
Abstract
Abstract
Purpose:
Cannabidiol (CBD), active component of plant Cannabis sativa, has anti-inflammatory properties that could potentially help treat diabetic retinopathy-induced pain and inflammation. However, CBD is a lipophilic molecule making its topical delivery to back of the eye challenging. This study aims at improving ocular penetration of CBD by means of analog derivatization.
Methods:
Analogs were designed using various ligands, such as amino acids (AAs) and dicarboxylic acids (DCAs) and their combinations. Select analogs were screened in vitro with respect to their stability in ocular tissue homogenates. Based on in vitro stability, analogs were selected for in rabbits testing. Formulations containing these compounds were tested in rabbits to determine ocular tissue disposition of CBD and the analogs after topical application. The rabbits were sacrificed 90 min post-topical application and the aqueous humor, vitreous humor (VH), iris–ciliary bodies (IC), and retina–choroid (RC) were analyzed for CBD and analog content.
Results:
CBD–divalinate–dihemisuccinate (CBD-Di-VHS) and CBD–divalinate (CBD-Di-Val) were stable in the ocular tissue homogenates. Post-topical application, CBD and CBD-Di-Val analog levels were detected only in RC. Dosing of CBD-Di-VHS nanoemulsion generated analog levels both in the VH and in the RC, respectively. In contrast, post dosing of CBD–monovalinate–monohemisuccinate (CBD-Mono-VHS), both the analog and CBD were detected in the IC and RC.
Conclusion:
The analogs demonstrated superior penetration into ocular tissues in comparison with CBD. CBD-Di-VHS and CBD-Mono-VHS exhibited better permeation properties, possibly due to improved stability and physicochemical characteristics imparted by AA and DCA combination derivatives.
Introduction
Diabetic retinopathy (DR) demonstrates features of chronic inflammation with signs such as edema and neovascularization, resulting in release of inflammatory mediators, thus requiring intervention with anti-inflammatory therapy. 1 DR is one of the leading causes of vision loss in working-age adults and the fifth most common cause of moderate-to-severe vision impairment.2,3 Studies testing the global prevalence of DR reported 285 million people with diabetes, one-third of whom show symptoms of DR. 4 DR involves leakage of the retinal blood vessels leading to distorted vision. Breakdown of the blood–retinal barrier leads to further vision loss through macular edema and retinal neovascularization.5,6 Degeneration of the retinal cells may be caused by a mechanism involving tyrosine nitration and may include a vascular endothelial growth factor (VEGF)-triggered breakdown component.7,8 Diabetic retinas have shown an increase in the vascular permeability, which can be associated with increase in VEGF and tumor necrosis factor alpha (TNF-α), pointing toward proinflammatory roots of this disease. 9 High-glucose conditions in diabetic retinas stimulate endothelial apoptosis by activation of p38 MAP kinase. 10
Current treatment options for DR include laser photocoagulation, vitreoretinal surgery, and intravitreal injections of anti-VEGF and steroids. Laser photocoagulation is the recommended therapy for DR; however, laser photocoagulation is associated with neural tissue death, raising the need for the development of noninvasive therapies for DR. 11 Intravitreal steroid therapy often leads to unwanted side effects such as elevated intraocular pressure, cataracts, and advent of opportunistic infections.12,13 Ophthalmic surgical procedures such as vitreoretinal surgeries are often accompanied by postsurgical complications such as elevated intraocular pressure, endopthalmitis, and cataract formation. 14
Discoveries pertaining to the involvement of the endocannabinoid system in modulation of ocular pain and inflammation open new avenues for targeting the cannabinoid receptor system (CB1 and CB2) for the management of ocular inflammatory conditions.15,16 CB1 receptors are Gi/o-protein-coupled receptors expressed in the central nervous system (CNS) especially in the basal ganglia, cerebellum, and hippocampus. They are also located in the periphery, including the retina, sperm cells, testis, colonic tissues, and peripheral neurons.17–19 Although CB2 receptors are located in the immune system, there have also been reports of localization of CB2 receptors in the retinal cells.17,20–23
Cannabidiol (CBD) is a major cannabinoid of the plant Cannabis sativa, free of cannabimimetic CNS activity, possessing neuroprotective, antiemetic, and anti-inflammatory properties. 24 Possible explanations for the anti-inflammatory activity of CBD could be its ability to interact with CB2 receptors and inhibiting immune cell migration. 25 Moreover, CBD acts as an effective antioxidant by scavenging reactive oxygen species (ROS) and blocking NADPH oxidase. 6 CBD has been shown to decrease retinal inflammation by blocking ROS and TNF-α formation and by p38 MAP kinase activation. 6 It has also been reported to exert anti-inflammatory activity by inhibiting adenosine reuptake in rat retinal microglial cells. 26 Thus, CBD, by virtue of its anti-inflammatory properties, might be a treatment option for DR-induced pain and inflammation, by modulating the formation of TNF-α and scavenging ROS.
