
Abstract
Purpose:
The objective of this study was to describe the short-term results of allogenic transplantation of limbal stem cells expanded on amniotic membrane for the ocular surface reconstruction.
Methods:
Prospective nonrandomized, nonmasked study in a single ophthalmological center. Ten patients with bilateral total limbal stem cell deficiency (LSCD) were included. Expression and presence of ABCB5 and Δp63α in amniotic membrane-cultured limbal epithelial stem cells were analyzed, in relationship with clinical changes after allogenic transplantation. An objective evaluation was performed to determine corneal transparency and superficial vascularization.
Results:
In a median follow-up time of 11.6 months, 7 patients (70%) were considered as failure compared with the preoperative status. ABCB5 and Δp63α are expressed in similar amount in the limbal epithelial cells expanded in vitro and transplanted in patients with bilateral LSCD.
Conclusions:
Transplantation of allogenic epithelial limbal cells expanded in amniotic membrane could be considered in patients with LSCD due to burns or congenital etiologies such as aniridia, but its benefit is limited for patients with immunologic diseases.
Introduction
The ocular surface is a complex structure, essential for the conservation of vision. The limbus is an anatomical transition zone between the cornea and the conjunctiva; the preservation of this structure is fundamental to avoid corneal conjunctivalization. The limbus contains a high number of mature and immature dendritic cells, T-lymphocytes, highly pigmented melanocytes, and blood vessels and in its basal layer, the less differentiated cells in the cornea. 1 The stem cells located in the limbal epithelial crypts are small, with a cubic structure; these cells centripetally migrate and differentiate into the corneal epithelium. 2 An affected limbus generates an unstable ocular surface, causing corneal conjunctivalization and vascularization, with stromal opacities and vision loss.3,4 Limbal stem cell deficiency (LSCD) causes include chemical and thermal burns, Stevens-Johnson syndrome (SJS), cicatricial ocular pemphigoid, pemphigus, iatrogenic, neoplasia, and the use of contact lenses among many others.5–7 Although rare, there are also some congenital etiologies causing LSCD, including aniridia, ectodermal dysplasia, and sclerocornea. 8 LSCD diagnosis is mainly clinical and confirmed with impression cytology and in vivo confocal microscopy.6,9
The first report of in vitro expansion of autologous limbal stem cells to treat LSCD goes back more than 20 years ago, in which the cells were obtained from a limbal biopsy of the healthy contralateral eye and cultured on a therapeutic contact lens. 10 After this report, some substrates have been used, including fibrin and amniotic membrane.11,12 The treatment for LSCD using cultivated autologous limbal cells on fibrin resulted in more than 70% of effectiveness according to some long-term follow-up studies.11,13 However, clinical success is very complex to determine because it depends on many factors such as the growing media, the donor eye quality, and the receptor microenvironment. 14
The use of limbal explants in the cultured cells influences the preservation of the stem cell markers. 15 The absence of a definitive limbal stem cell marker has contributed to the identification of various markers and their association with the clinical result after transplantation, and this is the case of the Δp63α transcription factor. The stem cells located in the limbus are characterized by the expression of the Δp63α nuclear transcription factor, which expression is exclusively in the epithelial basal cell of the limbus. 16 The high expression of this molecule in more than 3% of the epithelial limbal stem cells is associated with a successful outcome of up to 70% of cases, while a low expression in less than 3% of cells is associated with only 11% successful long-term outcome. 14 Up to date, there is no specific molecular marker to identify and isolate the limbal stem cells.
The ABCB5 protein presence has been observed in subpopulations of multiple cancer or tumor stem cells, including melanoma, breast cancer, hepatic cancer, colorectal cancer, and oral squamous carcinoma. 17 In the eye, it has been reported that ABCB5 presence is highly elevated in the ocular surface squamous neoplasia, suggesting that this protein might be involved in its pathogenesis. 17 Also, a murine model study in conjunctival melanoma demonstrated the presence of ABCB5 in different stages of the tumor development, as well as its role in the metastatic potential of the tumor. 18 It has been described that ABCB5 is coexpressed with Δp63α in the cells of the limbal basal epithelium, and it was proposed as a possible marker in the follow-up of the limbal cell transplantation. 19 Also, ABCB5 was shown as a unique molecular marker allowing the prospective isolation of limbal stem cell populations from human tissue, with the exclusive capacity to completely restore the cornea in preclinical models of LSCD. 20 Besides, in ABCB5 knockout mice, a defective corneal differentiation was found, including increased corneal fragility, reduced corneal cellularity, and decreased expression of corneal differentiation markers, such as PAX6 and KRT12, revealing an essential function in the normal corneal development. 19
The objective of this study is to describe the short-term results of allogenic transplantation of limbal stem cells expanded on amniotic membrane for the ocular surface reconstruction in patients with bilateral LSCD, as well as to analyze the expression and presence of ABCB5 and Δp63α in amniotic membrane cultured limbal epithelial stem cells.
