
Abstract
Purpose:
To evaluate the periodicity of the intervals of lesion reactivation in patients with neovascular age-related macular degeneration (AMD).
Methods:
This retrospective study included 139 eyes diagnosed with treatment-naive neovascular AMD and treated with antivascular endothelial growth factor (VEGF) therapy. Patients were initially treated with 3 loading anti-VEGF injections using either ranibizumab or aflibercept. Additional treatment was administered only when lesion reactivation was noted. The difference between the time intervals to the first and the second reactivations was evaluated. The included eyes were divided into 2 groups according to the time interval to the first reactivation: the early reactivation group (≤6 months, n = 86) and the late reactivation group (>6 months, n = 53). The association between the time intervals to the first and the second reactivations was evaluated within each group.
Results:
The mean follow-up period was 52.7 ± 8.9 months. The first reactivation was noted at mean 9.4 ± 10.4 months after the loading injections. The second reactivation was noted at mean 6.2 ± 4.9 months after the treatment for the first reactivation. The time interval to the second reactivation was significantly shorter compared with the first reactivation (P = 0.018). The association between the time interval to the first and the second reactivations was significant only in the early reactivation group (P = 0.002).
Conclusions:
A short first reactivation interval suggests that there is a high likelihood that the second reactivation will also be short. However, a long first reactivation interval does not suggest that the second reactivation interval will be similarly long.
Introduction
Antivascular endothelial growth factor (VEGF) therapy is an effective, first-line treatment for neovascular age-related macular degeneration (AMD). In early clinical trials, fixed dosing regimen requiring frequent injections was used.1,2 However, considering the increased burden on patients due to the high cost of the drug and the frequent hospital visits, more efficient treatment methods have been developed. Currently, 3 anti-VEGF agents, namely, ranibizumab, aflibercept, and bevacizumab are used to treat neovascular AMD.
The as-needed regimen 3 is one of the most widely used anti-VEGF treatment regimen for neovascular AMD. In this regimen, 3 loading injections are administered as an initial treatment, followed by regular follow-up without further injections until lesion reactivation is noted. 3 It is difficult to expect complete cure in neovascular AMD. Thus, long-term follow-up and treatment are required to preserve vision. When using the as-needed regimen, monthly follow-up is generally recommended for prompt detection and treatment of lesion reactivation. 3 However, in a clinical setting, it is often not possible to maintain this frequent visit schedule in the long term. The interval between the visits is sometimes adjusted or elongated at the patients' request. In such cases, it may be helpful to schedule the visit when the possibility of lesion reactivation is high. Moreover, if the prophylactic injection is performed right before the lesion reactivation, it may efficiently protect the retina from accumulation of damage. Treat-and-extend regimen is another widely used treatment regimen. 4 Recent evidences have shown that more favorable visual outcomes are achieved after the treat-and-extend regimen than after the as-needed regimen, and that the treat-and-extend regimen is associated with less frequent hospital visits.5,6 Thus, in patients for whom frequent reactivation is anticipated, the treat-and-extend regimen may be a plausible approach to minimize visual loss. To achieve this, it is important to try to predict the timing of lesion reactivation.
Previous studies have reported periodical lesion reactivation in eyes with neovascular AMD undergoing anti-VEGF therapy.7,8 However, these studies have several limitations, including small study population and relatively short follow-up period. Thus, it was difficult to evaluate the periodicity of reactivation sufficiently, especially in eyes showing late reactivations. Moreover, to the best of our knowledge, the periodicity of lesion reactivation has not yet been reported in Asian patients.
In the present study, we evaluated the periodicity of the intervals of lesion reactivation in Korean patients with neovascular AMD treated with anti-VEGF therapy. We focused especially on whether there was any difference in the periodicity according to the timing of the first reactivation.
Methods
The present retrospective observational study was performed at a single center. The study was approved by the Institutional Review Board of Kim's Eye Hospital and was conducted in accordance with the tenets of the Declaration of Helsinki.
