
Abstract
Purpose:
To evaluate the effects of a coexisting epiretinal membrane (ERM) on the treatment outcomes of a dexamethasone implant (DI) in diabetic macular edema (DME) patients.
Methods:
One hundred five eyes of 78 DME patients (44 F, 34 M; mean age: 65.7) treated with minimum 2 DIs were enrolled into this retrospective study. The study population was divided into the ERM (+) study group and the ERM (−) control group. The best corrected visual acuity (BCVA), intraocular pressure, and central macular thicknesses (CMTs) were evaluated at baseline and months 1, 2, and 3 after each DI treatment.
Results:
Both groups were comparable in baseline BCVA, CMT, HbA1c levels, and age. In the study group (n: 49), BCVA changed following the first DI from 0.83 to 0.76 and from 0.97 to 0.80 following the second DI. CMT decreased after the first DI from 465 to 377 μ (P < 0.001) and from 477 to 356 μ (P < 0.001) after the second DI. In the control group (n: 56), BCVA changed following the first DI from 0.81 to 0.77 and from 0.86 to 0.83 following the second DI. After the first DI, CMT decreased from 483 to 280 μ (P < 0.001) and from 468 to 301 μ (P < 0.001) after the second DI. The inter-group comparison revealed no significant difference in visual or anatomical gain (P = 0.46, P = 0.05, respectively).
Conclusion:
The presence of an epiretinal membrane did not change the treatment response to DI therapy.
Introduction
Visual impairment in the diabetic population is most commonly caused by diabetic macular edema (DME), 1 which affects ∼7% of all diabetic patients. 2 Although antivascular endothelial growth factor (VEGF) agents are generally considered as first-line therapy for center-involved DME, 3 a dexamethasone implant (DI) of 0.7 mg (Ozurdex, Allergan, Inc., Irvine, CA) has been shown to be effective in improving visual acuity and decreasing retinal thickness, 4 even in patients with DME refractory to anti-VEGF treatments. 5
With the introduction of optic coherence tomography (OCT), epiretinal membrane (ERM) formation has turned out to be one of the most highly detected asymptomatic foveal disorders among the elderly. Recent studies have demonstrated how its prevalence increases with diabetic retinopathy in addition to other risk factors, such as aging, smoking, or cataract surgery.6,7 The commonly practiced panretinal photocoagulation also contributes to ERM formation in diabetic populations with diabetic retinopathy. 8 In contrast to antero-posterior tractions as vitreomacular traction or proliferative preretinal membranes, which often require surgical intervention, the treatment of center-involving DME with coexisting ERM may be still controversial. Some authors have suggested DI therapy for persistent macular edema following idiopathic ERM removal,9,10 but many physicians consider intravitreal anti-VEGF agents or DI as first-line therapy in DME independent from the presence or absence of an ERM.
Although several reports have searched for the clinical effects of vitreomacular interface anomalies (VMIA), including ERMs in DME patients undergoing anti-VEGF therapy,11,12 the effect of ERM on ongoing DI therapy has not yet been reported. In this current study, we aimed to assess the influence of ERM formation on the therapeutic outcome of DI-treated DME cases in 2 comparable cohorts. Thus, the influence of such a tangential traction and the necessity of ERM removal before medical treatment of DME can be questioned.
