
Abstract
Purpose:
To investigate the efficacy and safety of coadministered intravitreal dexamethasone (IVD) implant and silicone oil endotamponade during pars plana vitrectomy (PPV) for the treatment of proliferative diabetic retinopathy (PDR) with tractional diabetic macular edema (DME).
Methods:
In this prospective, controlled, and randomized clinical study, the eyes with PDR and vitreomacular traction syndrome that underwent PPV with silicone oil endotamponade were divided into 2 groups. Group 1 was defined as the control group, and no other procedures were performed. IVD was implanted to the eyes in Group 2. In both groups, panretinal photocoagulation was completed to the missed areas during PPV. All cases followed for 6 months, postoperatively. Retinal findings were followed with optical coherence tomography and fluorescein fundus angiography.
Results:
A total of 52 eyes of 52 patients were included in the study. Twenty-six eyes of 23 patients were included in both groups. The improvement in best corrected visual acuity was statistically significantly higher in Group 2 (P > 0.05). In the postoperative period, the DME development rate and intravitreal ranibizumab (IVR) injection requirement were significantly higher in Group 1 (P > 0.05). There was no statistically significant difference in the proliferative vitroretinopathy development rate between the groups (P < 0.05).
Conclusion:
Coadministration of IVD implant and silicone oil endotamponade to the eyes with PDR during vitrectomy seems to be safe and effective application and may decrease the rate of DME and the requirement of IVR injection.
Introduction
Proliferative diabetic retinopathy (PDR) with diabetic macular edema (DME) is one of the leading preventable visual loss in working-aged people.1,2 Since PDR affects the microvascular system in particular, the retina is one of the most common tissues in the body where pathologies are observed. PDR is also associated with high risk of fatality vascular complications such as stroke, coronary heart disease, and heart failure. Tight blood sugar and blood pressure could reduce the risk of developing PDR and DME. Vascular endothelial growth factor (VEGF) is thought to play a key role in pathophysiology. Photocoagulation of ischemic areas with argon laser or intravitreal injection of anti-VEGF drugs is always aimed to reduce VEGF activity. Apart from VEGF, there are also studies in the literature which advocate that pro-inflammatory mediators may have an important role in the development of PDR and DME. The positive contribution of intravitreal steroid injections to the treatment of PDR and DME supports this relationship. 3 In this prospective, controlled, and randomized clinical study, we aimed to investigate the safety and effectiveness of coadministration of silicone oil endotamponade and intravitreal dexamethasone (IVD) implant injection during the pars plana vitrectomy (PPV) in patients with PDR and tractional DME.
Methods
This prospective and randomized study was approved by the Institutional Ethics Committee of University of Health Sciences (Study number: 17073117-050.99-2789) and was organized and carried out in accordance with the principles and recommendations of the Helsinki Declaration. Informed consent was obtained from all patients who participated in the study. The eyes of patients with DME due to vitreomacular traction syndrome and PDR that presented to our clinic between January 2019 and February 2020 that underwent 23 gauge PPV with retrobulbar anesthesia were included in this study. Before the study, Nd:YAG capsulotomy laser was applied to the pseudophakic eyes in presence of posterior capsule opacification and cataract surgery to the phakic eyes before the study. Cataract surgery was made by phacoemulsification technique 3 weeks before PPV. Three-piece acrylic hydrophobic monofocal intraocular lens (Acrysof, MA60AC; Alcon) was implanted into the bag. Silicone oil endotamponade (1000 centistoke; Teknomek, Istanbul, Turkey) was implanted to all eyes during PPV. The eyes included in this study were divided into 2 groups randomly. No additional procedures were applied to eyes in Group 1 (control group). Intravitreal dexamethasone (IVD, OZURDEX®; Allergan, Inc., CA) implant was coadministrated to the eyes in Group 2 during PPV.
Cases with intense vitreous hemorrhage, macular ischemia, retinal detachment, previous macular laser treatment, nontractional DME, type I diabetes mellitus, glaucoma, amblyopia, corneal pathology, and uveitis and patients with glycosylated serum hemoglobin A1c greater than 10% were excluded from the study. The eyes included in the study were followed for 6 months. Intravitreal ranibizumab (IVR) (LUCENTIS®; Genentech, Inc., San Francisco) injection was applied to all eyes 3 days before PPV to reduce the risk of hemorrhage during surgery. During the PPV operation, panretinal photocoagulation (PRP) was applied to missed areas, fibrovascular membranes were dissected, internal limiting membrane (ILM) was peeled, and 1000 centistoke silicone oil endotamponade (Teknomek) was implanted to all the eyes. While the eyes were filled with air, the IVD implant was placed on the inferior retina and then silicone oil endotamponade was injected. Silicone endotamponade was removed from all eyes 3 months later. All operations were performed by the same experienced vitreoretinal surgeon (A.A.) using the same instrument (Constellation; Alcon).
