
Abstract
Purpose:
To evaluate efficacy and safety of ripasudil for 1 year in addition to or replacing existing treatment regimens.
Methods:
We retrospectively reviewed the medical records for 128 eyes of 128 glaucoma patients who were prescribed ripasudil as an addition to or a switch from their preexisting antiglaucoma instillations. We investigated the rate and factors for discontinuation and intraocular pressure (IOP) reduction.
Results:
Almost half of the patients (60 eyes) discontinued ripasudil treatment before the 1 year mark, while remaining patients completed the treatment. The lack of efficacy and development of adverse effects were significantly correlated with discontinuation (P < 0.001) in the Cox proportional hazards model. In the Kaplan–Meier curve, adverse effects occurred in earlier phase and almost 60% dropped out within 3 months after ripasudil administration. However, adverse effects also occurred randomly throughout the study period. In patients who continued ripasudil, the mean IOPs (mmHg) at baseline, 6 and 12 months after treatment were 17.7 ± 5.1, 14.6 ± 5.0, and 14.8 ± 3.8 in the Addition group, and 17.8 ± 4.1, 15.4 ± 3.2, and 15.4 ± 5.0 in the Switch group, respectively (all P values <0.05).
Conclusions:
Almost half of the patients discontinued ripasudil owing to the lack of efficacy and the generation of adverse effects within the 1 year. In the remaining half, the addition and switching of ripasudil to the existing glaucoma treatment effectively reduced IOP for 1 year.
Introduction
Glaucoma is characterized by chronic progressive optic neuropathy with associated visual field loss. Evidence-based treatment for glaucoma involves reduction of intraocular pressure (IOP),1–3 and medical therapy is typically used at first. In recent years, the range of agents suitable for glaucoma instillations has expanded to include prostaglandin analogs (PGs), β-blockers, αβ-blockers, α1-blockers, carbonic anhydrase inhibitors (CAIs), sympathomimetics, and α2-agonists, and the options for glaucomatous instillation have increased accordingly.
The IOP-lowering mechanism of existing glaucoma treatments involves inhibition of aqueous humor production or promotion of uveoscleral outflow.4,5 In contrast, ripasudil, a selective Rho-associated, coiled-coil-containing protein kinase (ROCK) inhibitor (Glanatec ophthalmic solution 0.4%; Kowa Pharmaceutical Company Ltd.), acts on the main outflow tract via the trabecular meshwork (TM) and Schlemm's canal (SC). ROCK functions as a downstream molecule of Rho and activates the Rho-ROCK signal to promote contraction of the entire cellular tissue. The ROCK inhibitor suppresses this signal and promotes tissue relaxation, resulting in relaxation in the TM. In addition, the ROCK inhibitor not only relaxes tissues but also attenuates the adhesion between Schlemm's endothelial cells. The IOP-reducing effect is achieved by promoting outflow of aqueous humor from the main outflow channel.6–11 Ripasudil has a different IOP-lowering mechanism from the existing antiglaucoma instillations; therefore, it is expected to be used in combination with conventional antiglaucoma ophthalmic solutions. Although many studies have already reported the short-term IOP reduction and adverse effects associated with ripasudil treatment,12–27 the long-term efficacy of ripasudil over more than 1 year has been addressed by only a few studies.28,29 In addition, relatively few studies have evaluated the clinical factors affecting IOP reduction in cases wherein ripasudil was an addition to or a switch from the existing antiglaucoma instillations.30,31
A thorough understanding of the IOP-reducing effects of ripasudil added to or switched in multiple drug combinations may be useful for the treatment of glaucoma. The aim of this study was to evaluate the 1-year efficacy and safety of ripasudil that was an addition to or a switch from preexisting medical therapy regimens.
Methods
We retrospectively reviewed the medical records of glaucoma patients prescribed ripasudil in addition to or as a switch from their preexisting antiglaucoma instillations between February 2015 and May 2016. This research was approved by the Ethics Committee of Toho University Medical Center Ohashi Hospital (H16065).
