
Abstract
Purpose:
Diquafosol ophthalmic solution (DQS) stimulates P2Y2 receptors on the ocular surface, which enhances mucin secretion from goblet cells. Therefore, tear film stability and hydration of the ocular surface can be achieved independent from lacrimal gland function.
Methods:
This prospective, open-label pilot study included 60 eyes of 30 diabetic patients diagnosed with dry eye disease (DED) and were randomly assigned to either DQS (n = 30 eyes) or hyaluronate (HA) group (n = 30 eyes). Participants in the DQS group received 3% diquafosol ophthalmic solution, whereas HA group received 0.1% sodium HA preservative-free artificial tears. The dosage for both drugs was 1 drop, 6 times per day for 4 weeks. Tear film lipid layer (TFLL), noninvasive breakup time (NITBUT), corneoconjunctival staining (CS) score, meibomian gland (MG), conjunctival hyperemia [redness score (RS)], ocular surface disease index (OSDI) was assessed and compared at baseline, day 14, and day 28.
Results:
Comparing baseline and day 28 measurements revealed that both groups found significant improvements in NITBUT, CS, MG quality, MG expressibility, and OSDI scores significantly (P < 0.05), in addition TFLL improvements were only found in the DQS group. At day 28, the magnitude of change in mean NITBUT was 1.74 (DQS) versus 0.31 (HA), 1.16 (DQS) versus 0.37 (HA) point grade reduction in corneoconjunctival staining score and 9.80 (DQS) versus 4.80 (HA) point grade in mean OSDI score.
Conclusion:
Three percent diquafosol ophthalmic solution treatment demonstrated the ability to improve the tear film dry eye parameters and clinically reduced sign and symptoms of DED in diabetic dry eye patients. Clinical Trials.gov ID: NCT04980144.
Introduction
Type 2 diabetes mellitus (T2DM) is a prevalent chronic metabolic illness that causes relative insulin insufficiency in target organs owing to pancreatic β cell dysfunction and insulin resistance. 1 Shift to sedentary lifestyle, aging population, and obesity has significantly contributed to the global rise in the prevalence of T2DM. 2 In 2019 the prevalence of diabetes was documented to be 9.3% (463 million people) and in 2030 it is estimated to rise to 10.2% (578 million) and T2DM accounts for ∼90% of all diabetic occurrence. 3
Negative alterations to the tear film, corneal epithelium, corneal endothelium, and corneal nerves have been observed in 47%–64% of patients with diabetes.4,5 Ocular surface manifestation of signs and symptoms secondary to T2DM has been termed as diabetic keratopathy (DK). DK has been documented to increase central corneal thickness, 6 decrease in endothelial cell density, 7 leads of superficial punctate keratitis, 8 delay and impede wound repair, 9 and decrease in corneal sensitivity due to neuropathy. 10
Additionally, T2DM patients have also been noted to have compromised tear quantity and quality11,12 due to conjunctival goblet cell loss as documented on cytologic analysis. 11 Goblet cells secrete mucin, which stabilizes the tear film, minimizes tear evaporation, and reduces mechanical friction. Goblet cell loss in animal models suggests that it disrupts the ocular surface's immune tolerance 13 and increased expression of inflammatory cytokines in the conjunctiva. 14
Around 0.1% hyaluronate (HA) used in artificial tears have been reported to promote corneal re-epithelium and improve corneal healing. 15 Additionally, HA has been reported to decrease the rate of tear evaporation and enhance the stability of tear film. 16 Diquafosol tetrasodium is a dinucleotide polyphosphate, which is a purinoceptor agonist, and when administered to the ocular surface, it binds to P2Y2 receptors and stimulates mucin and tear secretion.17–19 The corneal epithelium, conjunctival epithelium, lacrimal gland ductal epithelium, meibomian gland sebaceous cells, and meibomian gland ductal cells all express the P2Y2 receptor.20,21
Subsequently, enhanced secretion of mucin and tear secretion due to diquafosol tetrasodium ophthalmic solution stabilizes the tear film, minimizes tear evaporation, and reduces mechanical friction, thereby protecting the corneal epithelium. 22 Various reports have concluded that 3% DQS is effective in the treatment of dry eye disease (DED)23–25 and Dota et al.'s 18 findings suggest that DQS improves corneal epithelial damage in T2DM rat model. However, the effect of DQS on the tear film of T2DM human participants has not been previously assessed. Therefore, the purpose of this study is to assess subjective and objective diabetic dry eye findings after using 3% DQS or 0.1% HA topical eye drops.
