
Abstract
Abstract
Purpose:
To compare management of postoperative pain after corneal collagen crosslinking (CXL) with oral gabapentin or ketorolac.
Methods:
Prospective interventional comparative case series in a single center. Patients undergoing epithelium-off (epi-off) or epithelium-on (epi-on) techniques performed by a single surgeon for progressive keratoconus were enrolled and randomly assigned to the ketorolac (10-mg tablets every 8 h) or the gabapentin (300-mg capsules every 8 h) group and instructed to take the medication for the first 3 postoperative days. Using a numeric scale of pain, scores were assessed for current pain (at the time of applying the questionnaire), and average pain over the preceding 24 h. Eye symptoms and systemic adverse events related to oral medication were also assessed.
Results:
Thirty-seven patients were included, with 22 (10 epi-on and 12 epi-off) assigned to the ketorolac group and 15 (7 epi-on and 8 epi-off) to the gabapentin group. No statistically significant differences were noted on the pain scale between groups at any point of the study, in the median pain scores of patients at the time of applying the questionnaire, nor in the severity of pain during the 24-h period before the assessment. Also, no differences were found among groups for the eye symptoms and the systemic adverse events. The median regression analysis showed no effect of the type of surgery or gender in the severity of pain.
Conclusions:
Both oral ketorolac and oral gabapentin can be used with similar results for pain and symptomatic control after epi-on or epi-off CXL procedures.
Introduction
Keratoconus is a noninflammatory disorder of unknown etiology; it is characterized by progressive thinning and cone-shaped protrusion of the cornea. 1 As keratoconus progresses, patients experience difficulties with their spectacle correction and contact lens fitting, leading to diminished vision and corneal scarring with 10%–20% of cases eventually requiring a corneal transplant.2,3
In 2003, Wollensak et al. introduced the corneal collagen crosslinking (CXL) as a new therapy to halt the progression of keratoconus, combining riboflavin and ultraviolet-A (UVA) to increase the corneal biomechanical stiffness.4,5 Since then, multiple studies have been published to evaluate the outcomes of different protocol variations. The “original” Dresden protocol is still the gold standard as it is the more studied, and there is no consensus at this moment among other protocols.
The cornea is the most densely innervated tissue in the body. The majority (∼70%) of sensory afferent fibers are polymodal nociceptors activated by mechanical forces, exogenous chemical irritants, endogenous chemical mediators, abnormal temperature, and only 20% are pure mechanoreceptors. 6 Intense pain after surface refractive surgery is attributable to enhanced spontaneous activity of injured nerve fibers and inflammatory molecules released that stimulate afferent nerve endings. 7
Postoperative pain and discomfort remain major issues and are attributed mainly to the epithelial debridement in the epithelium-off (epi-off) technique; however, pain is also present without removal of the epithelium in the epithelium-on (epi-on) technique, caused by the photochemical damage to subepithelial nerve plexus.8–10
Oral gabapentin and ketorolac are 2 medications commonly used in corneal refractive surgery surface procedures, and with extensive clinical studies regarding safety and effectivity. Therefore, we performed this study to compare management of postoperative pain after CXL with both medications.
Methods
This is a prospective interventional comparative case series. The Institutional Review Board and the ethics committee approved this study, which was performed in accordance with the tenets of the Declaration of Helsinki.
Patients enrolled in the study were randomly assigned to the ketorolac or the gabapentin group. The gabapentin (Neurontin, Pfizer, Mexico) group was instructed to take one 300-mg capsule the night before surgery, 1 capsule every 8 h on the day of surgery and for the first 3 postoperative days. The ketorolac group (Dolac; Siegfried Rhein, Mexico) was instructed to take their 10-mg tablets every 8 h on the day of surgery and for the first 3 postoperative days.