The exclusion criteria were patients with (1) history of intraocular or corneal surgery except for those who underwent cataract surgery and trabeculectomy more than 12 months before the study periods. (2) Aphakia, (3) concurrent steroid usage, and (4) inflammatory diseases such as uveitis and neovascular glaucoma.
The criteria for adding ripasudil (the Addition group) were (1) insufficient IOP control (not reaching the target IOP) with the present antiglaucoma instillations and (2) patient consent for addition of ripasudil. The criteria for switching to ripasudil (the Switch group) were (1) insufficient IOP control with the maximum tolerated dose of current instillations and (2) patient consent for changing from other antiglaucoma instillation to ripasudil. As patients were already on maximum tolerated medications in the Switch group, the latest added medication was replaced by ripasudil.
When patient's both eyes met the inclusion criteria, only the right eye was included in the study. Thus, total 128 eyes of 128 patients were evaluated in this study. Ripasudil was added to the eyes of 92 patients in the Addition group and 36 patients in the Switch group.
Among total 128, 68 patients continued to use ripasudil for 1 year and were defined as the Survival group. We further divided the survival group into the Addition-Survival (49 survival patients in the Addition group) and Switch-Survival (19 survival patients in the Switch group) groups.
Sixty out of 128 patients discontinued to use ripasudil within 1 year and these were defined as the Dropout group. We further divided the Dropout group into the Addition-Dropout (43 dropout patients in the Addition group) and Switch-Dropout (17 dropout patients in the Switch group) group and investigated the reasons for discontinuation.
Poor IOP control was defined, when more than 5% reduction of IOP from the baseline was not achieved within 6 months after the addition of or the switch to ripasudil. Among the 60 dropout patients, ripasudil was discontinued in 29 because of poor IOP control, and were classified as Poor IOP-dropout group. We further divided the Poor IOP-dropout group into the Addition-Poor IOP dropout (23 dropout patients because of poor IOP control in the Addition group) and Switch-Poor IOP dropout (6 dropout patients because of poor IOP control in the Switch group) group.
In summary, we divided all 128 patients into 4 groups; (a) Addition-Survival (49 survival patients in the Addition group), (b) Addition-Dropout (43 dropout patients in the Addition group), (c) Switch-Survival (19 survival patients in the Switch group), and (d) Switch-Dropout (17 dropout patients in the Switch group). We further divided 29 patients with Poor IOP control in the Dropout group into the (e) Addition-Poor IOP dropout (23 dropout patients because of poor IOP control in the Addition group) and (f) Switch-Poor IOP dropout (6 dropout patients because of poor IOP control in the Switch group) group.
For all 128 glaucoma patients, we created Kaplan–Meier survival curves, in which we defined dropout from using ripasudil as nonsurvival. The Cox proportional hazards model was used to detect factors related to dropout after using ripasudil.
We also compared the clinical characteristics between survival and dropout patients, and between each 2 group; (a) versus (b) and (c) versus (d) by using the unpaired t-test or the Mann–Whitney U test for continuous variables (age, spherical equivalent, IOP before ripasudil administration, IOP reduction rate (%) at 12 months, and prescription score before ripasudil administration), and the Fisher's exact test for categorical data (gender, lens status, glaucoma surgical history, and types of glaucoma diagnosis).
We evaluated IOP reduction at 3, 6, and 12 months in each group [(a) and (c)] by repeated-measures ANOVA with the Bonferroni correction. Univariate and multivariate regression analyses were used to determine factors contributing to IOP reduction rate (%) at 12 months in each group [(a) and (c)]. Independent variables were age, gender, spherical equivalent, IOP and prescription score before ripasudil administration, lens status, and glaucoma surgical history. The factors that showed significant probability less than 0.5 in the univariate regression analyses were included as independent variables for multiple stepwise regression analysis. Statistical significance was considered at P < 0.05. All analyses were performed using a statistical software (SPSS version 19.0 for Windows; SPSS, Inc., Chicago, IL).
