
Abstract
Purpose:
To explore safety and therapeutic efficacy of a topical ophthalmic triamcinolone acetonide-loaded liposome formulation (TA-LF) as primary therapy in patients with macular edema (ME) secondary to branch retinal vein occlusion (BRVO).
Methods:
Twelve eyes of 12 patients with ME secondary to BRVO were exposed to a topical instillation of 1 drop of TA-LF (TA 0.2%) 6 times a day for 12 weeks to evaluate safety and efficacy. Best corrected visual acuity (BCVA) intraocular pressure (IOP), slit lamp examination, and central foveal thickness (CFT) were analyzed at every visit. In addition, the morphology of TA-LF was analyzed using scanning electron microscopy (SEM) and transmission electron microscopy (TEM).
Results:
Patients presented a significant improvement of BCVA and CFT without significant IOP modification (P = 0.94). Treated eyes showed BCVA improvement from 40 ± 12.05 to 64.83 ± 15.97 letters and CFT reduction from 682.91 ± 278.60 to 271.58 ± 57.66 μm after 12 weeks of TA-LF therapy (P < 0.001). No adverse events, including IOP rising, were registered. SEM analysis of liposomal formulations showed that liposome (LP) size depends on its concentration. As the concentration of TA increased, the average size of LPs and the number of larger particles increased as well. TEM study displayed that LP formulation efficiently solubilizes TA crystals in nanoparticles and encapsulates them.
Conclusion:
LPs can function as nanocarriers of TA and they could be used as topical ophthalmic primary therapy instead of intravitreal drugs in patients with ME secondary to BRVO.
Introduction
Sophisticated eye barriers represent a major challenge for drug delivery into ocular tissues. Conventional ophthalmic formulations, such as eye drops, suspensions, and ointments, are effective enough when treating eye surface diseases. Nevertheless, because of the presence of ocular barriers, such as the sclerocorneal parenchyma, the corneal epithelium and endothelium, the inner and outer blood–retinal barriers, and the retinal inner limiting membrane, topical drugs hardly reach the posterior segment of the eye. 1 To avoid ocular barriers and to reach therapeutic doses into the vitreous, physicians use intravitreal injections (IVTs) to deliver drugs to the posterior segment. Currently, IVTs are the most performed intraocular procedures, increasing their number every year. 2 IVTs have become the standard delivery method for corticosteroids, antibiotics, antimetabolites, and anti-vascular endothelial growth factor (VEGF) agents,3–8 treating multiple vision-threatening retinal disorders like age-related macular degeneration, cystoid macular edema (ME), endophthalmitis, diabetic retinopathy, and ocular vascular occlusions.9,10
Although intravitreal administration of drugs is a standardized and efficient route, it is not free from potentially severe complications like endophthalmitis, lens damage, intravitreal hemorrhage, and retinal detachment.11–13 In addition, intravitreal administration is associated with reduced compliance due to the liability it may represent for health care systems, physicians, and patients. 14 Moreover, in developing countries, IVTs represent an expensive alternative because of the specialized human resource and infrastructure required. 15 Therefore, the development of novel ocular drug delivery systems using nanotechnology (nanocarriers) has received extensive attention, because of the ability of nanocarriers to promote drug delivery across tissue barriers; to control the release of a topical administered drug; to improve the bioavailability; and to direct a drug to the target tissue. 16 Among ophthalmic drug delivery nanosystems, liposomes (LPs) have been the most extensively studied.17–19 LPs are particles composed of an aqueous core limited by a membrane-like lipid bilayer that can be used as carriers for water-soluble, lipid-soluble, and amphiphilic drugs.20–23 Different studies have reported the efficacy of liposomal formulations for drug transport into the ocular posterior segment delivered by IVTs.24–27
Recently, a topical ophthalmic triamcinolone acetonide-loaded liposome formulation (TA-LF) was designed to release triamcinolone acetonide (TA) into the vitreous and retina. The efficiency of this drug delivery nanosystem was successfully tested in rabbits, 28 while its safety profile and therapeutic activity were clearly verified in patients with refractory pseudophakic cystoid ME. 29 Therefore, topical TA-LF may be a potential substitute for intravitreal steroids. However, it is necessary to demonstrate its therapeutic properties in diverse posterior segment disorders to confirm its effectiveness and safety.