We included patients with keratoconus grades 2 or 3, older than 18 years with documented bilateral progression by corneal tomography in the previous 6–12 months, defined as an increase of 1 diopter or more in the Kmax value. Exclusion criteria were previous ocular or systemic diseases that could potentially affect corneal wound healing (eg, diabetes mellitus, collagen vascular disease); use of topical or systemic nonsteroidal anti-inflammatory drugs (NSAIDs); or chronic use of any other pain medication, pregnancy, and allergy to the drugs of the study. All patients suspended the use of rigid contact lenses 1 month before surgery.
Crosslinking
Epi-off CXL was performed on patients with minimum corneal thickness greater or equal to 400μm on corneal tomography (Sirius; CSO, Italy). Topical anesthesia was achieved with tetracaine (Ponti; Sophia Laboratories, Guadalajara, Mexico) 1 drop before the procedure. After inserting the eyelid speculum, 20% ethanol was applied in a 9-mm diameter on the corneal surface for 30 s and rinsed with balanced saline. The corneal epithelium then was removed with a blunt spatula. The accelerated crosslinking protocol was used, which entails a 10-min soak time with isotonic riboflavin 0.1% and hydroxypropylmethylcellulose solution, and 4 min of exposure with 30 mw/cm2 UVA irradiation for a total energy of 5.4 mJ/cm2.
Epi-on CXL was performed on patients with minimum corneal thickness <400 μm on corneal tomography (Sirius; CSO). Topical anesthesia was achieved with tetracaine (Ponti; Sophia Laboratories) 1 drop before the procedure. After inserting the eyelid speculum, 2 to 4 drops of hypotonic riboflavin 0.25% solution, composed by benzalkonium chloride, EDTA, trometamol, hydroxypropylmethylcellulose, and phosphate buffered saline. Paracel (Avedro, Waltham, MA) was applied to coat the cornea, and an additional drop was applied every 30 s for a total soak of 4 min. The cornea was completely rinsed with 0.25% riboflavin and saline (Vibex Xtra; Avedro), applying an additional drop every 30 s for a total of 6 min. UVA irradiation was performed for 2 min and 40 s at 45 mw/cm2, for a total energy of 7.2 mJ/cm2.
For both epi-on and epi-off procedures, after UVA exposure, the eye was rinsed with balanced salt solution. Often, epi-on CXL may also exhibit corneal epithelial breakdown. For that reason, in all CXL patients, a silicone hydrogel bandage contact lens (PureVision2; Bausch + Lomb) was placed and maintained for 5 days until total re-epithelialization. Gatifloxacin with prednisolone acetate 1% ophthalmic suspension (Zypred; Allergan, Irvine, CA) was prescribed 4 times a day for 1 week. Nonpreserved artificial tears (Optive; Allergan) were also prescribed 4 to 8 times a day for 7 days.
Numeric pain scale questionnaire
Using a numeric scale of pain, patients were asked to state their pain intensity on a scale of 0–10, explaining the patient that a 0 represents no pain at all and 10 represents severe and incapacitating pain. The questionnaire was applied 2 h after surgery and at postoperative days 1–5. Pain scores were assessed for current pain (at the time of applying the questionnaire) and average pain over the preceding 24 h. Patients were asked to rate the severity of 4 different symptoms during the 24-h period before follow-up: tearing, light sensitivity, foreign body sensation, and discomfort/irritation. The last 4 items on the questionnaire were related to systemic adverse events related to oral medication, specifically dizziness, drowsiness, headaches, and gastrointestinal symptoms. A single blind investigator for treatment (OS-C) performed all questionnaires.
Statistical analysis was performed using Stata 13.1 (Stata Corp, College Station, TX). Outcomes between groups were compared using Wilcoxon rank-sum (Mann–Whitney) test. Comparisons before and after treatment in the same group were performed with a paired t-test. A median regression was performed to estimate the effect of covariates on severity of pain, with significance considered when P < 0.05.
