
Abstract
Purpose:
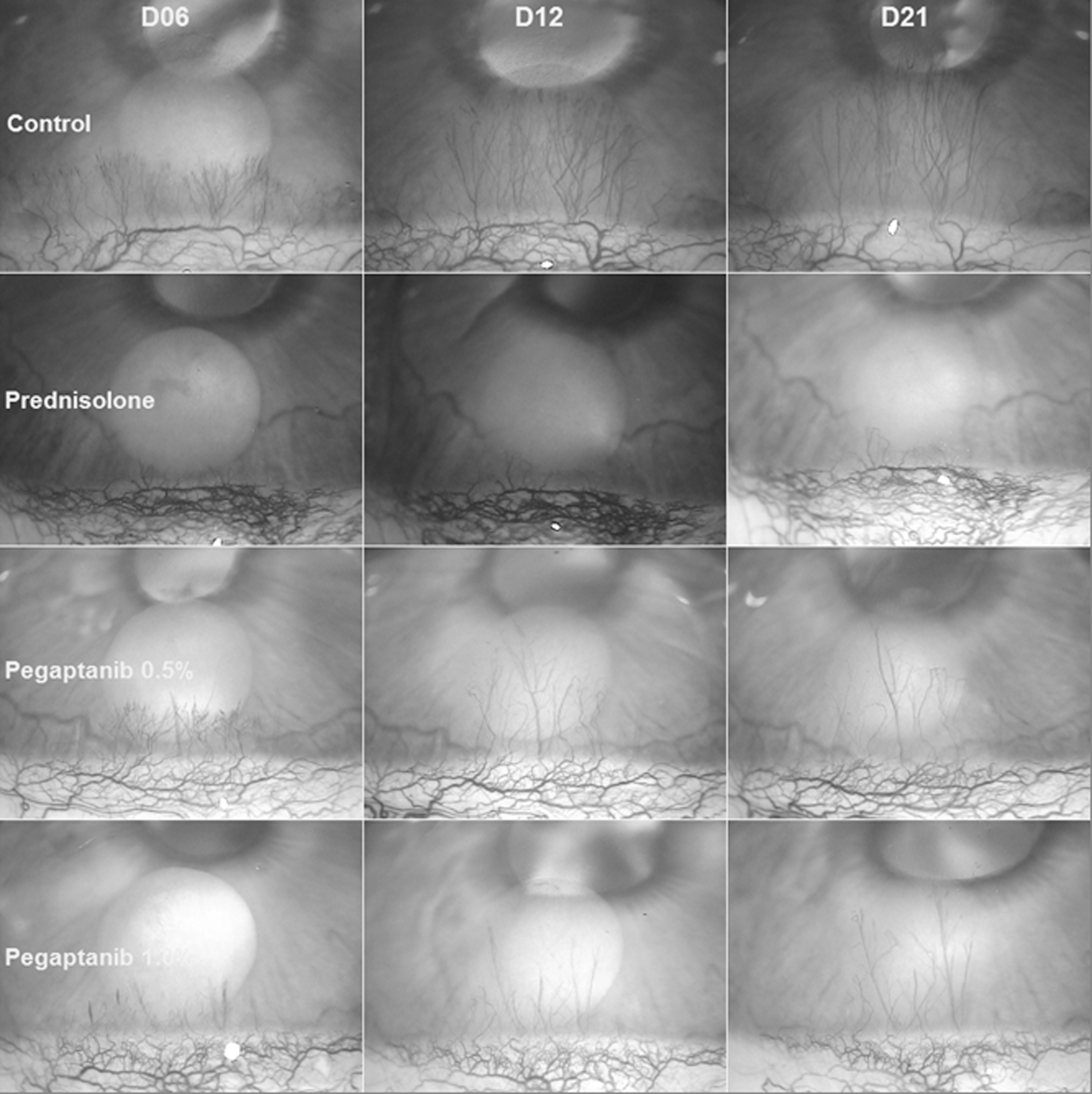
To evaluate the effect of topical instillation of pegaptanib sodium upon inflammatory angiogenesis induced in the rabbit cornea by alkaline cauterization.