Full ophthalmologic examination was performed monthly. DME was followed with optical coherence tomography monthly, and fundus fluorescein angiography was performed in the sixth month. The best corrected visual acuity (BCVA), presence of DME, and intraocular pressure (IOP) were measured during the 6-month-follow-up period. Visual acuities were measured with Snellen chart and converted to Logarithm of the Minimum Angle of Resolution (LogMAR) equivalents for statistical analysis.
Results
A total of 52 eyes of 52 patients were included in this study. Both groups had 26 eyes of 26 patients. All patients had Caucasian ethnicity. In the postoperative period, there was no uncontrolled IOP elevation in any of the patients. The mean age was 55.58 ± 4.40 and 54.23 ± 4.51 years, and the ratio of female:male was 14:12 and 12:14 in Group 1 and Group 2, respectively. There were no significant differences between the groups with respect to age and gender (P > 0.05) (Table 1).
Demographic Characteristics of the Groups
Mann–Whitney U test.
Chi-square test.
IVD, intravitreal dexamethasone; SD, standard deviation.
In both groups, statistically significant improvement in BCVA was developed in the postoperative period compared to the preoperative period. The improvement level in BCVA in Group 2 was statistically significantly higher compared to Group 1 in the whole postoperative 6-month follow-up period (P < 0.01) (Table 2 and Fig. 1).

Visual acuity change of the groups. BCVA, best corrected visual acuity; IVD, intravitreal dexamethasone.
Visual Acuity Change of the Groups
Mann–Whitney U test.
BCVA, best corrected visual acuity; LogMAR, Logarithm of the Minimum Angle of Resolution.
In the first 3 months of the postoperative period, the presence of DME in Group 2 was statistically significantly less than Group 1 (P < 0.05), but in the later period, there was no significant difference between the groups although it was more rare in Group 2 (P > 0.05) (Table 3 and Fig. 2).
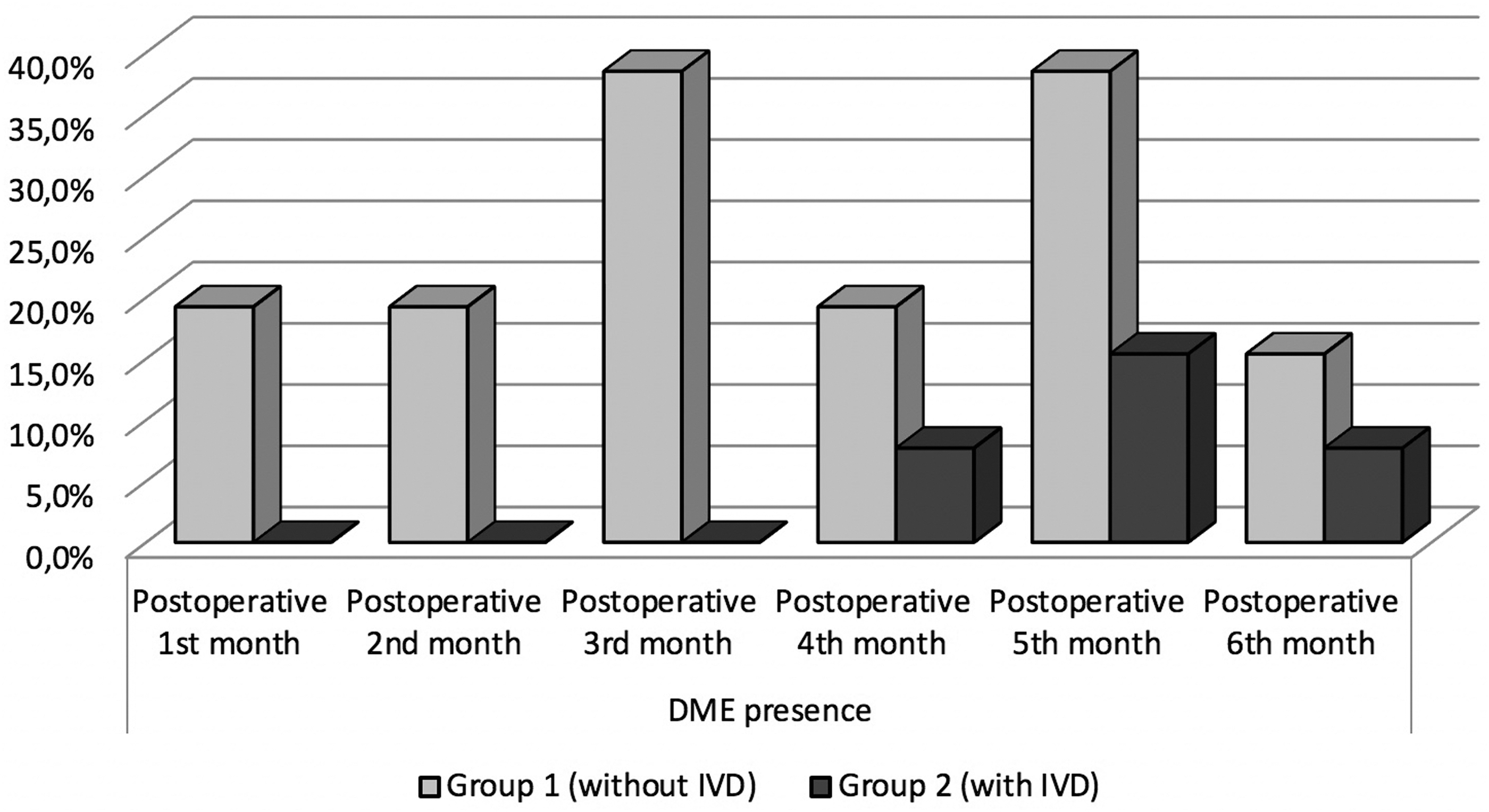
Presence of DME in the postoperative period in groups. DME, diabetic macular edema.
Presence of Diabetic Macular Edema in the Postoperative Period in Groups
Chi-square test.
DME, diabetic macular edema.
In the postoperative period, the need for IVR injection in Group 1 was required once in 4 eyes, twice in 9 eyes, and 3 times in 3 eyes. In Group 2, IVR injection was required once in 6 eyes and 2 times in 3 eyes. The mean IVR requirement was significantly lower in Group 2 than in Group 1 (P < 0.05). The PVR development rate after PPV in Group 1 and Group 2 was 11.5% and 3.8%, respectively. Although the PVR development rate in Group 2 was lower than Group 1, there was no statistically significant difference between the 2 groups (P = 0.298) (Table 4 and Fig. 3).

