
Abstract
Purpose:
To analyze changes in the levels of angiogenic and inflammatory cytokines following the administration of intravitreal conbercept (IVC) or intravitreal ranibizumab (IVR) in patients with macular edema (ME) due to central retinal vein occlusion (CRVO).
Methods:
This retrospective study was conducted between June 2015 and January 2016 in The First Hospital of China Medical University. We administered 3 consecutive monthly doses of IVC (23 eyes) or IVR (19 eyes) in 42 eyes with CRVO-ME. At each injection, we collected aqueous humor samples and used multiplex bead assays to measure 7 angiogenic and inflammatory cytokines [vascular endothelial growth factor (VEGF), placental growth factor (PlGF), platelet-derived growth factor (PDGF)-AA, monocyte chemoattractant protein (MCP)-1, and interleukins (ILs)-6, 8, and 12].
Results
: Visual acuity and ME improved significantly in both groups during the treatment period. Compared with the baseline, all the cytokine concentrations in the aqueous humor samples decreased significantly at 1 and 2 months after the initial dose of IVC or IVR. The improvement of visual acuity and ME and the changes of aqueous humor cytokine levels were similar in both groups. Concentrations of VEGF, PlGF, MCP-1, PDGF-AA, IL-6, IL-8, and IL-12 levels did not show significant intergroup differences after 1 month (P = 0.369, 0.312, 0.185, 0.353, 0.135, 0.487, and 0.337, respectively) and 2 months (P = 0.305, 0.376, 0.230, 0.519, 0.114, 0.960, and 0.830, respectively) of follow-up.
Conclusion:
IVC and IVR induced comparable improvements in clinical parameters, along with equivalent reductions in the concentrations of angiogenic and inflammatory cytokines in the aqueous humor.
Introduction
Among the retinal diseases, central retinal vein occlusion (CRVO) holds the second position in terms of frequency, immediately after diabetic retinopathy. Perfused or nonperfused macular edema (ME) occurs commonly in patients with CRVO and accounts for most cases of visual loss. After it was reported that intraocular vascular endothelial growth factor (VEGF) contributes to CRVO-related ME, anti-VEGF agents were considered the first-line therapy for ME due to CRVO. 1 Four currently available VEGF antagonists, namely, pegaptanib, bevacizumab, ranibizumab, and aflibercept, have been developed and verified in CRVO-ME patients. More recently, conbercept has also been approved. 2 Conbercept was intended to ensure a more potent and prolonged anti-VEGF effect. China Food and Drug Administration approved it in November 2013. Conbercept comprises VEGF-binding domains of human VEGF receptor (VEGFR)-1 and -2 in combination with the human immunoglobulin G1's Fc portion. Aside from having a high affinity for VEGF-A isoforms, conbercept reacts with VEGF-B and placental growth factor (PlGF). Conbercept has an additional fourth VEGF receptor (VEGFR)-2-binding domain that is absent in aflibercept. This domain is crucial for receptor dimerization and enhanced bonding of VEGF and VEGFR. Previous studies have demonstrated the effectiveness of conbercept in treating ME secondary to CRVO.2–4
CRVO pathogenesis involves increased permeability of capillaries that leads to edema, increased venous pressure, and hypoxia. 5 The substrate lies in VEGF- and inflammatory-cytokine-mediated damage of the blood–retina barrier. Studies have found elevated ocular concentrations of cytokines (angiogenic and inflammatory) in patients with CRVO, suggesting that the angiogenic and inflammatory cytokine network plays an important role in CRVO.6–9 To investigate the biological implications of antiangiogenic therapy in CRVO patients, several studies evaluated the effects of intravitreal administration of drugs from anti-VEGF family on intraocular concentrations of cytokines.10,11 For example, a previous study showed that the aqueous humor levels of angiogenic and inflammatory cytokines were significantly reduced by ranibizumab therapy in patients with CRVO. 12 Our previous study also demonstrated that conbercept treatment influenced various inflammatory cytokine concentrations and reduced VEGF and PlGF concentrations in the aqueous humor of patients with CRVO. 13 However, differences in changes in the levels of angiogenic and inflammatory cytokines following the administration of different anti-VEGF agents require further elucidation.
This study investigates and compares the changes in angiogenic and inflammatory cytokine aqueous humor levels in patients with CRVO-related ME after intravitreal administration of conbercept (IVC) or ranibizumab (IVR), the 2 most widely used anti-VEGF agents in China. To the best of our knowledge, this is the first study to compare the changes in intraocular cytokine levels following conbercept and ranibizumab treatment in CRVO patients.