El-Remessy et al. demonstrated neuroprotection in N-methyl-D-aspartate (NMDA)-induced retinal neurotoxicity in rats through the antioxidant effect of CBD. 6 They also determined the effect of blocking oxidative stress on the blood–retinal barrier (BRB) preservation in diabetic rats. 6 The benefits of CBD, that is, blocking oxidative stress and inhibiting adenosine reuptake to enhance a self-defense mechanism against retinal inflammation, potentially represent a novel therapeutic approach for the inflammatory complications of the eye. 26
The cLogP of a compound is a computed value of its partition between water and n-octanol and acts as a measure of its lipophilic character. CBD (Fig. 1A) is a lipophilic molecule with a cLogP of 5.91, making its topical delivery to treat retinal inflammation extremely challenging. For CBD to produce a therapeutic effect, the molecule has to transverse across the static ocular layers and the dynamic blood–ocular barriers to reach the back of the eye.27–29 This study aims at improving ocular penetration of CBD by means of bioengineered analog derivatization. Through structural modifications in the molecule, inherent molecular properties such as molecular size, structural conformation, lipophilicity, and solubility were optimized to increase the “druglikeness” of the molecule.
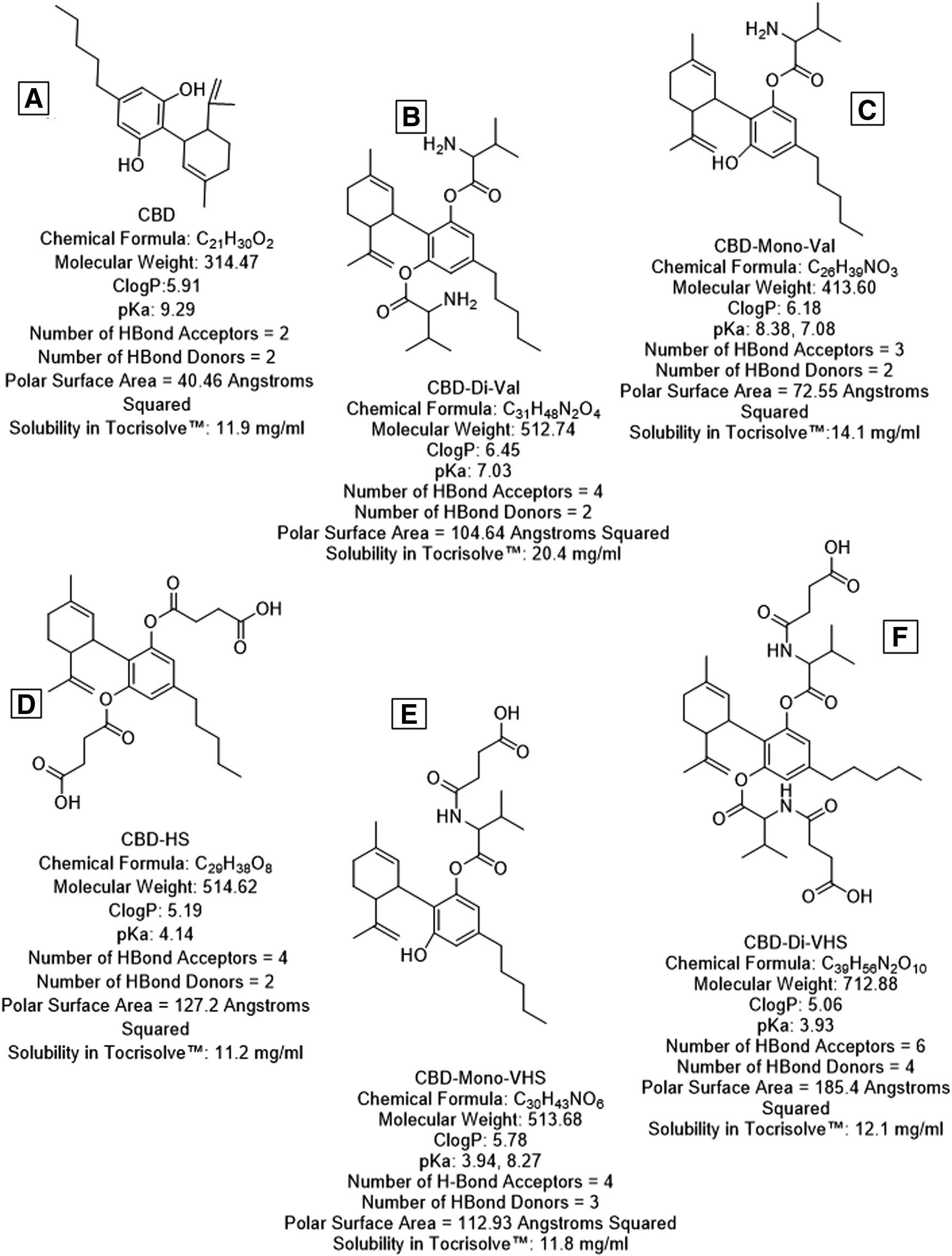
Structures, chemical formulae, and physicochemical parameters of CBD (cannabidiol) and biologically active CBD analogs.
