
Abstract
Purpose:
In this study, the aim was to evaluate the safety of transcorneal electrical stimulation (TES) treatment in retinitis pigmentosa (RP) patients and to investigate the effect of TES to the visual acuity (VA), visual field (VF), and multifocal electroretinogram (mfERG) findings.
Methods:
Two hundred two eyes of 101 RP patients with different stages were studied. TES was applied for 30 min once a week for 8 consecutive weeks. Two hundred eyes of 100 RP patients were enrolled as control. After the 2-month TES therapy sessions, patients were followed for 4 months without treatment. Examinations were done at the baseline before TES treatment and 1 and 6 months after the treatment. Best-corrected VA (BCVA), color fundus photography, VF test, optical coherence tomography, and mfERG tests were done at each visit.
Results:
The mean BCVA and VF tests improved 1 month after the beginning of TES treatment and the improvements were statistically significant (P < 0.05). There was an improvement in p1 wave amplitude in rings 1, 2, and 3 at the first month. The latency of the p1 wave showed a statistically significant shortening in rings 1 and 2. These improvements partially disappeared at 6-month follow-up. There were no serious ocular side effects related to the therapy. Mild dry eye symptoms were observed, which were revealed by artificial tears.
Conclusions:
TES is a safe therapy without any serious advers effects. Although it can improve VA and VF of RP patients, the beneficial effects could be transient and repeated sessions can be necessary for maintaining the efficiency.
Introduction
Retinitis pigmentosa (RP) is known as a genetic disease characterized by the degeneration of the photoreceptor cells. 1 In the early stages of the disease, loss of rod photoreceptors causes peripheral visual field (VF) defects and a decrease in night vision. With the progression of the disease, cone photoreceptors are also affected and the visual acuity (VA) in the daylight also deteriorates. In the last stage, the disease causes total vision loss. There is currently no effective treatment of RP.1,2 Studies on gene and stem cell therapy are still going on rapidly.2,3
Transcorneal electrical stimulation (TES) is a new treatment modality. Animal studies have shown that retinal neurons and photoreceptor cells such as retinal ganglion cells are protected against traumatically and genetically induced degenerations by the TES method. 4
Previous studies suggested that the neuroprotective effect of this treatment method is formed by many pathways. It is reported that TES can act by vasodilatory, neurotrophic, and antiapoptotic mechanisms.5,6
In vitro studies showed that TES increased endogenous neurotrophic factor expression and intrinsic sensitivity of neurons against these factors. A significant increase in insulin-like growth factor, ciliary neurotrophic factor, and vascular endothelial growth factor secretion was observed after TES.5–8 Because of the positive effects found in experimental studies, it is thought that TES can be useful in ophthalmology. After applications in eye diseases, successful results were reported in the pathologies related to optic nerve and retina such as RP, Best vitelliform dystrophy, retinal artery occlusion, traumatic optic neuropathy, and anterior ischemic optic neuropathy.9–17
TES treatment has been shown to have beneficial effects on RP cases.9,11,14 Although RP depends on many genetic factors, all these genetic mechanisms result in apoptotic cell death. Regardless of the genetic mutation, TES can be effective over apoptotic cascade and protect photoreceptors from programmed cell death.9,11,14,15
The purpose of this study was to evaluate the safety of TES treatment in RP patients and to investigate the effect of the therapy on VA, VF, and multifocal electroretinogram (mfERG) measurements. The study also aims to determine the continuity of the efficacy of the treatment.
Methods
Patient selection
This is a retrospective study that included 202 eyes of 101 RP patients. Data of 101 patients who underwent TES treatment in our clinic between January 2016 and January 2019 were screened. The study was conducted in adherence with the tenets of the Declaration of Helsinki. The patients were fully informed about the goals of the treatment and informed constent was obtained. The diagnosis of RP was established depending on clinical history, ophthalmological findings, VF measurement, optical coherence tomography (OCT), and mfERG test results.