Methods
Study design and participants
This study (https://clinicaltrials.gov/ct2/show/record/NCT04980144) was conducted in compliance with the tenets of the Declaration of Helsinki and the Institutional Review Board of the He Eye Specialist Hospital, Shenyang, China (approval number: IRB-2019.K002.01), approved on January 23, 2019. Consecutive volunteers were recruited from Shenyang's He Eye Specialist Hospital, and informed consent was acquired from all participants after a thorough description of the study's purpose and its implications. All data pertaining to participants in this study were anonymized.
Participants were randomly allocated to the DQS, or HA group, and clinical assessments were performed on days 0, 14, and 28 by a masked examiner who was not involved in the data collection or group allocation procedure for this research. Randomization was accomplished through the use of a computer-generated random number generator to enroll each participant consecutively.
DED diagnostic criteria: Diagnostic was based on the Japanese criteria, as suggested by Uchino et al. 26 : (1) the presence of dry eye symptomatology using Chinese version of the Ocular Surface Disease Index (C-OSDI) (Allergan, Inc., CA); (2) the presence of tear film disturbance; (3) the presence of conjunctivocorneal epithelial damage. The presence of all 3 criteria were needed to establish a positive DED diagnosis.
Inclusion criteria comprised the following: (1) age ≥18 years, (2) clinically diagnosed and confirmed with T2DM for 1 year or more, (3) able and willing to comply with the treatment/follow-up schedule, or (4) bilateral signs and symptoms of DED, as mentioned above.
Exclusion criteria: Participants with heart disease, stroke, hormonal disorder, or systemic immune-mediated illnesses, such as secondary Sjögren's syndrome or graft-versus-host disease, were excluded. Patients using topical medication(s) for the treatment of ocular disorders, such as glaucoma or allergic conjunctivitis were excluded from the study. Participants who had previous ocular surgery or trauma, 1-month history of blepharal and periorbital skin disease or allergies, severe dry eyes with corneal epithelial defect, limbic keratitis, pterygium, corneal neovascularization, glaucoma, breastfeeding, rheumatic immune systemic diseases, herpes zoster infection, pregnant women, individuals allergic to fluorescein, and contact lens wearers were excluded from the research.
Clinical evaluation
Noninvasive initial tear film breaking time was assessed using the Keratograph 5M (Oculus, Germany) topographer. Three sequential readings were captured, and the median value was included in the final analysis. The median value was recorded.
Following the methods of Arita et al., 27 conjunctivocorneal epithelial staining assesses corneal and conjunctival epithelium damage. Double vital staining approach with 2 μL of a preservative-free solution containing 1% lissamine green and 1% sodium fluorescein was instilled in the conjunctival sac. The eye was sectioned into 3 equal pieces (temporal conjunctiva, cornea, and nasal conjunctiva). Each region received a maximum staining score of 3 points and a minimum of 0 points. The combined scores from all 3 parts were then recorded on a scale ranging from 0 (normal) to 9 (severe). 28
Tear film lipid layer (TFLL) interferometry was assessed using DR-1 (Kowa, Nagoya, Japan). TFLL quality was classified according to Yokoi et al.'s 29 grading system and lower score suggests better TFLL quality (grade 1: somewhat gray color, uniform distribution; grade 2: somewhat gray color, nonuniform distribution; grade 3: a few colors, nonuniform distribution; and grade 4: many colors, nonuniform distribution).
The following criteria were used to determine the quality of meibum and the expressibility of the meibomian gland: (1) Meibum quality: 5 meibomian gland in the middle parts of the eyelid were assessed using a scale of 0 to 3 for each gland (0 represented clear meibum; 1 represented cloudy meibum; 2 represented cloudy and granular meibum; and 3 represented thick, toothpaste like consistency meibum). (2) Meibum expressibility: Eight meibomian glands in the middle part were evaluated on a scale of 0 to 3 (0 denoted that all glands were expressible; 1 denoted that 3 to 4 glands were expressible; 2 denoted that 1 to 2 glands were expressible; and 3 denoted that no glands were expressible). The overall score was computed using the mean scores of these 8 glands.
Chinese-translated, and validated OSDI (Allergan, Inc., Irvine) version was used to assess and quantify dry eye symptom. The 12 items of the questionnaire can be tabulated into a score that ranges from 0 (no symptoms) to 100 (severe symptoms) points. 30
Conjunctival hyperemia [redness score (RS)] was assessed by keratograph image (Oculus) of 1156 × 873 pixels, and RS (accurate to 0.1 U) was displayed on the computer screen that ranged from 0.0 to 4.0. 31
Safety evaluation: During all test visits, best corrected visual acuity (BCVA), intraocular pressure (IOP), endothelial cell count (ECC), and corneal and conjunctival examinations with slit lamp microscope were performed. Ocular surface and periorbital abnormities were assessed.