Branch retinal vein occlusion (BRVO) represents a common cause of vascular disease in the posterior segment of the eyeball with a prevalence of 4.42 per 1,000.30,31 The clinical relevance of BRVO is that it usually impairs visual function permanently. 32 The leading cause of impaired vision in patients with BRVO is ME and occurs in ∼30% of BRVO cases. 33 Presumably, this phenomenon results from the breaking of the blood–retinal barrier induced mainly by the secretion of VEGF into the vitreous,34–40 along with other cytokines and soluble receptors such as placental growth factor (PIGF), interleukins (ILs) 6, 8, 12, and 13, platelet-derived growth factor-AA, soluble intercellular adhesion molecule-1 (sICAM-1), aqueous angiopoietin-like 4 (ANGPTL4), monocyte chemoattractant protein-1 (MCP-1), soluble vascular endothelial growth factor receptor-1 (sVEGFR)-1, and sVEGFR-2.40–45
Treatment options for ME secondary to BRVO include macular grid laser photocoagulation and IVTs of steroids or anti-VEGF molecules.34,46,47 Because multiple cytokines are associated with the pathogenesis of the ME secondary to BRVO, the broad therapeutic spectrum of steroid is desirable. Previous studies have demonstrated that 2 IVTs of TA (TA-IVTs) 2 months apart are effective for ME secondary to BRVO. 48 This therapeutic success seems to be associated with the anti-inflammatory and antiangiogenic properties of TA such as downregulation of VEGF, IL-6, ICAM-1, and MCP-1.49,50 However, the use of TA-IVTs is linked to severe adverse events (AEs) some of them related to IVTs and others associated with the drug itself, such as increased intraocular pressure (IOP) and cataract progression.51–57 In consequence, the use of anti-VEGF agents as primary therapy prevails over steroids in BRVO.34,46,47
To take advantage of the biological activity of steroids for the treatment of ME secondary to BRVO, but avoiding the risks of TA-IVTs, we explore the therapeutic efficacy and safety of topical TA-LF, as primary therapy in patients with ME secondary to nonischemic BRVO. In addition, we report the electronic microscopic characterization of TA-LF.
Methods
Preparation of liposomal formulation
The LPs in TA-LF were provided by OPKO Health, Inc. (Guadalajara, Jalisco, Mexico). The preparation of TA-LF was performed in Good Manufacturing Practice facilities and was carried out as previously described. 28 In summary, self-forming and thermodynamically stable TA loaded LPs (QuSomes®) were created spontaneously upon adding polyethylene glycol (PEG-12) glyceryl dimyristate into an aqueous solution containing TA. Sterility of the formulation was guaranteed by mixing the excipients of the formulation at 121°C for 15 min and filtration of buffers and water containing TA through membranes of 0.22 mm pore size under aseptic conditions. The resulting formulation possesses a pH of 5.8, viscosity of 70 cP, and osmolarity of 334 mOsm/L. The composition of TA-LF is described in Table 1. Final TA concentration in the resultant dispersion was 2 mg/mL (0.2%). 28
Triamcinolone Acetonide Loaded Liposome Formulation Composition
PEG-12, polyethylene glycol.
Microscopic characterization
Morphology of TA in aqueous solution of TA loaded LPs was assessed through scanning electron microscopy (SEM) and also transmission electron microscopy (TEM). Aqueous solutions of TA were prepared adding ultrapure water (UPW) to the required quantity of TA crystals (TA+UPW) to achieve the concentrations of 0.2%, 0.4%, 1.0%, and 1.4%. Emulsions of TA loaded LPs (TA+LF) were produced varying the quantity of TA crystals in the formulation described in Table 1 to reach the concentration of the active ingredient (0.2%, 0.4%, 1.0%, and 1.4%, respectively). The formulation used in the trial (TA-LF) corresponds to the TA-loaded LP formulation of 0.2% (TA+LF 0.2%). For SEM analysis, a TESCAN MIRA3 LMU FE-SEM device was used (Tescan Orsay Holding, a.s., Brno-Kohoutovice, Czech Republic), while for TEM studies a JEOL JEM-1010 electron microscope was used (Jeol USA, Peabody, MA). SEM samples were kept at −4°C before being mounted onto stubs and gold-coated using a Denton Vacuum Desk II sputter coater. TEM samples were previously treated using phosphotungstic acid as negative staining agent in a 1:1 dilution (v/v) and were deposited onto FF 300 square mesh copper grids for observation. Manual counting and measurement of particles were performed using SEM micrographs at a view field of 63.6 μm to calculate the size and distribution of LPs.
Study design
To evaluate preliminary safety and efficacy of a topical TA-LF in ME secondary to BRVO patients, a single-center prospective pilot study was conducted in patients with diagnosis of nonischemic BRVO at a private-based retina specialty center in Guadalajara, Mexico (Centro de Retina Medica y Quirurgica, SC). The study observed the tenets of the Declaration of Helsinki and received approval by the Ministry of Health. Before enrollment, all patients delivered written informed consent agreeing to participate following explanation of the study and its objectives.