Results
Thirty-seven patients were included in this study: there were 20 men and 17 women. Twenty-two patients were assigned to the ketorolac group and 15 to the gabapentin group. The median age of the entire group was 24 years (range 18–41 years). The median age of the subgroup of ketorolac was 23.5 years (range 18–41 years) and that of the gabapentin group was 24 years (range 18–30 years). The distribution of the epi-on and epi-off CXL procedures was as follows: gabapentin group, 7 epi-on and 8 epi-off; ketorolac group, 10 epi-on and 12 epi-off.
Figure 1 shows the median pain scores of patients at the time of applying the questionnaire. Pain significantly decreased from immediate postoperative period (2 h) to 1 day post-CXL, from days 1 to 2, and from days 2 to 3. No statistically significant differences were noted on the pain scale between groups at any point of the study, from the immediate postoperative period (P = 0.82) onward day 1 (P = 0.94), day 2 (P = 0.35), day 3 (P = 0.60), day 4 (P = 0.28), and day 5 (P = 0.22).
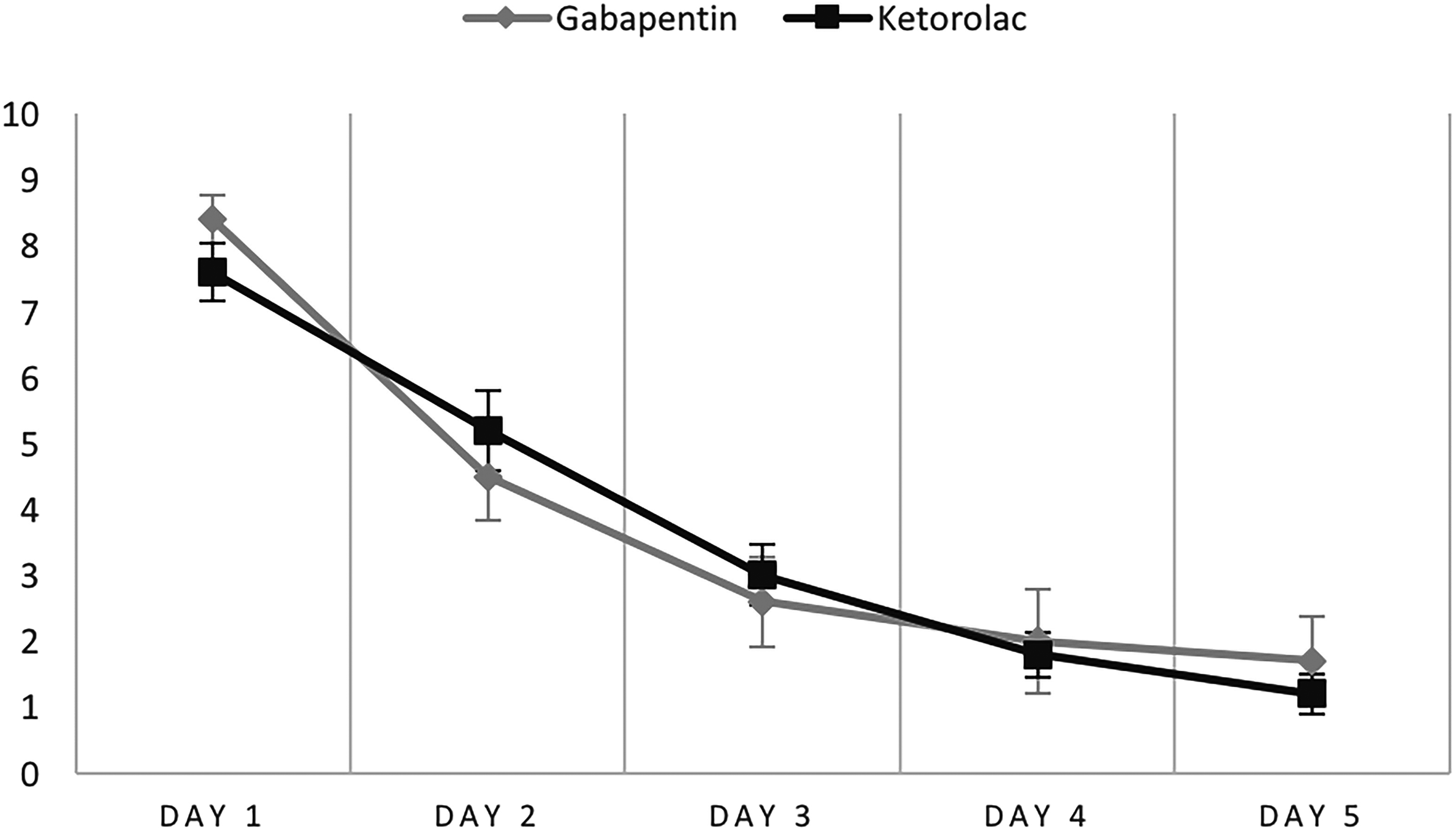
Mean ± standard deviation scores of patients regarding the question about current (at the time of questioning) pain at follow-up.