The number of intravitreal ranibizumab injections in the postoperative period.
Number of Ranibizumab Injections and Proliferative Vitreoretinopathy in Groups Postoperatively
Chi-square test.
IVR, intravitreal ranibizumab; PVR, proliferative vitroretinopathy.
Discussion
DME is one of the most important causes of vision loss in diabetic patients, and the risk of development is higher in patients with PDR. 4 DME may develop in 7% of patients with diabetes mellitus, and the risk factors contributing to its development are largely similar to PDR. 5 It has been reported that when systemic factors such as blood sugar and diastolic blood pressure are tightly controlled in DM patients, the risk of developing DME decreases. 6 In order for these systemic parameters to not negatively affect the results of our study and the comparison between groups, we excluded cases with HbA1c greater than 10% or uncontrolled hypertension in the last 3 months.
In the literature, many treatment methods have been identified in the treatment of DME. PRP,7–9 grid or micropulse yellow laser,10–12 intravitreal injection of anti-VEGF drugs,13–16 subtenon or intravitreal injection of glucocorticoid drugs,17,18 and PPV19,20 are the most known options. PRP is a standard treatment that has been showing its benefit in PDR management for nearly 40 years by reducing VEGF release from ischemic areas. 21 Most of the patients that we included in our study were treated with PRP previously. However, we completed the PRP applications to the missing parts of the peripheral retina that were difficult to access previously, during PPV.
PPV may benefit the treatment of PDR by dissecting fibrovascular membranes that form traction on the retina. 22 Nasrallah et al. reported that eyes with DME have a lower prevalence of posterior vitreous detachment than eyes without DME and suggested that vitreomacular adhesion may play a role in the development of DME. 23 Posterior vitreous detachment induced by vitrectomy may remove this adhesion and contribute to the treatment of DME. Vitrectomy for the treatment of DME was first performed in 1992, 24 and many studies have been done since.25–29 All of the eyes included in this study had tractional DME. We peeled ILM in all cases during PPV operation to eliminate vitreomacular traction and dissected existing fibrovascular membranes. Intravitreal injection of anti-VEGF drugs 3 days before the operation may improve PPV results and facilitate ILM peeling. 30 In our study, for the same purposes, we injected IVR to all eyes 3 days before the PPV operation.