CBD–amino acid ester (CBD-AA) analogs are prepared by linking both or one of its hydroxyl groups to an AA such as
Methods
CBD analogs were synthesized by ElSohly Labs, Inc., 36 Tocrisolve™ was purchased from Tocris® Bioscience, Bristol, United Kingdom. High performance liquid chromatography (HPLC)-grade solvents and other chemicals (analytical grade) were obtained from Fisher Scientific (Hampton, NH).
Animals
Male New Zealand white (NZW) rabbits (2–2.5 kg), obtained from Harlan laboratories® (Indianapolis, IN), were used in all studies. All animal experiments conformed to the tenets of the Association for Research in Vision and Ophthalmology statement on the use of animals in ophthalmic and vision research. All experiments followed the University of Mississippi Institutional Animal Care and Use Committee approved protocols.
Synthesis of analogs
CBD derivatives were prepared using the procedures described previously (US20190031601A1). 36 The final products were purified using column chromatography and characterized by mass spectroscopy in the positive ionization mode.
Stability of CBD and analogs in ocular tissue homogenates
Tissue preparation
The degradation of CBD analogs was determined in aqueous humor (AH), vitreous humor (VH), iris–ciliary bodies (IC), and retina–choroid (RC). The tissues were shipped on dry ice from Pel-Freez Biologicals; AR. Ice-cold isotonic phosphate buffer saline (IPBS) was used to homogenize the solid tissues, RC and IC, in an ice bath using a TISSUEMISER (Fisher Scientific). The homogenates were then centrifuged at 17,000 g at 4°C for 15 min. The protein contents of the supernatants were determined according to the method of Bradford and were adjusted to ∼1 mg/mL. 37
Hydrolysis procedure
Enzymatic degradation of CBD and analogs was studied at 37°C in a shaking water bath. The tissue homogenates were equilibrated for 30 min at 37°C to activate the enzymes. To 1.9 mL of the supernatant, 100 μL of the CBD/analog stock solution was added to make the final CBD/analog concentration as 25 μg/mL (analog concentration spiked for CBD-di-Val was 50 μg/mL). At predetermined time points, 100 μL aliquots of the sample were withdrawn up to 6 h post initiation. An equal volume of ice-cold acetonitrile was added to each sample to arrest the enzymatic degradation. The samples were centrifuged at 17,000 g for 15 min and the supernatant was analyzed for analog/CBD content using HPLC–Ultraviolet (UV).
Chromatography methods
Analytical method for in vitro samples
The in vitro samples were analyzed for CBD and analogs using an HPLC–UV system comprising a Waters 717 plus auto sampler, Waters 600E pump controller, Waters 2487 dual λ absorbance detector, and an Agilent 3395 integrator. Stock solutions of CBD and analogs were prepared in acetonitrile. A gradient method (Table 1) was used for elution of CBD and analogs with the mobile phase consisting of acetonitrile and 5 mM phosphate buffer (pH 2.5). A Phenomenex® C18 (4.6 × 150 mm) column was used at a flow rate of 1 mL/min. Detection was carried out at 222 nm.
High-Performance Liquid Chromatography Gradient Method for Separation and Quantification of Cannabidiol and Analogs
Preparation of topical ophthalmic nanoemulsion of CBD/analogs
CBD and the associated analogs were formulated into a soybean oil-based nanoemulsion composed of a 1:4 ratio of soya oil–water that was emulsified with the block copolymer Pluronic F68 (Tocrisolve). The formulations were prepared by adding the drug/analog to the blank emulsion. This mixture was vortexed for 5 min followed by sonication for 10 min. For quantification of CBD and analogs in the nanoemulsion, the formulations were centrifuged at 8,000 g for 5 min at 25°C. The solubility of CBD and the analogs is shown in Fig. 1.
Distribution of CBD and analogs in ocular tissues after topical administration
In vivo bioavailability of CBD and analogs was determined in male NZW rabbits, weighing between 2 and 2.5 kg, procured from Charles River Labs. CBD and its analogs, namely CBD-Di-VHS, CBD-Di-Val, CBD-Mono-Val, CBD-Mono-VHS, and CBD-HS were formulated in Tocrisolve emulsion. These formulations were evaluated in vivo in a conscious rabbit model, at least in triplicates (n = 3). The initial study compared ocular penetration of CBD-Di-VHS and CBD-Di-Val with that of CBD. The second study compared the ocular bioavailability of CBD-Mono-Val, CBD-Mono-VHS, CBD-HS, and CBD. Concentration of the CBD analog as well as CBD was determined in the AH, VH, RC, and IC. Fifty microliters of the mentioned formulations were dosed topically (dose: 250 μg CBD equivalent)—instilled in the conjunctival sac of the NZW rabbits. Ninety minutes after dosing, the rabbits were anesthetized using a combination of ketamine (35 mg/kg) and xylazine (3.5 mg/kg) injected intramuscularly. The rabbits were euthanized with an overdose of pentobarbital injected through the marginal ear vein. The eyes of the rabbits were then enucleated and washed thoroughly with IPBS and the intraocular tissues such as IC, AH, and VH were separated.