The exclusion criteria were determined as follows:
Presence of another retinal disease other than RP History of ocular surgery other than cataract surgery (keratoplasty, glaucoma surgery, vitreoretinal surgery, presence of silicone tamponade) Presence of advanced cataract Presence of an additional disease that affects the VF (such as glaucoma, neurological problems) Presence of any macular problems such as cystoid macular edema or epiretinal membrane Advanced dry eye disease
VA was measured with a Snellen chart at a distance of 3 m. OCT was performed using the Optovue (Optovue, Inc.) device. VF examination was performed by Humphrey VF field analyzer device (Carl Zeiss Meditec AG Germany). The 30–2 program was used for VF testing of each eye. mfERG was recorded on mfERG-Vision monitor (Metrovision, France). The readings were recorded from each eye as per the International Society for Clinical Electrophysiology of Vision (ISCEV) guidelines. Sixteen of the patients could not fixate for VF and mfERG recording, and so, their results were excluded. The central macular thickness (CMT) was measured manually by measuring the distance between the outer edge of the hyper-reflectivity of the RPE and the inner edge of the vitreo/foveal junction.The patients were treated with TES for 30 min once a week for 8 consecutive weeks. Best-corrected VA (BCVA), color fundus photography, OCT, VF, and mfERG tests were performed at baseline before starting the treatment and 1 and 6 months after the treatment.
TES application
TES was applied with an Okuvision device approved by CE (Okuvision GmbH, Reutlingen, Germany). This device has a useful property as being easy to apply in an outpatient clinic.
The device consists of 3 parts Read Stim, Oku Spex, and Oku El. Read Stim is a stimulation unit. OkuSpex is a spectacle frame-like section placed on the patient's face. This frame is adjusted according to the patient's face. TES was administered using sterile single-use DTL electrodes (OkuEl) positioned onto a rigid semicircular frame mounted onto the OkuSpex. Microfiber electrodes are placed on the corneal surface after topical anesthesia (proparacaine). Another inactive reference electrode is placed on the skin around the eye (Fig. 1).
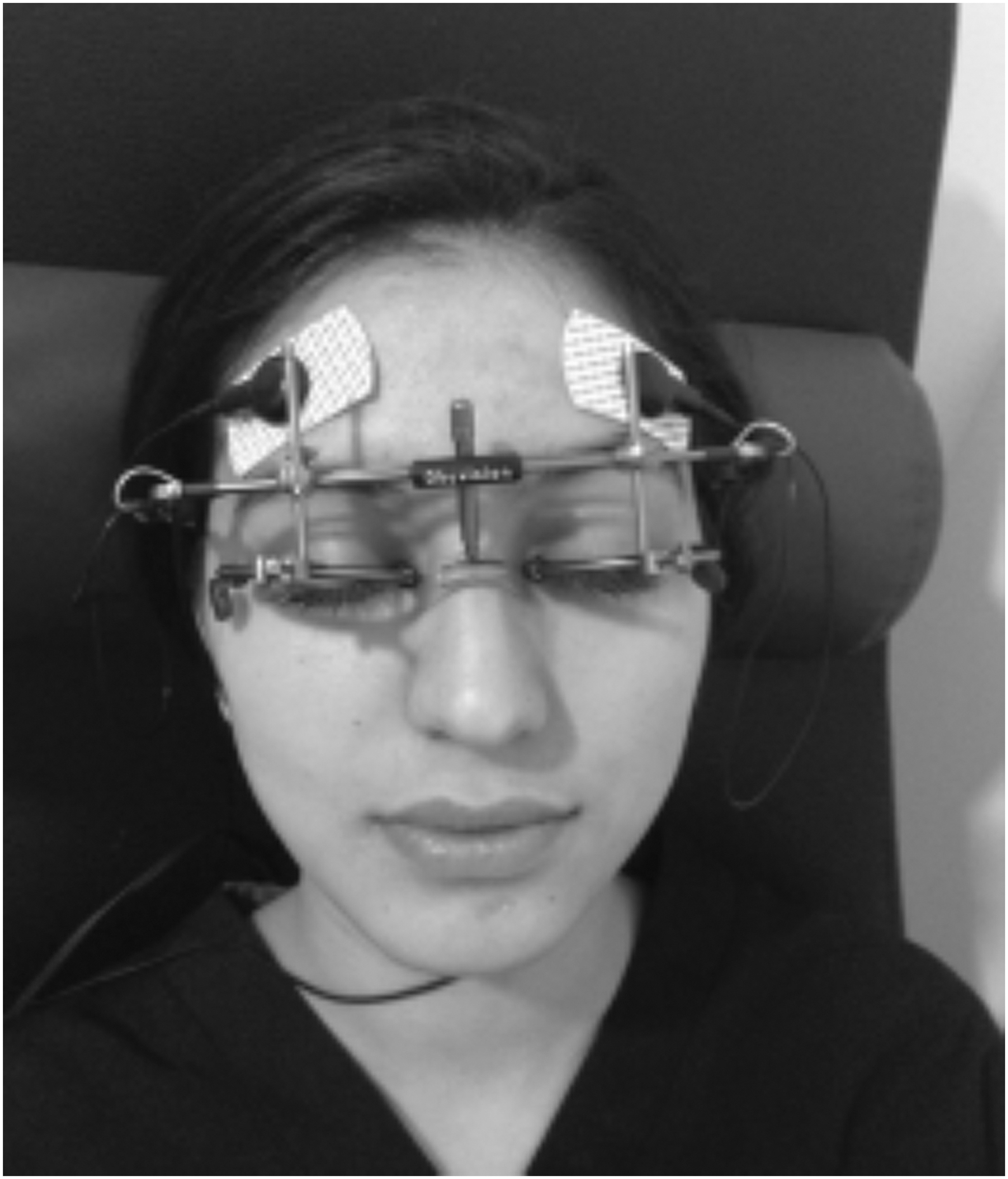