Patients
Among the patients diagnosed with neovascular AMD and polypoidal choroidal vasculopathy (PCV) between May 2014 and June 2015, those who were initially treated with 3 loading injections of an anti-VEGF agent and experienced at least 2 reactivations of the lesion were included. Only patients who experienced optical coherence tomography (OCT)-confirmed, complete resolution of the intraretinal/subretinal fluid with the initial 3 loading injections were included. If the intraretinal/subretinal fluid had not completely resolved after the 3 loading injections, the patient was excluded from the study even if complete fluid resolution was noted after the fourth or fifth injections. The additional exclusion criteria were as follows: (1) follow-up duration of <24 months, (2) no reactivation after the initial loading injections, (3) no second reactivation after the treatment for the first reactivation, (4) patients who underwent proactive treatment such as the treat-and-extend regimen, 4 right after the loading injections or right after the first reactivation, (5) failure to completely resolve the intraretinal/subretinal fluid accumulation after treatment for the first reactivation, (6) delayed treatment or no treatment for the first reactivation, (7) switching of the anti-VEGF agent while treating the first reactivation, (8) long-term follow-up loss of >6 months, (9) history of vitrectomy before the diagnosis of neovascular AMD, and (10) patients who underwent cataract surgery or vitrectomy before the second reactivation.
When both the eyes met the eligibility criteria, the eye that showed symptoms earlier, was included.
Examinations
The examination and the follow-up methods used in this study were similar to those used in our previous study. 9 At diagnosis, ophthalmological examinations, including measurement of the best-corrected visual acuity (BCVA) and 90D lens slit-lamp biomicroscopy were performed for all patients. Fundus photographs were obtained using CX-1® (Topcon, Tokyo, Japan). Fluorescein angiography images were acquired using combined confocal scanning laser ophthalmoscopy and spectral-domain OCT (Spectralis HRA+OCT®; Heidelberg Engineering GmbH, Heidelberg, Germany). Indocyanine green angiography (ICGA) was performed at the discretion of the doctor. OCT scans were performed using the Spectralis HRA+OCT and the RS 3000® (Nidek Co., Ltd., Tokyo, Japan) or Spectral OCT® (Ophthalmic Technologies, Inc., Toronto, Canada).
The diagnosis of PCV was based on the presence of polypoidal lesions with or without branching vascular networks in the ICGA images.10,11 For cases in whom definite diagnosis of PCV was not possible using the ICGA images obtained at the initial diagnosis, images obtained within 3 months after the diagnosis were also reviewed. Cases with available ICGA results, but without the features of PCV, were classified as neovascular AMD. Cases without the availability of ICGA results or cases in whom accurate classification could not be performed due to thick subretinal hemorrhage were termed unclassifiable.
Treatment and follow-up
Patients were initially administered 3 monthly injections of either 0.5 mg/0.05 mL ranibizumab (Lucentis®; Genentech, Inc., San Francisco, CA) or 2.0 mg/0.05 mL aflibercept (Eylea®; Regeneron, Tarrytown, NY). After the initial 3 loading injections, intraretinal/subretinal fluid was completely resolved in all the included patients. Retreatment was performed on an as-needed basis. Patients were followed up without additional treatment until the first reactivation. During the first 12 months, they were scheduled to visit the hospital every 1–2 months and the follow-up interval was extended to 3 months at the physician's discretion. Subsequently, the follow-up interval was extended to 4 or 5 months. Clinical examination and OCT examination were performed at each follow-up visit. Lesion reactivation was defined as the reaccumulation of subretinal/intraretinal fluid or new development of retinal/subretinal hemorrhage in patients who exhibited dry macula on the previous visit. Lesion reactivation was identified with a clinical examination and OCT. When the first reactivation was noted, 1 to 3 anti-VEGF injections were administered until the fluid accumulation was completely resolved. Patients were followed up until the second reactivation without additional treatment. When the second reactivation was noted, treatment similar to that used for the first reactivation was performed. Regular follow-up was conducted until the third reactivation without additional treatment.
In all the included patients, switching of the anti-VEGF agent was not performed before the second reactivation. After the second reactivation, the anti-VEGF agent was switched in selected patients at the discretion of the treating physician.
Outcome measures
The timings of the first and the second reactivations were recorded. The time interval between the third injection of the initial loading injections and the first reactivation was defined as the first reactivation interval (Fig. 1). The time interval between the last injection to treat the first reactivation and the second reactivation was defined as the second reactivation interval (Fig. 1). For example, if 3 consecutive injections were performed to treat the first reactivation, the interval between the first and the second reactivation was defined as the interval between the third injection and the second reactivation. The treatment period during 3 injections was not included in the interval. Eyes with the first reactivation interval of ≤6 months were included in the early reactivation group, whereas eyes with the first reactivation interval of >6 months were included in the late reactivation group.