Results
In all 128 eyes of 128 patients included in this study, 68 patients (53%) continued to use ripasudil for 1 year (Survival group), and 60 patients (47%) discontinued to use ripasudil within 1 year (Dropout group). Table 1 showed patients' characteristics and comparisons of those between survival and dropout patients. There was a significant difference in the diagnosis of glaucoma between Survival and Dropout group (P = 0.002), and the number of glaucoma other than primary open angle glaucoma (POAG) was significantly more in the Dropout group (32%) than in the Survival group (8.8%).
Patient Characteristics of Both Survival and Dropout Group
Continuous variables are expressed as N (range), mean ± SD. Values in bold are statistically significant (P < 0.05).
Unpaired t-test.
Chi-square test.
Mann–Whitney U-test.
POAG, primary open angle glaucoma; XFG, exfoliation glaucoma; ACG, angle closure glaucoma; SG, secondary glaucoma; IOP, intraocular pressure; SD, standard deviation.
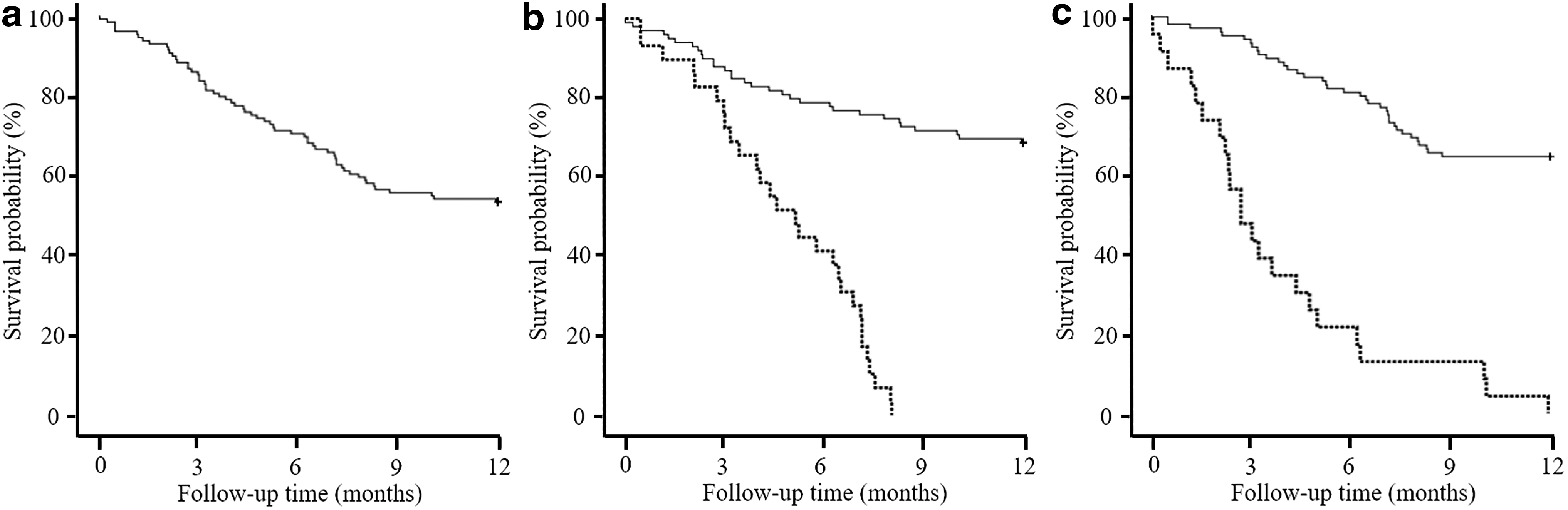
In the Kaplan–Meier curve, the cumulative survival probability and the number of eyes was 83.6% and 107, 70.3% and 90, and 53.1% and 68 at 3, 6, and 12 months, respectively (Fig. 1a). We also created Kaplan–Meier survival curves divided by poor IOP control (Fig. 1b) or adverse effects (Fig. 1c) as nonsurvival. There were significant differences between survival curves (P < 0.001 in Fig. 1b and P < 0.001 in Fig. 1c by Log-rank test). In the Cox proportional hazards model, poor IOP control and adverse effects were significantly correlated with dropout, with hazard ratios of 33.388 (P < 0.001) and 45.931 (P < 0.001) (Table 2).