Treatment
Participants in DQS group used 1 drop of 3% DQS (Diquas; Santen Pharmaceutical Co., Ltd., Osaka, Japan) 6 times per day for 4 weeks (28 days), whereas participants in HA group used 1 drop of 0.1% Sodium HA artificial tears (preservative free) 6 times per day for 4 weeks (28 days). In all groups, all additional medicines, or treatments for DED were stopped throughout the research period.
Statistical analysis
Data are presented as mean ± standard deviation and all analysis was performed using SPSS version 24 (SPSS, Inc., Chicago, IL). Data were found to be non-normally distributed with the Shapiro–Wilk test (P < 0.05), and nonparametric testing was therefore applied. A linear mixed model with Bonferroni post hoc analysis was used to evaluate repeated measurements of continuous variables, including noninvasive breakup time (NITBUT), OSDI score, BCVA, ECC, and IOP. Generalized linear mixed-model analysis with Bonferroni post hoc analysis was used for repeated measurements of discrete variables, including the TFLL, corneoconjunctival staining (CS) score, RS, and MG assessments.
The level of statistical significance was set at P < 0.05. The power (1 − β) was 0.90 at the level of α = 0.05, and the sample 30 eyes in each group was sufficient. 32
Results
Patient characteristics
The duration of T2DM and medications were noted. The mean ± SD age of DQS group was 49.87 ± 9.08 years (range, 35–67 years) and consisting of 15 participants (7 females, 8 males). While the mean ± SD age of the HA group was 49.93 ± 9.18 years (range, 36–67 years) and comprised 15 participants (7 females, 8 males). Participants in both groups had symptoms and signs of DED after being diagnosed with T2DM. The demographic characteristics of participants in the study are presented in Table 1. The final analysis consisted of 30 Asian adult participants (60 eyes) (Fig. 1). Baseline clinical DED parameters did not differ between the DQS group and HA group (all P > 0.05; Table 1). As shown in Table 2, there were no significant differences between the 2 groups in terms of dry eye-related parameters at baseline (P > 0.05).