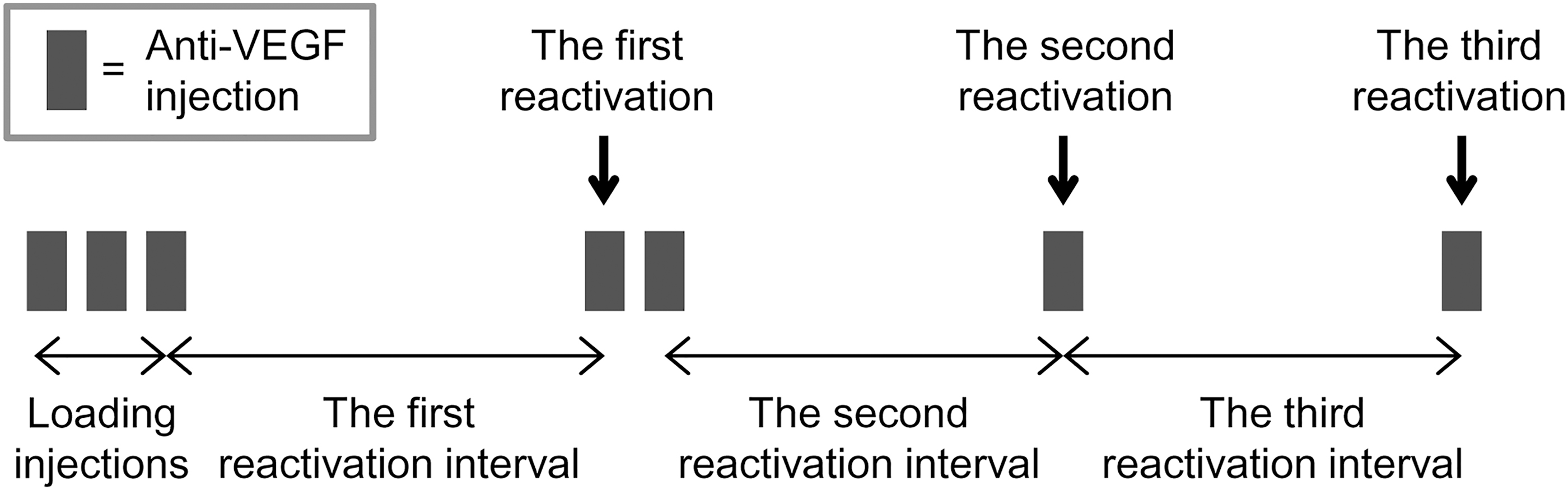
Definitions of the first, the second, and the third reactivation intervals.
The following analyses were performed. (1) The difference in the first and the second reactivation intervals was compared. The difference between the first and the second reactivation intervals was compared between the ranibizumab and the aflibercept groups and the late reactivation group. (2) The association between the first and the second reactivation intervals was evaluated. This analysis was performed for 3 groups: all the included eyes, the early reactivation group, and late reactivation group. (3) The association of the first reactivation interval with the difference between the first and the second reactivation intervals was evaluated. In this analysis, absolute values of the difference in the 2 intervals were used.
The following characteristics were compared between the early reactivation group and the late reactivation group: age, sex, presence of diabetes mellitus, presence of hypertension, subtype of neovascular AMD, type of anti-VEGF agent used for loading injections, follow-up duration, BCVA, lesion size, central retinal thickness, presence of ≥1 disc area of subretinal hemorrhage, and size of hemorrhage. Comparison of size of hemorrhage was performed for patients exhibiting ≥1 disc area of subretinal hemorrhage. As greater than 25 disc areas of hemorrhage size may not be accurately measurable, 25 disc areas was set as the upper limit of size measurement, that is, hemorrhages of a size greater than this limit was measured as 25 disc areas.