Cox Proportional Hazard Model of Risk Factors That May Be Associated with Discontinuation of Ripasudil
Others: others include exfoliation glaucoma, angle closure glaucoma, and secondary glaucoma.
CI, confidence interval.
The reasons for discontinuation of ripasudil within 1 year in the Dropout group (60 patients) are shown in Table 3. Forty-three patients from the Addition group and 17 from the Switch group had dropped out. The most common cause of dropout was poor IOP control in 48.3% (53.5% in Addition-Dropout and 35.3% in Switch-Dropout), and the second-most common cause was adverse effects in 38.3% (30.2% in Addition-Dropout and 58.8% in Switch-Dropout). The adverse effects included conjunctival hyperemia and blepharitis. Eight patients were not followed-up.
Reasons for Discontinuation of Ripasudil in the Dropout Group
Data are shown as number of eyes (%).
Addition-Dropout, dropout patients in the addition group; Switch-Dropout, dropout patients in the switch group.
Table 4 shows the characteristics comparisons among the subgroups. The clinical characteristics were compared between (a) Addition-Survival and (b) Addition-Dropout, and (c) Switch-Survival and (d) Switch-Dropout. Type of glaucoma diagnosis was significantly different only between survival and dropout patients in the Addition group [(a) vs. (b), P = 0.011]. There were no significant intergroup; (a) versus (b) and (c) versus (d) differences in other factors.
Subgroups' Characteristics Comparison
Continuous variables are expressed as N (range), mean ± SD. Values in bold are statistically significant (P < 0.05).
Unpaired t-test.
Mann–Whitney U-test.
Chi-square test.
The clinical characteristics were also compared between (a) Addition-Survival and (e) Addition-Poor IOP dropout and (c) Switch-Survival and (f) Switch-Poor IOP dropout. The patient age (P = 0.023), IOP before ripasudil administration (P = 0.045), lens status (P = 0.017), and types of glaucoma diagnosis (P = 0.020) were significantly different between survival and dropout patients due to Poor IOP control in the Addition group [(a) vs. (e)].
There were no significant difference in clinical characteristics between survival and dropout patients due to Poor IOP control in the Switch group [(c) vs. (f)].
The number of medications (Table 5) and details regarding the medication pattern before ripasudil administration (Table 6) were presented by 4 subgroups. In (a) Addition-Survival group, 3-drug regimens (24 patients; 49.0%) and 4-drug regimen (22 patients; 44.9%) were frequently observed (Table 5), and PGs+a combination of β-blockers/CAI in 3-drug regimen and PGs+a combination of β-blockers/CAI+α2 adrenergic antagonists in 4-drug regimen comprised the most frequently used pattern, respectively (Table 6). In (b) Addition-Dropout group, 3-drug regimens (17 patients; 39.5%), and 4-drug regimen (11 patients; 25.6%) were most frequently observed (Table 5), and a combination of PGs/β-blockers+CAI in 3-drug regimen and PGs+a combination of β-blockers/CAI+α2 adrenergic antagonists in 4-drug regimen comprised the most frequently used pattern, respectively (Table 6).
The Number of Medications Before Ripasudil Administration in the Addition Group and the Switching Group
The Detailed Medication Patterns Before Ripasudil Administration
( ), Drug combination; α1, α1-adrenergic antagonist; α2, α2-adrenergic agonist; Acetazolamide, oral medication; β, beta-blockers; CAI, carbonic anhydrase inhibitor; PG, prostaglandin analog.