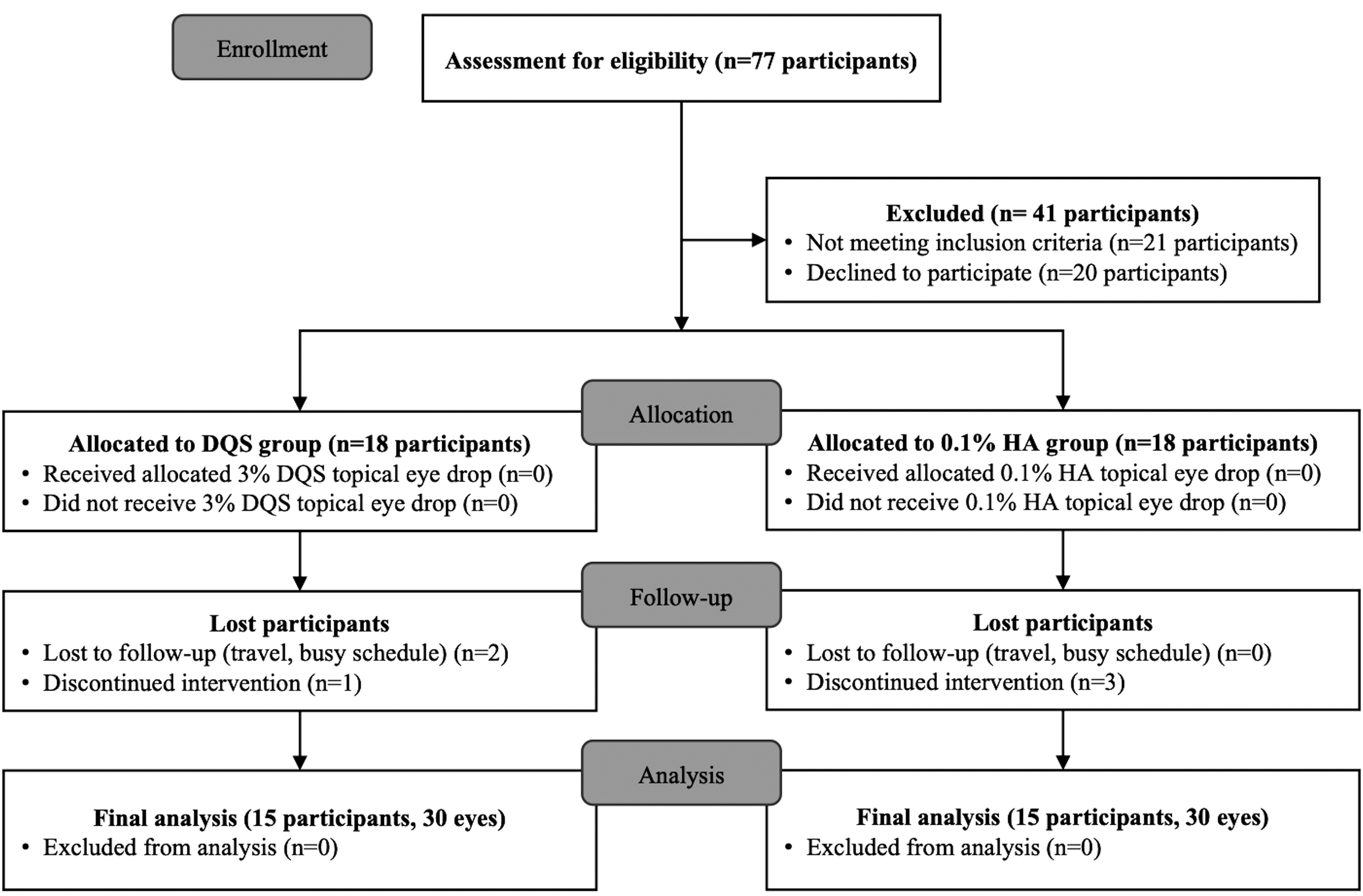
Consolidated standards of reporting trials (CONSORT) 2010 flow diagram.
Demographic Characteristics of Participants in the Study
Year/s since diabetes grading: 1: <5 years, 2: 5–10 years; 3: >10–20 years, 4: >20 years; Hemoglobin A1c % grading: 1: <7%, 2:7 to <9%, 3: >9%; P values were determined with Mann–Whitney U test, Fisher's exact test or ANOVA.
DED, dry eye disease; DQS, diquafosol ophthalmic solution; OSDI, ocular surface disease index; HA, hyaluronate; SD, standard deviation.
Characteristics of Participants in Diquafosol Ophthalmic Solution Group and Hyaluronate Group at Baseline and After Treatment
P values were determined with Mann–Whitney U test, Fisher's exact or ANOVA. *Statistically significant at P < 0.05.
CS, corneoconjunctival staining score; MG, meibomian gland; NITBUT, noninvasive tear breakup time; RS, redness score; TFLL, tear film lipid layer.
Efficacy of treatment
Interferometric pattern (lipid layer grade) was used to grade TFLL quality from a scale of 1 to 5. There were no significant differences between the groups at baseline scores (P > 0.05) between DQS (2.73 ± 0.74) and HA group (2.80 ± 0.71). While comparing TFLL grade at day 28 between DQS group and HA group, DQS group showed significant improvement (P < 0.001). Additionally, when baseline and day 28 grades were compared within each group, only DQS showed significant improvements (P < 0.05).
NITBUT was significantly prolonged in the DQS group (4.04 ± 0.67, 4.58 ± 0.65, 5.78 ± 0.79 s) in comparison to HA group (4.00 ± 0.54, 4.09 ± 0.58, 4.31 ± 0.50 s) at all assessment time points, excluding baseline measurements. At day 28 within-group comparison revealed significant improvements (DQS: P < 0.001, HA: P = 0.028) in the mean NITBUT measurements in both groups (Table 2 and Fig. 2).