Additional analysis was performed for eyes that exhibited a third reactivation during the follow-up period. The following cases were excluded: (1) patients who underwent proactive treatment right after the second reactivation, (2) cases with a failure to completely resolve the intraretinal/subretinal fluid accumulation after the treatment for the second reactivation, (3) delayed treatment or no treatment for the second reactivation, (4) switching of anti-VEGF agent while treating the second reactivation, and (5) patients who underwent cataract surgery or vitrectomy between the second and the third reactivation. The time interval between the last injection to treat the second reactivation and the third reactivation was defined as the third reactivation interval (Fig. 1). The second and the third reactivation intervals were compared.
Eyes treated with ranibizumab were included in the ranibizumab group and those treated with aflibercept were included in the aflibercept group. The following characteristics were compared between the early and late reactivation groups: age, sex, presence of diabetes mellitus, presence of hypertension, subtype of neovascular AMD, follow-up duration, BCVA, lesion size, central retinal thickness, presence of ≥1 disc area of a subretinal hemorrhage, first reactivation interval, and second reactivation interval. In addition, the difference between the first and the second reactivation intervals and that in the absolute values between the first and the second reactivation intervals were compared within each group.
Statistical analyses
The data are presented as mean ± standard deviation or number (percentage) wherever applicable. The BCVA values were converted to logarithm of minimal angle of resolution values for analysis. Statistical analyses were performed using a commercially available software package (SPSS Statistics for Windows, version 12.0; SPSS, Inc., Chicago, IL). The Shapiro–Wilk test was used to identify parameters with a normal distribution. Based on the result, all analyses, except for the comparison of age between 2 groups, were performed using nonparametric methods. Intragroup comparisons were performed using the Wilcoxon signed-rank test. Intergroup comparisons were performed using the independent-samples t-test, the Mann–Whitney U test, the chi-square test, or Fisher's exact test. Correlations were analyzed using Spearman's correlation analysis. P values <0.05 were considered statistically significant.
Results
Among the 411 eyes (411 patients) treated with 3 loading injections during the study period, 272 were excluded for the following reasons: (1) follow-up duration of <24 months (121 eyes), (2) no reactivation after the initial loading injections (33 eyes), (3) no second reactivation after the treatment for the first reactivation (11 eyes), (4) proactive treatment right after the loading injections or right after the first reactivation (37 eyes), (5) failure to completely resolve the intraretinal/subretinal fluid accumulation after the initial loading injection or after the treatment for the first reactivation (47 eyes), (6) delayed treatment or no treatment for the first reactivation (9 eyes), (7) switching of anti-VEGF agent while treating the first reactivation (3 eyes), (8) long-term follow-up loss of >6 months (3 eyes), (9) history of vitrectomy before the diagnosis of neovascular AMD (2 eyes), and (10) cataract surgery or vitrectomy before the second reactivation (6 eyes).
Thus, 139 eyes were included in the final analysis (Table 1). The mean age of the patients was 70.6 ± 8.5 years and the mean follow-up period was 52.7 ± 8.9 months. Eighty-six eyes (61.9%) were included in the early reactivation group and the remaining 53 eyes (38.1%) were included in the late reactivation group. Table 2 summarizes the results of comparisons between the early reactivation group and the late reactivation group. The proportion of male was higher in the late reactivation group (77.4%) than the early reactivation group (58.1%) (P = 0.021). Fifty-eight eyes (41.7%) were classified as having neovascular AMD and 69 eyes (49.6%) were classified as having PCV. Three cases were reclassified based on the ICGA images taken 3 months after diagnosis. Two of them were classified as having PCV and the remaining 1 was classified as having neovascular AMD. In all 3 eyes, accurate classification based on ICGA images taken at diagnosis was not possible owing to submacular hemorrhage.
Baseline Characteristics of the Included Patients (n = 139)
Data are presented as mean ± standard deviation or number (percentage).
AMD, age-related macular degeneration; logMAR, logarithm of minimal angle of resolution; VEGF, vascular endothelial growth factor.
Comparison of Characteristics Between the Early Reactivation Group and Late Reactivation Group
Data are presented as mean ± standard deviation or number (percentage).
Statistical analysis was performed using the independent samples t-test.
Statistical analysis was performed using the chi-square test.
Statistical analysis was performed using Fisher's exact test.
Statistical analysis was performed using the Mann–Whitney U test.