Tissue sample preparation and extractions
A protein precipitation technique was employed to determine the amount of CBD and analogs in the ocular tissue homogenates. The solid tissues, namely IC (50 mg) and RC (30 mg), were cut into small pieces and homogenized with ice-cold IPBS in an ice bath using a TISSUEMISER (Fisher Scientific), whereas the liquid tissues, AH (50 μL) and VH (100 μL), were taken as they were. For the calibrators, standards were prepared by spiking the tissues with CBD and the analogs to yield final concentrations of 2.5, 5, 10, 25, 50, and 100 ng/mL. Twenty-five microliters ice-cold acetonitrile was then added to the samples/calibrators, precipitating proteins from individual tissues. Samples were vortexed and kept aside for 10 min. The supernatant was collected after centrifuging for 30 min at 17,000 g and analyzed using liquid chromatography tandem mass spectrometry (LC-MS/MS).
Bioanalytical quantification method
Analysis was performed on two LC-MS-MS systems consisting of a Shimadzu Prominence HPLC with a dual pump, a vacuum solvent microdegasser, a temperature-controlled autosampler, and an MS-MS detector (Applied Biosystems/MSD Sciex Qtrap 3200 and 4500 with a turboion electrospray ionization (ESI) source operating the positive-ion multiple reaction monitoring, or MRM, mode). Specific MRM transitions were monitored for each compound for maximum selectivity and sensitivity. Separation was achieved on a Synergi Hydro-RP column (50 × 3.00 mm; 2.5 μm; 100 Å) from Phenomenex (Torrance, CA). Water with 0.1% formic acid (Pump A) and acetonitrile with 0.1% formic acid (Pump B) were used as the mobile phase with a gradient elution. Data acquisition and processing were performed with Analyst™ 1.6.2 software (Applied Biosystems [AB Sciex], Foster City, CA).
Statistical analyses
Data are represented as the mean ± standard deviation, for a minimum of 3 independent experimental runs. Statistical comparisons of the means were performed using one-way analysis of variance or Student's t-test. The differences were considered significant when the P value was <0.05.
Results
Stability of CBD and analogs in ocular tissue homogenates
Stability of CBD in ocular tissue homogenates
The stability of CBD in the biological matrix and its resistance to enzymatic attack are shown in Table 2. CBD was stable in most of the ocular tissues tested. Some degradation is observed in the IC.
Stability of Cannabidiol in Ocular Tissue/Tissue Homogenates
CBD, cannabidiol
Stability of CBD-Di-Val in ocular tissue homogenates
The results (Fig. 2) suggest that CBD-Di-Val is enzymatically hydrolyzed in some of the ocular tissues with detectable levels of CBD observed 90 min post initiation of the study. The half-life of CBD-Di-Val in AH and VH was 5.78 and 2.89 h, respectively, with apparent first-order degradation rate constants of 0.33 × 10–4 h−1 and 0.67 × 10–4 h−1. In the solid tissues, IC and RC, we observe restricted formation of CBD over the period of 360 min. In the IC, we observe a gradual drop in analog concentrations, from 27.7 ± 0.96 nM at 0 min to 7.66 ± 1.1 nM at 90 min, with levels dropping further past the 90 min time point.

In vitro enzymatic stability of CBD-Di-Val in ocular tissue homogenates; AH, VH, RC, and IC. The blue bars represent CBD-Di-Val concentrations (nM) and the red bars represent regenerated CBD (nM) concentrations. AH, aqueous humor; CBD-Di-Val, CBD–divalinate; IC, iris–ciliary bodies; RC, retina–choroid; VH, vitreous humor. Color images are available online.
Stability of CBD-HS in ocular tissue homogenates
CBD-HS, like CBD-Di-Val, is enzymatically hydrolyzed in some of the ocular tissues (Fig. 3). The half-life of CBD-HS in AH and VH was 13.07 and 13.52 min, respectively, with apparent first-order degradation rate constants of 0.053 and 0.051 min−1, respectively. The half-life of CBD-HS in IC was 16.5 min and the apparent first-order degradation rate constant was 0.042 min−1. We observe regeneration of CBD in AH, VH, and RC at the 60, 120, and 120 min time point, respectively.