Methods
Patient enrollment
In this retrospective chart study, medical and electronic records of 196 eyes in 142 DME patients who had undergone at least 2 consecutive DIs between January 2016 and January 2019 in our retina department were reviewed by investigators. Our inclusion criteria were defined as center-involving DME with a minimum baseline central macular thickness (CMT) value of 350 μm; a minimum baseline best corrected visual acuity (BCVA) of 20/200 (Snellen); diagnosis of diabetes mellitus type II; and foveal center involving ERM formation on spectral domain OCT (SD-OCT) scans graded as “Grade 2” ERM according to the Gass classification (Fig. 1). Our exclusion criteria were irregular follow-up visits within the study period; any previous anti-VEGF treatments in the last 3 months before study enrollment; administration of DI within the last 4 months; additional ocular pathology, such as glaucoma or venous occlusions; any intraocular surgery; additional focal or panretinal laser photocoagulation; or intravitreal anti-VEGF treatment within the study period. The foveal vitreomacular interface (VMI) was evaluated via baseline SD-OCT scans by 2 independent, experienced retinal physicians, and cases with any VMI disorders other than Grade 2 ERM (such as Grade 1 ERMs in the form of cellophane maculopathy or eccentric ERM formations not involving central fovea) were excluded from the study population. Eyes with cataract progression within the study period or any lens opacities at baseline were also excluded from both study cohorts to eliminate the effect of cataract formation on the visual outcomes. Finally, 49 eyes of 37 DME patients with concurrent ERMs were included in the study group (ERM+), and 56 eyes of 41 DME patients without any ERMs were enrolled into the control group (ERM−).
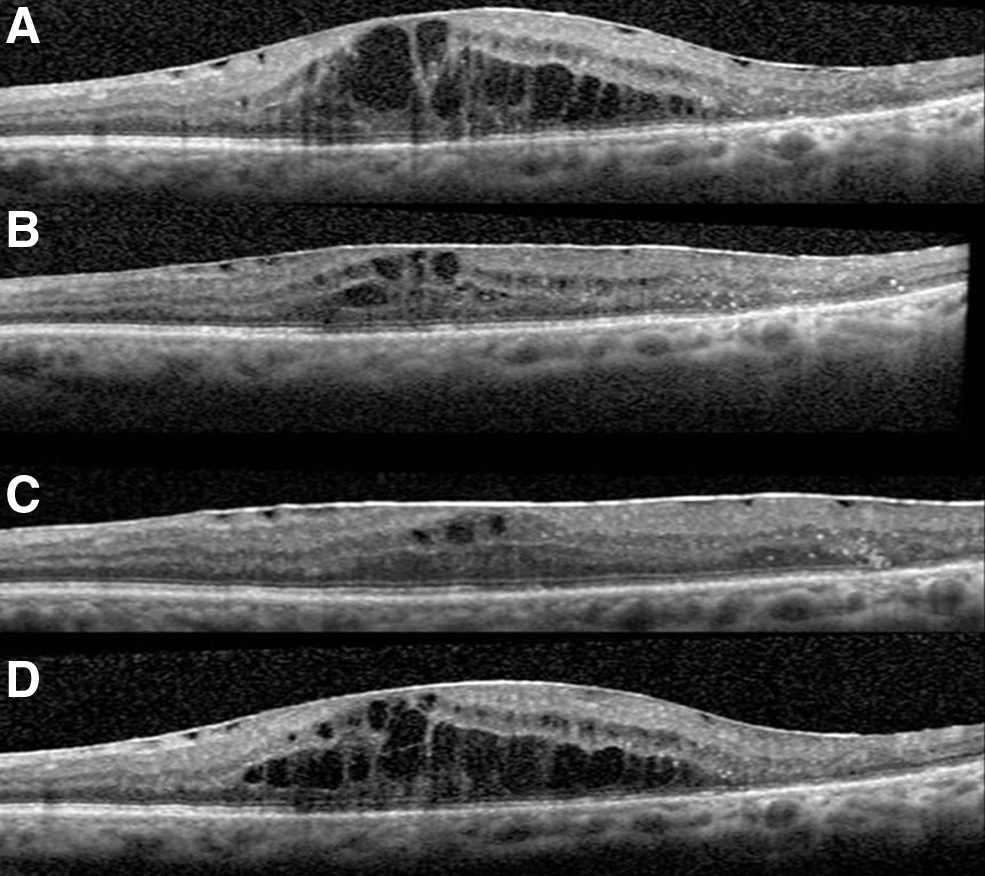
A typical case with its fovea involving central ERM in the study group; the DME regressed significantly after the first DI administration and returned in a bouncing effect at postoperative sixth month visit.
