
Abstract
Purpose:
Difluprednate ophthalmic emulsion (Durezol®) is currently used for the treatment of anterior uveitis; however, recent studies have shown that difluprednate can treat posterior eye conditions. Topical formulations limit the amount of drug capable of permeating to the posterior segment due to permeation barriers, lacrimation, and lymphatic clearance.
Methods:
Resomer®-based microneedle patches were fabricated for difluprednate using poly(acrylic acid) (PAA) for the rapidly dissolvable backing. The patches were analyzed for microneedle uniformity and sharpness using scanning electron microscopy, and the penetration depth was analyzed by confocal microscopy. Failure force necessary to break the microneedles and force needed to penetrate the sclera were analyzed by the texture analyzer. Difluprednate release and trans-scleral permeation studies on microneedles were performed using Franz diffusion cells.
Results:
The microneedles were uniform, sharp, and penetrated to 500 μm depth on sclera. The microneedles have a failure force proportional to the molecular weight (MW) of the polymer used. There was no correlation between failure force and the penetration force of the microneedles. The PAA backing dissolved within 30–40 min, while release studies showed a matrix diffusion-controlled release over the 7-day study. The amount of drug permeation and retention in the sclera were decreased with an increase in the MW of the Resomer and failure force of each array.
Conclusions:
Resomer-based microneedles have a potential application for the sustained release of difluprednate for posterior segment conditions.
Introduction
Ophthalmic solutions, suspensions, or emulsions often require multiple applications each day, 1 which is not convenient for the patient, especially for treating chronic diseases. 1 Additionally, topical formulations are generally meant for the delivery of drugs to the anterior segment of the eye (iris, ciliary body, cornea, lens) and cannot deliver therapeutic concentrations to the posterior segment of the eye (choroid, vitreous body, retina). 2 Intravitreal injections are a common treatment for posterior segment conditions. However, injections are not patient friendly as they can result in pain, cataracts, trauma, and endophthalmitis. 3 Thus, there is a need for noninvasive methods of drug delivery to the posterior segment of the eye that includes the benefits of both topical delivery and intravitreal injections. 2
Difluprednate topical emulsion (Durezol®) is used in the treatment of pain and inflammation in the anterior segment of the eye. 4 However, research has shown that Durezol had beneficial long-term effects on posterior segment conditions, such as retinal vasculitis, 5 Harada disease ocular manifestations,6,7 pars planitis, 8 and macular edema.9,10 Ocular distribution studies in rabbits revealed penetration to the choroid/retina using Durezol. 11 Furthermore, difluprednate is shown to have a large potency due to the high affinity between the glucocorticosteroid and the difluprednate active metabolite 12 ; only Durezol is available to date 13 ; therefore, it is desirable to formulate a minimally invasive sustained-release drug delivery system for the posterior eye.
Biodegradable polymeric microneedles offer a noninvasive patient-friendly alternative to intravitreal injections while providing easy administration for the patient as they do not cause pain like traditional hypodermic needles. The microneedles can last for a specified duration, leading to a decrease in repeat administration and improved residence time. The microneedles can be made long enough to penetrate the sclera, which poses as an ocular barrier for drug delivery to the posterior segment. 14
Different microneedle types have been attempted for ocular delivery, such as solid coated microneedles,15,16 and hollow microneedles.17–19 The solid or hollow silicon microneedles are difficult to fabricate as they are brittle and pose the risk of breaking off into the ocular tissue. 20 Additionally, silicon and glass-based microneedles are complex, expensive to manufacture, and complicated for patients to administer themselves.