In (c) Switch-Survival group, 4-drug regimens were the most frequent (14 patients; 73.7%) (Table 5), and PGs+a combination of β-blockers/CAI+α1 adrenergic antagonists comprised the most frequently used 4-drug regimen (Table 6). In (d) Switch-Dropout group, 4-drug regimens were the most frequent (9 eyes; 52.9%) (Table 5), and PGs+a combination of β-blockers/CAI+α2 adrenergic antagonists comprised the most frequently used pattern (Table 6).
Table 7 shows details of medications replaced by ripasudil in the Switch group. Bunazosin hydrochloride was the most frequently replaced in both survival and dropout patients in the Switch group [47.4% in (c) Switch-Survival and 52.9% in (d) Switch-Dropout].
Medications Replaced by Ripasudil in the Switch Group
Figure 2 shows IOPs during follow-up periods. In (a) Addition-Survival group, the mean IOP values (mmHg) at baseline and 3, 6, and 12 months after treatment were 17.7 ± 5.1, 15.0 ± 4.6, 14.6 ± 5.0 and 14.8 ± 3.8, respectively; the IOP had reduced significantly after ripasudil addition (P < 0.001) (Fig. 2a). In (b) Switch-Survival group, the mean IOP values (mmHg) at baseline and 3, 6, and 12 months after treatment were 17.8 ± 4.1, 15.1 ± 3.0, 15.4 ± 3.2, and 15.4 ± 5.0, respectively; the IOP had reduced significantly after ripasudil switch (P ≦ 0.035) (Fig. 2b).

Changes in IOP in the
In the multiple regression analysis, IOP before ripasudil administration [slope = 1.420, standardized partial regression coefficient (β) = 0.458, 95% confidence interval (CI) 0.610–2.229, P = 0.001] in (a) Addition-Survival group (Table 8), and glaucoma surgical history (slope = −23.224, β = −0.616, 95% CI −38.407 to −8.040, P = 0.005) (Table 9) in (b) Switch-Survival group was selected as a significant contributing factor to the IOP-reduction rate at 12 months, respectively.
Univariate and Multiple Regression Analysis for IOP Reduction Rate (%) at 12 Months in (a) Addition-Survival Group
These factors, which showed significant probability of lower than 0.5 in univariate regression, were included in multiple stepwise regression analysis as explanatory variables. Values in bold are P < 0.5 in univariate regression analysis, and are statistically significant (P < 0.05) in multiple regression analysis.
β, standard partial regression coefficient; SE, standard error.
Univariate and Multiple Regression Analysis of IOP Reduction Rate (%) at 12 Months in (c) Switch-Survival Group
These factors, which showed significant probability of lower than 0.5 in univariate regression, were included in multiple stepwise regression analysis as explanatory variables. Values in bold are P < 0.5 in univariate regression analysis, and are statistically significant (P < 0.05) in multiple regression analysis.
Discussion
Multiple drug usage is a common treatment strategy for glaucoma patients and is used with a wide range of drug combinations. Ripasudil, which acts on the main outflow tract via the TM and SC, has a different IOP-lowering mechanism to other existing antiglaucoma instillations; therefore, it could be used in combination with conventional therapy. In this study, we added or switched to ripasudil in patients who were receiving single or multiple antiglaucoma ophthalmic solutions and evaluated the long-term IOP-reducing effect and safety effects of ripasudil for 1 year.
The cumulative probability of continuation of ripasudil administration (survival) was 53.1% at 1 year (Fig. 1a). Although glaucoma diagnosis was significantly different between survival and dropout patients (Table 1), the Cox proportional hazards model (Table 2) detected poor IOP control and the adverse effects, not glaucoma diagnosis, as risk factors for dropout. The 2 most frequent dropout reasons were poor IOP control (48.3%) and adverse effects (38.3%) (Table 3). Before determining poor IOP control, IOP is usually evaluated several times. The cumulative probability of ripasudil administration decreased gradually (Fig. 1b). On the contrary, as shown in Fig. 1c, adverse effects occurred in earlier phase and almost 60% dropped out within 3 months after ripasudil administration. However, adverse effects also occurred randomly throughout the study period.