Follow-up and ethics
All eligible patients underwent baseline fluoresceine angiography (FA; Visucam500; Carl Zeiss Meditec, Jena, Germany) and comprehensive ophthalmological examination, including assessing BCVA, biomicroscopy, fundoscopy, measurement of intraocular pressure (IOP) via Goldmann tonometry, and SD-OCT examination before enrollment. OCT images were obtained by SD-OCT (Spectralis; Heidelberg Engineering, Heidelberg, Germany) by a certified operator. The following scan acquisition parameters were required: dense volume scan (30° × 25°, roughly 9 mm × 7.5 mm), 31 B-scans each spaced 244 μm apart, automatic real-time mean of 20, and high speed (512 A-scans/B scan). All examinations except for FA were done on a monthly basis. The BCVA, IOP, and CMT values at preinjection, month 1, 2, and 3 visits following each DI treatment were taken into consideration. On day 1, all patients underwent ophthalmic examination, including BCVA, IOP, and biomicroscopy.
Intravitreal DI injection was performed under topical anesthesia with 0.5% proparacain hydrochloride and sterile conditions using single-use injection kits and a 5% povidone iodine solution for ocular surface preparation. Topical antibiotics were prescribed for the 2 weeks following drug administration. Retreatment criteria on a monthly follow-up basis were a decline in BCVA more than one Snellen line or an increase in CMT value more than 50 μm, both in comparison to the previous visit.
This study adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients before all invasive procedures in the follow-up. Ethical board approval was obtained from the Ethical Committee of Okmeydanı Education and Research Hospital, University of Health Sciences. Written informed consent was obtained from each patient before all invasive procedures.
Statistical methods
Following data collection from the review of medical records, all BCVA values were converted from Snellen ratios into logarithms of minimum angle of resolution (logMAR) values for a more accurate statistical analysis. Although Snellen charts are not directly comparable to logMAR charts, we used the international Snellen-to-logMAR conversion tables and calculators to assure a proper conversion. The data were evaluated for normality using the Kolmogorov–Smirnov test. As the distribution of BCVA and CMT values were found to be normal, changes in these parameters between baseline and following time points were assessed with a repeated measures test. Student t-tests and repeated measures of analysis of variance were preferred for intergroup and intragroup statistical analyses using SPSS (Version 22.0; SPSS, Inc., Chicago, IL). An overall 5% type-1 error level was considered to be statistically significant.
Before starting the study, we calculated the minimum sample size by using the G*Power 3.1.9.2 (Universitat Düsseldorf) program. The effect size was assumed as 0.8 in the automatic program embedded within the G*power, and we found out that a minimum number of 42 individuals per each group were to be enrolled to have 95% power with a 5% type 1 error level.
Results
One hundred five eyes of 78 patients were enrolled into this retrospective study according to our inclusion/exclusion criteria. The demographical and baseline clinical features are reflected in Table 1. Both study cohorts were comparable in demographic features, including age, duration of diabetes, systemic regulation in means of serum HbA1c levels, and distribution of gender. Baseline clinical findings, such as pseudophakia, finalized panretinal laser photocoagulation ratios, and baseline clinical findings such as BCVA, CMT, and percentage of serous retinal detachment (31% vs. 36%) between groups were statistically similar. All eyes (n: 105) from our study population had a history of anti-VEGF therapies (ranibizumab, n: 62; aflibercept, n: 43) earlier than 3 months before the first DI injection and study enrollment.
Demographic and Clinical Characteristics of the Study Population
PRP, panretinal photocoagulation; SRD, serous retinal detachment; BCVA, best corrected visual acuity; CMT, central macular thickness; IOP, intraocular pressure; logMAR, logarithms of minimum angle of resolution.