Patients
Patients 18 years of age or older with ME secondary to nonischemic BRVO with a best corrected visual acuity (BCVA) worse than 20/80 were enrolled. Patients with macular ischemia >1 mm2 determined by fluorescein angiography (FA) were excluded since these patients required IVT of anti-VEGF agents, steroids, or laser as primary therapy. Patients with venous stasis retinopathy or hemi-central retinal vein occlusion, diabetic maculopathy and/or retinopathy, age-related macular degeneration, or advanced glaucoma were also excluded from the study. Additional exclusion criteria were medical history of myocardial infarction and/or stroke within 6 months before recruitment, any prior intravitreal anti-VEGF or corticosteroid injections, and any prior laser treatment. FA was performed at baseline to confirm ME in all cases. Written informed consent was obtained after full explanation of the nature and possible AEs of the study. One to three days before the beginning of the TA-LF therapy, demographics and baseline clinical examinations were obtained for the enrolled patients. The 2 mg/mL (0.2%) concentration was established according to the data obtained from the pharmacokinetic study. 28 Included subjects applied 1 drop of TALF 6 times a day, for 12 weeks in the study eye (the eye with ME secondary to nonischemic BRVO). Compliance of the patient to the TALF therapy was evaluated through a patient care journal as follows: AD = (RA)100/IA; where AD is adherence, RA corresponds to the registered applications, and IA represents the indicated number of applications. A value of adherence <80% was considered as compliance failure, and in that case, the patient was excluded from the statistical analysis.
Efficacy assessment
To assess the efficiency of TA-LF in ME secondary to BRVO, we evaluated the central foveal thickness (CFT) and BCVA in the study and the fellow eyes of patients for 12 weeks. BCVA was measured with the Early Treatment Diabetic Retinopathy Study (ETDRS) chart at 4 m, and the average CFT was measured by retinal optical coherence tomography (OCT) (Cirrus OCT Carl Zeiss, Meditec, Dublin, CA). Patients were evaluated every week throughout the first month and every 2 weeks for the rest of the follow-up. To identify AEs, at each visit, a slit lamp anterior and posterior segment evaluations were performed, and the IOP was recorded.
Safety assessment
To assess safety, any ocular and nonocular AEs or any serious AEs were recorded whether informed by enrolled patients, determined by study site personnel, or other means. In the case of any evidence of low tolerability or any AEs, such as ocular surface problems (ie, corneal ulcers, opacities, epithelial defects, conjunctival and/or episcleral injection) and anterior chamber inflammation (cell/flare) related to the TA-LF, patients were removed from the study. Based on the MedDRA Coding dictionary version 18.1, AEs were assigned using standard code terms.
Rescue treatment
Rescue treatment with IVTs of ranibizumab 0.5 mg (Lucentis®; Novartis Farmacéutica, S.A. de C.V., Ciudad de Mexico, Mexico) was considered if persistent or recurrent ME was evident at any visit during the follow-up. If the registered IOP was ≥22 or >4 mmHg compared with the fellow eye, IOP lowering drugs were contemplated.
Statistical analysis
To examine the obtained data, we used the SPSS 22.0 software IBM SPSS Statistics for Macintosh, Version 22.0 (IBM Corp, Armonk, NY). Quantitative variables are presented as means ± standard deviations of the mean (except average particle size that is presented as mean ± standard error), while qualitative variables were described using frequencies and percentages. For the analysis of BCVA, CFT, and IOP, a Friedman test of repeated measures was performed. Significance was defined as a P value <0.05.
Results
Twelve eyes of 12 patients with ME secondary to BRVO were included. Mean age of participants was 69.41 ± 8.79 years. The male:female ratio was 7:5. Seven out of 12 studied eyes were right and 5 were left. Twenty-five percent of the included eyes had their natural lens. Seventy-five percent of the occlusions occurred in the temporal superior vein area. In contrast, none of the fellow eyes had glaucoma or retinal abnormalities. Of the fellow eyes, 99.66% had intraocular lenses. Notably, all 12 patients had hypertension (HTN). Subjects' demographics and characteristics are recapitulated in Table 2.
Demographics and Clinical Characteristics of Patients with Macular Edema Secondary to Branch Retinal Vein Occlusion Treated with Triamcinolone Acetonide-Loaded Liposome Formulation
BRVO, branch retinal vein occlusion; DM, diabetes mellitus; F, female; HTN, hypertension; M, male; ME, macular edema; OD, right eye; OS, left eye; TA-LF, triamcinolone acetonide-loaded liposome formulation; TI, temporal inferior; TS, temporal superior.