Analysis was performed for the eyes with a subretinal hemorrhage (12 in the early reactivation group and 13 in the late reactivation group).
During the follow-up, the first reactivation was noted at mean 9.4 ± 10.4 months (range 2–49 months) after the third anti-VEGF injection, which was equivalent to 11.4 months after the diagnosis. Mean 1.3 ± 0.6 anti-VEGF injections were administered to treat the first reactivation. The second reactivation was noted at mean 6.2 ± 4.9 months (range 2–45 months) after the last anti-VEGF injection to treat the first reactivation. The mean BCVA was 0.63 ± 0.43 at diagnosis, 0.41 ± 0.36 at 3 months after diagnosis, and 0.57 ± 0.43 at the time of second reactivation. The second reactivation interval was significantly shorter than the first reactivation interval (P = 0.018). Moreover, the difference between the first and the second reactivation intervals was significantly lower in the early reactivation group (mean −1.2 ± 2.9 months; the plus value indicates that the first reactivation interval was longer than the second reactivation interval, whereas the minus value indicates the opposite) than in the late reactivation group (mean 10.5 ± 15.2 months) (P < 0.001).
Figure 2 shows the distribution of the second reactivation interval according to the first reactivation interval. When all the eyes were analyzed (139 eyes), a significant association was observed between the 2 values (P < 0.001, r = 0.308). The association was not significant in the late reactivation group (P = 0.379). However, in the early reactivation group, a significant positive association was observed between the 2 values (P = 0.002, r = 0.323).
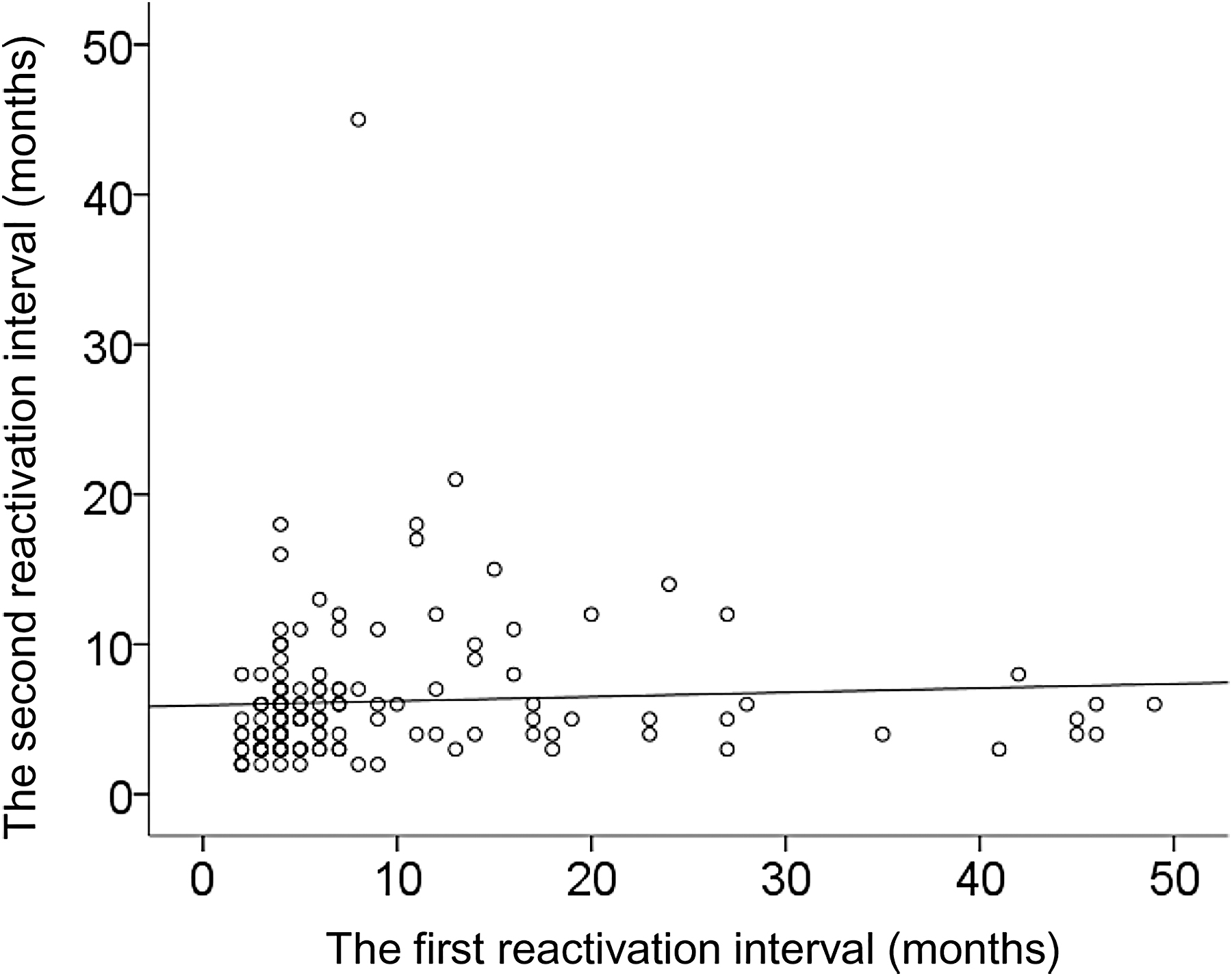
A scatterplot showing distribution of the second reactivation interval according to the first reactivation interval.