Methods
Patients
All the methods and experimental protocols were carried out in accordance to the Ethical Review Board (ERB) from the Institute of Ophthalmology Conde de Valenciana and the study was performed with adherence to the tenets of the Declaration of Helsinki. The informed consent was obtained from all the patients and caregivers involved in the present study. This study has been registered at ClinicalTrials.gov with the number NCT02579993. This is a nonrandomized, nonmasked study with at least 3 months of follow-up. Patients were assessed in the Cornea and Refractive Surgery Department at the Instituto de Oftalmologia “Conde de Valenciana.” Patients with severe bilateral LSCD of any etiology were included in the present study. All the eyes were positive to periodic acid-Schiff (PAS)-stained cells in the impression cytology; also, rounding reflective cells corresponding to goblet cells were identified by in vivo confocal microscopy. All the patients included presented normal B-mode ultrasound scanning and visual evoked potential. Patients with an active ocular immunologic or infectious disease were excluded from the study.
LSCD diagnosis
LSCD was diagnosed clinically by signs and symptoms, which were recurrent epithelial defects and superficial vascularization, conjunctivalization of the corneal surface, and presence of a fibrovascular pannus; also, the presence of goblet cells in the corneal surface with absence or decrease in the epithelial corneal cells was suggestive for LSCD. In vivo confocal microscopy was performed according to Shortt et al. and this and the impression cytology were reported as presence of epithelial cells, conjunctival cells, or mixed. 21
Reagents
Dulbecco's modified Eagle medium/nutrient mixture F-12 (DMEM-F12), dimethyl sulfoxide (DMSO), hydrocortisone, cholera toxin A subunit, 2-(4-Amidinophenyl)-6-indolecarbamidine dihydrochloride (DAPI), KAPPA SYBR FAST One-Step kit, and para-formaldehyde (PFA) were purchased from Sigma-Aldrich (St. Louis, MO). Phosphate-buffered saline (PBS), dispase II, gentamycin, penicillin-streptomycin, gamma-irradiated fetal bovine serum (FBS), recombinant human Epidermal Growth Factor (EGF), insulin–transferrin-sodium selenite (ITS) supplement, and trypsin were obtained from Thermo Fisher Scientific (Waltham, MA). Cytofix/cytoperm and Perm/Wash reagents were obtained from BD Biosciences (San Jose, CA). RNeasy Mini Kit was purchased from Qiagen (Hilden, Germany). Primers sequences for β2 microglobulin (b2m forward 5′-CAC CCC CAC TGA AAA AGA TG-3′ and reverse 5′-ATA TTA AAA AGC AAG CAA GCA-3′), Δp63α (forward 5′-GGA AAA CAA TGC CCA GAC TC-3′ and reverse 5′-CAC AGT TTC GAC GTG TCC TTC-3′) and abcb5 (forward 5′-GAC CAA GGC GAC TGT CTC TC-3′ and reverse 5′-TTG AAA CCT TCG CAA TAG CC-3′) were obtained from IDT (San Jose, CA). Mouse monoclonal anti-human ABCB5 was obtained from Abcam (Cambridge, UK); purified polyclonal rabbit anti-human p63 (ΔN) was obtained from BioLegend (San Diego, CA). Donkey anti-rabbit Alexa Fluor 488 and goat anti-mouse Alexa Fluor 594 were from Thermo Fisher Technologies (Walthman, MA). Polytetrafluoroethylene (PTFE) membrane was obtained from Millipore (Darmstadt, Germany).
In vitro limbal stem cells expanded on amniotic membrane
Amniotic tissue was obtained from the Instituto de Oftalmologia Conde de Valenciana Amnion Bank. Amniotic membrane was thawed at room temperature (RT), washed 3 times in PBS to eliminate the residual glycerol, and deepithelialized using enzymatic technique with dispase II at a concentration of 1.2 IU/mL. The epithelium was removed with cotton swabs and verified in inverted microscope for complete deepithelialization; amniotic membranes were then placed on glass slides with the epithelial basement side-up. The amniotic membrane fragments were placed in a 6-well plate.