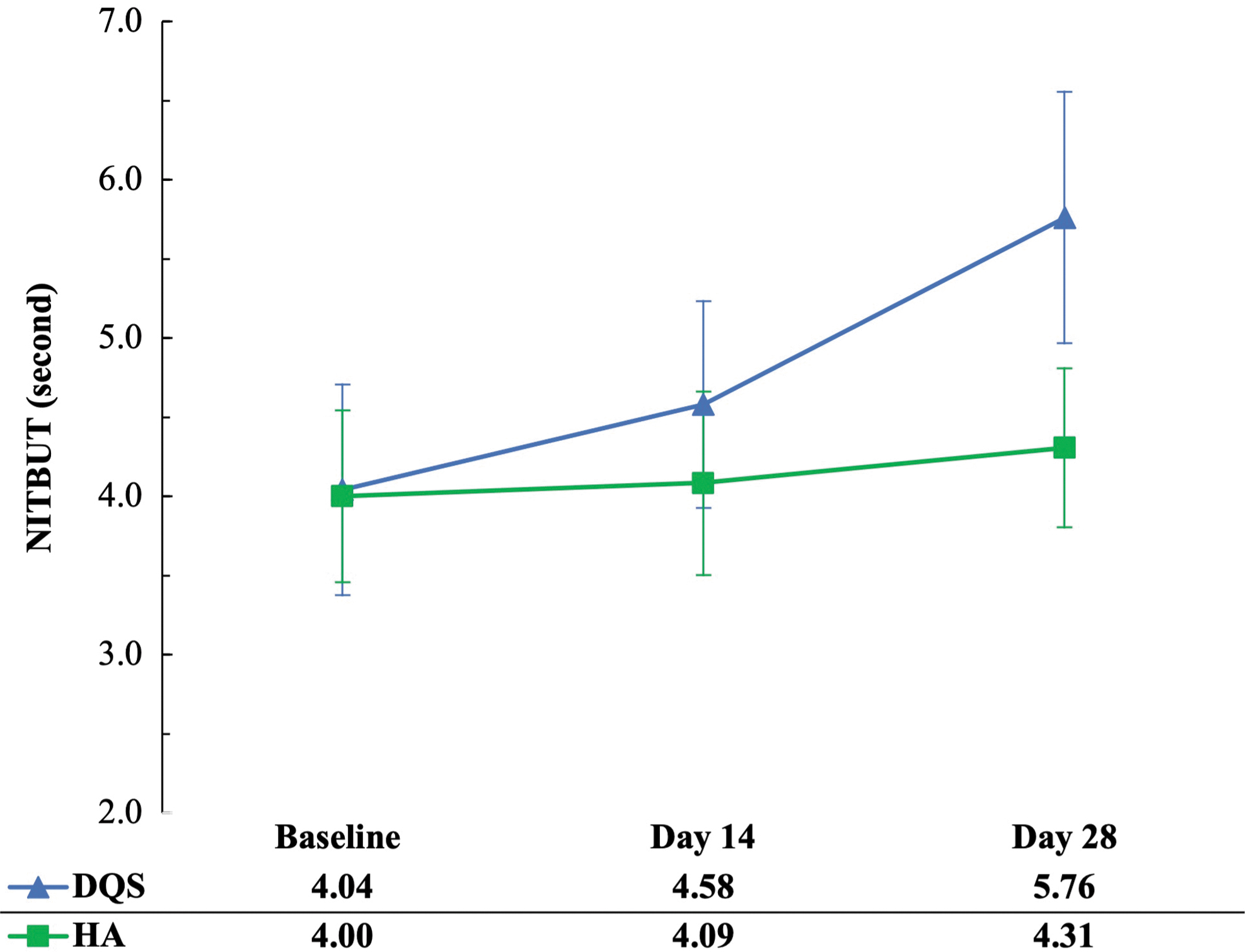
Comparison of mean NITBUT of participants in DQS and HA groups. DQS, diquafosol ophthalmic solution; HA, hyaluronate; NITBUT, noninvasive breakup time.
CS score revealed that DQS and HA groups had significant improvements in their scores at day 28 when compared with their respective baseline scores (DQS: P < 0.001, HA: P = 0.016). However, while comparing mean CS scores between DQS group (day 14: 3.97 ± 0.49, day 28: 3.27 ± 0.45) and HA group (day 14: 4.27 ± 0.58, day 28: 4.00 ± 0.53), DQS group showed significantly higher improvement (day 14: P = 0.035, day 28: P < 0.001) at both time points (Table 2 and Fig. 3).