Methods
Study subjects
The present retrospective study was conducted between June 2015 and January 2016 at the Department of Ophthalmology in The First Hospital of China Medical University (Shenyang, China). The ethical and review board of the university approved the protocol. Each patient provided a written informed consent before treatment, and all procedures were conducted according to the provisions of the Declaration of Helsinki for human research.
The inclusion criteria were ME secondary to CRVO treated with IVC or IVR; best-corrected visual acuity (BCVA) of <20/40, and baseline central retinal thickness (CRT) ≥250 μm owing to the presence of intraretinal fluid or subretinal fluid, measured using optical coherence tomography (OCT); and the completion of 3 successive monthly injections. The exclusion criteria were rubeosis iridis, presence of neovascularization on the optic disc or elsewhere, severe ischemic retinopathy (fluorescein angiography [FA]-detected 10 disc areas of nonperfusion), intravitreal treatment with corticosteroids or with anti-VEGF agents or laser photocoagulation during 6 months before the study; intraocular surgery, glaucoma, or ocular hypertension, and retinal conditions other than CRVO.
Full ophthalmologic evaluation was conducted on each eye at baseline. BCVA was measured using the standard Snellen chart. Other methods applied included slit-lamp biomicroscopy, measuring intraocular pressure (IOP), and indirect ophthalmoscopy. Moreover, we applied spectral-domain OCT (Spectralis, Heidelberg Engineering, Heidelberg, Germany), as well as FA (HRA 2; Heidelberg Engineering).
Treatment with IVC or IVR
Each patient received 3 consecutive monthly intravitreal injections of conbercept at a dose of 0.5 mg per 0.05 mL (KH902; Chengdu Kanghong Biotech Co., Ltd., Sichuan, China) or ranibizumab (Lucentis; Novartis, Pharma AG, Switzerland, and Genentech, Inc., South San Francisco, CA). Each injection was administered in an operating room under sterile conditions. Briefly, after cleaning the eyelid with a povidone-iodine solution an eyelid speculum was introduced. Then, after the application of topical anesthesia, 5% povidone-iodine was used to irrigate the conjunctiva. The operator inserted a 30-gauge needle through the pars plana and administered an intravitreal injection of 0.05 mL of conbercept or ranibizumab.
At 1 day, 1 week, and 1 month after the first IVC or IVR administration, as well as at monthly intervals thereafter, follow-up examinations encompassing BCVA testing, slit-lamp examination, IOP measurement, indirect ophthalmoscopy, and OCT were performed.
Sample collection
The samples of aqueous humor were collected while administering of IVC or IVR each time. A 30-gauge needle on an insulin syringe was used for anterior chamber limbal paracentesis and collection of ∼0.1 mL (mean volume) of aqueous humor. Immediately after collection, the fluid samples were placed in sterile plastic tubes to be kept at −80°C until analysis.
Age-matched patients undergoing cataract surgery provided reference samples. The exclusion criteria for controls comprised any type of retinal disorder, previous ocular surgery, glaucoma, laser photocoagulation, and recent history of medication. Before routine cataract surgery, aqueous humor samples were immediately collected using limbal paracentesis. These samples were stored at −80°C until analyzed.
Measuring angiogenic and inflammatory cytokines
Suspension array technology (xMAP; Luminex Corp., Austin, TX) and capture bead kits (Beadlyte; Upstate Biotechnology, Lake Placid, NY) were used for measuring the concentrations of angiogenic and inflammatory cytokines (VEGF, PlGF, platelet-derived growth factor (PDGF)-AA, monocyte chemoattractant protein (MCP)-1, as well as interleukins IL-6, -8, and -12 (P 70)). The kits were used as recommended by the manufacturers.
Statistical analysis
For statistical analysis, Snellen visual acuity was converted to the logarithm of minimal angle of resolution (logMAR) equivalent. Depending on the distribution, the data were represented as mean values with standard deviations (SDs) or medians with range. Normal distribution was tested using histogram analysis and Shapiro–Wilk test. In case of normally distributed data, a 2-tailed t-test was conducted to compare 2 groups; otherwise, the Wilcoxon signed rank test and the Mann–Whitney U-test were utilized. Adjustment methods for multiple comparisons (Bonferroni test, SNK test, and Tukey's HSD test) were performed to confirm our results. Fisher's test was used for comparisons of categorical data. Statistical significance was ascertained when P values were below 0.05. All analyses were performed using SPSS v20 (IBM Corp., Armonk, NY).