Regarding tolerability and safety, TA-LF was well tolerated, and neither ocular nor systemic AE was reported. While using TA-LF, none of the subjects needed IOP lowering drugs, and no one presented corneal opacities, epithelial defects, anterior chamber inflammation, or conjunctival/episcleral injection. Remarkably, nonsignificant variations in IOP were recorded between the study and the fellow eyes, supporting the presumable safety of TA-LF (Fig. 2).
Related to efficacy, we found that TA-LF showed a presumable suitable therapeutic activity in ME secondary to BRVO patients. Demonstrative OCT images of all 12 patients are presented in Fig. 1. All included patients reduced their CFT and increased the number of ETDRS letters significantly from week 8 and continued until week 12 without rise in their IOP. The follow-up points where statistically significant variations were observed are presented in Fig. 2 and in Table 3. CFT changed from 682.91 ± 278.60 at baseline to 271.58 ± 57.66 μm, after 12 weeks of TA-LF therapy. Notably, CFT value was nonstatistically different between the fellow and the study eyes at week 12; 270.67 ± 14.92 versus 271.58 ± 57.66 μm, respectively (Fig. 2). Meanwhile, the BCVA changed from 40 ± 12.05 at baseline to 64.83 ± 15.97 ETDRS letters, after 12 weeks of TA-LF application. As expected, nonsignificant modifications in BCVA and CFT values were registered in the fellow eyes (Fig. 2). Importantly, none of the patients needed rescue treatment.
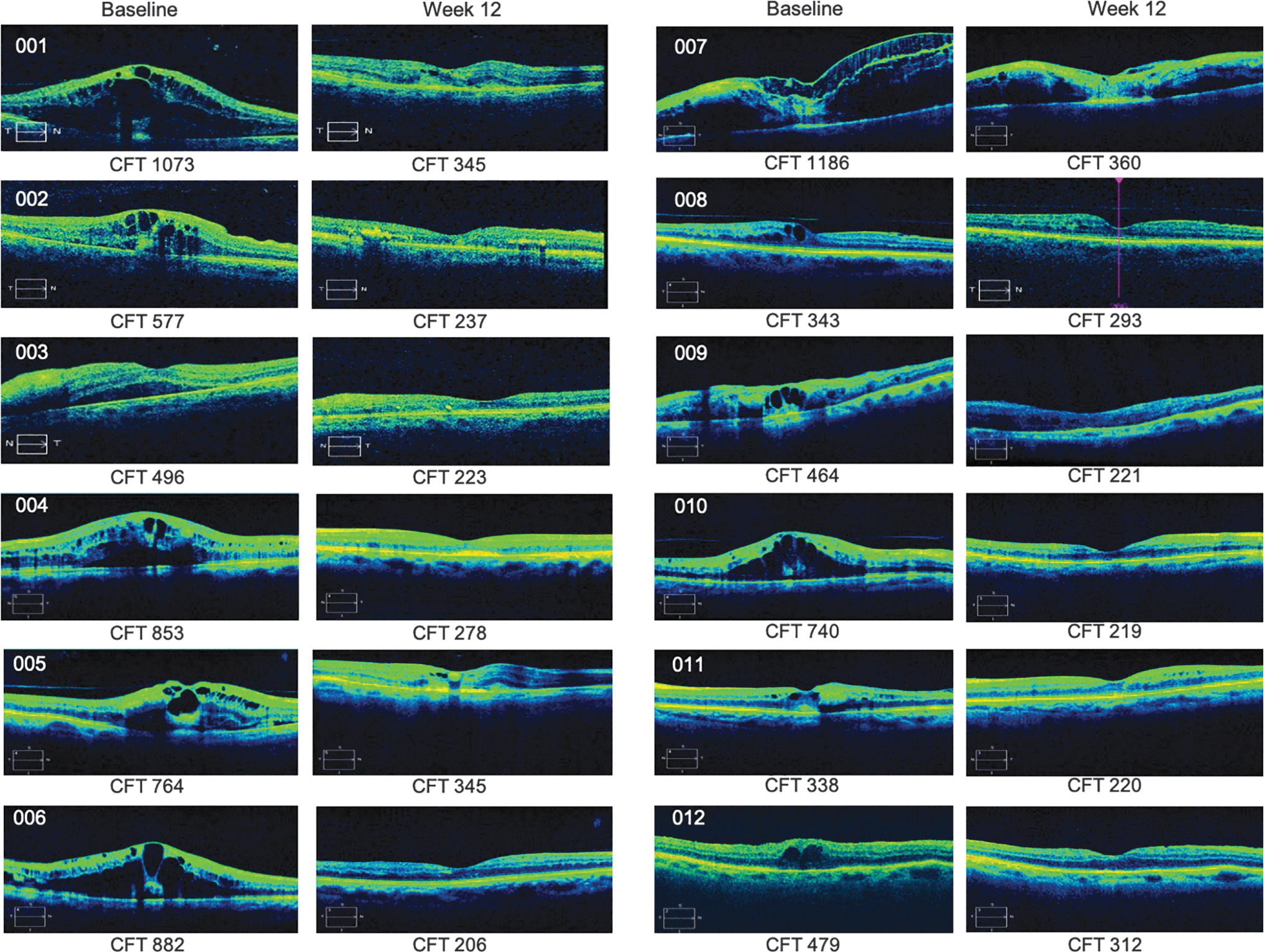
OCT images before and after 12 weeks of TA-LF therapy. The figure is composed of representative retinal OCT images of all cases of ME secondary to BRVO before and after 12 weeks of topical TA-LF therapy. Measure of CFT is presented in μm. BRVO, branch retinal vein occlusion; CFT, central foveal thickness; ME, macular edema; OCT, optical coherence tomography; TA-LF, triamcinolone acetonide-loaded liposome formulation.