The study population underwent 2 consecutive DI administrations within the study period (12.2 ± 2.1 months). The mean retreatment interval between the first and second DI injections were similar in both cohorts (study and control groups) as 5.8 ± 2.1 versus 5.9 ± 3.2 months (P = 0.79), respectively. None of the patients reported any systemic or severe adverse events such as endophthalmitis, retinal detachment, or vitreus hemorrhage. In 8 eyes of the total population (n: 105; 7.6%), IOP was elevated over 25 mmHg following the first DI administration, and in all cases, IOP was under control with topical antiglaucomatous agents in further follow-up. Seven eyes of these 8 cases were in the study group (n: 49; 14.3%), and only 1 patient was in the control group (n: 56; 1.8%). Thus, IOP elevation was found to be significantly higher in the ERM (+) study group (14.3% vs. 1.8%; P = 0.01).
Anatomical results
After the administration of the first DI, the mean baseline CMT value decreased in the study group from 465 ± 156 μm to 312 ± 111 μm, 320 ± 62 μm, and then increased to 377 ± 118 μm at the first-, second-, and third-month visits, respectively (P < 0.001 at all visits). Following the second DI, baseline CMT decreased significantly from 477 ± 123 μm to 365 ± 88 μm, 356 ± 65 μm (P < 0.01), and finally increased to 428 ± 122 μm (P = 0.04) postinjection in the first-, second-, and third-month visits. In the control group, the baseline CMT also decreased (in response to the first DI administration) significantly from 483 ± 128 μm to 316 ± 95 μm, 280 ± 80 μm, and then changed to 401 ± 157 μm at the first-, second-, and third-month visits, respectively (P < 0.001; at all visits). After the second DI, the CMT declined significantly from 468 ± 140 μm to 306 ± 93 μm, 301 ± 91 μm (P < 0.001), and changed to 440 ± 134 μm (P = 0.02) at the first-, second-, and third-month visits. The comparison between the study and control groups regarding CMT changes revealed no statistical difference (repeated measures; P = 0.056), although control group showed greater CMT changes within the study period (Fig. 2).
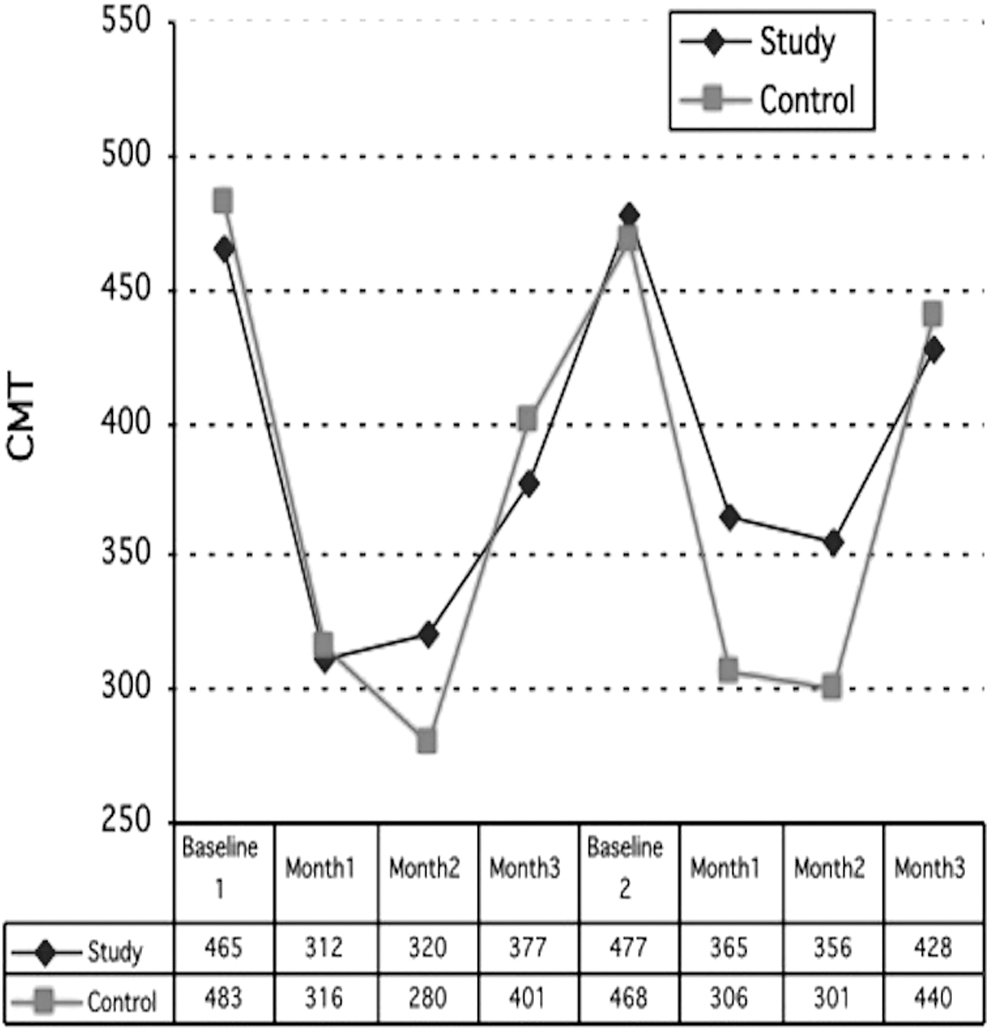
Although CMT values decreased in the control group at second month visits more distinctly, both groups' CMT changes followed similar curves and the intergroup comparison did not reach statistical significance (repeated measures; P = 0.056).
Visual results