The discontinuation rate due to adverse effects was 38.3% in this study (Table 3), which was similar to the rates of 8.0%–40.7% reported in previous studies.22,25,26,28 Blepharitis was the most commonly observed adverse effect that led to termination of ripasudil use. 25 However, the incidence of blepharitis in this study was 15.0%, which was lower than the rates (20.6%–25.2%) reported in previous studies.25,28 The incidence of conjunctival hyperemia was 23.3%, which was higher than a previous study (19.2%). 25 In the dropout patients, 13 of 23 (56.5%) eyes and 8 of 29 (27.6%) eyes stopped receiving ripasudil within 3 months because of adverse effects and insufficient IOP control, respectively. In those who had adverse effects, the discontinuation rates due to conjunctival hyperemia and blepharitis within 3 months were 64.3% (9 of 14 patients with hyperemia) and 44.4% (4 of 9 patients with blepharitis), respectively. In many cases, treatment was interrupted due to the development of conjunctival hyperemia at a relatively early stage. Rho kinase inhibitors can induce conjunctival hyperemia as a result of smooth muscle relaxation and the resultant dilatation of the blood vessels.9,16,32 Therefore, previous studies reported that conjunctival hyperemia will occur generally at a high frequency (55%–96.0%) as a part of the action mechanism of ripasudil.13–15 However, conjunctival hyperemia generally resolves on its own within 1–2 h, 33 so it is necessary to adequately explain this possible complication to patients and inform them that it could disappear naturally, which is also important to prevent early dropout. In the (b) Addition-Dropout and (d) Switch-Dropout groups, the average number of preexisting glaucoma medications before ripasudil administration was already 3.1 and 3.7, and further research is necessary to elucidate whether the combinations of previous glaucoma medications and ripasudil reinforce the conjunctival hyperemia.
In a comparison of clinical characteristics between the survival and dropout groups, the significant difference of type of glaucoma diagnosis was found between 2 groups [(a) vs. (b) and (a) vs. (e), P = 0.011, P = 0.020, respectively] in Table 4. Kawara et al. 24 reported a significant difference in the types of glaucoma diagnoses between survival and dropout groups based on 6-month observation data. They suggested that the dropout group included a higher proportion of secondary glaucoma (SG) cases and that ripasudil has a weak IOP-lowering effect in eyes with SG, which led to surgery earlier than in cases of open angle glaucoma. Although total numbers were small, the Addition-Dropout and the Addition-Poor IOP control included significantly more SG than the Addition-Survival groups. Future research would need to include large number of patients to investigate whether types of glaucoma may affect the efficacy of ripasudil.
As the inhibition of ROCK reduces cell tension and stiffness, regulates fibrogenic activity, and decreases extracellular matrix (ECM) synthesis and rigidity in the TM, SC, and juxtacanalicular tissue,34,35 the effect of ripasudil may decline with age due to the reduced numbers of cells in the TM and sclerosis of tissue.36–38
Patient's age was significantly higher in the (e) Addition-Poor IOP dropout than (a) Addition-Survival group (Table 4). Low compliance with eye drops is age-dependent39,40 and could have influenced poor IOP control in this study (Table 4). IOP before ripasudil administration in (e) Addition-Poor IOP dropout was significantly higher than (a) Addition-Survival (Table 4). In mean deviation (MD) measurements obtained by standard automated perimetry with the Humphrey field analyzer using the 30-2 Swedish Interactive Threshold Algorithm, the average of MD in (e) Addition-Poor IOP dropout was −13.70 ± 9.04 and that in the (a) Addition-Survival group was −12.73 ± 7.72 before ripasudil administration. The (e) Addition-Poor IOP dropout was at a more advanced stage of progression than (a) Addition-Survival group, so it is possible that IOP before ripasudil administration was also higher in the poor IOP dropout group.