Results
Characteristics at baseline
In this study, we included 42 eyes/patients (23 and 19 eyes in the IVC and IVR groups, respectively). Table 1 shows the baseline characteristics of the IVC and IVR groups. There were no significant differences between the groups in mean age, sex, duration of symptoms, type of ME (presence of serous retinal detachment, SRD), and presence of hypertension or diabetes mellitus.
Baseline Clinical Features of Eyes Treated with Conbercept and Ranibizumab
BCVA, best-corrected visual acuity; CRT, central retinal thickness; IL, interleukin; logMAR, logarithm of minimal angle of resolution; MCP, monocyte chemoattractant protein; PDGF, platelet-derived growth factor; PlGF, placental growth factor; VEGF, vascular endothelial growth factor.
The mean ± SD logMAR of BCVA at baseline was 0.70 ± 0.21 (Snellen equivalent, 20/100) in the IVC group compared to 0.78 ± 0.20 (Snellen equivalent, 20/121) in the IVR group (P = 0.248). The OCT-measured CRT at baseline was 583.4 ± 204.0 μm and 612.3 ± 195.7 μm in the IVC and IVR group, respectively (P = 0.649).
Visual and anatomic outcomes
The logMAR of BCVA after 1 month in the IVC group increased significantly to 0.53 ± 0.23 (P = 0.012); similarly, there was an increase in the IVR group to 0.58 ± 0.22 (P = 0.007). The mean BCVA changes were similar between IVC and IVR groups (P = 0.523). The mean logMAR of BCVA continued to improve and was 0.48 ± 0.22 (P = 0.002) and 0.53 ± 0.23 (P = 0.002) after 2 months of follow-up in the