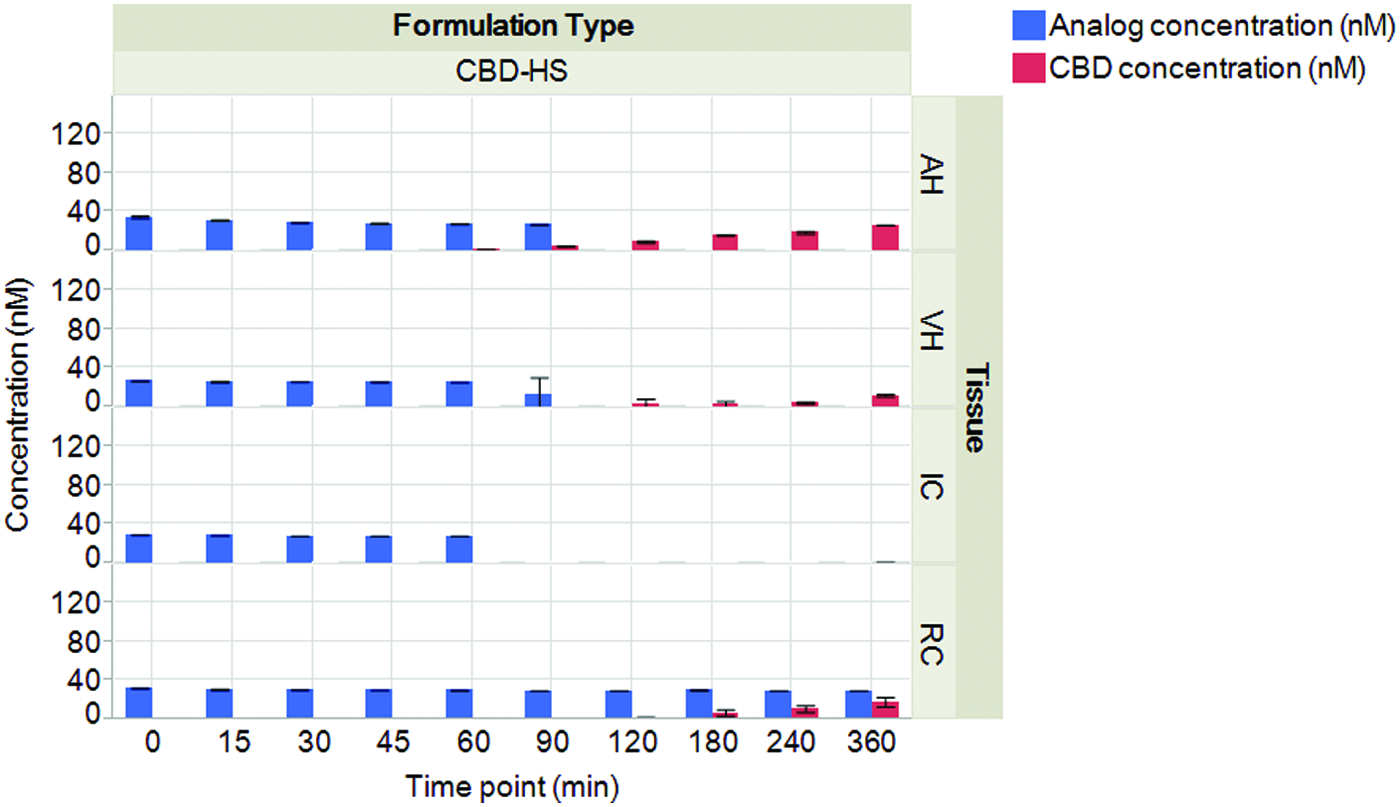
In vitro enzymatic stability of CBD-HS in ocular tissue homogenates; AH, VH, RC, and IC. The blue bars represent CBD-HS concentrations (nM) and the red bars represent regenerated CBD (nM) concentrations. Color images are available online.
Stability of CBD-Di-VHS in ocular tissue homogenates
CBD-Di-VHS demonstrates excellent stability in the ocular tissues without any CBD generation even after a 6 h exposure (Fig. 4). We observe 34 ± 0.47, 30.1 ± 4.38, 36.3 ± 0.08, and 35.8 ± 1.49 nM of the analog at the 0 time point in tissues AH, VH, IC, and RC, respectively, and steady analog concentrations thereafter.

In vitro enzymatic stability of CBD-Di-VHS in ocular tissue homogenates; AH, VH, RC, and IC. The blue bars represent CBD-Di-VHS concentrations (nM) and the red bars represent regenerated CBD (nM) concentrations. CBD-Di-VHS, CBD–divalinate–dihemisuccinate. Color images are available online.
Distribution of CBD and analogs in ocular tissues after topical administration
First pharmacokinetic study
Fifty microliters of 3 formulations was dosed in the first study, CBD, CBD-Di-Val, and CBD-Di-VHS (n = 6) in Tocrisolve emulsion in NZW rabbits (n = 3), with the dose being equivalent to 250 μg CBD (Fig. 5). CBD, from CBD formulations, did not penetrate across the ocular tissues after topical instillation, with CBD being detected only in the RC tissues (17.35 ± 4.57 ng/g). CBD-Di-Val did not permeate significantly into the ocular tissues with ∼9.11 ± 1.07 ng/g of the analog (equivalent to ng/g of CBD) being detected in the RC only. CBD-Di-VHS concentration was 612.48 ± 187.11 ng/mL (detected in 3 of the 6 test animals) in the VH and 279.77 ± 75.29 ng/g tissue weight in the RC. Concentrations in the front of the eye tissues were lower with 12.32 ± 7.53 ng/mL in the AH and 160.31 ng/g tissue weight in the IC (detected in IC of only 1 animal).