TES system. The frame is adjusted according to the patient's face, microfiber electrodes are placed on the corneal surface, and another inactive electrode is placed on the skin around the eye as a reference electrode. TES, transcorneal electrical stimulation.
During the study, dose adjustment was determined by the physicion in each case. The current was slowly titrated up from 0.02 mA, in increments of 0.01–0.05 mA to a maximum current of 1.0 mA, until participants perceived phosphenes. The average of the 3 values formed the participant's individual phosphene threshold (IPT). The current of TES delivered was 150% of the IPT.
Ophthalmological examination and tests: BCVA with Snellen chart, biomicroscopic examination, fundus examination, color fundus photography, OCT, VF, and mfERG were performed at baseline before starting treatment and repeated at 1 and 6 months after the treatment. Each patient was informed by the physician about the expected results and possible side effects of the treatment, and patient consent form was obtained from the patients.
Statistical methods
Measurement data are expressed as mean ± standard deviation. SPSS was used for data analysis. The BCVA and parametric results for VF and mfERG were analyzed using the t-test and repeated analysis of variance test. P values smaller than 0.05 were considered statistically significant.
Results
Two hundred two eyes of 101 RP patients attending the ophtalmology clinic of our hospital were enrolled. The mean age of the subjects was 31.70 ± 13.75 years (range 18–60 years). Fifty-eight of them were male, 43 were female.
TES was well tolerated with no serious ocular or systemic side effects during or after treatment. The most frequent side effect was transient foreign body sensation, which was experienced by nearly all participants. For temporary dry eye symptoms, artificial tear support was given for several days after TES application.
The mean BCVA of the 202 studied eyes before treatment was 0.19 ± 0.23 Snellen lines (range between 0.01 and 1.0 Snellen lines). It improved to 0.25 ± 0.27 Snellen lines 1 month after TES treatment, which was statistically significant (P < 0.05). Final BCVA (6 months after BCVA) was 0.24 ± 0.26, which was significantly higher when compared with baseline.
