
Abstract
Purpose:
To evaluate the reduction of conjunctival and episcleral hyperemia and bleeding in pterygium surgery following the use of topical brimonidine preoperatively.
Methods:
In this study, 45 patients who had undergone pterygium surgery under topical anesthesia were enrolled. Brominidine tartrate 0.15% eye drops were applied topically to 25 eyes of 25 patients at the sixth and third minutes preoperatively, and no drops were applied to 20 eyes of 20 patients for vasoconstriction. Preoperative and postoperative photographs and video images were taken.
Results:
Vasoconstriction effects of topical brimonidine tartrate on surface vessels were observed. The surface area of blood vessels was reduced 60% within 5 min; this effect was observed with the help of Photoshop and ImageJ programs and it lasted for ∼20 min. The surgery lasts for 7 min, on average, so the conjunctival whitening formed by brimonidine tartrate provides a safe and comfortable operative area throughout the surgery.
Conclusion:
We recommend applying brimonidine tartrate before pterygium surgery due to its conjunctival whitening effect to provide a safe and comfortable operative area throughout the surgery.
Introduction
Pterygium is a proliferative, fibrovascular disease that extends from the limbal conjunctiva to the cornea, showing prominent vascularity. The etiology of pterygium is not known exactly; however, geographic regions (lower parallels), increased age, and male gender are predisposing factors. Pterygium is treated with steroidal and artificial tear eye drops, but if it affects vision, it is excised surgically.1,2
Brimonidine tartrate, which is a selective alpha2-adrenergic receptor (AR) agonist, is used for ocular hypertension and glaucoma. It decreases aqueous humor production and increases uveoscleral outflow. In decreased doses, brimonidine causes conjunctival whitening (blanching) and reduces bleeding; for this reason, it is used in intravitreal injections and ophthalmic surgeries.3–6 Alpha1-AR agonists, which are also vasoconstrictors, may cause rebound redness or tachphylaxis. 7 While mydriasis is a known adverse effect of alpha1-AR agonists, this was not reported with brimonidine, in keeping with its known selectivity for the alpha2-AR. 8 Like other alpha2-AR agonists, brimonidine's binding affinity differs only very modestly among the 3 receptor subtypes (A–C) with a moderate preference (20-fold) for alpha2A-AR versus alpha2C-AR. Its affinity on alpha2-AR is less than those of clonidine and dexmedetomidine. 9
Bleeding during pterygium surgery deteriorates the ability to see anatomical structures. The use of brimonidine before surgery provides better visualization of the anatomical structures and, thus, shortens the duration of surgery.
In this study, we retrospectively evaluated the effect of topical brimonidine on the reduction of conjunctival and episcleral hyperemia and bleeding in pterygium surgery.
Methods
The study protocol was approved by the local ethics committee (Necmettin Erbakan University, Faculty of Medicine Ethics Committee, Konya, Turkey). An informed written consent form was obtained from each patient before surgery. The study was conducted according to the tenets of the Declaration of Helsinki.
A total of 45 patients with 45 eyes that had undergone pterygium surgery under topical anesthesia in Konyagoz Hospital between October 2018 and November 2018 were enrolled in this study. Patients who had any systemic or ocular diseases that might affect their vision were excluded from the study.
Brominidine tartrate 0.15% eye drops were applied to 25 eyes of 25 patients at the sixth and third minutes preoperatively (group 1), and no drops were applied to 20 eyes of 20 patients for vasoconstriction (group 2). Preoperative and postoperative photographs and video images were taken, and vision analysis software was used. The mean age of the first group was 38.08 ± 11.75 (19–53); 12 were males (48%) and 13 were females (52%). The mean age of the second group was 35.20 ± 11.88 (20–55); 11 were males (55%) and 9 were females (45%).
To remove the artificial images and make correct comparisons by matching, we used the Adobe Photoshop system. The vessels were seen as black, and the rest of the area was seen as white. These photographs were transferred to ImageJ software (http://rsbweb. nih.gov/ij/, public domain software), and the program counted the black pixels (vessel area) and white pixels (remaining area). With the help of the program's algorithm, we compared preoperative and postoperative pictures. We accepted the preoperative value (without drops) as normal and evaluated preoperative, intraoperative, and postoperative photographs.