IVC and IVR group, respectively; no intergroup differences were observed at that time point either (P = 0.531). CRT was reduced at 1 month after the initial treatment to 282.1 ± 67.6 μm (P < 0.001) and 299.2 ± 95.4 μm (P < 0.001) in the IVC and IVR group, respectively. After 2 months, we observed a further decrease in CRT in both groups (IVC: 255.3 ± 52.2 μm, P < 0.001; IVR: 268.1 ± 73.9 μm, P < 0.001). Both groups showed similar changes in mean CRT values after 1 and 2 months of follow-up (P = 0.733 and 0.791, respectively). The changes in BCVA and CRT from baseline over 2 months are shown in Figs. 1 and 2.
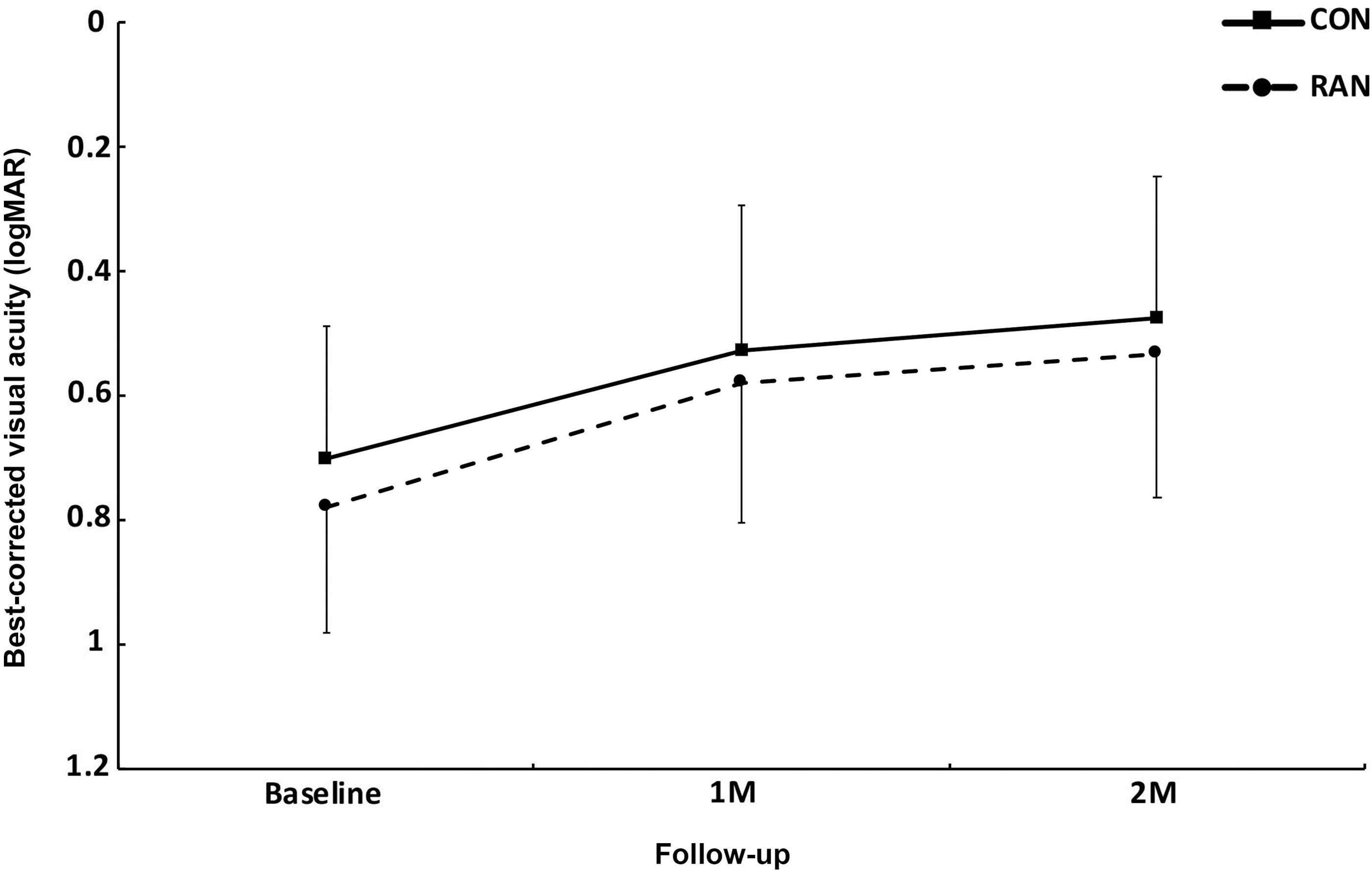
Changes in the mean logMAR of BCVA during the course of 3 consecutive monthly IVC or IVR injections for the treatment of ME secondary to CRVO. Error bars indicate the SD from the mean. BCVA, best-corrected visual acuity; logMAR, logarithm of minimal angle of resolution; IVC, intravitreal conbercept; IVR, intravitreal ranibizumab; ME, macular edema; CRVO, central retinal vein occlusion; SD, standard deviation.
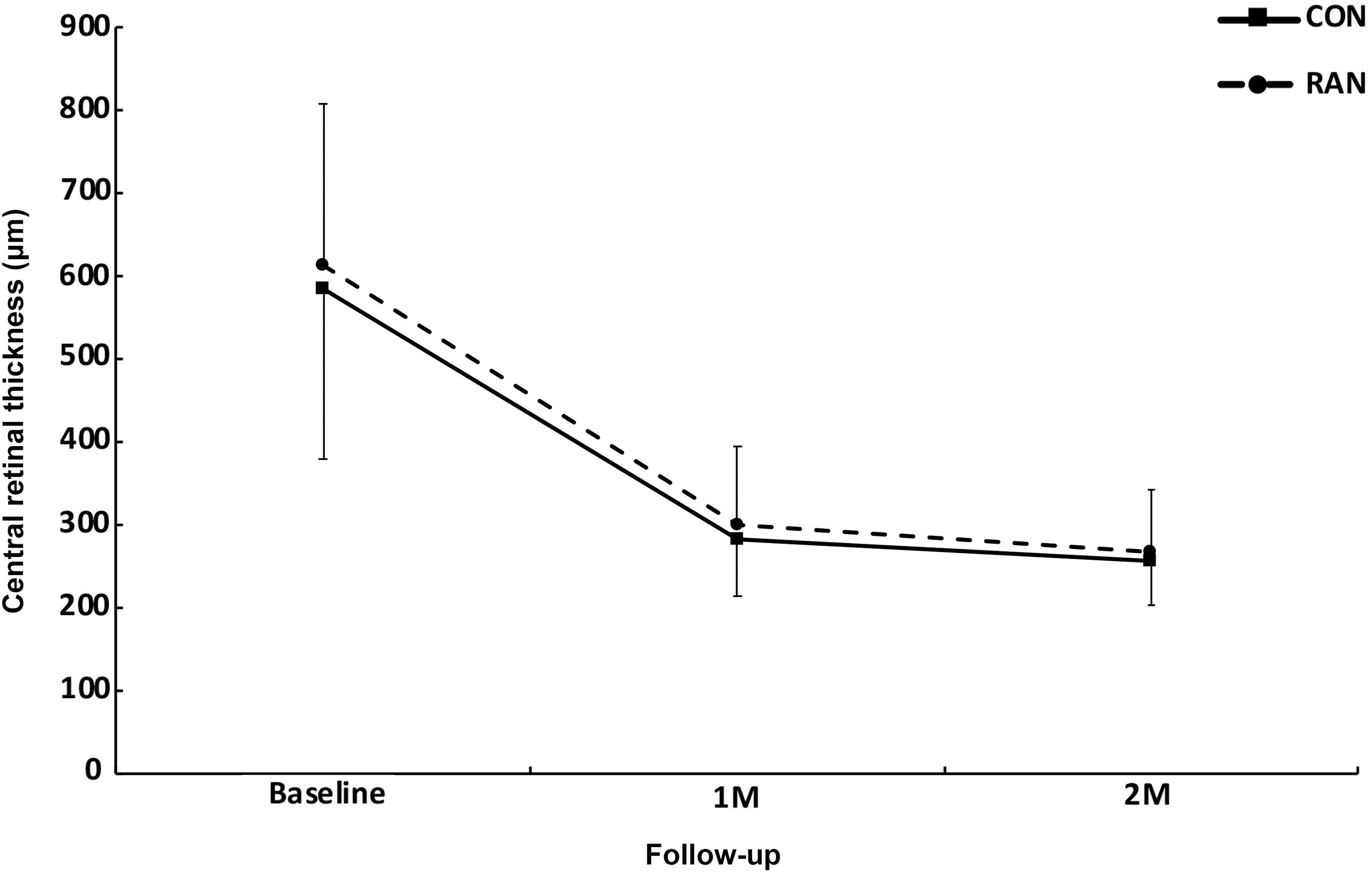
Changes in mean CRT during the course of 3 consecutive monthly IVC or IVR injections for the treatment of ME secondary to CRVO. Error bars indicate the SD from the mean. CRT, central retinal thickness.
No systemic or ocular complications were observed.
Cytokine concentrations after conbercept and ranibizumab administration