Methods:
Inflammatory angiogenesis was induced by alkaline (sodium hydroxide) cauterization in the corneas of 29 male New Zealand rabbits. The animals were divided into 4 groups: a control group treated with 0.5% carboxymethylcellulose sodium eye drops, a group treated with 1.0% prednisolone acetate eye drops, a group treated with 0.5% pegaptanib sodium diluted in 15 mL 0.5% carboxymethylcellulose sodium, and a group treated with 1.0% pegaptanib sodium diluted in 15 mL 0.5% carboxymethylcellulose sodium. After cauterization, eye drops were administered every 12 hours for 21 days. The animals were evaluated every 3 days after cauterization, and the newly formed vessels were quantified from photographs. The treatment effectiveness was analyzed with 3 parameters of antiangiogenic response: neovascularization area (NA), total vascular length (TVL), and number of blood vessels (BVN).
Results:
Average NA, TVL, and BVN values were significantly higher in both pegaptanib groups than in the prednisolone group. A nonstatistically significant reduction in parameters on days 18 and 21 was the minimum achieved in both pegaptanib groups. The efficacy of the treatments in relation to the control was significantly greater in the prednisolone group than in the 0.5% pegaptanib group or the 1.0% pegaptanib group (P < 0.001).
Conclusion:
Topical instillation of 0.5% and 1.0% pegaptanib sodium diluted in 15 mL 0.5% carboxymethylcellulose sodium had no inhibitory effect on corneal neovascularization in this rabbit model.
Introduction
Corneal neovascularization is a category of several inflammatory diseases of the anterior segment such as infections, degenerative and traumatic disorders, reaction to corneal grafts, and extended contact lens wear.1–4 Vascular endothelial growth factor (VEGF) has been implicated in corneal neovascularization.3–5 Medical topical approaches to stop corneal neovascularization has included mitomycin C, 5-fluorouracil, and corticosteroids. The value of such therapy, however, is limited because of potential ocular side effects, including superficial punctate keratitis, poor epithelial healing, scleral ulceration, bacterial infection, and increased intraocular pressure. 6 This motivates our interest in search of alternative therapy with pegaptanib.
VEGF is a glycoprotein involved in the vasculogenesis process with a primary action on blood vessel endothelial cells. It can also act on other more specific cells in the myeloid, neuronal, and epithelial tissues of the kidneys. VEGF is an important angiogenic factor in the healing response process, ischemic process, and inflammatory process.
During an inflammatory process in the cornea, an expression of VEGF occurs in the 3 cell types of the cornea: epithelium, stroma, and endothelium. It especially acts in new immature limbic vessels with few keratinocytes. During anti-VEGF therapy, there is an interruption of the inflammatory cascade that occurs at the site.7,8 Neutralization of VEGF-A with agents on the surface of the cornea has no impact on corneal epithelial healing. The cornea remains normal and the density remains normal in nerve fibers. Therefore, anti-VEGF eye drops appear to be a reasonable and safe option in the treatment of corneal neovascularization.9,10
Pegaptanib sodium was the first targeted anti-VEGF therapy. It is a pegylated anti-VEGF aptamer (ribonucleic acid oligonucleotide ligand) and may theoretically bind to longer VEGF-A isoforms. It was the first ophthalmic antiangiogenic agent approved by the Food and Drug Administration (FDA) for the treatment of all angiographic subtypes of neovascular age-related macular degeneration (AMD). When binding to VEGF165, it inhibits angiogenesis and thereby delays disease progression and preserves vision. Pegaptanib significantly inhibits vascular permeability and retinal neovascularization both in cell cultures and in animal models. 11
Anti-VEGF antibodies such as bevacizumab, ranibizumab, and pegaptanib sodium have been widely used to control neovascularization in neovascular AMD12–16 and proliferative diabetic retinopathy. 17 In addition, the inhibitory effect (IE) of bevacizumab on corneal neovascularization in an alkali burn-induced model of corneal angiogenesis is very well described.1,2 Studies were also carried out with nonviable corneas for transplantation from human donors. These were organ cultured for up to 4 weeks with ranibizumab and bevacizumab and demonstrated the absence of cytotoxic effects. 18
The use of bevacizumab with triamcinolone showed satisfactory results in combating corneal neovascularization associated with blepharoceratoconjunctivitis. 19 The aim of this study was to evaluate the effect of topical instillation of pegaptanib sodium on inflammatory corneal angiogenesis induced by alkaline cauterization in rabbits.