The absolute values of the difference between the first and the second reactivation intervals showed significant association with the first reactivation interval (P < 0.001, r = 0.648).
The analysis regarding the third reactivation was performed for 110 eyes. Twenty-nine eyes were excluded for the following reasons: (1) absence of a third reactivation during the follow-up period (14 eyes), (2) proactive treatment right after the second reactivation (1 eye), (3) failure to completely resolve the intraretinal/subretinal fluid accumulation after the treatment for the second reactivation (3 eyes), (4) delayed treatment or no treatment for the second reactivation (6 eyes), (5) switching of anti-VEGF agent while treating the second reactivation (4 eyes), and (6) cataract surgery or vitrectomy between the second and the third reactivation (1 eye). In the 110 eyes, the average second reactivation interval was 5.9 ± 3.5 months and the average third reactivation interval was 5.7 ± 4.2 months. There was no significant difference between the second and the third reactivation intervals (P = 0.174).
Table 3 summarizes the results of comparisons between the ranibizumab (n = 86) and aflibercept (n = 53) groups. There were significant differences in the subtypes of neovascular AMD (P = 0.009) and the incidence of ≥1 disc area of subretinal hemorrhages (P = 0.039) between the groups. In the ranibizumab group, the first reactivation interval was 9.9 ± 10.4 months, and second reactivation interval was 5.8 ± 3.5 months. In the aflibercept group, the first reactivation interval was 8.6 ± 10.3 months, and second reactivation interval was 6.8 ± 6.5 months. There was no significant difference in the first (P = 0.377) or second (P = 0.541) reactivation interval between the groups. In the ranibizumab group, the second reactivation interval was significantly shorter compared with the first reactivation interval (P = 0.005). In the aflibercept group, however, there was no significant difference between the first and second reactivation intervals (P = 0.861).
Comparison of Characteristics Between the Ranibizumab and Aflibercept Groups
Data are expressed as mean ± standard deviation or number (percentage).
Statistical analysis was performed using the independent-samples t-test.
Statistical analysis was performed using the chi-square test.
Statistical analysis was performed using Fisher's exact test.
Statistical analysis was performed using the Mann–Whitney U test.
Discussion
It has been reported that lesion reactivation in neovascular AMD undergoing anti-VEGF therapy shows some periodicity. Horster et al. reported that 22 eyes (76%) out of 29 showed at least 2 periodical lesion reactivation intervals, 7 ; 12 eyes (41%) showed regular reactivation intervals, and 7 eyes (24%) showed irregular recurrence intervals. A study by Mantel et al., which included 39 eyes, also showed regularity of the retreatment rhythm. 8 The rhythm of 11 eyes (35%) was highly regular, showing almost the same time interval between the lesion reactivations. In addition, the time interval to the first lesion reactivation after the 3 loading injections was found to be a good predictor of the following intervals.