Table 1 shows the baseline levels of 7 angiogenic and inflammatory cytokines measured (Table 1). There were no significant intergroup differences in terms of the concentrations of each cytokine in the aqueous humor. The mean levels of VEGF, PlGF, MCP-1, PDGF-AA, IL-6, IL-8, and IL-12 in reference samples were 29.9 ± 6.7, 1.8 ± 0.7, 402.0 ± 75.6, 28.1 ± 6.4, 2.7 ± 0.9, 2.4 ± 0.7, and 3.1 ± 0.8 pg/mL, respectively. All cytokine levels in CRVO patients were significantly higher than those observed in control patients (P < 0.001 for all).
The cytokine levels during conbercept and ranibizumab treatment are shown in Fig. 3. Under therapy with 3 consecutive monthly IVC injections, the concentrations of angiogenic cytokines declined significantly. After 1 month of follow-up, the mean level of VEGF and PlGF decreased significantly to 35.3 ± 29.3 pg/mL (P < 0.001) and 3.4 ± 1.5 pg/mL (P < 0.001), respectively. The trend of decrease in VEGF and PlGF continued at 2 months after the treatment (24.2 ± 26.1 pg/mL and 2.1 ± 0.9 pg/mL (both P < 0.001) in IVC group, respectively). IVR group showed similar results. After 1 month of follow-up, the mean level of VEGF and PlGF decreased significantly to 43.5 ± 31.5 pg/mL and 4.2 ± 1.8 pg/mL, respectively (both P < 0.001); further decrease was notable at 2 months [29.0 ± 29.0 pg/mL and 2.4 ± 1.3 pg/mL, respectively (both P < 0.001)]. The concentrations of VEGF and PlGF did not differ significantly between the groups after 1 month (P = 0.369 and 0.312, respectively) and 2 months of follow-up (P = 0.305 and 0.376, respectively).