Methods
The study protocol was previously approved (number 07/03) by the Committee on Animal Research and Ethics from Federal University Ceara (UFC) and developed at the UFC and Christus University Center with adherence to the Association for Research in Vision and Ophthalmology (ARVO) statement for the Use of Animals in Ophthalmic and Vision Research. It used 29 male white New Zealand rabbits weighing 1.5–2.5 kg housed at the animal facility of the Department of Experimental Surgery from UFC in appropriate cages under standard conditions of temperature, humidity, and circadian cycle with food and water ad libitum.
Model of inflammatory corneal angiogenesis
Before cauterization and all subsequent evaluations, the animals were anesthetized with a combination of 12 mg/kg ketamine hydrochloride and 4 mg/kg xylazine hydrochloride i.m. with 2 drops of 0.5% proxymethacaine hydrochloride applied topically to the conjunctival sac. The anesthetized animals were placed on a Styrofoam surface in the left lateral position with its back to the examiner. A blepharostat kept the eyelids open exposing almost the entire surface of the cornea and the area of the upper limbus.
Aided by a 16 × magnification surgical microscope, the upper edge of the right cornea was subjected to alkaline cauterization using a round piece of filter paper (3 mm in diameter) soaked in 1 molar solution (M) of sodium hydroxide (NaOH) for 1 min (excess solution was removed with gauze). The filter paper was left for 2 min at ∼1 mm from the corneal-conjunctival limbus at the 11 o'clock position near the insertion of the superior rectus muscle. The eye was subsequently washed with 10 mL of 0.9% sodium chloride solution to remove excess NaOH. A homogeneous circular surface, 3.5 mm wide, with well-defined edges was created after cauterization. The animals were returned to the cages after anesthetic suppression.
Experimental design
The UFC's Experimental Surgery Laboratory was the location chosen for the experiments. The rabbits were randomly divided into 4 treatment groups: (1) a control group composed of 11 rabbits treated with 1 drop (40 μL) of 0.5% sodium carboxymethyl cellulose ophthalmic solution instilled in the conjunctival sac twice a day, (2) a prednisolone group consisting of 6 rabbits treated with topical instillation of 1 drop (40 μL) of 1.0% prednisolone acetate eye drops twice daily, (3) a 0.5% pegaptanib group composed of 6 rabbits treated with 1 drop (40 μL) of pegaptanib (diluted in 0.5% solution) in the conjunctival sac twice a day, and (4) a 1.0% pegaptanib group composed of 6 rabbits treated with a drop (40 μL) of pegaptanib (diluted in 1.0% solution) in the conjunctival sac twice a day. The beginning of the treatments took place on the day of the cauterization (day 0) and treatments continued for 21 days.
Image acquisition and processing
The animals were evaluated on days 3, 6, 9, 12, 15, 18, and 21 after cauterization. During exposure, corneal hydration was maintained with frequent applications of a liquid eye gel based on polyacrylic acid—a substitute for tear fluids. Corneal images were acquired with a video camera attached to a surgical microscope with data sent to a microcomputer. The microscope axis was positioned perpendicular to the tangent of the corneal margin to minimize spatial distortion. In addition, a green filter was used to increase the contrast of the blood vessels. The images were acquired and had a 25 × magnification and were saved as Windows® bitmaps (.bmp) measuring 320 × 240 pixels.
{kind=link}
The angiogenesis quantifier system was the software developed for this purpose and measured the angiogenesis response. 20 The system processed digital images of the cornea and determined the neovascularization area (NA), the total vascular length (TVL), and the number of blood vessels (BVN). From the NA, it was possible to calculate the angiogenesis rate for each treatment using the following equation:
The IE of the tested drugs was determined in relation to the control group on days 3, 6, 9, 12, 15, 18, and 21, using the following equation:
Treatment efficacy was expressed as mean inhibitory effect (MIE) defined as the sum of all IE values divided by the number of tests.
