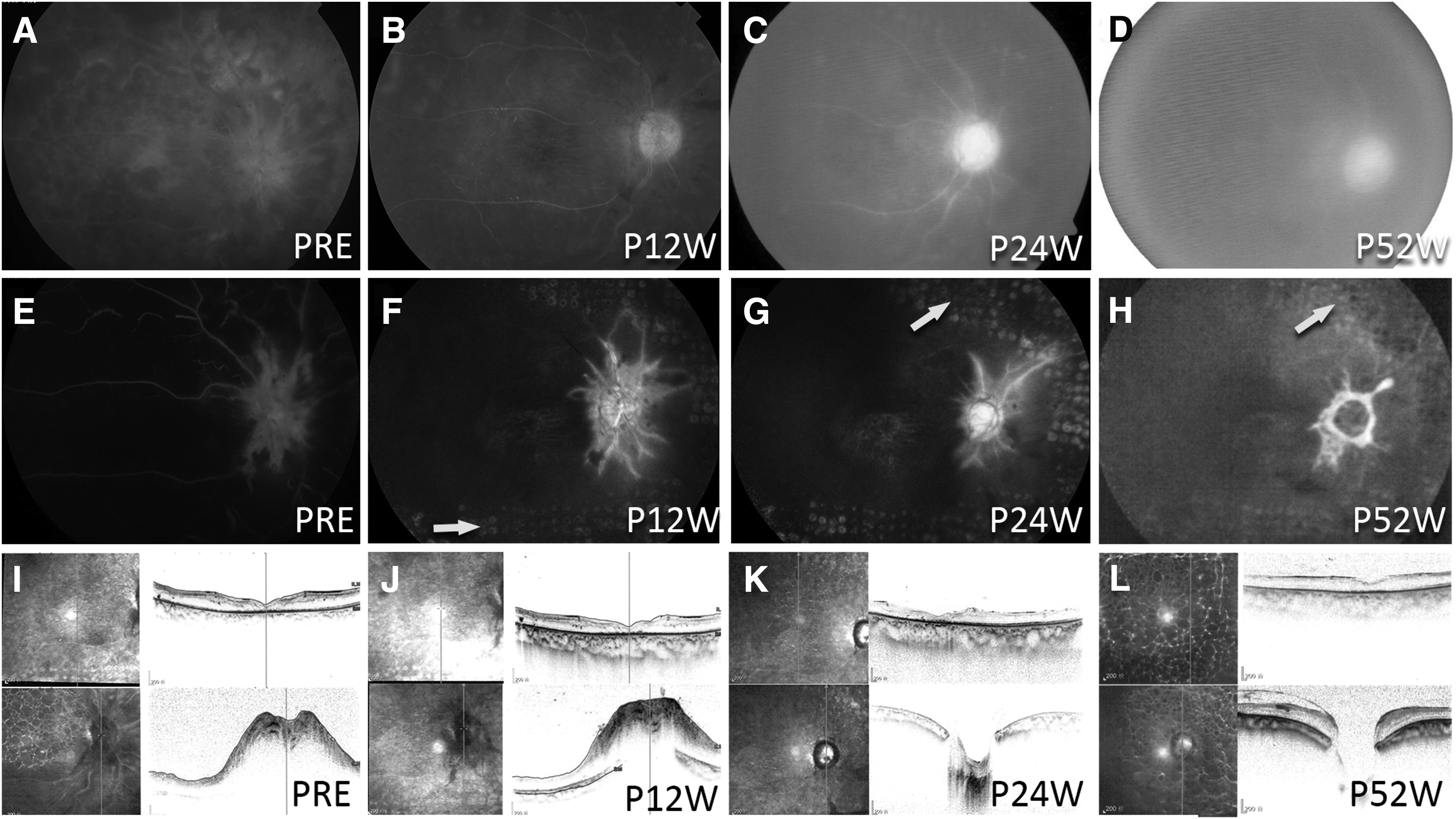
Attenuation of retinal neovascularization secondary to central retinal vein occlusion in Patient 5.