After the first DI, the baseline BCVA in the study group increased from 0.83 ± 0.35 (20/135) to 0.76 ± 0.44 (20/115) at the first month (P = 0.02) and changed insignificantly afterward to 0.80 ± 0.51 (20/126) and 0.90 ± 0.62 (20/158) at months 2 and 3 (P = 0.2), respectively. Following the second DI, however, the mean BCVA increased significantly (P = 0.03) from 0.97 ± 0.61 (20/186) to 0.82 ± 0.58 (20/132), 0.80 ± 0.57 (20/126), and 0.80 ± 0.50 (20/126) at the first-, second-, and third-month visits, respectively. In the control group, the BCVA improved significantly (in response to the first DI administration) from 0.81 ± 0.52 (20/130) to 0.70 ± 0.50 (20/100) (P = 0.02), 0.70 ± 0.47 (20/100) (P = 0.01) and changed to 0.77 ± 0.54 (20/117) (P = 0.53) at the third-month visit. After the second DI, BCVA increased from 0.86 ± 0.62 (20/144) to 0.74 ± 0.56 (20/110) (P = 0.04), 0.77 ± 0.53 (20/118) (P = 0.05), and finally decreased to 0.83 ± 0.64 (20/135) at months 1, 2, and 3, respectively. Intergroup analyses revealed that ERM formation did not significantly affect the monthly changes of BCVA in the study population (repeated measures; P = 0.46) (Fig. 3).
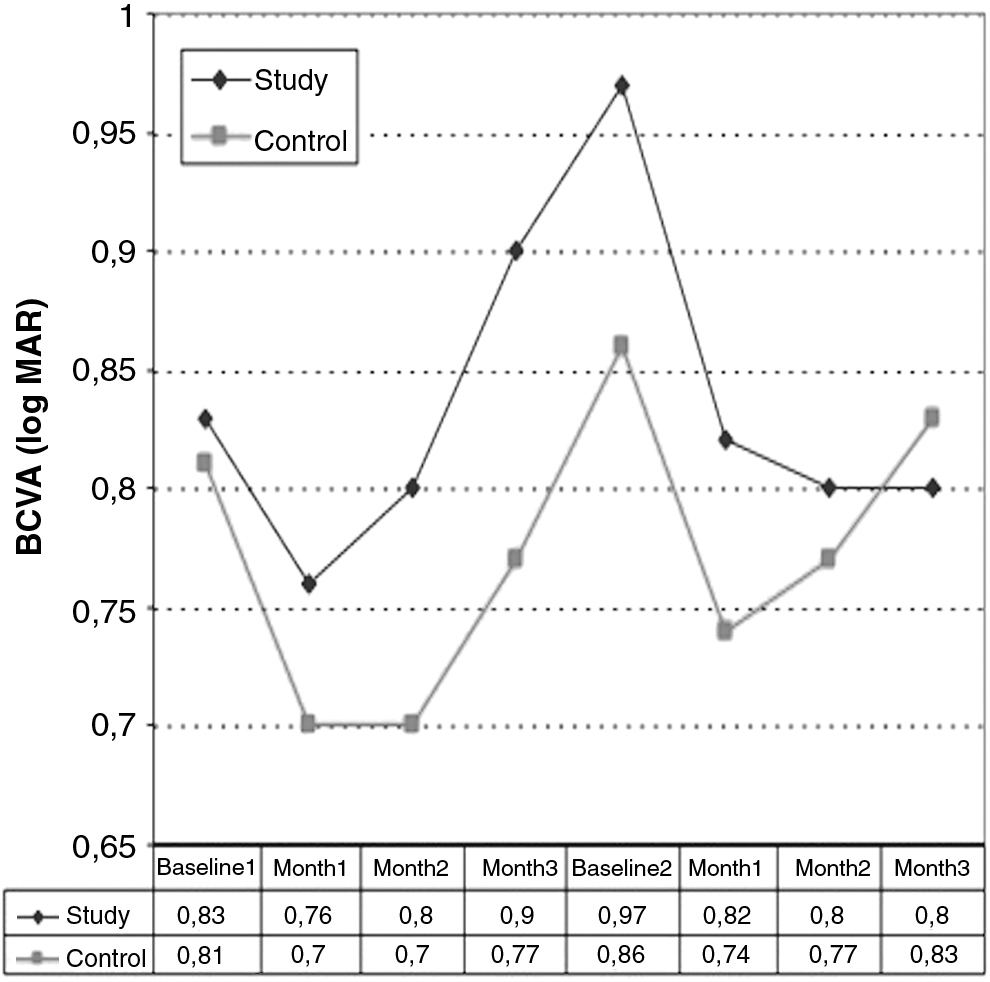
The visual acuity changes of both groups demonstrated parallel curves and statistical analyses revealed no difference between study and control groups (repeated measures; P = 0.46).
Discussion
In the last decade, anti-VEGF agents have dominated the treatment of center-involved DME and are positioned as the first-line therapy according to the recent DME guidelines. 3 DI was introduced later and proved itself effective in refractory and naive center-involved macular edema, with its unique pharmacokinetics even in vitrectomized cases.13,14 Since VMIA could change the effectiveness of intravitreal therapies, we believe it was beneficial to research the clinical influence of concurrent ERMs in DME cases undergoing repeated DI administrations. This is the first study to focus on the impact of ERMs on treatment outcomes after DI in DME.
Several retrospective and comparative studies have reported the relationship between VMIA and DME treatment outcomes under anti-VEGF therapies. Yoon et al. demonstrated, in a small group, that VMIAs, including ERMs, significantly reduced the final visual gain in DME patients under anti-VEGF treatment. 15 Later, Ercalik et al. found that ERM formation inhibited both visual and anatomical gains following a single dose of 0.5 mg of intravitreal ranibizumab (IVR) administration. 11 In a prospective study, Wong et al. searched for VMIAs and their effects on clinical outcomes in a DME population receiving IVR therapy for 1 year. In a subgroup analysis, they pointed out that clinically significant ERMs at baseline were significantly predictive of less visual improvement. 