Culture of limbal epithelial cells
Corneoscleral rims were obtained from cadaveric donor corneas. The conjunctiva, Tenon's capsule, iris, and endothelium were carefully removed with a blade. The remaining tissue was incubated in 1.2 IU/mL of dispase II for 30 min. Limbal explants were placed epithelial side-up in the center of deepithelialized amniotic membrane. To allow the adhesion of the limbal explant on the amniotic membrane, 25 μL of decomplemented gamma-irradiated FBS were added and incubated overnight. Three milliliters of supplemented DMEM-F12 medium [FBS (5%), DMSO (0.5%), EGF (2 ng/mL), cholera toxin A subunit (30 ng/mL), insulin (5 μg/mL), transferrin (2.5 μg/mL), sodium selenite (6 ng/mL),and gentamycin (40 μg/mL)] were added and incubated at 37°C, 5% CO2, and 95% humidity. Six grafts were prepared for each assay, changing the medium every other day with evaluation of the cellular growth under an inverted microscope during 3 weeks until the formation of a uniform cellular layer.
Flow cytometry profiles of ABCB5 and Δp63α
The limbal epithelial cells that grew on amniotic membrane were obtained with trypsinization digestion. In brief, the graft was washed 3 times with PBS and incubated with trypsin-EDTA solution 0.25%. The cells were obtained and centrifuged at 300 g for 5 min at 4°C and fixed and permeabilized for 20 min. The cells were then stained with the primary antibodies, the excess was washed and finally the cells were stained with fluorochrome-conjugated secondary antibodies. All the samples were obtained in a FACSCalibur flow cytometer. Data analysis was performed with the CellQuest Pro software (BD Biosciences).
Reverse transcription polymerase chain reaction (RT-PCR)
For the detection of the specific human gene transcripts, total RNA was isolated from the expanded cells in vitro over amniotic membrane using the RNeasy Mini Kit. Ten nanograms of total RNA were used to amplify b2m, Δp63α, and abcb5.
Immunofluorescence
Immunofluorescence was performed to determine the expression of ABCB5 and Δp63α proteins in the graft. Representative samples were obtained from the expanded cultured limbal stem cells on amniotic membrane. In brief, the grafts samples were fixed with Bouin's solution during 3 h at RT. Then, they were exhaustively washed. The samples were paraffin embedded and transverse sections (5 μm) were performed with a microtome. Antigen retrieval was achieved using citrate solution. Primary antibodies were incubated overnight at 4°C in a wet chamber; afterward, the samples were incubated with fluorochrome-conjugated secondary antibodies for 1 h at RT in darkness. Finally, the samples were mounted with DAPI-VECTASHIELD. The stained samples were observed in an Apotome-II microscope (Carl Zeiss, Jena Germany) and analyzed using AxioVision 2.0 software (Carl Zeiss).
Histological examination
After 3 weeks of culture, the neotissue was evaluated by light microscopy. In brief, the neotissue samples were fixed with Bouin's solution during 3 h at RT. Then, they were exhaustively washed. The samples were paraffin embedded and transverse sections (5 μm) were performed with a microtome and mounted onto glass slides; the samples were hematoxylin and eosin (H&E) stained and observed by direct light microscope. At least 3 random microscopic fields on each independent assay were recorded.
Cellular density
Cellular density analysis was performed with the count of the cell nuclei stained with DAPI. Representative images were taken from 6 different fields from a single uniform layer of epithelial cells expanded in amniotic membrane. Cell count was done by 3 independent investigators and an average was obtained. Images were obtained in a microscope ApoTome.2 Imager.Z2 (Carl Zeiss).
Surgical technique, follow-up, and postoperative care
After a 360° conjunctival peritomy and removal of 2 mm of adjacent bulbar conjunctiva, the abnormal corneal epithelium and fibrovascular pannus were carefully removed. The allogenic cultivated graft was then transferred to the ocular surface, with the stromal side of the graft in contact with the cornea and limbus, and fixed in place with fibrin glue. Another intact amniotic membrane was then placed over the graft and also fixed with fibrin glue. A soft bandage contact lens was placed, followed by topical antibiotic. Patients were followed for inflammation control, infection prophylaxis and detection, and management of rejections. Postoperatively, topical prednisolone acetate 1% was administered 4–6 times a day initially, and then in tapering doses, with topical antibiotic drops for 1 month, and 50% autologous serum eye drops. For systemic immunosuppression, oral prednisone 1 mg/kg/day was also started and gradually tapered; in addition, oral cyclosporine A, 150–200 mg/day for the first 2 months, with posterior reduction to 25–50 mg/day. All patients underwent comprehensive ophthalmic examinations at every follow-up visit, evaluated on day 1, 1, 3, and 6 weeks and every month thereafter. An objective evaluation was performed with a score system from 1+ to 4+ based in slit-lamp photographs to determine corneal transparency and superficial vascularization, considering the preoperative image as 4+. 22 Visual acuity was measured with Snellen or Feinbloom charts, or with the capacity for counting fingers, appreciate hand motion of light perception according to each patient.