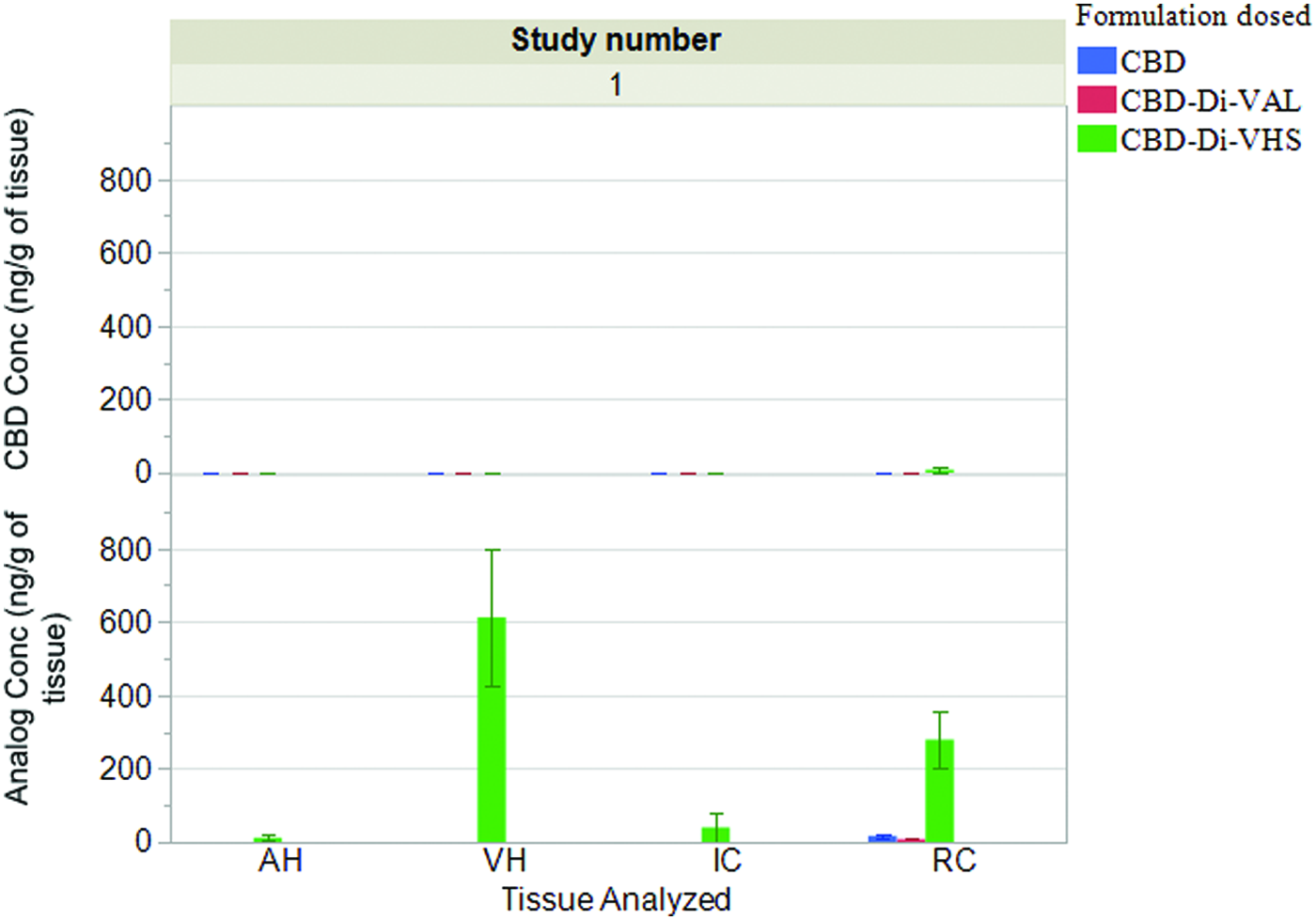
Ocular tissue concentrations of CBD, CBD-Di-Val, and CBD-Di-VHS 90 min post-topical application of CBD (0.47%), CBD-Di-Val (0.94%), or CBD-Di-VHS (1.2%) in Tocrisolve™ emulsion (dose: 250 μg CBD; 50 μL instilled volume), respectively. Data represented are mean ± SEM. SEM, standard error of the mean. Color images are available online.
Second PK study
Fifty microliters of the 4 formulations was dosed in the second study: CBD, CBD-Mono-Val, CBD-Mono-VHS (n = 6), and CBD-HS in Tocrisolve emulsion in NZW rabbits (n = 3), with the dose being equivalent to 250 μg CBD (Fig. 6). After topical administration of CBD-HS, the analog concentrations were below detection levels in all the ocular tissues tested at the end of 90 min; however, bioreversed CBD, 263.15 ± 93.33 ng/g tissue weight in RC and 266.69 ± 35.52 ng/g in IC, was observed, consistent with the in vitro stability profile. CBD-Mono-VHS, in contrast, showed significantly higher levels of the analog in IC (728.18 ± 152.62 ng/g) and RC (603.92 ± 160.42 ng/g tissue weight), in comparison with CBD-HS and CBD-Mono-Val (Fig. 6). We also observe bioconverted CBD, after topical application of CBD-mono-VHS formulations, in RC (348.37 ± 131.17 ng/g), IC (469.09 ± 62.78 ng/g), and AH (30.66 ± 13.84 ng/mL). We did not observe any analog or CBD levels post dosing with CBD and CBD-Mono-Val.