12 These results might be easily associated with the physical barrier effect of VMIAs such as ERMs. In a recent retrospective comparative study, Namba et al. 16 reported that DME patients with ERMs responded anatomically and functionally to anti-VEGF less than the DME patients without ERMs in a 1-year follow-up. In their report, they included an in vitro ERM model (constructed histologically equal to an excised diabetic ERM specimen) and demonstrated that in vitro ERM itself served as a mechanical barrier and inhibited anti-VEGF-like fractional antibody (Fab) diffusion. Thus, the researchers associated the clinically anti-VEGF resistance of DME patients with ERMs with this barrier effect of ERM formation. 16 However, the subtype of DME may also have a critical effect on treatment outcomes. Wu et al., 17 for example, researched DME patterns and VMIAs and their effect on intravitreal bevacizumab (IVB) treatment outcome. They found that DME in the form of cystoid macular edema responded best to the therapy, but cases with VMIAs did not benefit functionally or anatomically from IVB therapy. 17
In contrast to these previous anti-VEGF studies, in this pilot study with DI, we found that ERMs did not significantly influence our final visual outcomes. This finding may be a result of the broad anti-inflammatory effect of dexamethasone that targets many inflammatory mediators, not just the VEGF molecules unlike the anti-VEGF agents. There is still no established evidence that ERMs are an inflammatory biomarker among DME patients, even though DME is accompanied by VMIAs in 28% of patients. 18 Zandi et al. reported that eyes with ERMs have a higher vitreal level of several cytokines than eyes with macular holes. 19 Compared to idiopathic ERMs, diabetic ERMs apparently a more predominant inflammatory character, 20 therefore DME with concurrent ERMs might benefit from this broad-acting anti-inflammatory therapy. Urbančič et al. investigated the surgically removed epiretinal membranes of proliferative diabetic retinopathy (PDR) patients with immunohistochemical methods and found that T and B lymphocytes were significantly more numerous in ERMs removed from eyes with active PDR. 21 They concluded that ERMs' inflammatory cell density reflected the severity of PDR. Likewise, we believe that ERMs might easily contribute with their presence and tangential traction forces to the chronic inflammation in diabetic retinopathy. Therefore, a potent anti-inflammatory drug such as DI could be much more beneficial in DME cases with concomitant ERMs.