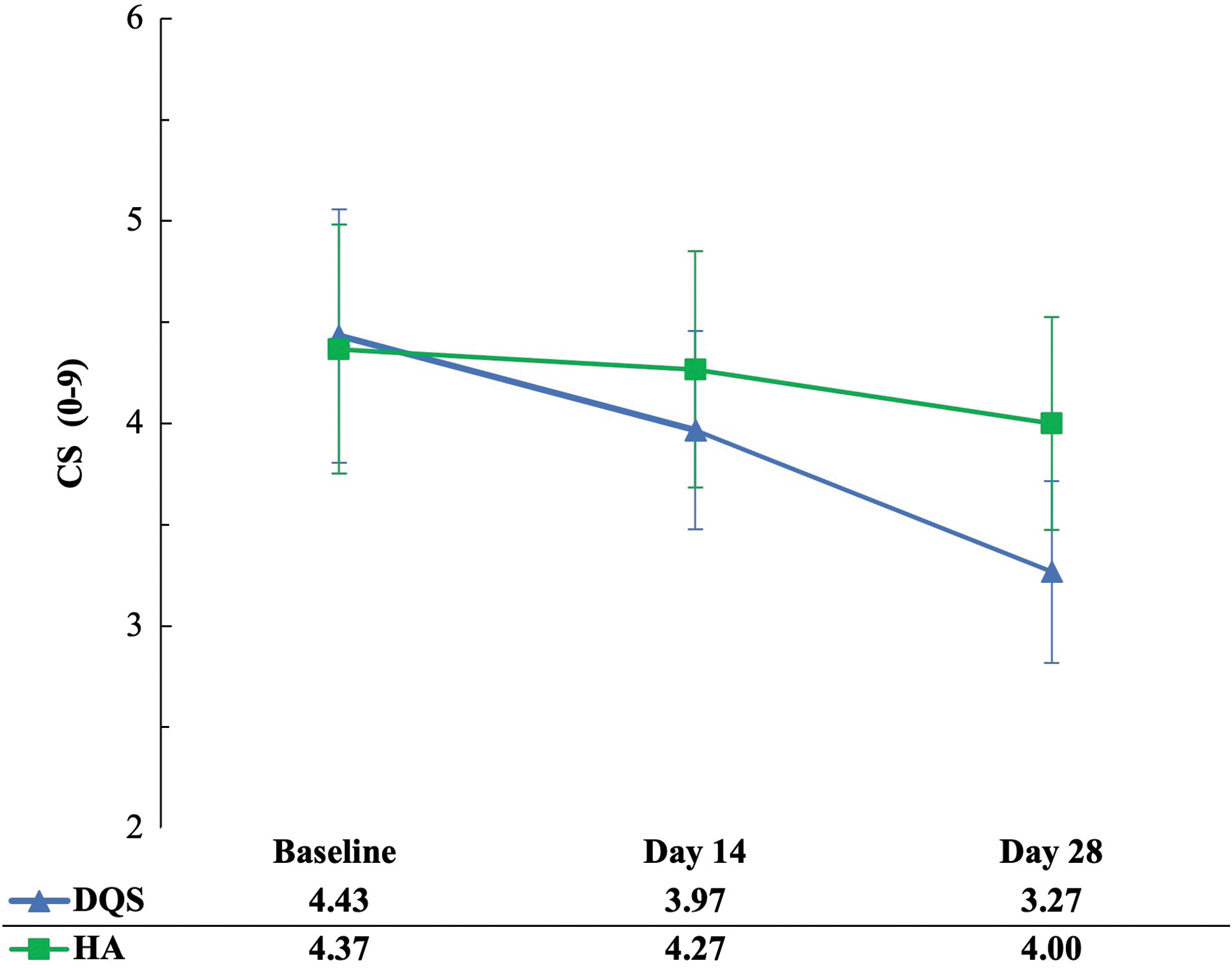
Comparison of mean CS of participants in DQS and HA groups.
Meibomian gland quality when compared with their respective mean baseline measurements significantly improved (DQS: P < 0.001, HA: P < 0.024) in both groups at day 28. However, between-group comparison revealed no significant differences (P = 0.062). Between-group meibomian gland expressibility score comparison revealed no significant differences (P = 0.062), whereas within-group comparison found significant improvement at day 14 and day 28 in DQS group (day 14: 1.77 ± 0.73, P = 0.003, day 28: 1.70 ± 0.65, P = 0.003) and HA group (day 14: 1.80 ± 0.81, P = 0.161, day 28: 1.80 ± 0.66, P = 0.024).
Conjunctival hyperemia redness score at baseline, day 14 and day 28was 1.18 ± 0.31, 1.07 ± 0.30, and 1.01 ± 0.36, respectively, for the DQS group and 1.17 ± 0.39, 1.13 ± 0.35, and 1.09 ± 0.34, respectively, for HA group. Inter-group and within-group comparison revealed no significant changes (P > 0.05).
The total mean OSDI score at day 14 for DQS group and HA group was 32.80 ± 9.34 and 36.93 ± 9.17, respectively, and was not significantly different (DQS: P = 0.089). At day 28, total mean OSDI scores in DQS group (32.80 ± 9.34 vs. 27.80 ± 7.31, P = 0.015) was significantly better in comparison to HA group (Table 3 and Fig. 4). Additionally, significant changes were recorded in both groups while comparing their day 28 scores with respective baseline scores (DQS: P < 0.001, HA: P = 0.021).