Statistical analysis
A descriptive analysis of the assays was performed. Comparison between groups of markers were performed using nonpaired t-test using Stata 13.1 (StataCorp, College Station, TX), with significance considered when P < 0.05.
Results
Preoperative evaluation of patients
Eleven patients were included in this study, from which 10 underwent the expanded limbal stem cell transplantation and 1 patient withdrew his informed consent previous to surgery. Median age was 47 years (range 17–60 years), 6 men and 4 women. Etiologies of the LSCD included chemical burns 3 patients (30%); immunologic (rheumatoid arthritis, ocular cicatricial pemphigoid, and SJS) 3 patients (30%); thermal burn 1 patient (10%); allergic keratoconjunctivitis 1 patient (10%); aniridia 1 patient (10%), and idiopathic 1 patient (10%). Median visual acuity 20/200, logMAR 2.0 (range 20/300, logMAR 1.17 to hand motion, logMAR 3.0). These results are summarized in Table 1. All subjects had a preoperative evaluation showing normal B-mode ultrasound scans and visual evoked potentials. Impression cytology of the ocular surface revealed a mixed pattern, showing presence of both epithelial and mucin producing goblet cells (Fig. 1). In vivo corneal confocal microscopy showed the presence of metaplastic epithelial cells appearing with high reflectivity, cuboidal or polygonal elements with nondefined borders, hyporeflective cytoplasm with barely detectable nuclei, and several roundish reflective cells corresponding to goblet cells (Fig. 1).

Preoperative Evaluation of Patients
AMT, amniotic membrane transplantation; BCVA, best corrected visual acuity; HM, hand motion; LSCD, limbal stem cell deficiency; PK, penetrating keratectomy; RA, rheumatoid arthritis; SJS, Stevens-Johnson syndrome; SLET: simple limbal epithelial transplantation; SS, Sjögren syndrome.
In vitro expansion of limbal epithelial cells in amniotic membrane
Limbal epithelial explants were cultured for 21 days over deepithelialized amniotic membrane (dAM), which served as a scaffold and a stem cell carrier. After 3 days of culture, there was cell clumping establishing colony-forming units. There was an evident growing margin from the explant to the periphery (centrifugally) at day 7 of culture, and at the day 20 of culture, a single-cell layer was obtained covering all the dAM. The predominant morphology of the cells was small with prominent nucleus
All the process was observed in an inverted microscope daily. After 21 days of culture, some specimens were used to perform H&E staining, as well as immunohistochemistry. Interestingly, H&E staining showed that there was a stratified epithelium supported on a dense avascular, acellular connective tissue. Inflammatory cells were not identified in any studied sample. In addition, when 3 independent samples of the human limbal cells were analyzed by flow cytometry, 90% ± 5% were ABCB5+ cells, meanwhile, 85% ± 12% of the cells were Δp63α+; moreover, 80% ± 7% of the cells were positive for both Δp63α and ABCB5 markers. To corroborate that the samples possessed the genetic information to produce the Δp63α and ABCB5 proteins, RT-PCR were performed, showing that all the samples presented the transcript for Δp63α and abcb5 (Fig. 2).