Patients were asked to rate the severity of pain during the 24-h period before the assessment; the median scores are presented in Fig. 2. In both gabapentin and ketorolac groups analyzed individually, cumulative pain scale scores significantly decreased from days 1 to 2 and from days 2 to 3. Only in the ketorolac group, there was also a decrease of pain scores from days 3 to 4 and from days 4 to 5. In addition, no statistically significant differences were noted between groups at any postoperative follow-up: day 1 (P = 0.33), day 2 (P = 0.47), day 3 (P = 0.38), day 4 (P = 0.25), and day 5 (P = 0.74).

Mean ± standard deviation scores of patients regarding the question about pain during the 24-h period before follow-up.
Patients were asked to rate the severity of 4 different eye symptoms during the 24-h period before assessment. No statistically significant differences were noted between groups for these symptoms during all the follow-ups (Table 1).
Severity of Symptoms in Both Groups at All Study Points
Gabapentin group n = 15 and ketorolac group n = 22.
Table 2 gives the percentage of patients reporting a variety of systemic adverse events. No statistically significant differences were noted between groups for these at follow-up.
Percentage (%) of Patients with Systemic Symptoms Reported as Positive in Both Groups at All Study Points
Gabapentin group n = 15 and ketorolac group n = 22.
The median regression analysis showed no effect of the type of surgery (epi-on or epi-off) or gender, in the severity of pain at the moment of the questionnaire, and during the 24-h period before the questionnaire at any point of follow-up.
Discussion
This study prospectively compares 2 oral medications for pain and symptomatic control after both epi-on and epi-off CXL. The results suggest that oral ketorolac and oral gabapentin similarly decrease postoperative pain, with comparable decrease of symptoms and similar rates of side effects.
The corneal epithelium is the most densely innervated and sensitive surface of the body. 10 Therefore, pain control after corneal surface surgery is of utmost importance. Most of the current evidence comes from studies related to refractive surgery, mostly photorefractive keratectomy (PRK).11–13 No method of pain control is considered ideal or universally accepted; currently used analgesic medications include NSAIDs such as ketorolac, anesthetics, opiates, acetaminophen, and para-aminobenzoic acid analogues (gabapentin and pregabalin). Topical prednisolone acetate might also play a role in pain management; however, its more important action is to control the inflammation that is a fundamental part of this surgery.
Postoperative pain after CXL comes from different pathways. The process starts when epithelial disruption in the epi-off procedures causes exposure of nerve terminations, the induction of apoptosis, and the necrosis of epithelial cells. Together, these factors initiate an inflammatory cascade in which the different inflammatory cytokines stimulate the nerve terminals sensitive to chemical stimuli. Inflammatory mediators also activate ion channels in the nerve membrane, and this process continues until the epithelium heals.9,11,14–16 The previous discussion takes into account that inflammation causes increased stimulation in the nerve endings of the cornea. 6 Epi-on procedure sometimes present incidental de-epithelization due to the UVA irradiation alone, and this, in part, causes the previously described mechanisms. In both types of procedures, pain also may be influenced by UVA exposure causing additional nerve damage.10,17 Pain signal is then propagated to the somatosensory cortex.