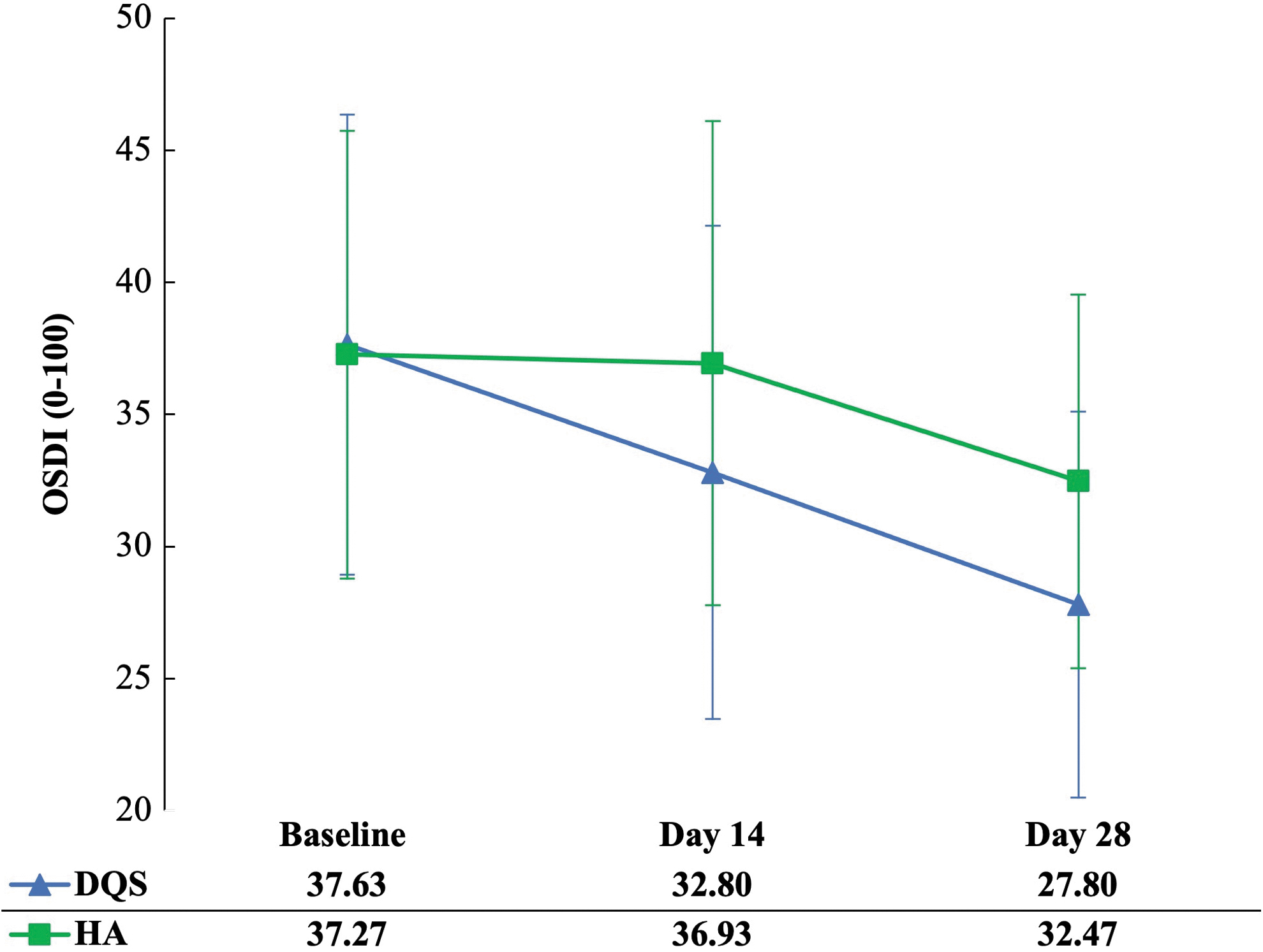
Comparison of mean OSDI scores of participants in DQS and HA groups. OSDI, ocular surface disease index.
Safety Assessments
BCVA, best corrected visual acuity; ECC, endothelium cell count; IOP, intraocular pressure.
Safety data
During the research, no systemic adverse event or adverse clinical signs and symptoms was detected in either group. BCVA remained stable throughout all visits. No significant change was seen in either group at day 14, or day 28 in comparison to baseline measurements for BCVA, IOP, and ECC in both groups (Table 3).