In the present study, we focused on the first and the second reactivation intervals. Since eyes with late reactivation were included, it was difficult to assess the third or the fourth reactivation intervals during the follow-up period. As a result, there was a relatively small variation (<2 months) between the first and the second reactivation intervals in 51.8% of the included eyes. This result suggests that the periodic reactivation in these eyes and the timing of the second reactivation can be predicted to some extent by the first reactivation interval.
However, it is noteworthy that this periodicity was valid only in the eyes with relatively short first reactivation intervals. There was a strong tendency of increase in the difference between the first and the second reactivation intervals with increase in the first reactivation interval. In the late reactivation group, the second reactivation interval was markedly shortened compared with the first reactivation interval. Thus, a relatively long first reactivation interval may not guarantee a long second reactivation interval.
After intraocular anti-VEGF injection, intraocular concentration of VEGF decreases continuously over time. 12 Thus, there is a limit to the period of VEGF suppression after injection and the reactivation of the lesion can be accompanied by increase in intraocular VEGF level. 13 There is a significant interindividual variation in the VEGF suppression time. Nevertheless, very late lesion reactivation noted in some of our patients may not be fully explained by the VEGF suppression time alone, as rebounding of VEGF level is usually noted several months after the anti-VEGF injection. We postulate that the nature of the underlying neovascular lesion is more indolent in these patients. In fact, lesion reactivation was reported to be associated with the characteristics of the lesion.14,15 The relatively shorter second reactivation interval than the first reactivation interval may be primarily associated with the changing nature of the neovascular lesion to a more advanced form. In fact, the size of choroidal neovascularization may enlarge during the injection-free period. 16 In addition, the vascular characteristics of choroidal neovascularization may change in eyes undergoing anti-VEGF therapy. 17 Hence, the characteristics of choroidal neovascularization at the time of the first reactivation may differ from those at the initial diagnosis. In our patients, we found no significant difference between the second and the third reactivation intervals. We believe that this result may support our postulation.
The initial loading injection might also have some influence on the late first reactivation in some patients. All patients in the present study received 3 loading injections as an initial treatment, whereas mean 1.3 injections were performed to treat the first reactivation. Thus, prolonged suppression of VEGF during the loading phase might influence the relatively late first reactivation.
Results of the present study may provide useful information for planning efficient treatment for neovascular AMD. Previous studies have shown that lesion reactivation was not observed during the first year in 27.5% to 34.3% of the patients who were initially treated with 3 loading injections.18,19 The as-needed regimen may help these patients avoid unnecessary injections. However, potential accumulation of retinal damage due to recurrent reactivation is a concern while using the as-needed regimen. 7 Moreover, if the treatment is delayed, the chances of visual recovery are lowered. 20 To minimize these risks, frequent monthly follow-up is necessary. However, if a patient cannot adhere to such a frequent follow-up schedule, it is helpful to predict the timing of reactivation. Based on this prediction, frequent follow-ups can be performed only during the period of high possibility of reactivation. Based on the results of the present study, we suggest performing frequent follow-up examinations for cases with a short first reactivation interval. In addition, frequent follow-up examinations are also required when the second reactivation interval is short, regardless of the length of the first reactivation interval.
The treat-and-extend regimen was introduced to reduce the frequency of hospital visit as well as injection frequency. 21 Frequent hospital visit is a large burden to the patients and caregivers. A previous study reported that patients spent almost 12 h for 1 treatment visit. 22 In addition, approximately half of the caregivers took time away from work and personal activities to provide transportation to appointments. 22 When compared with the as-needed regimen, the treat-and-extend regimen is associated with a higher injection frequency.5,6 However, based on the fact that the treat-and-extend regimen is associated with superior visual outcomes and a marked decrease in the frequency of hospital visits,5,6 it has become one of the most widely used regimen in the developed countries. As the treat-and-extend regimen is a “proactive” treatment where injection is administered even in eyes without any sign of reactivation, it may continuously suppress the intraocular VEGF level. We postulate that the enlargement and progression of the underlying neovascularization lesion may be partially prevented or at least slowed by using the treat-and-extend regimen. However, it is merely a postulation. Further follow-up studies with continuous monitoring of the size and characteristics of the neovascularization lesion are required to validate our postulation.