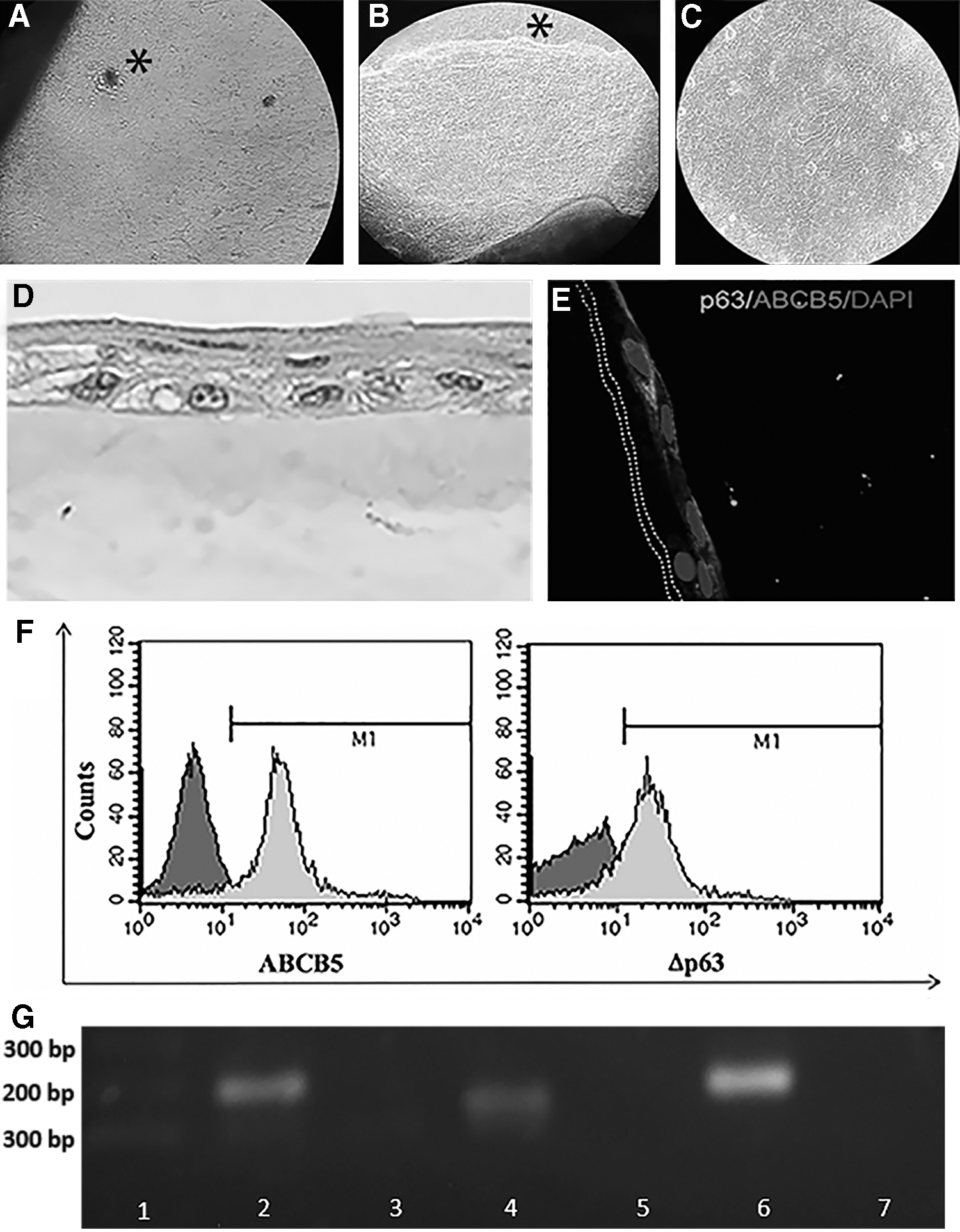
Limbal stem cells cultured on dAM. Explant from a cadaveric sclerocorneal rim attached on dAM. Cell clumps as indicated with an * at day 3 making colony-forming units over dAM
Clinical postoperative results
During the surgical procedures, there were no intraoperative complications. Moreover, no patient presented adverse effect to the topical medication, oral steroids nor systemic ciplosporine A during follow-up. The median follow-up time was 11.6 months (range 3–20 months). Seven patients (70%) were considered as failure and 2 patients (20%) were considered as improvement compared with the preoperative status. In the patients that presented failure, the amniotic membranes remained in situ in all of them, with partial clearance of the ocular surface during the first month after surgery; however, by the end of the first month corneal vascularization started to become evident as the amniotic membrane integrated, and by the second month, corneal conjunctivalization recurrence. In all the patients, the recurrence of the conjunctivalization presented in the same areas existing before surgery; however, in the patients with rheumatoid arthritis, ocular cicatricial pemphigoid and one of the chemical burns, the conjunctivalization involved other areas without preexisting vessels, apparently related to expansion of contiguous conjunctiva. Two patients who presented improvement after surgery, the first with thermal burn showed improvement in the ocular surface, with decrease in the superficial blood vessels and no recurrence of the conjunctivalization and clearance of the central corneal; the second, the patient with congenital aniridia showed and important decrease in the central aniridic keratopathy. Figure 3 shows representative images of patients who presented failure, and the patients who presented improvement, before and after the surgery. Visual acuity remains the same for all of the patients, either for failure of the surgery or for extensive corneal fibrosis that requires penetrating keratoplasty. All the patients reported decrease in ocular pain and photophobia, and by the end of the follow-up, no epithelial defects were evident. One patient (10%) with a chemical burn presented extensive corneal lysis 1 month after the surgery, presenting an extensive corneal perforation and requiring a sclerokeratoplasty to maintain ocular integrity.