Ocular tissue concentrations of CBD-Mono-VHS, CBD-Mono-Val, CBD, CBD-HS 90 min post-topical application in Tocrisolve emulsion (dose: 250 μg; 50 μL instilled volume), respectively. Data represented are mean ± SEM, the differences were considered significant when the P value was <0.05. *CBD-Mono-VHS >CBD, CBD-HS, CBD-Mono-Val. **CBD-HS > CBD, and CBD-Mono-Val. CBD-Mono-VHS, CBD–monovalinate–monohemisuccinate. Color images are available online.
Discussion
CBD was derivatized to generate CBD analogs to improve aqueous solubility and tissue permeability: the aim of analog design was to modify molecular properties in the desired direction. Physicochemical parameters such as molecular weight, Log P, pKa, hydrogen bond donors and acceptors, and polar surface area were estimated using the ChemDraw software (PerkinElmer®) to obtain a better understanding of the membrane permeation characteristics of the molecule. Figure 1 lists the computed physicochemical parameters for CBD and analogs. Optimum physicochemical parameters would, in turn, prove to be efficient predictors of overall ocular bioavailability. The rule of 5 (RO5) defined by Lipinski determines limitations for drug design for an oral-targeted molecule to be successful through all the stages of drug development (molecular weight 500, Log P 5, H-bond donors 5, H-bond acceptors 10). With a few modifications, we can utilize the Lipinski's RO5 in designing molecules for nonoral routes of delivery.38,39
Comparing the stability of CBD analogs in an in vitro setup, we observed delayed and restricted generation of CBD (Fig. 2) from CBD-Di-Val, which could be explained by possible formation of intermediate degradation products such as CBD-Mono-Val. AA derivatives synthesized with promoeties such as valine, isoleucine, and phenylalanine have been reported to provide stability to hydrolytic attack in comparison with the DCA analogs due to the presence of steric groups such as branched aliphatic AA (valine) or aromatic AA (phenylalanine).40–43 CBD-Di-Val is a lipophilic molecule with a cLogP of 6.45 (Fig. 1B), and shows limited dissolution in the homogenized tissues. Figure 2 depicts low initial concentrations of CBD-Di-Val followed by a slight increase and steady analog concentrations through the duration of the study. This behavior could be attributed to the drug concentrations exceeding equilibrium solubility in the biological matrices, leading to possible precipitation of the analog followed by continual dissolution of the same in the tissue matrix, leading to an equilibrium between the drug in solution and undissolved drug. In solid tissues, IC and RC, no CBD as a breakdown product was observed. However, a decline in the analog levels was detected. This could again be attributed to generation of intermediate degradation products and the resistance of the analog to hydrolytic attack.
Looking at stability of CBD-HS in ocular tissue homogenates (Fig. 3), the AH, VH, and IC data show constant analog levels initially with a sudden drop below detection levels hinting toward solubility issues of the analog and the stability of ester bond governing the overall rate of the reaction, with it changing from pseudozero to first-order degradation process. The delayed generation of CBD suggests formation of an intermediate degradation product, like CBD-Mono-HS, before generating CBD or a different degradation pathway. The observed bioconversion in IC was similar to the results for bioconversion of CBD-Di-Val in IC; CBD-HS failed to regenerate CBD through the duration of the study. We can attribute this phenomenon to secondary degradation products formed due to the presence of multiple sites for hydrolytic attack and presence of unexplored degradation pathways. The results in RC point toward formation of an initial supersaturated solution followed by precipitation and generation of an equilibrium between the solid state and solution state as evidenced by the CBD-HS levels remaining almost constant even though generation of CBD is observed 2 h postinitiation.34,43
Out of all the analogs tested, CBD-Di-VHS was observed to be the most stable, with no degradation within the study duration, whereas CBD-Di-Val and CBD-HS regenerated CBD but at a slow rate. This finding points to the increased chain length of CBD-Di-VHS, leading to steric hindrance, in turn, providing greater protection from enzyme attack. Moreover, the number of intermediates that can form is double than that with CBD-Di-Val and CBD-HS. The in vitro data point toward the solubility of the analogs, the stability of the ester bond, involvement of different degradation pathways, and formation of multiple degradation intermediates as a possible explanation for the low rate of bioconversion observed in the biological matrices of the analogs and generation of CBD.