Several studies have reported stabilization or improvement in visual acuity after switching from the as-needed regimen to the treat-and-extend regimen.23–26 Thus, switching the treatment regimen to treat-and-extend may also be a plausible approach to preserve vision if frequent reactivations are anticipated. In the present study, a significant association was observed between the first and the second reactivation intervals. This result suggests that switching the treatment regimen can be considered right after the first reactivation in eyes experiencing very early first reactivation.
Treatment course of neovascular AMD is usually associated with considerable burden to the patient with respect to cost and time.27,28 Thus, to improve adherence, it is important to make sure that the patient understands the future treatment plan and the reasons why he or she should follow such a plan. We believe that the results of the present study may be useful while discussing the future treatment plan with the patients. Among the patients experiencing late first reactivation, we occasionally encounter patients who anticipate that their second reactivation may also be late. Sometimes it is difficult for these patients to understand the need for frequent follow-up visits after the first reactivation. The results of the present study suggest that such an anticipation is possibly incorrect, as there can be a marked difference between the second reactivation interval and the first reactivation interval in cases with a late first reactivation.
In the present study, the proportion of male patients was higher in the late reactivation group than in the early reactivation group. The exact reason for this difference is not clear. In the study by Kuroda et al., 18 male sex was associated with a higher reactivation rate after initial treatment. Thus, our result was somewhat contradictory to that of this previous study. However, in the present study, only patients who experienced at least 2 reactivations and were followed up for 24 months were excluded. Thus, selection bias may have been present in the study result.
As the primary focus of the present study was lesion reactivation during the treatment-free period, patients treated with the treat-and-extend regimen were excluded from the study. Thus, the present study could not provide relevant information for patients treated using the treat-and-extend regimen. With the growing usage of the treat-and-extend regimen worldwide, investigation of the reactivation of the lesion in patients treated using treat-and-extend regimen would be of great value.
In the present study, 2 anti-VEGF agents, namely, ranibizumab and aflibercept, were used. Previous studies reported that aflibercept has a longer duration of action compared with ranibizumab. 13 In addition, time to first reactivation is slightly longer in eyes treated with aflibercept than in those treated with ranibizumab. 19 In our patients, there was no significant difference in the first or second reactivation interval between the ranibizumab and aflibercept groups. A significant difference between the first and second reactivation interval was noted in the ranibizumab group, whereas the difference was not significant in the aflibercept group. It is not certain whether or not this difference in the outcome originated from the difference in anti-VEGF agents. Nevertheless, it is possible that this difference may have influenced the main result of the study, especially the difference between the first and the second reactivation intervals. Further studies with a controlled design and more frequent follow-ups are required to more accurately evaluate the difference in periodicity of reactivation between different anti-VEGF agents.
In the present study, patients were treated for an extended period of time, and all the patients experienced multiple reactivations. Thus, our study may underscore the chronic nature of neovascular AMD. The present study was not designed to compare neovascular AMD and PCV. Therefore, the results of the present study do not support the assumption that PCV is generally more refractory to anti-VEGF therapy and requires more frequent injections than neovascular AMD.
In addition to its retrospective nature, there are limitations to the present study. Since strict monthly follow-up was not performed, time interval to the reactivations may have been overestimated in some eyes. Since patients who experienced at least 2 reactivations were included, there may have been some influence of selection bias on the study results. As described above, analyses results differed between eyes treated with ranibizumab and those treated with aflibercept.
Finally, PCV cases were not excluded from the study. Although anti-VEGF is an effective first-line treatment for PCV, 29 there are some differences in the response to treatment between PCV and neovascular AMD. 30 In addition, photodynamic therapy is still considered as a useful treatment option for PCV. 31 Thus, including patients with PCV may have some influence on the study result. Further studies with a more controlled design are necessary to identify whether the findings noted in the neovascular AMD and PCV groups in the present study can be reproduced.
In conclusion, a short first reactivation interval suggests that there is a high likelihood that the second reactivation will also occur early. However, a long first reactivation interval does not suggest that the second reactivation interval will be similarly long. This raises the question of whether or not the late reactivations are actually reactivations or whether they are new manifestations of the disease with different dynamic. In addition, these results suggest the need for careful monitoring or proactive treatment, regardless of the first reactivation interval. Considering the chronic nature of neovascular AMD, further studies are required to elucidate the longer-term changes in the periodicity of lesion reactivation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Kim's Eye Hospital Research Center.