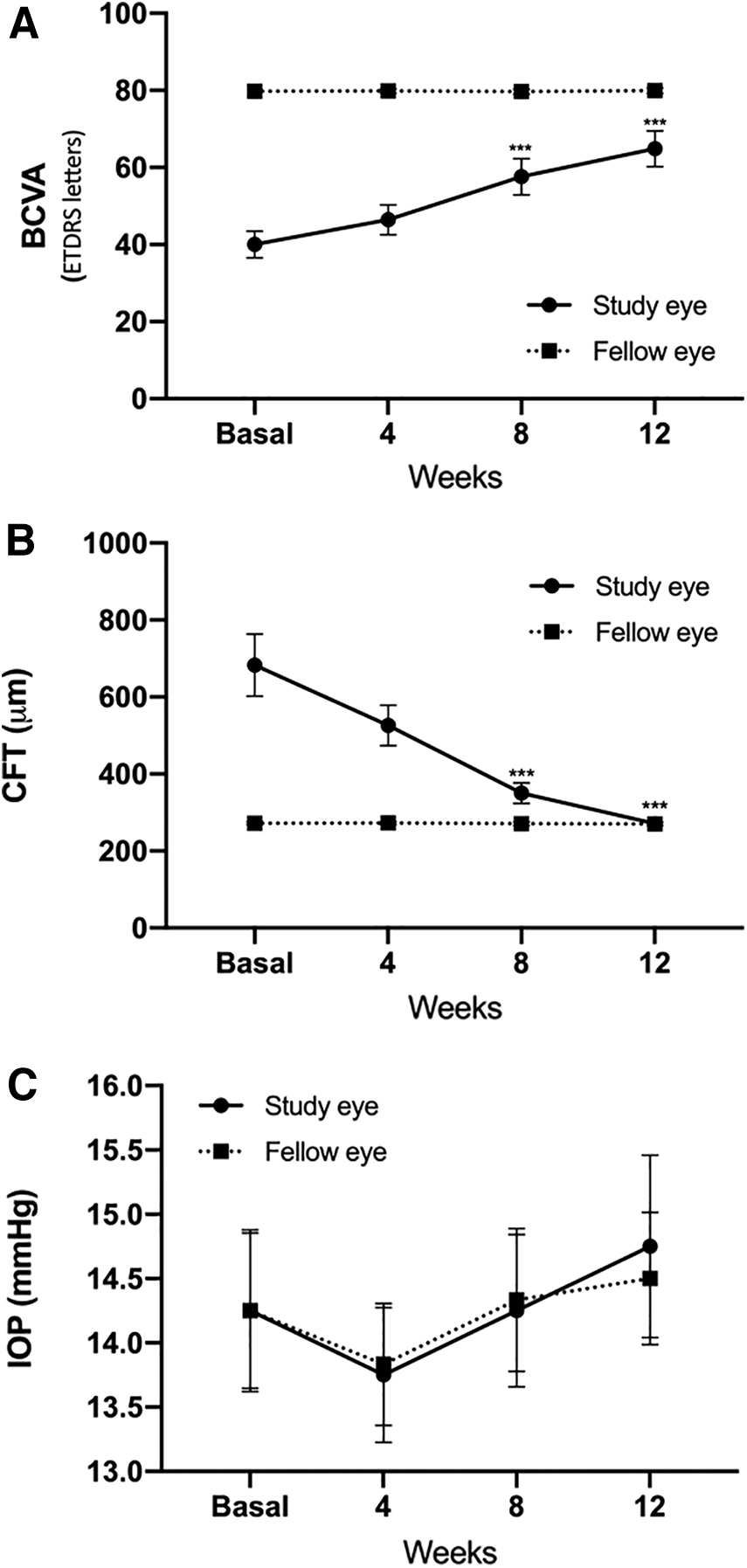
Variations in CFT, BCVA, and IOP during follow-up of TA-LF therapy in the study and fellow eyes of patients with ME secondary to BRVO.