The rate of phakic in (a) Addition-Survival was significantly higher than in (e) Addition-Poor IOP dropout (Table 4). Higher age and significant more SG in the Addition-Poor IOP dropout group may be accompanied with larger numbers of pseudophakic patients. Further research may be necessary to elucidate the effect of ripasudil on lens status.
We also evaluated the IOP-lowering effect of ripasudil in the Survival group. The IOP at 3, 6, and 12 months after adding or switching ripasudil was significantly lower than the baseline IOP in both groups (Fig. 2a, b). This result supported the findings of previous studies with added ripasudil in short-term18,20,24,26 and long-term observations. 29 In our study, although the total number of medications used before addition of ripasudil varied from 1 to 4 agents (Table 5), the findings were similar to previous reports reporting that addition of ripasudil to existing glaucoma treatment regimens is effective in reducing IOP, regardless of the number of medications in use 20 and in patients receiving maximum medical therapy.18,24,26 Ripasudil has a different IOP-reducing mechanism and can be expected to cause further IOP reduction even under multiple drug use.
As a significant contributing factor to the IOP-reduction rate (%) at 12 months, multiple regression analysis selected the IOP before ripasudil administration (P = 0.001) in the (a) Addition-Survival group (Table 8) and glaucoma surgical history (P = 0.005) in the (c) Switching-Survival group, respectively (Table 9). Therefore, the contributing factors may differ when ripasudil is added or switched in patients receiving multiple drug therapy for glaucoma. In the (a) Addition-Survival group, higher IOP before ripasudil administration was associated with a greater reduction in IOP, which supports previous reports showing that high baseline IOP levels are associated with greater IOP reduction after instillation of PGs41–43 or ripasudil.4,22,24
In the (c) Switching-Survival group, the IOP reduction rate may be high in cases without a glaucoma surgical history. This is because after filtration surgery, the main outflow pathway of the aqueous humor changes from the TM to the conjunctival filtration bleb through the scleral window. Thus, the main route is presumably abandoned during this period. Therefore, even if administration of ripasudil is performed after bleb failure, the long-abandoned TM may not respond to the action of ripasudil. However, these post hoc subgroup analyses were statistically underpowered, and its interpretation was limited.
This study has some other limitations. As the study had a retrospective design, there may be selection bias. Although the Addition-Dropout and the Addition-Poor IOP control included significantly more SG, detailed comparison by types of glaucoma disease could not be performed, due to the small number of cases for each glaucoma type other than POAG. Previous studies showed that ROCK inhibitors are effective for exfoliation glaucoma (XFG).22,23,27 XFG is an SG, in which the exfoliative material blocks the aqueous humor outflow path, resulting in an increase in the IOP. Ripasudil lowers IOP by relaxing TM cells, expanding the meshwork gap, and suppressing production of the ECM. 7 Some previous studies, however, showed no effectiveness of ripasudil in XFG and SG.12,26 This may be explained by damage to the outflow pathways and cells by exfoliative material and inflammation, respectively. In this study, the subjects were all Japanese with dense pigmented eyes; ripasudil may have different effects on other races. Further prospective studies are required to evaluate the efficacy of ripasudil for lowering IOP in patients in different races and types of glaucoma.
The multiple drug usages are covered by the Japanese Health Insurance System; however, these situations may be different in other nations with various health insurances.
In conclusion, we evaluated 128 eyes of 128 patients with adjunctive ripasudil therapy. Almost half of the patients discontinued ripasudil within 1 year due to the lack of efficacy and the generation of adverse effects. In the remaining patients (53.1%), the addition of and switching to ripasudil from existing glaucoma treatment regimens effectively reduced IOP for 1 year.
Footnotes
Acknowledgment
The authors thank Mari S. Oba, Ph.D for assistance with statistical analyses.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.