Statistical analysis
The Kolmogorov–Smirnov test was used to analyze the normality of the distribution. The data were expressed as means and standard deviations. The analysis of variance (ANOVA) and the Tukey multiple comparison test were tools used for comparisons between treatment groups. A value of P < 0.05 was considered statistically significant. All statistical analyses were performed using GraphPad Prism software version 5.00 for Windows (GraphPad Software, San Diego, CA).
Results
The evolution of the angiogenesis parameters (NA, TVL, and BVN) in the control group reveals a biphasic pattern characterized by a period of intense vascular growth up to day 9 followed by a period of stability up to day 21 (Figs. 1–4). The maximum NA, TVL, and BVN values recorded on day 21 were 1.922 ± 1.247 mm2, 31.127 ± 20.238 mm, and 203.182 ± 121.773 vessels, respectively.
Angiogenic response in the 4 study groups.

NA. Quantification of the angiogenic response of the animals in the 4 study groups: control (n = 11), prednisolone (n = 6), 0.5% pegaptanib (n = 6), and 1.0% pegaptanib (n = 6) according to NA. Average measures ± SD expressed in mm2 were taken on days 3, 6, 9, 12, 15, 18, and 21 postcauterization. **P < 0.01: prednisolone group < control. ***P < 0.001: prednisolone group < control. +P < 0.05: prednisolone group <0.5% pegaptanib group. ++P < 0.01: prednisolone group <0.5% pegaptanib group. #P < 0.05: prednisolone group <1.0% pegaptanib group. ##P < 0.01: prednisolone group <1.0% pegaptanib group. NA, neovascularization area; SD, standard deviation.
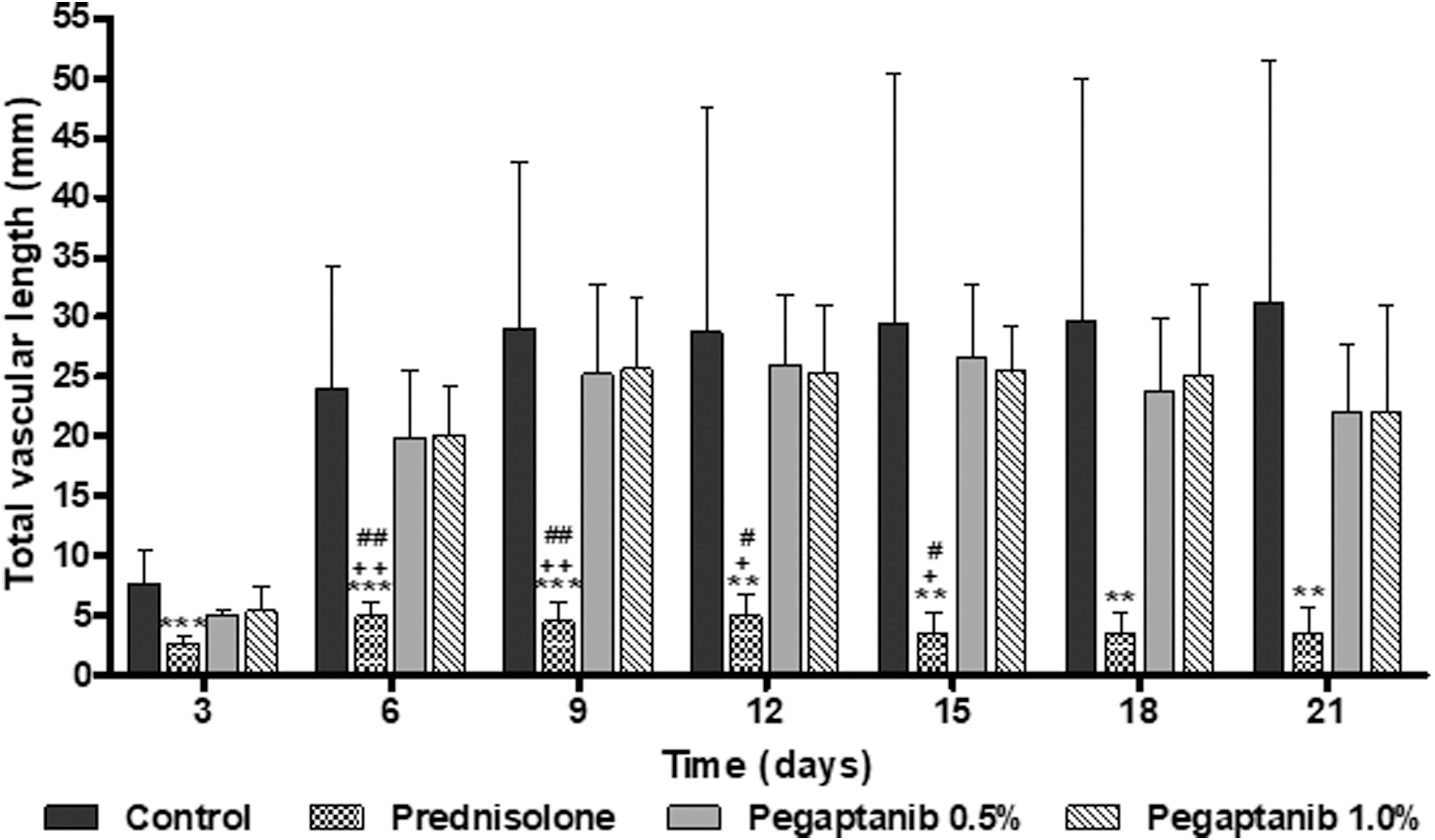
TVL. Quantification of the angiogenic response of the animals in the 4 study groups: control (n = 11), prednisolone (n = 6), 0.5% pegaptanib (n = 6), and 1.0% pegaptanib (n = 6) according to TVL. Average measures ± SD expressed in mm2 were taken on days 3, 6, 9, 12, 15, 18, and 21 postcauterization. **P < 0.01: prednisolone group < control. ***P < 0.001: prednisolone group < control. +P < 0.05: prednisolone group <0.5% pegaptanib group. ++P < 0.01: prednisolone group <0.5% pegaptanib group. #P < 0.05: prednisolone group <1.0% pegaptanib group. ##P < 0.01: prednisolone group <1.0% pegaptanib group. TVL, total vascular length.
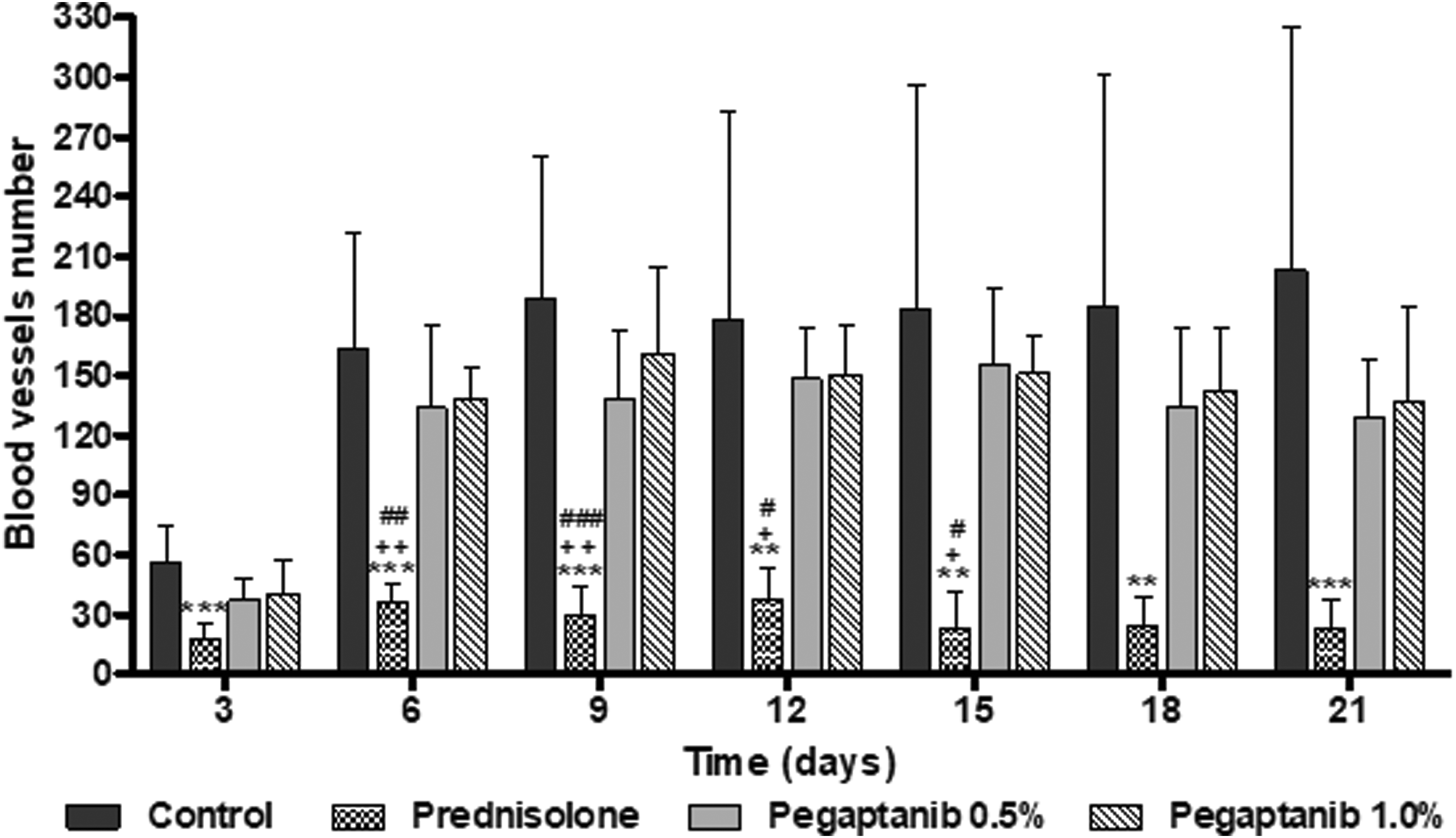
BVN. Quantification of the angiogenic response of the animals in the 4 study groups: control (n = 11), prednisolone (n = 6), 0.5% pegaptanib (n = 6), and 1.0% pegaptanib (n = 6) according to the BVN. Average measures ± SD expressed in mm2 were taken on days 3, 6, 9, 12, 15, 18, and 21 postcauterization. **P < 0.01: prednisolone group < control. ***P < 0.001: prednisolone group < control. +P < 0.05: prednisolone group <0.5% pegaptanib group. ++P < 0.01: prednisolone group <0.5% pegaptanib group. ##P < 0.01: prednisolone group <1.0% pegaptanib group. ###P < 0.001: prednisolone group <1.0% pegaptanib group. BVN, number of blood vessels.
In the prednisolone group, the average NA, TVL, and BVN values were nearly constant during the experiment and significantly lower (P < 0.01) than in the control group on all follow-up examinations (Figs. 1–4). The maximum NA, TVL, and BVN values were 0.322 ± 0.069 mm2 (day 6), 5.013 ± 1.076 mm (day 6), and 37.667 ± 16.182 vessels (day 12).
In both pegaptanib groups, the NA, TVL, and BVN evolved as in the control group up to day 15. On days 18 and 21, vascular growth decreased as shown by a reduction in the study parameters (Figs. 1–4). However, the observed reduction was not statistically significant versus the prednisolone group.
The rate of vascular growth was measured throughout the study as RA (Fig. 5). RA was significantly lower in the prednisolone group than in the control group (0.003 ± 0.006 mm2/day vs. 0.079 ± 0.066 mm2/day; P < 0.05). RA was also lower in the 0.5% pegaptanib group (0.056 ± 0.019 mm2/day) and in the 1.0% pegaptanib group (0.053 ± 0.026 mm2/day).