Discussion
This randomized controlled, assessor-blinded pilot study compared the effectiveness and safety of 3% diquafosol ophthalmic solution (DQS group, n = 30 eyes) and 0.1% sodium HA ophthalmic solution (HA group, n = 30 eyes), which demonstrated that 3% DQS was comparable or more effective in ameliorating the signs and symptoms of dry eye in patients with T2DM.
DQS groups were found to have significant improvements at day 28 in all DED parameters assessed in this study, except for RS (RS: 1.18 ± 0.31 vs. 1.01 ± 0.36, P > 0.05) when compared with baseline measurements. While comparing baseline and day-28 measurements, HA group had significant improvements in NITBUT, CS score, MG quality, MG expression, and OSDI score, but parameters, such as TFLL (2.80 ± 0.71 vs. 2.43 ± 0.72, P = 0.054) and RS (1.17 ± 0.39 vs. 1.09 ± 0.34, P = 0.431), were recorded to have no significant change.
Dry eye symptoms assessed using OSDI in both groups were on the severe region (normal: 0–12, mild: 13–22, moderate: 23–32, and severe: 33–100) at baseline (DQS: 37.60 ± 8.71 and HA: 37.27 ± 8.48), at day 28 both groups recorded significant reduction in their mean symptom scores (DQS: 27.80 ± 7.31 and HA: 32.47 ± 7.07) and the mean symptom score moved to moderate region for the DQS group, whereas HA group hovered between moderate to severe region on the OSDI severity scale.
DED is a common ocular surface condition defined as a multifactorial disease of the ocular surface, in which tear film instability, hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities are involved.33,34
Sodium HA is a glycosaminoglycan disaccharide that consists of repeating alternate sequences of N-acetyl-glucosamine and glucuronate. HA is used topically to increase the amount of water and mucin on the ocular surface. Ocular surface, tear film stability, and dry eye symptoms have been found to benefit by using varying doses and concentrations of HA eye drops.35,36 It has been reported that topical HA eye drop formulations improve signs and symptoms of DED and relieves inflammation. Additionally, various studies have reported that diquafosol increases the amount and quality of tear film.16,37–39 Diquafosol has also been found to promote cell survival and modulate reactive oxygen species-induced apoptosis and inflammation of epithelial cells in dry eye cornea. 40
Therefore, DQS group from similar other DED studies was found to have higher magnitude of change (Δ2) at day 28 in comparison to HA group, suggesting that 3% diquafosol was better at stabilizing the tear film, significantly and clinically improved NITBUT and OSDI scores in comparison to HA group. The magnitude of improvement in DED signs and symptoms was more noticeable in the DQS group. The 1.74 (DQS) versus 0.31 (HA) point grade improvement in mean NITBUT measurement, 9.80 (DQS) versus 4.80 (HA) point grade in mean OSDI score, and 1.16 (DQS) versus 0.37 (HA) point grade reduction in corneoconjunctival staining score after 28 days is double the improvement (Table 2).
However, histopathology and pathophysiology assessments such as tear film osmolarity, impression cytology, and inflammatory markers of the ocular surface were not assessed in this study. Considering the consensus that TBUT is considered a surrogate, convenient assessment is performed by clinicians to assess tear film stability. 41 Improvements in NITBUT in both groups imply improved integrity of the tear film, which tends to lower evaporation, hyperosmolarity, and progression of DED.
The study's limitations include the trial's limited sample size and data collection at a single location. The fact that statistical significance was reached in both signs and symptoms with such a small sample demonstrates the effectiveness of the mechanism of action and the magnitude of therapeutic relief. Thus, the pilot study's early results are promising. However, further research is necessary to validate the impact of 3% diquafosol ophthalmic solution on diabetic dry eye participants. Another limitation of the study was that critical test such as corneal sensitivity and high-definition corneal confocal microscopy assessments were not performed. Studies have previously reported that corneal nerve degeneration due to T2DM is one of the primary causes of ocular surface health degeneration.42,43
Since the purpose of this pilot study was to only assess the tear film changes and symptoms of DED, future studies will therefore be designed to assess corneal sensitivity and corneal confocal microscopy changes.
Conclusion
Three percent diquafosol ophthalmic solution and 0.1% hyaluronic acid artificial tears in type 2 diabetic dry eye patients was found to be safe, and well tolerated. Overall, 3% diquafosol ophthalmic solution was found to be better than 0.1% sodium HA, in improving both signs and symptoms of severe DED in type 2 diabetic subjects. Statistically significant treatment effects and numerous trends toward improvement suggest further studies should be aimed at elucidating the therapeutic effect of 3% diquafosol ophthalmic solution in a larger diabetic dry eye patient cohort.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.