Safety assessment of artesunate intravitreal injection
The dose of intravitreal injection is 1/750 of the systemic intravenous dose. None of the 5 patients, including Patient 5 who received 2 injections, experienced adverse events, such as endophthalmitis, cardiovascular events, or any other systemic reaction. At P24W after injection, the average IOP had decreased from 25.5 to 17.66 mmHg. All IOP readings in the 5 patients are listed in Fig. 6A. On the other hand, after injections, the lenses of Patients 4 and 5 became slightly opaque, whereas the lens transparency of Patient 2 did not show any obvious changes (as shown in Fig. 6B). Considering the patient's primary disease and intraocular conditions, this clinical trial cannot determine a relationship between intravitreal injection of artesunate and the turbidity of the lens, nor can it prove that intravitreal injection of artesunate will not affect the transparency of the lens. Therefore, safety of this intraocular application still needs further research and verification.
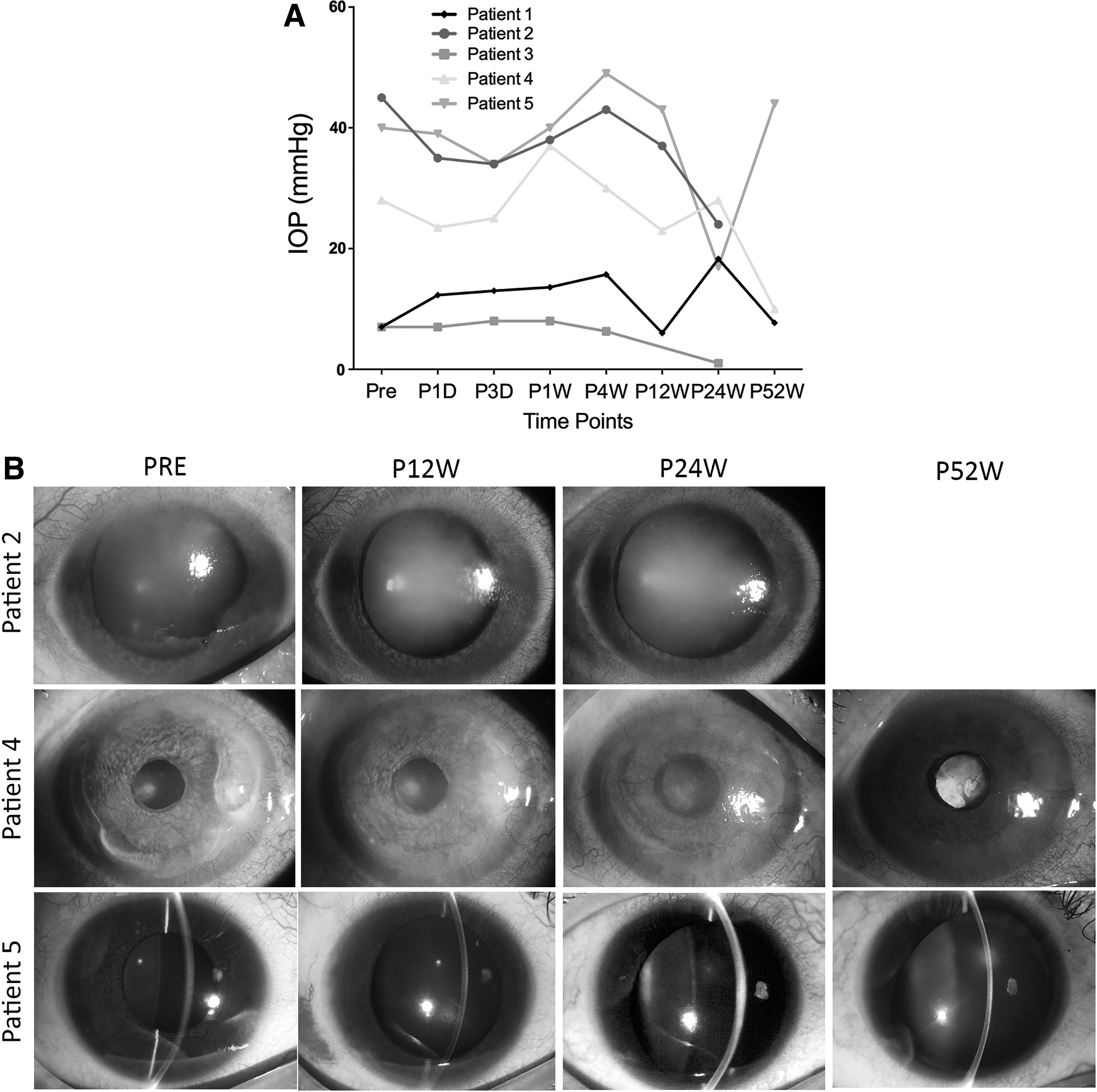
Safety assessment of artesunate intravitreal injection.