VF values were not measurable in all eyes because of poor fixation. VF of 170 eyes from 85 patients was evaluated and mean deviation (MD) values were recorded. Because of the wide spectrum of disease severity, VF showed a variation with a range of −19.10 and −33.94. Baseline and 1- and 6-month mean MD values were −27.46 ± 7.49, −25.79 ± 8.69, and −26.21 ± 8.5 respectively (P < 0.01). Statistically significant VF improvement was detected 1 month after TES when compared with baseline values. Unfortunately, this improvement decreased slightly at the 6-month follow-up (Figs. 2–4).

The improvement in the VF after TES (Case 1).
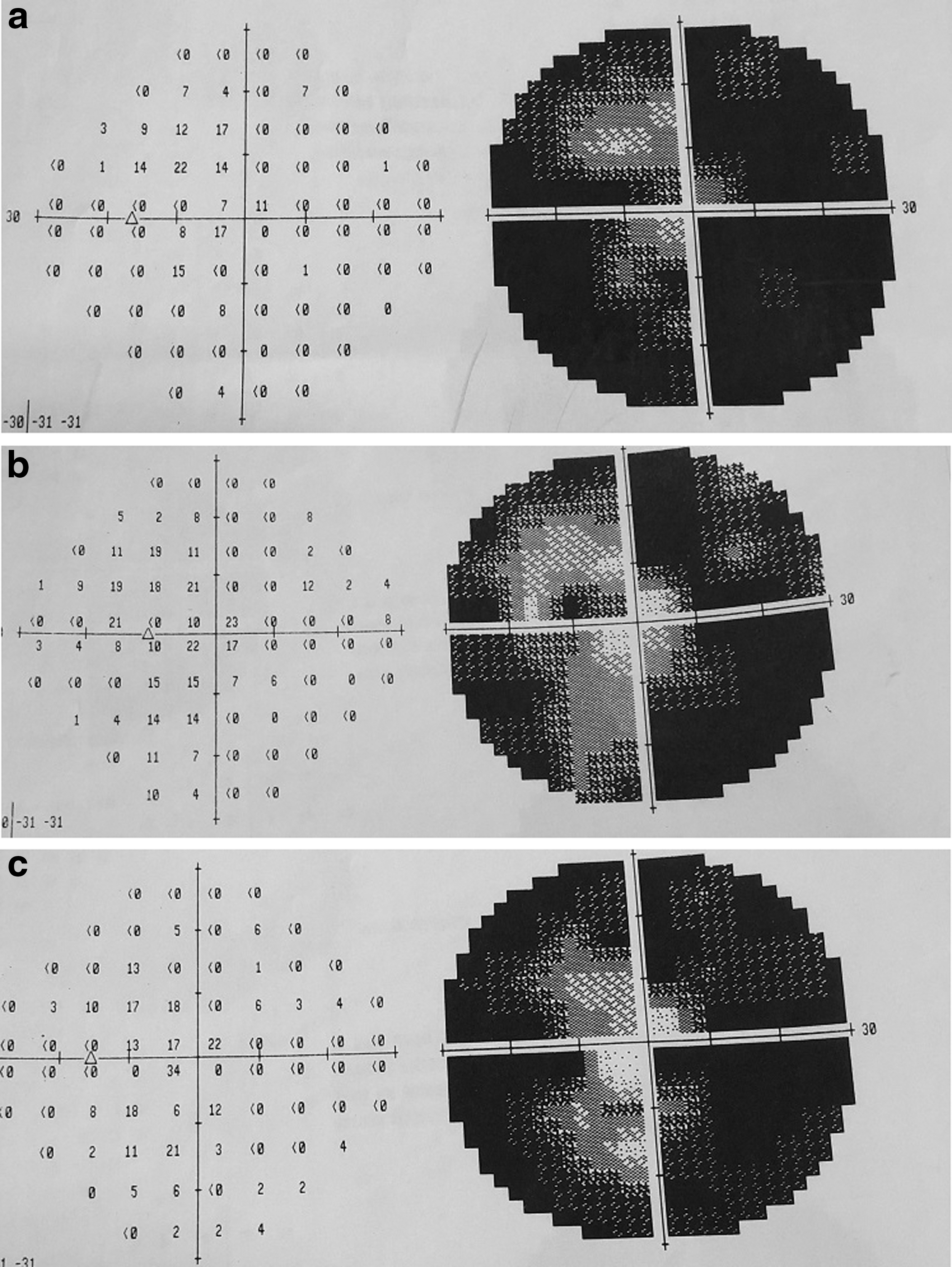
The improvement in the VF after TES (Case 2).