A study reported on rapidly dissolving ocular microneedles using polyvinylpyrrolidone (PVP) polymer, 20 which is desirable for rapid drug release. Likewise, a study discusses using sustained-release biodegradable PLA microneedles as a means for sustained delivery of methotrexate. 21 These biodegradable microneedle arrays are less complex for patient use and lasted for 8 weeks. Recently, self-adhesive microneedles with interlocking features for sustained ocular delivery of drugs have been reported. 22
PLGA or poly(lactic-co-glycolic acid) is an FDA-approved copolymer used in a plethora of biological applications such as nanoparticles and controlled drug delivery devices.23,24 The degradation time of PLGA is based on the ratio of lactide to glycolide. As the lactide concentration increases, the water solubility of the polymer decreases, leading to an increase in degradation time. 25
The mechanical strength of PLGA is dependent on the crystallinity of the polymers, which is directly related to the molecular weight (MW). Furthermore, increased MW generally results in a slower degradation time. Therefore, biodegradable polymeric microneedles can be modified to degrade at a specific time by varying the MW and concentration of lactide. While many studies have been conducted using biodegradable microneedles for transdermal applications,26–28 only a few studies have been performed using sustained-release ocular biodegradable microneedles.21,29 PLGA is safe for ocular use, as this polymer has been approved for its use in intravitreal implants (Ozurdex®).
The objective of this work was to develop biodegradable microneedles for the sustained-released delivery of difluprednate to the suprachoroidal space (SCS) for the treatment of posterior uveitis. Targeting the SCS allows for enhanced delivery to the retina and choroid with higher bioavailability compared with topical formulations and intravitreal injections.30,31 Polymers with varying MWs and lactide concentrations were tested to compare the mechanical strength and release profiles of each microneedle formulation. Furthermore, the microneedle patch contains a poly(acrylic acid) (PAA) backing that will undergo rapid dissolution upon instillation into the eye, leaving a thin malleable PLGA sheet with the microneedle imbedded in the sclera. 26
Methods
Materials
Difluprednate was procured from Chemieliva Pharmaceutical Co., Ltd. (Chongqing China). PAA 35% (w/w) solution in water, Resomer® R 202 S, Poly(
Fabrication of PLGA biodegradable microneedles
To formulate microneedles, 5 mg of difluprednate was dissolved in acetonitrile, and 50 mg of the desired polymer was added to the aforementioned solution and sonicated for 30 min. Three different mixtures were prepared to test the variation in drug release and strength of the microneedle patches. Fifty microliters was pipetted into each microneedle mold and centrifuged for 30 min at 3,300 rpm using a Beckman Coulter Allegra™ 6R (Indianapolis, IN) benchtop cell culture centrifuge. Following centrifugation, ∼80 mg of 35% PAA solution was placed into the microneedle molds using a dropper to serve as the dissolving backing. The microneedle arrays were then left on the benchtop overnight to dry. The dried microneedle patches were collected from the molds and stored in polythene bags.
HPLC analysis
An Alliance Waters e2695 Separations Module and a Waters 2998 Photodiode Array Detector interfaced with Empower 3 software (Waters Corporation, Milford MA) were used for quantifying the difluprednate extracted from microneedles, release, and trans-scleral permeation studies. A Luna C18(2) 5 μm, 150 × 4.60 mm reversed-phase HPLC column was employed for difluprednate analysis. The mobile phase consisted of 60:40 acetonitrile:phosphate buffer (10 mM, pH = 6). Samples were eluted at a flow rate of 1 mL/min at ambient temperature—the absorbance wavelength set at 254 nm, with an injection volume of 10 μL.
Characterization of microneedle patches containing difluprednate
Scanning electron microscopy
The microneedles were analyzed to determine microneedle structure and uniformity using a Jeol 7000f Scanning Electron Microscope. Before analysis, each microneedle array was coated with a 20–22 nm gold coating.
Microneedle PAA backing dissolution study
The PAA backing dissolution test was performed by submerging the microneedle arrays in a 6-well plate in 5 mL of phosphate-buffered saline (PBS, pH = 7.4) maintained at 37°C in an incubator. The well plate remained in a water bath (37°C) for the duration of the study. The backing was visually inspected at 15, 30, and 40 min by removing the microneedle with a pair of tweezers and analyzing the backing thickness. The microneedles were removed once the backing was completely dissolved.