Variations in Best Corrected Visual Acuity, Central Foveal Thickness, and Intraocular Pressure of Patients with Macular Edema Secondary to Branch Retinal Vein Occlusion Throughout Triamcinolone Acetonide-Loaded Liposome Formulation Therapy
No statistically significant differences from baseline values (P > 0.05).
Statistically significant differences from baseline values (P < 0.05),
BCVA, best corrected visual acuity; CFT, central foveal thickness; ETDRS, Early Treatment Diabetic Retinopathy Study; IOP, intraocular pressure.
Finally, microscopic observation of TA LP formulations revealed interesting findings. On one hand, SEM analysis showed that LPs' size depends on the concentration of TA in the LP formulation. As the concentration of TA increased, the average size of LPs and the number of particles with a diameter >1,000 nm increased as well (Fig. 3 and Table 4). For example, TA+LF 0.2% (the formulation used in this pilot study) presented an average particle size of 147 ± 6 nm with 0% of particles superior than 1,000 nm, whereas TA+LF 1.4% showed an average particle size of 1,443 ± 71 nm with 53% of particles greater than 1,000 nm (Table 4). On the other hand, TEM study displayed that the LP formulation is able to solubilize large TA crystals into nanoparticles and encapsulate them at the same time (Fig. 4).

Liposomal encapsulation depends on concentration of TA.
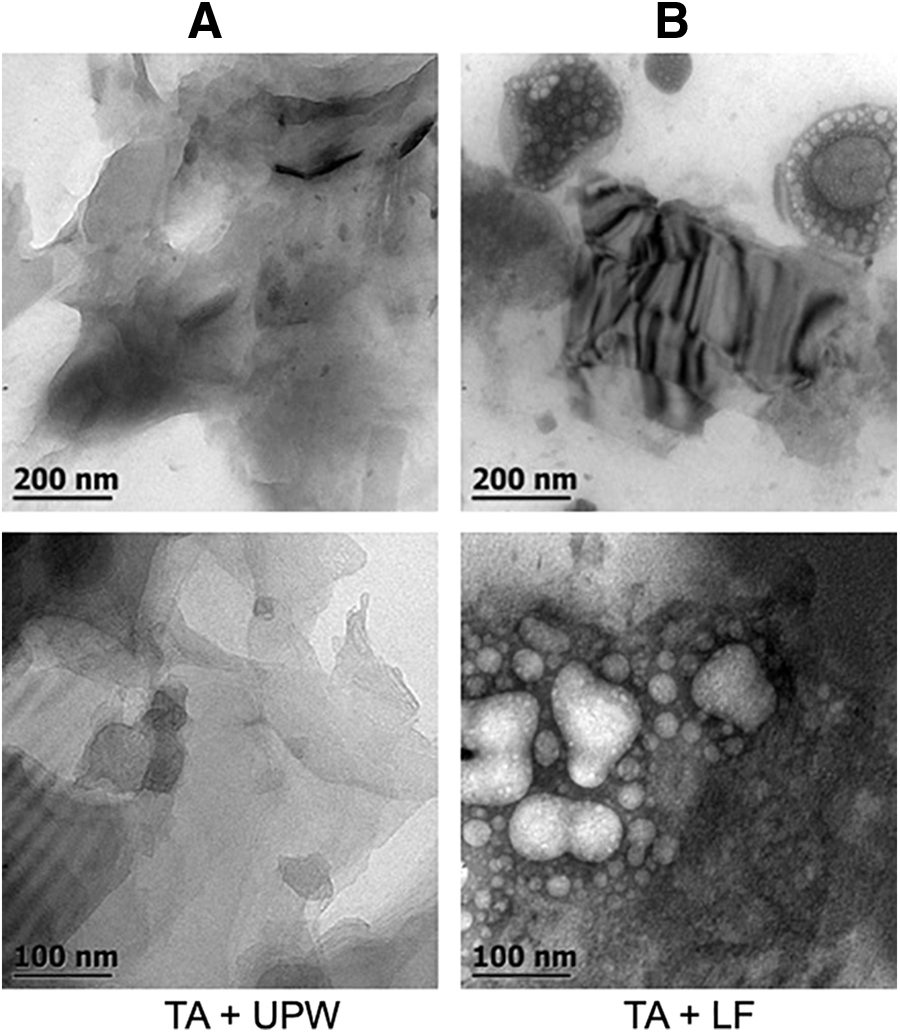
Liposomes function as nanocarriers of TA. TEM images of TA crystals in aqueous solution composed by TA and UPW
Number of Particles and Particle Size Obtained from Scanning Electron Microscopy Micrographs of Triamcinolone Acetonide-Loaded Liposome Formulations
Discussion
Currently, intravitreal anti-VEGF therapy is the gold standard treatment for ME in vein occlusions.58,59 Nevertheless, single injection of anti-VEGF agents only provides temporary relief of ME so repeated injections are required, increasing the risk of severe AEs related to IVTs, which might lead to retinal atrophy due to blockage of neuroprotective cytokines and the regression of the natural vasculature.60,61 Another available option is IVTs of corticosteroids, especially TA, which is used when the cost of the monthly treatment with anti-VEGF drugs is problematic for patients. 53 TA-IVTs have comparable or even better short-term results in nonischemic BRVO than IVTs of anti-VEGF agents, 48 but the rate of ocular AEs is even greater than the rate of AEs for intravitreal anti-VEGF agents.51,52,54–57,62