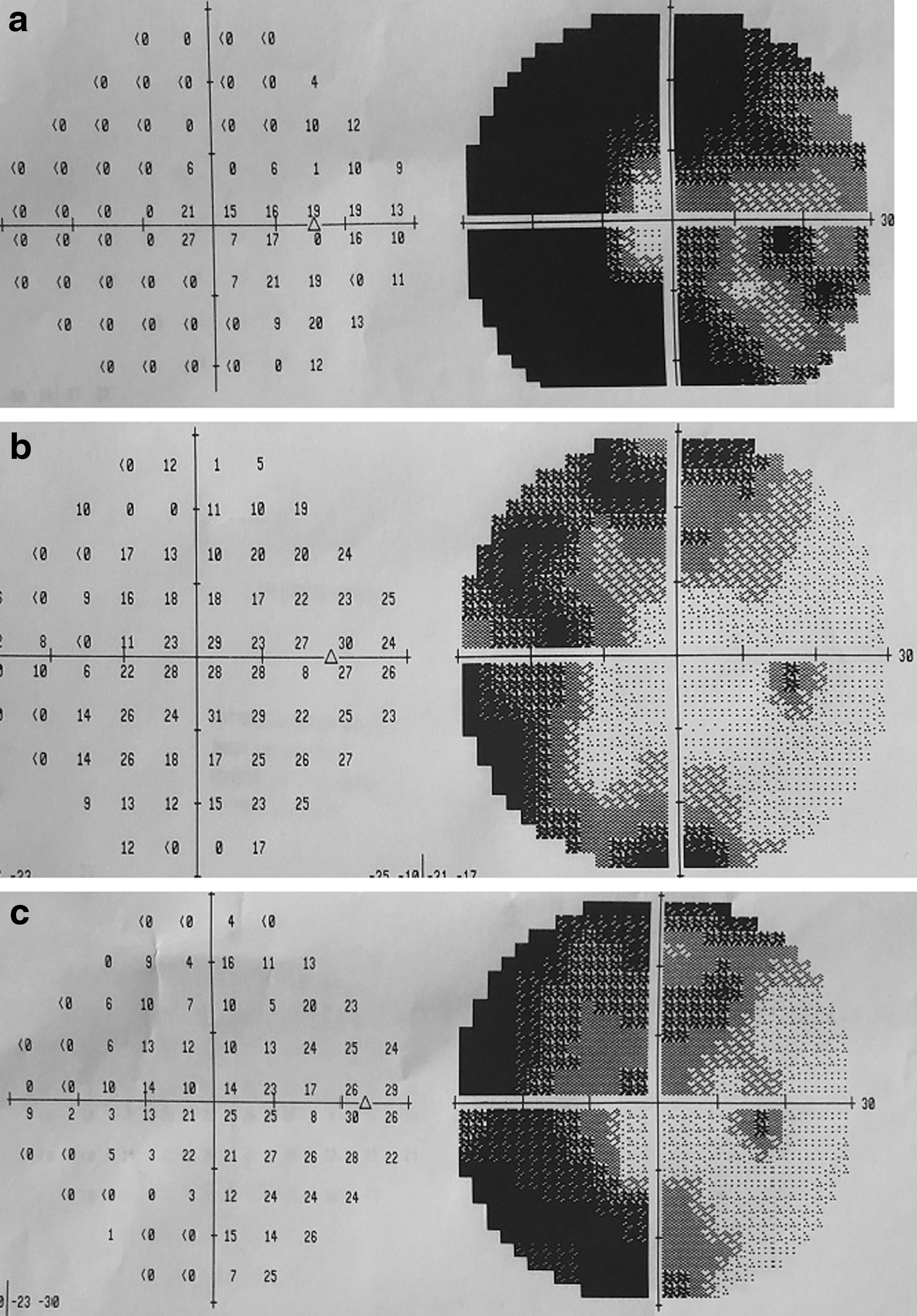
The improvement in the VF after TES (Case 3).