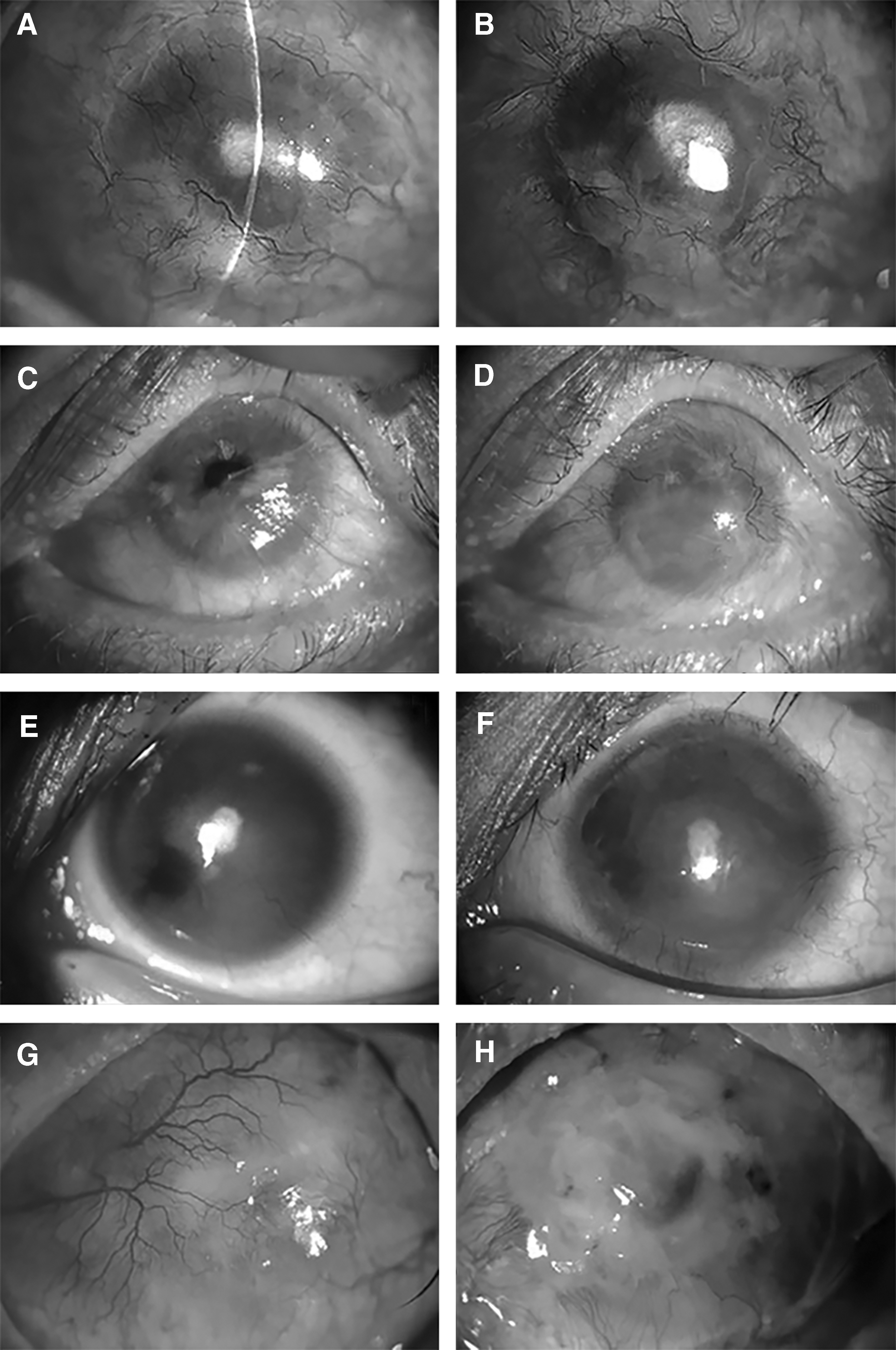
Representative clinical pictures of 2 patients who presented failure
Discussion
Patients included in this study presented diverse etiologies of LSCD. Even when approximately half of the patients had causes related with burns, it must be considered also that other etiologies were present, including SJS, cicatricial ocular pemphigoid, rheumatoid arthritis, and longstanding allergic conjunctivitis among others. With regard to the preoperative evaluation, the diagnostic agreement between the impression cytology and in vivo confocal microscopy has been reported high, being up to 90% in some studies, showing in both diagnostic tests the presence of only corneal epithelium (eyes without LSCD), only conjunctival epithelium (eyes with total LSCD), and a mixed pattern with both corneal and conjunctival epithelium (eyes with partial LSCD). 23 Similar to other series, patients in this study presented in the impression cytology a mixed pattern of corneal and conjunctival goblet cells24,25; and in the in vivo confocal microscopy, the presence of epithelial conjunctival cells with superficial reflectivity, the presence of goblet cells with roundish highly reflective cells, and the presence of conjunctival stromal collagen and the presence of pannus.23,26,27
On the contrary, we have shown that limbal cells cultured over dAM presented transcripts for Δp63α and ABCB5. Furthermore, the protein presence of these transcripts was corroborated by immunohistochemistry and flow cytometry. These results indicate that the cells grown from limbal explants over dAM are epithelial stem cells. In this context, transcript analyses in other studies have also shown positive differentiation for corneal epithelial stem cell markers such as Δp63α and ABCG2, although in some cases they also include analyses of other transcripts for nonkeratinized corneal epithelial cells such as CK3, CK12, and CK13. 28 In a study to investigate the epithelial–stromal cells interactions, in which a tridimensional model was used to cultivate a mixed population of epithelial limbal cells with corneal stromal stem cells, ABCB5 was found in a larger proportion in the basal epithelial layer of the limbus. 29 Likewise, a study performing the comparison of ABCB5 expression in a normal limbus, with the comparison in ocular surface squamous neoplasia, showed that ABCB5 is expressed clearly in the basal epithelial layer in the healthy limbus, without expression in the suprabasal layers. 17 In patients with ocular surface squamous neoplasia, ABCB5 was overexpressed, without being confined to the basal epithelial layer, appearing also in the suprabasal and superficial cells, presenting with 3 specific patterns: (1) perivascular, where the major expression is observed around the vascular structures; (2) marginal, where the expression is in the basal margin of the tumors; and (3) diffuse, where ABCB5 was diffusely expressed in all the epithelial layers. 17 Sphere-forming cells isolated from peripheral cornea used to repopulate the ocular surface in human corneoscleral rims and also showed positive staining for stem markers such as Δp63, ABCG2, and ABCB5. 