With the purpose of developing a safer and more effective platform to deliver steroids into the posterior segment of the eyeball, different nanomedicine initiatives have been reported; however, only a few have reached the clinical phase. One of them is using cyclodextrins (CDs) as nanocarriers of dexamethasone (Dex). CDs are a family of natural cyclic oligosaccharides usually composed of no >20 α-D-glucopyranoside units through covalent conjugation of α-1,4-glycosidic linkages. CDs show a cyclic structure with a hydrophilic outer surface and a lipophilic internal cavity of low polarity that form inclusion complexes with poorly water-soluble chemicals. 63 In the preclinical study of Loftsson et al., 64 inclusion complexes of Dex and γ-CD were able to deliver Dex in the vitreous and retina of rabbits when they are administered topically. This finding allowed the same group to perform a clinical trial to prove the efficiency of a topical 1.5% Dexγ-CD nanoparticle eye drops (DexNP) in diabetic ME. Topical DexNP significantly improve visual acuity and decrease macular thickness with a comparable efficiency of subtenon TA. However, a modest increase in IOP was seen with DexNP, but IOP normalized after the discontinuation of the eye drops. 65
In contrast, LPs are nanoparticles that have been successfully used in topical ophthalmic formulations to carry TA and deliver it into retina and vitreous of rabbits.28,66 Due to this finding, TA-LF has been successfully proved in Phase II clinical assays, where its efficiency and safety profile have been satisfactorily demonstrated in the management of refractory pseudophakic cystoid ME. 29
In the present study, our group explored the efficacy and safety of TA-LF in subjects with ME resulting from nonischemic BRVO. We observed that TA-LF therapy was related to BCVA improvement and CFT reduction in absence of AEs. The treated eyes showed BCVA improvement from 40 ± 12.05 to 64.83 ± 15.97 ETDRS letters and CFT reduction from 682.91 ± 278.60 to 271.58 ± 57.66 μm after 12 weeks of TA-LF therapy. It is essential to emphasize that in some patients the association between CFT and BCVA was weak. Nevertheless, it has been widely described that variations in BCVA and CFT are weakly associated irrespective of the underlying disease.67–70 Remarkably, no AEs, including IOP rising, were reported in our series. It is possible that smaller amounts of steroids delivered by LP, compared to the quantities released by TA-IVT and Dex implant, prevent the IOP rise. The TA concentration achieved by IVT in rabbits is 14434.0 ± 10,768 μg/L 71 versus 252.10 ± 90.00 ng/g by the TA-LF topical application in rabbits. 28
Therefore, these preliminary findings support the efficiency and safety profile of TA-LF in patients with ME secondary to nonischemic BRVO. Consequently, TA-LF might be not only an efficient option, but additionally a safer method than IVTs of steroids to treat ME because topical formulations do not have the potential hazards associated with IVTs. Nonetheless, more studies are needed to verify this assertion.