CMT measurements at baseline and 1 and 6 months were 196 ± 13 μm, 198 ± 14 μm, and 195 ± 14 μm, respectively, which showed no significant difference (P > 0.05) (Table 1). OCT of the patients showed no new retinal pathology, such as cystoid macular edema and epiretinal membrane, which was induced by TES treatment. These results are given in Table 1.
Best-Corrected Visual Acuity, Visual Field, and Optical Coherence Tomography Measurements of the Patients
Values are expressed as mean ± SD.
There was a statistically significant improvement in the VA values of the treatment group. However, there was a significant decrease in the values of the control group.
There was a statistically significant improvement in the MD values of the treatment group. However, there was a significant decrease in the values of the control group.
BCVA, best-corrected visual acuity; MD, mean deviation; SD, standard deviation.
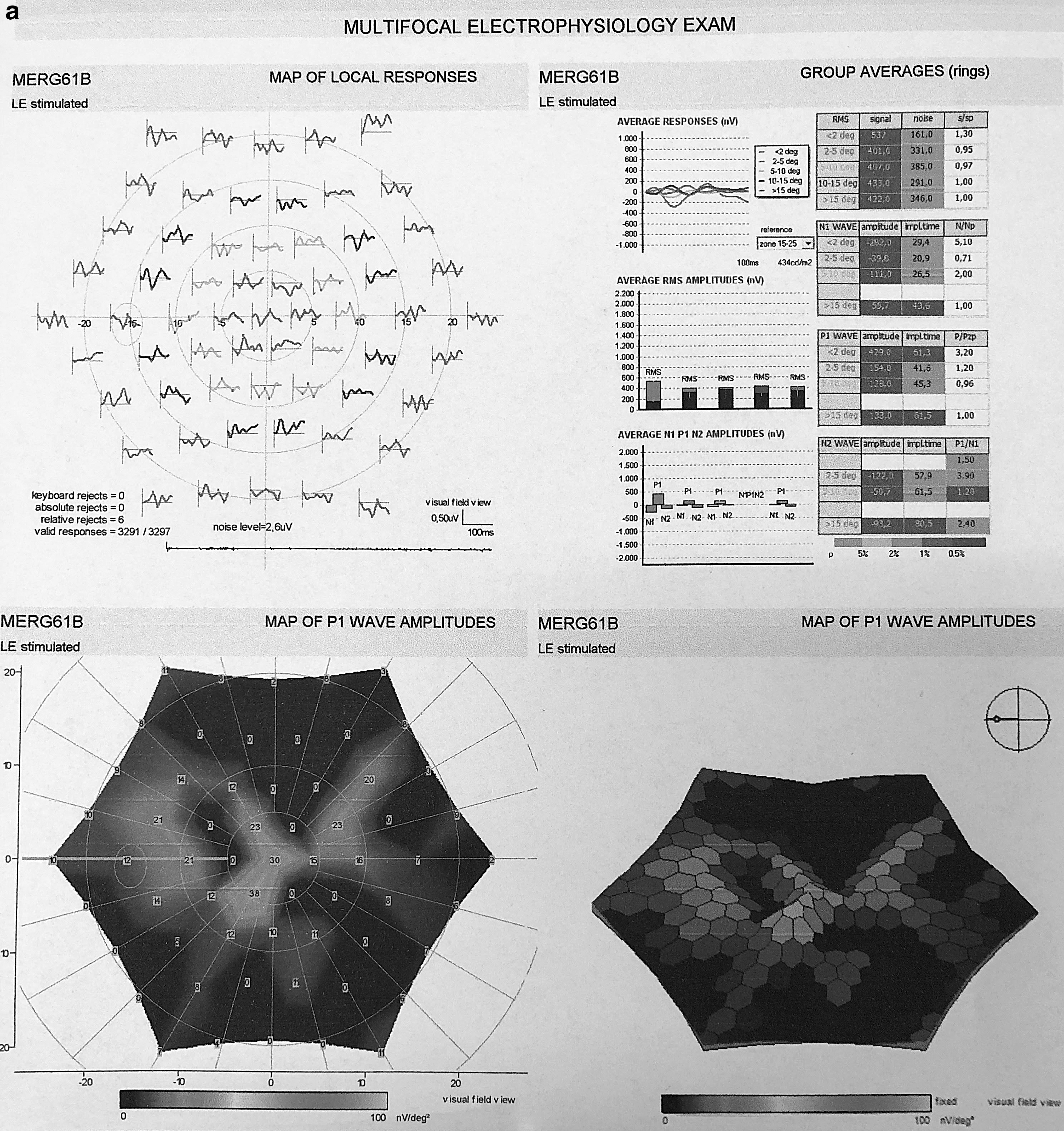
mfERG values were also obtained in 170 eyes of 85 patients. There was an increase in p1 wave amplitude values in rings 1, 2, and 3 at 1 month control, which was statistically significant (P < 0.05). The mean latency of the p1 wave showed statistically significant shortening in rings 1 and 2. These improvements partially disappeared at the 6-month follow-up. There was no significant differences in the values of rings 4 and 5 (Tables 2 and 3 and Fig. 5a, b).
Multifocal Electroretinogram Results of the Patients During the Follow-Up Examinations, P Wave Amplitude, Nanovolts
Mean ± SD.
Multifocal Electroretinogram Results of the Patients During the Follow-Up Examinations, P Wave İmplicit Time, Milliseconds
Mean ± SD.
Discussion
RP is known as a genetic retinal disease that causes irreversible blindness by progressive degeneration of retina cells. Although there is no curative treatment for the disease up to date, new approaches, including restoring defective genes and stem cell transplantation to replace defective or dead cells, have been under investigation.2,3
There are successful results of TES in experimental studies. TES could prevent the degeneration of retinal cells and the deterioration of retinal function in an animal model of RP. There was also a preservation of b waves in the ERG. According to the ERG results, the protective effect of TES was better in cone photoreceptors than rods. During these animal studies, fundus examinations were performed and no serious complications were seen such as retinal detachment and vitreous hemorrhage. TES was reported as a safe and a reliable method for retinal tissues.4,5,18,19
Up to date, there is no standard treatment protocol of TES for all pathologies. In an experimental study by Morimoto et al., the researchers used different parameters of intensity, frequency, pulse duration, waveform, and number of sessions to assess the optimal parameters for TES. They reported that the best neuroprotective effect on RGCs was achieved with these stimulation parameters: 1 and 2 ms per phase, 100 and 200 mA, frequency of 1.5 and 20 Hz, and at least a 30-min duration in rats. 20 Inomata et al. showed that the strength of the signals increased with longer stimulus durations, and the maximum signals were achieved when the stimulation frequency was between 15 and 20 Hz. 12