Different approaches have been implanted to attempt pain reduction after CXL. For example, partial epithelium removal, 18 using a hybrid technique that involves disruption of the corneal epithelium with a custom-designed surgical instrument and CXL, may be performed without epithelium debridement (transepithelial).9,16
NSAIDS are considered excellent analgesics in many acute pain settings. 12 The basic mechanism of action is inhibition of the proinflammatory enzyme cyclooxygenase involved in production of proinflammatory mediators. 19 Some authors have studied other oral NSAIDs in PRK surgery: Eslampour concluded that perioperative administration of oral diclofenac is more effective than other routine analgesics (acetaminophen and ibuprofen) in the management of pain. 20 Ketorolac is a NSAID drug effective in cases wherein inflammation causes hypersensitivity of nociceptors (hyperalgesia).
More recently gabapentinoids (gabapentin and pregabalin) have been the subject of trials investigating pain treatment options in patients undergoing refractive surgery.21–25 These are γ-aminobutyric acid analogues with a mechanism of action not fully understood. Their analgesic effect in neuropathic pain is theorized to be the result of gabapentinoids blocking the release of excitatory neurotransmitters by binding to voltage-gated calcium channels.26,27 In a systematic review of trials including perioperative gabapentin or pregabalin, gabapentinoids effectively reduced postoperative pain, opioid consumption, and opioid-related adverse effects after surgery. 21 In a study by Nissman et al., 22 these authors compared the efficacy of oral gabapentin versus oxycodone/acetaminophen for the control of severe pain after PRK, and they found no difference in overall subjective pain management ratings comparing the 2 groups. In contrast, a study by Lichtinger et al. 23 confirmed that low-dose gabapentin used for a short duration reduced postoperative pain after PRK when compared with placebo with no increase in side effects. In the same way, Pakravan et al. 25 and Meek et al. 21 demonstrated that pregabalin and gabapentin seem to be helpful in alleviating post-PRK pain when combined with other measures.
The evaluation of pain remains challenging: for this study, we decided to partially use the questionnaire, including the section related to adverse events, previously used by one of the authors in a prospective randomized clinical trial to study oral gabapentin after PRK. 23 Our study found that both oral gabapentin and oral ketorolac decreased pain at the moment of the questionnaire, as well as cumulative pain in the 24 h before questionnaire at several points of the study. Both had similar efficacy since no statistically significant differences were noted on the pain scale between groups at any point of the study. This suggests that both medications may be used for surgeons performing CXL with either epi-on or epi-off techniques.
This study also found similar percentage of patients reporting different systemic adverse events, with no statistically significant differences noted between groups along the follow-up period. The most common adverse effects of the gabapentinoids reported in a systematic review were sedation and dizziness. 27 However, it is important to note that the percentage of systemic symptoms was high for both groups, specifically cephalea; this may be explained by the nonspecific nature of this symptom, which may be caused by other variables, or even by the CXL procedure itself. Also, some other adverse reactions not assessed in this study, such as renal or hepatic, are rare but must be considered when prescribing these drugs.
This study has some limitations. First, the size of the population was small. Second, there was no comparison with a group treated with placebo; the authors considered that treating those patients with placebo may be unethical. Finally, pain perception may have an interpersonal variability and may be affected by other variables not assessed in this study, making a more objective evaluation challenging.
Interestingly both epi-on and epi-off had similar pain scales and duration. Although not designed to explore these differences, this fact highlights the importance of further studies aiming to decipher the physiopathology of pain after UVA radiation that may uncover new strategies for alleviating pain after CXL. In conclusion, both oral ketorolac and oral gabapentin can be used with similar results for pain and symptomatic control after either epi-on or epi-off CXL procedures. This study may lead to randomized clinical trials to address the best pain management after this procedure.
Footnotes
Acknowledgment
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.