Notably, all subjects included in this trial were elderly and hypertensive patients. Advancing age is an important risk factor for BRVO since the main pathogenic mechanism of BRVO is arterial stiffness that causes venous compression in the common adventitial sheath. 72 Therefore, it is not surprising that the mean age of the enrolled participants was 69.41 ± 8.79 years. In contrast, systemic vascular diseases, such as HTN, hyperlipidemia, and peripheral arterial disease, are related to BRVO. In fact, the reported odds ratio for HTN is 3.073; this factor seems to be determinant for the increased risk of BRVO; also those with more severe HTN were at even greater risk of BRVO. 74 Therefore, it is not unexpected that the patients of our series have HTN. It is important to emphasize that the subjects in our study were medicated with angiotensin II receptor type 1 antagonist and nonselective beta blockers. Interestingly, these groups of drugs have been related to VEGF-A downregulation (the main cytokine involved in the pathophysiology of ME secondary to BRVO). Although candesartan reduced the expression of VEGF-A and its intracellular signaling,75,76 and limits VEGF receptor-2 expression, 77 the evidence was collected in cell cultures or in animal models using high doses and parenteral administration. Nonselective beta blockers, such as propranolol, have been reported to inhibit retinal neovascularization and reducing VEGF expression in oxygen-induced retinopathy of premature animal models78,79; however, these findings have not been consistent. 80 At this time, the anti-VEGF activity of candesartan or propranolol has not been demonstrated in a clinical trial. Therefore, it is unlikely that the antihypertensive drugs taken by our patients could have modified the course of the BRVO event.
In this study, the microscopic characterization of TA-LF was of major importance because it allowed to establish features of the TA encapsulation process and to determine characteristics of the nanoparticle. It is important to mention that TA has a molecular weight of 434.49 g/mol; it is insoluble in water (8 mg/100 mL at 25°C) and partially soluble in ethanol (500 mg/100 mL at 28°C). TA has a logP value of 2.53, which is considered lipophilic according to the partition coefficient scale; however, it is partially soluble in vegetable oils but insoluble in mineral oils. 81 As a consequence of its lipophilic nature, TA crystals were only partially solubilized in water as it can be observed in all SEM images. Due to its lipophilic character, TA is solubilized in the “Lipids solution of liposomes formulation” that contains ethanol. Therefore, as TA concentration increases, a higher amount of solubilized-TA is present in the lipidic medium. This is the reason why as the concentration of TA increased, the greater the size and number of LP were observed. After the LP formation using homogenization, small-sized TA crystals are trapped into the LPs' aqueous core enclosed by 1 or more phospholipid bilayers or lamellae as observed in TEM images. 82
Finally, we are aware that our study has some limitations. Foremost, the absence of a control group and the fact that patients with ME secondary to BRVO can improve across time even without treatment. However, the median time for ME to resolve is 21 months in cases with major BRVO (like the patients included in this study) and 18 months in cases with macular BRVO. 83 Therefore, it is unlikely that the improvement observed in our patients was the result of the natural course of the disease, since the statistically significant improvement in CFT and BCVA rose at week 8 of the treatment. Besides, we used the cohort of BCVA worse than 20/80 as selection criteria to limit the effect of spontaneous resolution of the ME. It has been reported that in eyes with initial visual acuity (VA) of 20/60 or better, 75% had improved or stable VA, whereas in eyes with initial VA of 20/70 or worse, 69% had improved VA. 84 In addition, we evaluate adherence to TA-LF therapy with the purpose of evaluating compliance and reducing the effect of missing applications in the observed findings. The second main limitation is the sample size. Although our study sample is small, it was possible to observe the clinical and anatomical associations described for BRVO. For example, as we previously mentioned all patients had history of HTN at the time of the occlusion, and in 75% of the cases, the occlusion occurred in the superior temporal retinal vein. It has been well described in the literature that most of the cases of BRVO (65%) happen in the temporal superior quadrant because of the presence of more arteriovenous crossing at this site.85,86 Nevertheless, additional studies with longer follow-up periods and bigger sample size are needed.
In conclusion, we have presented topical ophthalmic LPs as nanocarriers of TA as primary therapy for patients with ME secondary to BRVO. Our results indicate that topical applied TA-LF might be as efficient as intravitreal anti-VEGF drugs and steroids for the treatment of patients with BRVO and has the potential to replace IVTs of steroids. Our findings support the role of LPs as an emerging nanocarrier platform for posterior pole diseases. However, larger trials are required to evaluate long-term safety and efficacy profile of this nanoparticle.
Footnotes
Acknowledgment
The authors want to thank Ma. de Lourdes Palma-Tirado at Instituto de Neurobiologia, UNAM for her technical support during this work.
Author Disclosure Statement
This research is sponsored by Centro de Retina Medica y Quirurgica S.C. and may lead to the development of products.
Funding Information
No funding was received for this article.