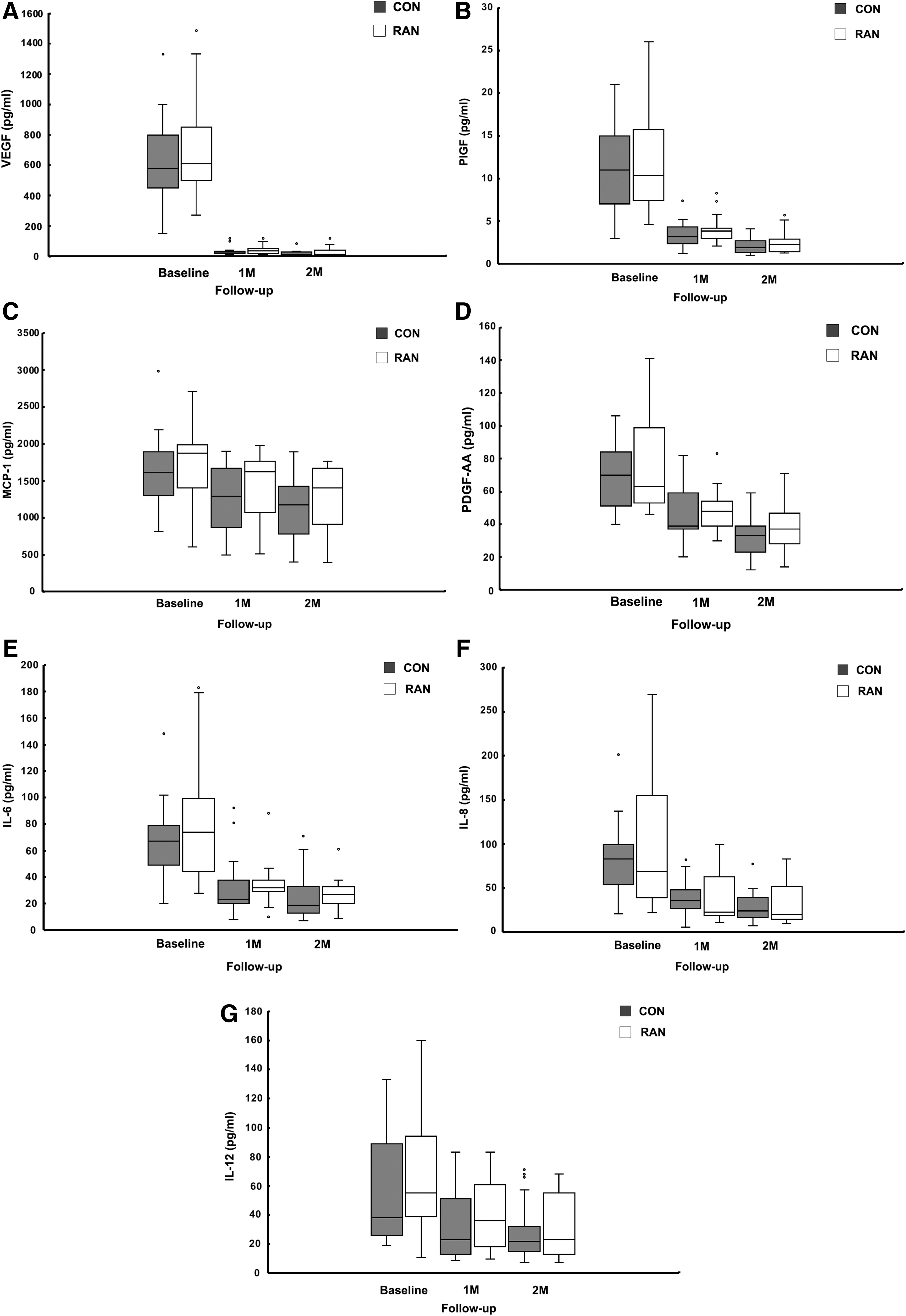
Concentrations of angiogenic and inflammatory cytokines in patients with ME secondary to CRVO during the course of 3 consecutive monthly IVC or IVR injections (
Inflammatory cytokines (including MCP-1, PDGF-AA, IL-6, IL-8, and IL-12) in the IVC group showed lower concentrations at 1 month of follow-up: 1,266.8 ± 423.9 pg/mL (P = 0.033), 45.5 ± 16.2 pg/mL (P < 0.001), 31.7 ± 20.0 pg/mL (P < 0.001), 38.5 ± 17.6 pg/mL (P < 0.001), and 31.4 ± 23.0 pg/mL (P = 0.010), respectively, as well as further decrease at 2 months: 1,112.3 ± 436.9 pg/mL (P = 0.002), 33.2 ± 11.6 pg/mL (P < 0.001), 24.9 ± 17.0 pg/mL (P < 0.001), 28.3 ± 16.3 pg/mL (P < 0.001), and 27.6 ± 19.2 pg/mL (P = 0.001), respectively. As with the angiogenic cytokines, similar results were achieved for inflammatory cytokines in the IVR group. Similarly, the IVR group showed significantly decreased concentrations of inflammatory cytokines (MCP-1, PDGF-AA, IL-6, IL-8, and IL-12) at 1 month after the treatment: 1,427.5 ± 438.0 pg/mL (P = 0.030), 48.1 ± 13.0 pg/mL (P < 0.001), 34.1 ± 15.5 pg/mL (P < 0.001), 41.8 ± 31.0 pg/mL (P = 0.003), and 38.1 ± 23.4 pg/mL (P = 0.008), respectively; at 2 months of follow-up, the levels further decreased to: 1,276.1 ± 447.5 pg/mL (P = 0.004), 36.7 ± 14.2 pg/mL (P < 0.001), 27.6 ± 11.2 pg/mL (P < 0.001), 32.9 ± 24.0 pg/mL (P < 0.001), and 31.1 ± 20.9 pg/mL (P = 0.002), respectively. The concentrations of MCP-1, PDGF-AA, IL-6, IL-8, and IL-12 did not show significant intergroup differences after 1 month (P = 0.185, 0.353, 0.135, 0.487, and 0.337, respectively) and 2 months (P = 0.230, 0.519, 0.114, 0.960, and 0.830, respectively) of follow-up.