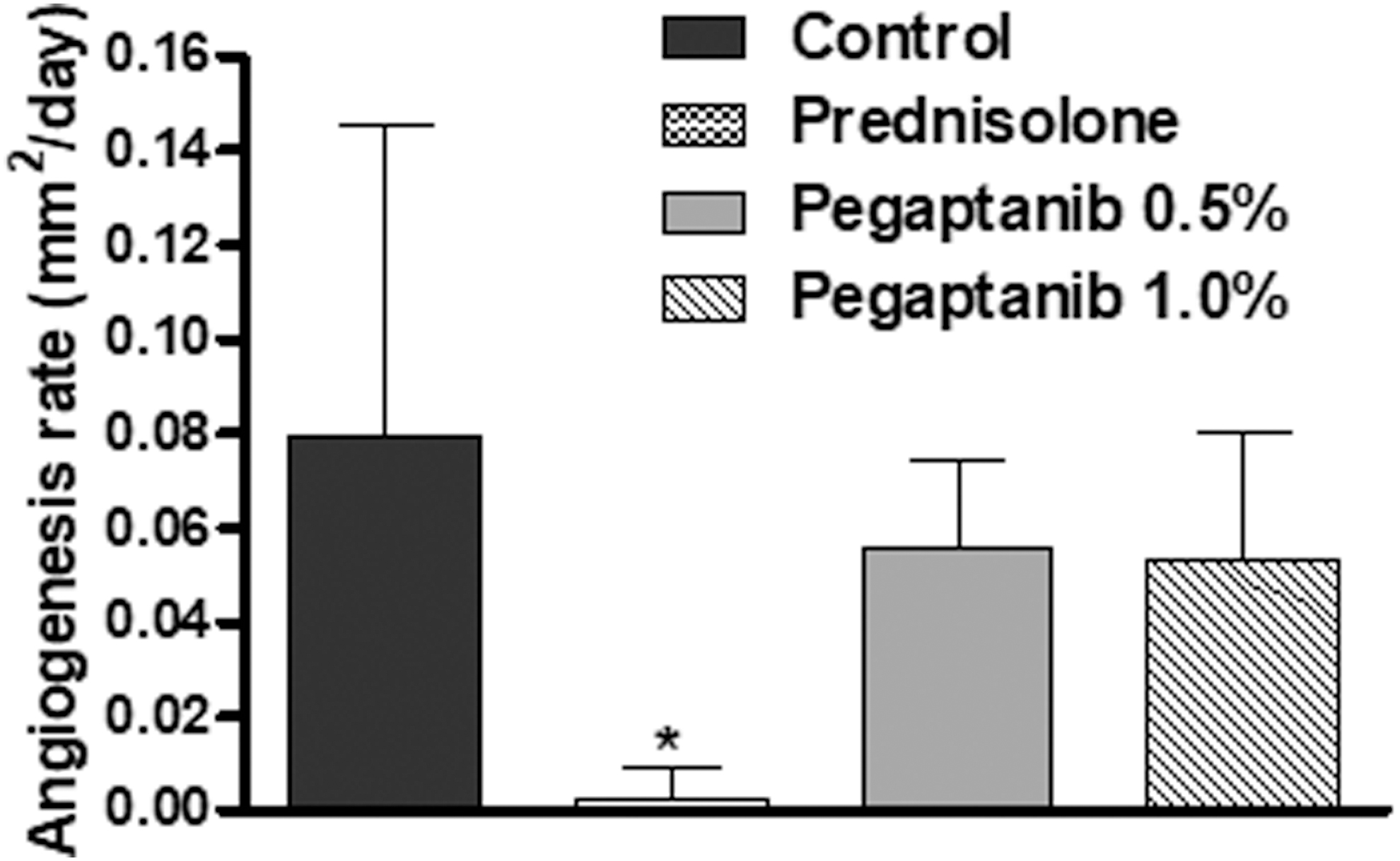
AR. AR in mm2/day for the period between days 3 and 21, calculated for the control, prednisolone, and 0.5% and 1.0% pegaptanib groups. The data represent the mean and SD of measurements in each group. *P < 0.05: prednisolone group < control. AR, angiogenesis rate.
The efficacy of the treatments in relation to the control group was expressed as MIE (Fig. 6). The MIE was significantly greater in the prednisolone group (82.459% ± 7.911%) than in the 0.5% pegaptanib group (20.628% ± 9.389%) or the 1.0% pegaptanib group (20.067% ± 7.384%) (P < 0.001).