Although silicone oil endotamponade is most commonly applied in surgeries for retinal detachment, it might be a method for other purposes today. In eyes with PDR during the vitrectomy operation, silicone oil endotamponade could be applied to prevent recurrent intravitreal hemorrhage and allow rapid visual recovery. 31 Kanclerz et al. reported that silicone endotamponade ensures effective hemostasis in eyes with PDR. 32 In addition, to reduce the risk of vitreous hemorrhage in the early period, to prevent the development of proliferative vitreoretinopathy, and to inhibit the risk of retinal detachment, we implanted silicone oil endotamponade to all eyes. Although the time of removal of the silicone oil could vary according to the indication for implantation, it is recommended to do it as soon as possible, as silicone oil may have a toxic effect on the retina.33–36 In our study, we removed the silicone oil endotamponade from all eyes 3 months later. There have been reported rare cases of IVD-related acute retinal necrosis, 37 epiretinal proliferation around the IVD, 38 and implant trapped at the macula 39 in vitrectomized eyes with silicone oil. In our study, we did not face any such complications.
Many studies showing the effectiveness of IVD in the treatment of DME in vitrectomized eyes have been published recently,40–43 but the management of DME in vitrectomized eyes that had silicone endotamponade implanted is still a dilemma. According to our detailed literature search, there are a few studies in the literature that investigated the effectiveness of IVD implant in eyes with silicone oil endotamponade. Banerjee et al. investigated the results of IVD application in eyes with retinal detachment and established PVR during vitrectomy and during silicone oil removal in their single-center, randomized, prospective clinical study on 140 patients. As a result of their research, they reported that the anatomical success and PVR recurrence of the study group were similar compared to the control group receiving standard care, but that cystoid macular edema was statistically significantly lower. 44 Iglicki et al. investigated the effect of IVD application during vitrectomy in eyes with diabetic tractional retinal detachment in their multicenter, comparative, and retrospective study on 148 eyes. As a result of their study, they reported that the reattachment rate was lower and the PVR severity was higher in the eyes that had IVD compared to the control group. 45 Cho and Yoon investigated the effects of coimplantation of silicone oil and IVD during vitrectomy in 7 eyes with atopic dermatitis and retinal detachment in their case series and reported that this could be a tolerable application and beneficial to PVR management. 46 In our study, there was no statistically significant difference in the rate of PVR development between the IVD and non-IVD groups.
Siqueira et al. investigated the potential neuroprotective effects of triamcinolone acetonide and IVD after vitrectomy and silicone oil injection in their experimental studies on rabbits and reported that retinal neuronal survival was increased in the steroid-treated groups compared to the control group. 47 The possible neuroprotective effect of steroids in vitrectomized eyes with silicone oil may also be effective on DME with PDR. The results of our study support that IVD reduces the risk of DME in the eyes with silicone oil endotamponade in the first 3 months and indicate that this application may positively affect the DME prognosis after silicone oil removal. The approach of the BCVA level of Group 1 to Group 2 after the silicone oil has been removed may be due to the anti-VEGF injections. In vitrectomized eyes, although the entire segment of the posterior segment is aimed to be filled with silicone oil for endotamponade, this goal is often not fully achieved due to hypotonia or residual fluid in posterior segment. This is the most common reason why heavy silicone oil or perfluorocarbon is preferred for endotamponading in inferior retinal detachments.48,49
The purpose of placing IVD in the inferior region in our study group was to ensure that dexamethasone dissolves in the liquid medium that will accumulate in the inferior region while the patient is standing. We anticipate that dexamethasone dissolved in the residual fluid in the posterior segment may have passed to the macula when the patients were lying on back and provided effectiveness in DME treatment. After removing the silicone oil, we observed that the IVD implant was dissolved faster in all cases. This observation may be due to the shorter half-life of IVD in eyes with silicone oil endotamponade; however, experimental and controlled studies are needed to reveal this hypothesis.
This study has some limitations. Small sample size and short follow-up time can be meaningful. Long-term randomized clinical trials with comprehensive outcomes are needed to evaluate the safety and effectiveness of coadministration of dexamethasone implant and silicone oil endotamponade in the treatment of PDR with tractional DME.
Conclusion
In patients with PDR, coadministration of IVD implant and silicone oil endotamponade during vitrectomy might be an effective and safe application in the treatment of DME and reduce the need of anti-VEGF drugs postoperatively.
Data Availability
The data produced and analyzed during the current study are not publicly available due to the prohibition of hospital's archive system, but could be obtained from the corresponding author upon plausible and acceptable request.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The author has no financial or nonfinancial relationships, ownership, or commercial interests with any of the materials mentioned in this article.