Discussion
Since the initial evidence indicating the role of VEGF in ischemic and inflammatory eye diseases, a variety of angiogenic and inflammatory cytokines have been confirmed at ME. 14 However, the complex chain of events involved in this process is yet to be completely elucidated. In addition to angiogenic cytokines, elevated intraocular levels of numerous inflammatory cytokines have been reported in patients with CRVO-ME, and their correlation with retinal thickness has been demonstrated. 15 Our previous study showed high expression of both angiogenic and inflammatory cytokines (including VEGF, PlGF, MCP-1, PDGF-AA, IL-6, IL-8, and IL-12) in eyes with CRVO-ME, suggesting their role in CRVO. 13 VEGF is a primary proangiogenic cytokine. The cells of damaged retina and choroid secrete VEGF in response to ischemia-induced abnormal vascular perfusion; therefore, VEGF is considered as a critical player in CRVO-ME pathogenesis. 15 Furthermore, substantial overlap is observed in the VEGF and inflammatory cytokine pathways. Pro-inflammatory cytokines (such as IL-1, IL-6, IL-8, MCP-1, transforming growth factor beta, and tumor necrosis factor alpha) are associated with VEGF expression.16,17 VEGF stimulates the expression of several pro-inflammatory genes and permits leukocyte infiltration into the retina.18,19 Theoretically, as VEGF is a pro-inflammatory mediator, anti-VEGF therapy may suppress intraocular cytokine levels.
Previous studies analyzed how anti-VEGF agents affect intraocular cytokine concentrations, but the results are conflicting. For example, Wen et al. evaluated the changes in VEGF and inflammatory cytokine concentrations following intravitreal bevacizumab (IVB) for CRVO-ME 10 and showed significantly reduced VEGF and unchanged MCP-1 and IL-6 levels after IVB. In contrast, Noma et al. showed significantly decreased intraocular concentrations of VEGF, PDGF-AA, MCP-1, and IL-8 in patients with ME secondary to CRVO after IVB treatment. 11 Similar findings were observed in patients with ME secondary to CRVO following IVR therapy, in whom intraocular concentrations of angiogenic cytokines (VEGF and PlGF) and inflammatory cytokines (MCP-1, PDGF-AA, and IL-6) were reduced by IVR treatment. 12 In our present study, IVC or IVR was administered at 3 monthly doses to treat CRVO-ME. Compared with the baseline levels of aqueous humor, those of VEGF, PlGF, MCP-1, PDGF-AA, IL-6, IL-8, and IL-12 declined significantly at 1 and 2 months after the initial dose of IVC or IVR. IVC and IVR groups showed similar cytokine levels during treatment. Similarly, a previous study with ranibizumab and aflibercept demonstrated reduced ocular VEGF, PlGF, and inflammatory cytokine (MCP-1 and IL-6) levels in both agents, without any interagent differences. 20
We found that both IVC and IVR reduced the ocular concentration of PlGF in CRVO-ME patients. Based on its chemical structure, it was expected that conbercept would reduce the levels of PlGF. 2 Of note, ocular ligands of VEGF and PlGF are present in the form of homodimers or heterodimers (VEGF/VEGF and PlGF/PlGF, or VEGF/PlGF, respectively). 21 Therefore, ranibizumab may have significantly suppressed PlGF by neutralizing the heterodimers (VEGF/PlGF). Moreover, VEGF upregulates PlGF through the protein kinase C signaling pathway in endothelial cells. 22 Therefore, VEGF suppression by ranibizumab treatment could downregulate PlGF indirectly. The other notable finding was that both agents used in this study significantly affected various inflammatory cytokines in CRVO patients. As mentioned above, as a pro-inflammatory mediator, the binding of VEGF and VEGFR-2 promotes the expression of inflammatory cytokines.23–25 Therefore, IVC or IVR treatment may decrease inflammatory cytokine levels by suppressing signaling through VEGFR-2. PlGF may also have a role in inflammatory modulation as a VEGFR-1 ligand, which participates in the secretion of inflammatory cytokines by monocytes/macrophages. 26 Thus, inflammation may also be suppressed by PlGF neutralization in patients with CRVO treated by IVC or IVR injections.