Mean inhibitory effect. Average efficacy (±SD) of treatments with prednisolone, 0.5% pegaptanib, and 1.0% pegaptanib expressed in percentages in relation to controls on days 3, 6, 9, 12, 15, 18, and 21 postcauterization. ***P < 0.001: prednisolone group >0.5% and 1.0% pegaptanib groups.
Discussion
The exact mechanisms underlying loss of normal corneal angiogenic privilege and the development of pathologic neovascularization remain unclear. Studies have demonstrated the existence of 2 phases during the mechanism, the first phase characterized by intense vascular proliferation, and the second phase is marked by the maturation of the vessels. 20 Ocular neovascularization represents a major public health problem and is responsible for more irreversible blindness in middle-aged and senior citizens than any other pathology. The major stimuli for corneal neovascularization are corneal inflammation, hypoxia, and limbal stem cell destruction. 4 A study has confirmed the increase in expression of VEGF in human corneas with neovascularization 21 and VEGF may play a role in the maintenance of new vessels.
The alkaline cauterization model chosen for this study (using 1 M NaOH) is simple, and the results are easily quantified. 22 It has been used to study the role of leukocytes, angiogenic factors, and inflammation mediators during angiogenesis and can test a number of drugs such as anti-VEGF drugs as well as steroidal and nonsteroidal agents. Among these drugs, steroids are the most efficient and remain the strategy of choice for the prevention of corneal graft rejection despite the potential ocular side effects.23,24
Previously, in a rat corneal angiogenesis model induced by pellets containing VEGF165, animals were subjected to systemic treatment with an intravenous injection of pegaptanib. It showed that VEGF-dependent angiogenesis was significantly (65%) inhibited in relation to controls. 9 This result shows the true efficacy of pegaptanib in a model of angiogenesis induced by VEGF165.
In fact, the wide variety of angiogenic and inflammatory mediators responsible for the neovascularization process is very well documented, best exemplified in models of inflammatory angiogenesis. This may explain the lack of efficacy of pegaptanib monotherapy in models of inflammatory angiogenesis. Ju et al. 25 showed that in an inflammatory corneal neovascularization model, pegaptanib sodium monotherapy, given i.p., yielded little regression of further vessel growth. The combination of pegaptanib sodium and photodynamic therapy resulted in the regression of neovascular lesions and also prevented significant vessel regrowth, leading to a significantly greater reduction in lesion size.
Another study comparing the effects of bevacizumab, ranibizumab, and pegaptanib to prevent corneal neovascularization in rats resulted in a satisfactory effect of the 3 substances; however, bevacizumab showed a better effect than the other 2 substances. The study used in the corneas of the rats, the dosage of antiangiogens was 0.05 mL/1.25 mg of bevacizumab, 0.05 mL/0.15 mg of pegaptanib, and 0.05 mL/0.5 mg of ranibizumab, and the analysis was based on macroscopy and microscopy. Among the data cited, we observed significant differences in our study in relation to the cited study, which obtained good results, evidencing that these differences influenced our results. 26
Another study evaluated the mechanisms of the neovascularization phases of the cornea and was carried out with LASSBio-5960—a thalidomide hybrid. LASSBio-596 showed more effective results in the second phase of neovascularization but showed less IE on the neovascularization process versus the dexamethasone group. Dexamethasone is well established and has led to more significant results with high rates of reduction in the neovascular area since the beginning of vascular progression. 20 In the phases of neovascularization, we observed significant similarities between our study and the prior study. 27
Our results show that corneal neovascularization is potentially inhibited by topical instillation of prednisolone but not by topical instillation of 0.5% and 1% pegaptanib. The absence of effects in the latter case may also be explained by inadequate dosage, insufficient diffusion/absorption of the drug through the conjunctiva and cornea, inappropriate frequency of instillation, or other mediators interfering with the IE of the drug.
Topical instillation is an easy form of treatment associated with high levels of patient acceptance and compliance. Although topical administration of pegaptanib was not observed to inhibit corneal neovascularization in this study, further studies testing this and other antiangiogenic drugs are needed to identify efficient topical agents capable of preventing corneal neovascularization. Further studies are also needed to assess adverse events and to consider the optimal dosing regimens for these drugs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.