The above results preliminarily show that intravitreal injection of artesunate is a relatively effective treatment for intraocular neovascularization.
Discussion
The results of this pilot clinical study showed the preliminary efficacy of artesunate intravitreal injection for the treatment of corneal, iris, and retinal neovascularization. This synthetic drug may provide a new, improved approach to the management of ocular neovascular diseases. It is noteworthy that the 5 subjects included in the study were all at the end stage of various primary diseases, including 3 cases of retinal detachment. Persistent retinal detachment decreases retinal blood flow and causes the ischemic retina to release vasoproliferative cytokines, such as VEGF, which circulate anteriorly into the aqueous humor, provoking neovascularization of iris and cornea.14–16 Vitreous surgery, silicone oil-filled eyes, and chronic intraocular inflammation may be other factors contributing to neovascularization.14,16
Such pathological mechanism of VEGF's mediation of neovascularization is suitable for validating the efficacy of anti-VEGF drugs. At the same time, the end stage of primary diseases usually involves extremely severe angiogenesis, chronic inflammatory reactions, and atrophy, which might reduce the efficacy of drugs and interfere with our safety evaluation. However, since the current treatment for ocular neovascularization diseases has a relatively clear curative effect and supports the interests of patients, we have to recruit patients at the end stage of diseases for this exploratory clinical study. Nevertheless, the results of the clinical study indicate that artesunate had apparent therapeutic effects in most patients for up to 52 weeks after just 2 injections. This may be a result of the lower molecular weight of artesunate, its ability to multitarget, and PKCα's major role in mediating control of proliferative vitreoretinopathy17,18 and tumor generation. 19 Taken together, the results of this pilot study suggest that artesunate is efficacious. It is worth evaluating further with a larger clinical trial that includes appropriate controls and a larger number of patients.
In terms of intraocular safety, no serious adverse systemic events occurred in the 5 patients after 2 injections. The intravitreal injection dose of artesunate is nearly one-thousandth that of the systemically applied intravenous dose, which provides some basis for future evaluations of its systemic safety. In this pilot clinical study, it was observed that patient 1 had progressive turbidity of the cornea and the lenses of patients 4 and 5 were slightly turbid after treatment. Due to the lack of a control group and small sample size, this exploratory study cannot rule out the possibility that corneal and lens turbidity were caused by intravitreal injection of artesunate. However, the long-standing retinal detachment in patient 1 may have caused the observed corneal opacity. Additionally, the lens turbidity of patients 4 and 5 gradually occurred within 1 year after treatment, although the intraocular half-life of artesunate is only 9.82 weeks. Furthermore, intravitreal injection of artesunate did not affect the crystals in animal experiments.20–23 Therefore, further experimental studies are needed to verify the intraocular safety of intravitreally injected artesunate.
Compared with other clinical anti-VEGF trials, the present study had some limitations, including a small number of subjects, lack of a control group, and lack of comparison with conventional treatment strategies. A large-scale randomized controlled trial will be needed to confirm the efficacy and safety of artesunate treatment. In the future, it will also be necessary to identify the most effective and selective therapeutic dosage for use in the eye.
In summary, these clinical results preliminarily illustrate the efficacy of artesunate, indicating that it could have the potential to be developed as a drug for inhibition of neovascular ocular diseases. This study lays the foundation for future research on this topic.
Footnotes
Acknowledgments
This work was supported by the Guangzhou Science and Technology Program key projects (201504010003), the Science and Technology Planning Project of Guangdong Province, China (2015B020211004), and the Medical Scientific Research Foundation of Guangdong Province (A2016291). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the article.
Author Disclosure Statement
No competing financial interests exist.