The findings vary among the previous studies because of several possible reasons. First, various anti-VEGF agents were used across the different studies. Most studies do not demonstrate any significant effects of anti-VEGF therapy on the intraocular concentrations of inflammatory cytokines that used bevacizumab.10,27,28 Compared with bevacizumab, ranibizumab may exert more potent effects on the intraocular inflammatory cytokine profile, as the previous studies showed altered concentrations of various inflammatory cytokines that were altered by IVR therapy.12,29 Our previous study demonstrated that IVC has a significant impact on different inflammatory cytokines in CRVO patients. 13 Similarly, a previous study showed that conbercept could inhibit VEGF downstream inflammatory mediators in patients with ME secondary to retinal vein occlusion (RVO), as well as in a mouse model. 30 Second, patient cohorts may have impacted the results. In a previous study, the authors examined the relationship between angiogenic/inflammatory cytokines and retinal ischemia in RVO patients and found significantly increased concentration of VEGF and some inflammatory cytokines in ischemic RVO patients compared with nonischemic RVO. 8 Therefore, patients' characteristics, such as the type of CRVO (ischemic or nonischemic, central or branch) and duration of CRVO symptoms, may have influenced the levels of angiogenic and inflammatory cytokines at baseline, as well as changes observed following anti-VEGF therapy. On the other hand, we observed that baseline levels of each angiogenic and inflammatory cytokine varied widely among individual patients, from very high to very low levels. Because studies using low patient numbers may not capture the full picture, the small sample sizes may have influenced our results.
In our present study, the improvement achieved was similar with either conbercept or ranibizumab, possibly based on the comparable inhibitory effect on VEGF and PlGF. Similarly, the ocular levels of inflammatory cytokines were equivalent in both groups. Our findings corroborate the results of a previous study on similar efficacy of these 2 drugs in the vision improvement of CRVO patients. 31
OCT studies have shown that ME secondary to CRVO is frequently associated with subretinal SRD, as well as with cystoid macular edema and inner retinal thickening. In the present study, we included some CRVO patients with SRD. Although the mechanism underlying SRD associated with CRVO remains unclear, studies have found elevated ocular levels of VEGF, IL-6, and soluble intercellular adhesion molecule 1 in patients with CRVO-SRD, suggesting that the angiogenic and inflammatory cytokine network plays an important role in CRVO-SRD.32,33 In addition, Poon et al. demonstrated that the presence of SRD is an indicator of favorable clinical response after bevacizumab treatment in branch RVO (BRVO) patients. 34 Due to the small sample size, we did not perform statistical analysis to evaluate the cytokine levels or treatment outcomes in the CRVO-SRD patients in the current study. Further studies are warranted to investigate aqueous angiogenic and inflammatory cytokine concentrations in patients with CRVO-SRD and evaluate the efficacy of different anti-VEGF agents in the treatment of CRVO-SRD.
Our study was not without limitations. First, this was not a prospective study, which limits the generalizability of our findings. Second, sampling of aqueous humor instead of vitreous fluid was used as an indicator of pathology of primarily posterior segment. Despite higher levels of cytokines in the vitreous fluid, aqueous humor sampling is less invasive. In addition, because the cytokine levels in the aqueous humor correlate well with those of vitreous fluid, 35 analyzing their concentration in aqueous humor samples is both valuable and achievable. Third, the sample size was relatively small, and the follow-up period was short. The results of a recent systematic review and meta-analysis showed that conbercept was superior to ranibizumab in reducing CRT in RVO patients over 6 months, which could correlate with the intraocular level of cytokines, also requiring reduced number of injections after loading phase. 36 Confirmation of our results is needed in future studies.
In conclusion, in the present study, we demonstrated that both conbercept and ranibizumab treatment led to a comparable improvement in the measured clinical parameters and similar reductions in levels of angiogenic and inflammatory cytokines in aqueous humor of patients with ME due to CRVO. Further studies are required to better understand the complex network of signaling pathways in CRVO-ME, determine the relative importance of specific cytokines in the pathogenesis of CRVO-ME, and evaluate the utility of biomarkers in predicting response to anti-VEGF treatment.
Footnotes
Author Disclosure Statement
The authors declare that there are no competing interests.
Funding Information
Liaoning Science and Technology Project (No. 2013225303, H. Z.) supported this work. However, the funder played no role in the study design, data assembly or analysis, publishing decision, or article preparation.