CBD, from CBD formulations, did not penetrate across the ocular tissues after topical instillation. This indicates that CBD, because of its physicochemical characteristics, is not suited for penetration across the ocular membranes. CBD-Di-Val formulations demonstrated poor permeation and were detected in the RC only. A potential explanation for this phenomenon could be that CBD-Di-Val, being slightly more hydrophobic than the other analogs, displays poor solubility in the tissue environment at physiological pH. In comparison with CBD, CBD-Di-Val is more lipophilic (cLogP 6.45) and is a bulkier molecule, resulting in overall lower bioavailability than the parent molecule. Because of its lipophilic nature and high solubility in the oily emulsion (Fig. 1B), its dissolution in the tissue microenvironment serves as a rate-limiting step, preventing the molecule from partitioning into the hydrophilic tear fluid. CBD-Di-VHS (Fig. 1F) has a pKa of 3.93, and is charged at physiological pH, resulting in higher solubility of the analog, in turn, increasing its partitioning into the tear and permeation. CBD-Di-VHS was not metabolized to CBD in the ocular tissues within the timeframe tested. This observation was consistent with the in vitro stability data in the tissue homogenates. The analog demonstrated surprisingly high penetration into the VH. The charge of the analog at physiological pH and the route of ocular permeation could possibly explain penetration of the analog from the RC into the VH. However, the overall tissue disposition profile of CBD and the analogs, from the nanoemulsion formulations, suggests a noncorneal route of absorption, with higher levels of the analogs present in the posterior tissues.
Taking into consideration the in vitro and in vivo data of CBD, CBD-Di-Val, and CBD-Di-VHS, monoderivatized AA and AA-DCA analogs of CBD (CBD-Mono-VHS, CBD-Mono-Val) were synthesized for in vivo evaluation, aiming to reduce the steric bulk of the molecule but retaining the overall permeation/stability profile offered by AA and AA-DCA analogs.
Comparing the data obtained in both sets, after CBD administration, lower levels of CBD were observed in the RC in the first study; however, the difference in the drug concentrations detected was not statistically significant and this variation could be attributed to biological system variability. CBD-HS (Fig. 1D), being a DCA analog, has 2 ester bonds prone to hydrolysis, rendering it susceptible to chemical and enzymatic hydrolysis. CBD-Mono-Val is a hydrophobic molecule with a cLogP value of 6.18 (Fig. 1C). The lipophilic nature as well as other physicochemical characteristics of the molecule along with restricted solubility in the tissue microenvironment results in low ocular bioavailability (below detection limit in all tissues tested) as observed in the in vivo study. The in vivo studies suggest that the monoderivatized form, CBD-Mono-VHS, permeates more effectively than CBD-Di-VHS, with higher concentrations of the analog detected in the tissues. CBD-Mono-VHS levels are almost 2 times, 4 times, and 8 times higher in RC, IC, and AH (Fig. 6), respectively, in comparison with CBD-Di-VHS (Fig. 5) along with bioconversion to parent molecule. Looking at the ocular bioavailability in relation to drug design, several features about the physicochemical properties of the molecule stand out (Fig. 1E): CBD-Mono-VHS is a smaller molecule (MW 513.68) than CBD-Di-VHS (MW 712.88) and has 1 charged group at physiological pH, balancing its hydrophilic and lipophilic nature. The transmembrane permeation of CBD-Mono-VHS, which has a PSA of 112.93 A2, is comparatively more effective than that of CBD-Di-VHS, a more polar molecule with a PSA of 185.4 A 2 . Looking at the total number of hydrogen bond donors and acceptors (Fig. 1E), even though both molecules follow Lipinski's RO5, CBD-Mono-VHS displays a better profile due to a lower number of donors and acceptors, giving it a comparatively better Absorption Distribution Metabolism Excretion profile.
Conclusion
The mentioned results demonstrate that CBD displays poor ocular tissue permeation after topical application. When analogs are designed with a natural AA modification (eg, CBD-Di-Val) or as a DCA ester (eg, CBD-HS), penetration into the ocular tissues is not adequate. A combination of an AA and DCA (eg, CBD-Di-VHS) strikes an effective balance between the hydrophilicity and lipophilicity and other physicochemical characteristics, effectively increasing ocular bioavailability.
CBD-mono-AA analogs, wherein one of the hydroxy groups is derivatized as a valine ester and the other hydroxyl group is unsubstituted, do not penetrate the ocular tissues. In contrast, when one of the hydroxyl groups is derivatized with a valine–hemisuccinate moiety and the other hydroxyl group is free (CBD-Mono-VHS), ocular bioavailability after topical application is significantly enhanced. The results suggest that the free COOH group and stability of the linkage play an important role in the penetration across the ocular tissues. Among all the derivatives studied, the AA-DCA analog possessed optimum physicochemical properties, permeating effectively across ocular barriers.
Footnotes
Acknowledgment
This research was supported, in part, by a research grant from Nemus Bioscience, Inc.
Author Disclosure Statement
This research is sponsored by Nemus Bioscience and may lead to the development of products from which W.G., M.E., and S.M. may receive income as part of licensing fees and royalties paid to the University of Mississippi. M.E. is a scientific advisor to Nemus Bioscience. No competing financial interests exist for the other authors, that is, P.T., G.A., A.P., P.L., and E.A.