30 All these studies, together with the current study, make evident the importance of the expression of ABCB5 in the stemness of the limbal zone. The study by Rama et al. using autologous cultivated limbal epithelial transplantation (CLET) in patients with burns, demonstrated that cultures in which more than 3% of the total number of clonogenic cells constituted p63-bright cells were associated with successful transplantation in 78% of eyes, with 8% of failure and 14% of partial regeneration; in contrast, those cultures having 3% or less of p63-bright cells were successful in only 11% of eye, with failure in 67%, giving a prognosis factor in this type of transplantation. 11 The analysis was performed with quantification of fluorescence immunohistochemistry. 31 In our study, the limited sample size and the elevated rate of failure did not allow us to make a statistical analysis to determine whether ABCB5 and/or Δp63 also play a prognostic role in the survival of cultivated epithelial cells transplantation in LSCD.
The postoperative results in this study show a high rate of failure. The corneal epithelium is the more antigenic structure from all the ocular tissues, and, although the immunoreactivity decreases during the in vitro cellular culture, the occurrence of an immune rejection is present after all type of allogenic transplantation procedures in ocular surface, and immunosuppression plays a pivotal role in those procedures.32–34 Immune rejection can actually present in every procedure of corneal epithelial transplantation, including keratolimbal allografts, and living-related conjunctival allografts. 32 Identification of an immune rejection in patients with allogenic CLET which can lead to failure is difficult to recognize. The appearance of an immune rejection in those patients, normally presents as an edematous corneal epithelium with rejection epithelial lines and peripheral epithelial defects, with perilimbal vessels turning hyperemic and extending to the corneal stroma, giving as a result corneal neovascularization, generating increased stromal opacity, and at a cellular level an increase in T CD4 or CD8 cells. 33
Results of the different series of patients who underwent CLET are difficult to compare as they have a variety of etiologies, culture media, surgical techniques, and subjective and objective results.35,36 An initial factor to consider is the origin of the cells obtained for culture. The presence of an immunologic rejection in the different series is variable; for example, Miri et al., demonstrated that the best long-term results in CLET occurred with an autologous graft, followed by a living-related donor and finally cells obtained from a cadaveric donor, in which 5 out of the 6 patients failed. 37 These results contrast with a study from Prabhasawat et al.; they described that clinical success was lower in autologous grafts than in those with allografts; however, the authors concluded that these results were due to a higher incidence of eyelid malposition in the former group. 28 In the same manner, other groups have reported a success in more than 70% of allogenic CLET for bilateral LSCD. 38 A meta-analysis evaluated the different studies of CLET, without finding a significant difference in successful procedures nor best-corrected visual acuity between autologous or allogenic grafts. 36 In this context, cells taken for culture from living-related donors imply the possibility of a lesser risk of immunologic rejection, due to the HLA matching. 37 In the present study, all the grafts were obtained from cadaveric donors, because all the patients presented bilateral severe LSCD.