In RP disease, vascular attenuation and obliteration of the vessels were seen. This led to deterioration of retinal blood flow and retinal cells. TES application in healthy human subjects showed an increase in central chorioretinal blood flow. 21 Another sham controlled study with healthy human subjects suggested that TES increased the retinal blood flow after a single application of 30 min. They suggested that TES could regulate the retinal blood flow and prevent the visual impairment induced by ischemic insults. 11
In recent years, the number of clinical studies, including the results of clinical applications of TES, is increasing. In a study including 24 RP patients who received TES treatment for 6 consecutive weeks, significant improvements in VF and scotopic b wave amplitude have been reported. RP cases were separated into 3 groups according to the electrical stimulation power (0%, 66%, 150%). Visual function of the patients showed an increase or stabilization in the 150% group; on the contrary, no significant changes were observed in the other groups. 9
The results of a prospective, controlled, randomized trial of 1-year follow-up of TES treatment in the 52 RP cases were reported by Schatz et al. In this study, the VA, VF, and ERG of the sham, 150%, and 200% groups were compared. The results of this study showed that visual loss was prevented and the VF had a tendency to be protected in the 200% group. There was also a statistically significant improvement in the b wave amplitudes of photopic ERG in the 200% and 150% groups compared with the sham group. Although scotopic b wave amplitudes showed an improvement in the 200% group, the difference was not statistically significant. 14 Regarding the side effects, no symptoms other than mild dry eye symptoms were observed. As a conclusion, this study reported that TES is a safe method to protect retinal function in RP cases. 14
A short-term, randomized-controlled trial with 7 RP subjects showed that 4 of the patients experienced improvements in VA, contrast sensitivity, and VF tests. They received 6 weekly TES sessions and the improvements were preserved for a month after the cessation of the therapy. 22
A case series of retinal artery occlusion showed that both VA and VF improved after TES. In addition, it was reported that the latency and amplitude of all waves in the multifocal ERG significantly improved. It was suggested that TES had positive effects on whole retina layers.12,16