Regarding our anatomical outcomes, we found no difference between our study groups—at least not at a statistically significant level, although the CMT changes in the control group were greater and did differ to some degree from the study group at early postinjection visits. Since a bouncing effect is typically expected under consecutive DI treatment sessions, the CMT curves followed a sinusoidal pattern in both groups. We believe that the presence of a clinically significant ERM limited both CMT reduction and DME recurrence with its tangential forces. In most of the previous reports with patients under anti-VEGF therapies, however, the negative inhibitor effect of ERMs on CMT reduction was found to be statistically significant.11,12 Kulikov et al., for example, in a recent SD-OCT study in a DME population, found that a center involving ERMs other than vitreomacular tractions or adhesions dramatically reduced the anatomical response to anti-VEGF drugs. 22
Interestingly, in our study, the IOP elevation secondary to the DI treatment was found to be significantly higher rated in the study group than in the control group. Regarding the limited patient number of our study cohorts, this finding should be interpreted carefully. In a recent study, Sakimoto et al. concluded that the presence of a unilateral ERM can be a potential risk factor for the unilateral severity of primary open angle glaucoma (POAG). 23 We believe that further studies must be conducted to exhibit a possible relationship between ERMs and POAG or the steroid responder subgroup of the general population to enlighten this co-finding of ours.
This study naturally has several limitations. The relatively small sample size in each cohort necessitates further studies to be conducted to make a definite conclusion about this topic. The lack of randomization deriving from the retrospective nature is another limitation, although we have set our inclusion and exclusion criteria strictly to prevent any biases to arise within the study process. Despite these limitations, our study has revealed valuable findings based on our real-life data and experience. An extension of this study could further investigate the therapeutic effects of DI in the concomitant ERM group of our study population following the possible surgical removal of their ERMs in later follow-up.
Conclusion
Concurrent ERMs may complicate, among other VMIAs, the treatment outcomes of DME patients undergoing anti-VEGF therapy according to the previous reports. DI, however, overcomes the inhibitory effect of ERMs in DME populations—both in functional and anatomical aspects—according to the results of our study. Hence, retinal physicians might consider DI as an alternative therapy in DME patients with a center involving ERMs, especially in anti-VEGF non- or poor-responding cases.
Footnotes
Acknowledgments
Special thanks to the Heidelberg-certified SD-OCT operator of our retina department, Esra Çınar, for acquiring OCT scans in the study period.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no funding for this article.