All surgeries were performed by the same surgeon (F.U.). Brimonidine tartrate 0.15% (Brimogut, Bilim İlac, Turkey) was applied at the sixth and third minutes preoperatively. Proparacaine HCl drops (Alcaine; Alcon) were used for topical anesthesia. The nasal pterygium was excised, and a conjunctival graft containing superior limbal tissue was implanted in the bare scleral area with the help of fibrin glue (Tissel; Baxter). Following surgery, all patients used moxifloxacin and dexamethasone combination drops (Moxidexa; Abdi İbrahim, Turkey) 4 times a day for 2 weeks.
The images were taken before and during surgery. The appearance of anterior segment before the application of brimonidine (A, C) and 5 min after brimonidine application (B, D); A and B are colored images; C and D are black images to identify blood vessel surface areas. Image J calculates the surface area by counting black pixels (Fig. 1).
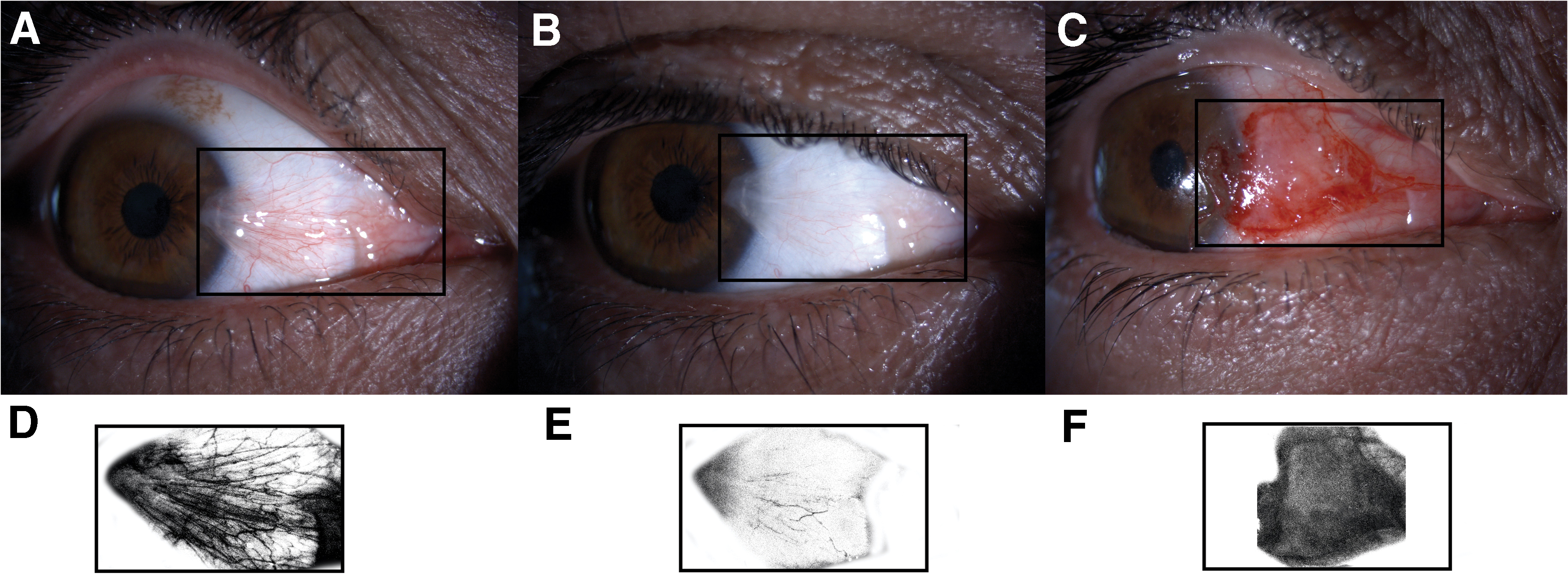
The appearance of anterior segment before the application of brimonidine
Statistical analysis was performed using SPSS version 22. The comparison of data was made using chi-square test, t-test, and paired t-test; p < 0.05 was accepted as statistically significant.
Results
When we compared the preoperative photographs with no drops to the preoperative photographs of the first minute with drops in the first group, we saw that redness decreased from 457.20 ± 29.03 to 270.53 ± 20.99 pixels, on average. However, this did not change in the second group (p < 0.05). The hyperemic area at the intraoperative fifth minute before autograft implantation was 270.53 ± 20.99 pixels in the first group and 496.91 ± 20.27 pixels in the second group (p < 0.05). At postoperative 30 min, the whitening effect of brimonidine had ceased. Brimonidine decreased bleeding at least 50% on average in the first group, but this could not be measured numerically.