Our study included 101 subjects with RP, and to the best of our knowledge, this is the biggest number of patients in the literature. Based on previous studies, our study was carried out for 8 consecutive weeks. When setting the dose, the rate reported to be effective in this study was considered and 150% of the minimum perceptible amount was applied. The patients were treated with TES for 30 min every week for 8 consecutive weeks.
Our results showed that TES led to an increase in VA and VF tests. Although these improvements disappeared partially at 6-month control, 4 months after the cessation of the therapy, the values were significantly higher from baseline values. These findings may indicate that the beneficial effect of the treatment could be preserved after the cessation of the therapy. We found an increase in the amplitude and shortening in the latency of p1 waves in the central rings. These findings may demonstrate that TES is mostly effective on central retina. Another explanation for this observation may be the degenerative course of the disease in the periphery. Affected rod photoreceptors cause peripheral deterioration of the mfERG recordings. Cone functions can be preserved until the end stage of the disease. As a result of the course of the disease, the effects of TES may be seen mainly on central retinal function in this study. Regarding safety, dry eye findings were found as side effects and artificial tear support was routinely prescribed to the patients. No serious ocular or systemic complications were observed during the 6-month follow-up period of the study.
Limitations of the study
The limitations of our study can be listed as follows.
We know that the follow-up period is short for a progressive degenerative disease such as RP. Therefore, long-term control is needed to evaluate the duration of this treatment.
Up to date, there are no clear data on the frequency and continuity of TES application. We applied 8 consecutive TES sessions in 2 months. Since this is a new clinical practice, further studies on the frequency and continuity of treatment will clarify this issue.
Another limitation is the lack of data about molecular characterization of the patients. It is known that RP is a heterogenous group of disorders. Genetic analysis of most of the patients was not available, and so, we cannot clarify if there is a subset of patients who may benefit most from this treatment.
There is another limitation about the evaluation methods used in the study. VF is a subjective test, and therefore, the addition of a more objective test such as microperimetry will contribute to the assessment of the results in a more objective and reliable way. Hence, the full field flash ERG recordings of most of the patients were undetectable, mfERG was used to evaluate the retinal function in our study.
We believe that long-term follow-up studies, including tests such as microperimetry and OCT angiography, would be more valuable to understand the effect and mechanism of action of TES treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.