Another important factor to consider is the etiology presented by the patients included in this study. In the series published by Qi et al., the immune rejection was reported up to 23.8% of the patients who underwent allogenic transplantation, although all the etiologies were thermal or chemical burns. 33 Patients in our study presented different etiologies of LSCD, with an important inflammatory component, which makes difficult to differentiate between immune rejection and inflammation; even for burns as etiology, in some of these patients, it is demonstrated that they show a chronic inflammatory reaction after the initial trigger. 32 Therefore, for future studies, a more aggressive anti-inflammatory and immunomodulatory treatment should be considered.
Therefore, the factors that could lead our patients from graft rejection to failure include the late reference or treatment of the initial event, the inability of patients to note the presence of rejection mainly in initial stages when the red eye, discomfort, and photophobia are anyway present, and with the knowledge that the highest incidence of rejection is present in the first months. 33 The stem cells require a niche to develop in an appropriate way, considering that the niche is not only an anatomical structure but also functional, interacting with the extrinsic signals like growth factors and cytokines that determine properties and behavior of those cells, leading to the reestablishment of the microenvironment where these cells were initially developed. 39 Recently, it was demonstrated that the low survival of some transplanted cells in ophthalmology, depends on the microenvironment, which is involved in survival, proliferation, and differentiation of the stem cells. 40 Whether the main cause of stem cells transplantation failure was an unhealthy niche of the patients cannot be ruled out.
The results from the 2 patients, who presented improvement in our study, reaffirm that between the diverse etiologies of LSCD, patients with ocular burns are some of those who may present higher possibilities of improvement, and the finding of the positive result in the patient with aniridia may lead to further studies in patients with congenital LSCD. The patient with the melting after CLET is uncommon as there are no severe corneal lysis reported in other series, with the more common complication usually being infectious keratitis and bleeding.11,28,39 Although visual acuity from all of the patients maintained without significant changes, improvement in symptoms such as ocular pain and photophobia is an important finding in the present study.
The present study has limitations. The sample of patients is small and heterogeneous. With the results presenting a high rate (70%) of failure, it is not possible to make a statistical determination of prognostic factors and the correlation with presence and expression of ABCB5. Another limitation is that due to the short follow-up and the low rate of success, no rehabilitation procedures like a penetrating keratoplasty were performed in these patients.
So far we know, this is the first study of limbal stem cells expanded on amniotic membrane transplantation in which both markers ABCB5 and Δp63α are studied in a Mexican population.
In conclusion, ABCB5 and Δp63α are expressed in similar amount in the limbal epithelial cells expanded in vitro and transplanted in patients with bilateral LSCD. Transplantation of allogenic epithelial limbal cells expanded in amniotic membrane could be considered in patients with LSCD due to burns or congenital etiologies such as aniridia, but its benefit is limited for patients with immunologic diseases.
Footnotes
Acknowledgment
We thank Dr. Mohamed A. Pereyra Morales for his technical support.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Consejo Nacional de Ciencia y Tecnología-Problemas Nacionales 2015-311, Consejo Nacional de Ciencia y Tecnología -Ciencia Básica 167438, Consejo Nacional de Ciencia y Tecnología-Fondo Sectorial en Salud: 160286; Dirección General de Asuntos del Personal Académico, Universidad Nacional Autónoma de México-Programa de Apoyo a Proyectos de Investigación e Innovación Tecnológica IN215617, CVU 668682 and Conde de Valenciana Foundation. This study has been registered at ![]() with the number NCT02579993.
with the number NCT02579993.