The mean preoperative and postoperative intraocular pressures were not significantly different from each other in both groups (p > 0.05); in addition, there was significant difference between the 2 groups in respect to both preoperative and postoperative intraocular pressures (p > 0.05). All these findings are shown in Table 1. The mean operation time of the first group was 6.57 ± 1.015–8 min and that of the second group was 9.21 ± 1.238–12 min (P = 0.02).
Preoperative and Postoperative Findings of the Patients
SD, standard deviation.
Brimonidine decreased the hyperemic area by 60%. Its effect lasted for ∼20 min. The surgery lasts for 7 min, on average, so the conjunctival whitening formed by brimonidine tartrate provides a safe and comfortable operative area throughout the surgery. The hyperemic areas of preoperative dropless, preoperative 1st minute (5 min after the first drop), intraoperative 4th minute (10 min after the first drop), and postoperative 30th minute are shown in Fig. 2.

Preoperative, intraoperative, and postoperative hyperemic areas. Color images are available online.
Discussion
The results of our study support the conjunctival blanching effect of brimonidine, which has been observed in different studies.10–12 Dahlmann-Noor et al. 5 demonstrated vasoconstriction of anterior segment ocular circulation with a noninvasive imaging system. The blood loss should be measured to get the best result, but unfortunately this is not practical.
Brimonidine is a selective alpha2 adrenergic agonist. Its affinity to alpha2 receptors is 790-fold more than to that of alpha1 receptors. This property provides brimonidine with a stronger and more rapid effect. It was reported that phenylephrine 0.25% caused less and short-lived vasoconstriction. 13 In another study, it was reported that apraclonidine is less selective than brimonidine, and its vasoconstrictive effect was found to be smaller and short lived. 14
Brimonidine causes light miosis but does not affect accommodation.15,16 In pterygium surgery, the size of the pupil and accommodation are not important; however, in strabismus surgery, this effect should be taken into account. Side effects such as cyanosis, apnea, hypotonicity, hyperthermia, hypotension, and bradycardia were reported related to brimonidine use in children.17,18 Therefore, even though such side effects may disappear following the cessation of the drug's use, we should be extremely cautious in regard to pediatric use. 19
Brimonidine can also be used in other ocular surgeries, except pterygium, to reduce bleeding and hyperemia. Desco et al. 13 evaluated the effect of prophylactic brimonidine on bleeding complications after cataract surgery. They suggested that brimonidine administered before cataract surgery might significantly reduce subconjunctival hemorrhage in the general population. It has been shown to be beneficial in hypertensive patients. A strong statistical trend, but not significance, has been found in diabetic patients or in patients treated with antiplatelet or anticoagulant drugs. Dahlmann-Noor et al. 5 reported that conjunctival and episcleral bleeding can interfere with visualization of anatomic structures during strabismus surgery. In the United Kingdom, dilute adrenaline (epinephrine) is routinely used to induce vasoconstriction at the beginning of strabismus surgery. Because it causes mydriasis and mildly inhibits accommodation, it is relatively contraindicated if early postoperative suture adjustment is planned. They tested whether topical alpha(2)-adrenergic agonists (brimonidine 0.2% and apraclonidine 1%) were useful alternatives to topical adrenaline (epinephrine) in adjustable suture strabismus surgery. Both agents induced potent transient vasoconstriction of ocular surface vessels. Within 5 min of application, brimonidine reduces blood vessel surface area by 69.2% [confidence interval (95% CI) 50.4–88]; this effect persists for 20 min. Apraclonidine reduces vessel area by 64.6% (95% CI 57.2–72) within 10 min and begins to wear off over the following 10 min. They concluded that, both brimonidine and apraclonidine may be useful alternatives to topical adrenaline (epinephrine) in adjustable suture strabismus surgery.
Hong et al. 20 investigated the effects of preoperative brimonidine-purite 0.15% instillation on intraoperative bleeding and postoperative subconjunctival hemorrhage during strabismus surgery in adult patients and stated that topical brimonidine administration before strabismus surgery may reduce intraoperative bleeding and postoperative subconjunctival hemorrhage in adult patients. McLaurin et al. 21 reported that, Brimonidine 0.025% appeared safe and effective for reduction of ocular redness, with an 8-h duration of action, no evidence of tachyphylaxis, and negligible rebound redness.
Conclusion
Brimonidine causes vasoconstriction and, thereby, decreases hyperemia, making it useful in pterygium surgery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.