Microneedle failure force
The strength of the microneedle patches was determined by analyzing the failure force of each patch.28,32 Stress–strain curves were produced using a displacement force test station, TA-HDi Texture Analyzer (Texture Technologies Corp., Hamilton, MA). An individual microneedle array was pressed against a stainless steel surface at a rate of 1 mm/s until a preset distance was reached (1 mm). Failure force was indicated by a sudden drop in applied force.
Microneedle insertion force into sclera
The force required for the insertion of microneedles into the excised porcine sclera was determined using the TA-HDi Texture Analyzer. Scleral tissues were washed with PBS pH 7.4 and blotted dry and then placed underneath the Texture Analyzer probe with the epithelium side facing upward. Microneedles were gently placed on the tissue, and the probe is lowered with a test speed of 0.1 mm/s and a trigger force of 0.1 N. The microneedles were allowed to penetrate the sclera to a value of 0.5 mm, after which the microneedles were retracted with a speed of 1 mm/s. 20 The data were recorded as force required per microneedle array versus the depth of insertion.
Depth of penetration into sclera
To determine the penetration depth of microneedles into the sclera, fluorescein isothiocyanate (FITC)-loaded microneedles were prepared. A 1 mg/mL solution of FITC was prepared in acetonitrile and from this 250 μL of solution was utilized to prepare blank microneedles as mentioned earlier in the fabrication of microneedles.
Excised porcine scleras were washed with PBS pH 7.4 and blotted dry and then placed on a flat surface with epithelium side facing upward. The microneedles were manually inserted into the sclera by applying gentle thumb pressure for 1 min, and then the microneedles were left on the sclera for 1 h by placing the cellophane tape. After 1 h, the microneedles were gently removed and examined under Nikon A1+/MP confocal laser scanning microscope (Nikon Instruments, Melville, NY) with a 4 × objective, step size of 10 μm, and excitation laser lines at 488 and 520 nm. Z-stacked optical sections were collected up to 600 μm. Three-dimensional images were then processed by Nikon NIS-Elements AR software.
Microneedle array release study
For release studies, the individual arrays were glued to the bottom of each well in a 24-well plate and submerged in 2 mL of the dissolution media (PBS, pH 7.4: ethanol, 8:2, preheated to 37°C). The well plate was placed in the water bath incubator set at 37°C. The full volume (2 mL) of each well was removed at the following time points: 4, 8, 12, 24, 48, 72, 96, 120, and 168 h and replenished with the fresh dissolution medium. The release samples were analyzed for the drug content by HPLC. The drug release from each microneedle array was modeled using the Higuchi equation for matrix systems, which describes Fickian diffusion33,34:
In this expression, τ is time, r is the radius of the microneedle tip (10 μm), D is the diffusion coefficient, Mt is the cumulative drug released at a specific time, and M0 is the total drug loaded in the microneedle patch, which was determined to be ∼1 mg by dissolving microneedle patches in 100% acetonitrile. The diffusion coefficient is the only unknown and is calculated by fitting the experimental data to Equation (1).
Ex vivo scleral permeation experiments
Scleral excision
Fresh porcine eyeballs were obtained from Auburn University Lambert-Powell Meats Laboratory (Auburn University, Auburn, AL). The animals were sacrificed according to the Institutional Animal Care and Use Committee (IACUC)-approved protocol (SOP 2015-2727). The excess tissue was first cut from the globe, and the scleras were excised from the globe using a 3.0 mm slit Eagle blade to create an insertion point between the iris and the cornea. Corneal scissors were used to excise the sclera. The scleral tissues were rinsed with tap water and then placed in PBS, pH 7.4 until used in the permeation studies. The permeation studies began within 2 h of excision.
Scleral permeation studies
Franz diffusion cells were assembled between the donor and receptor halves of the diffusion cells to hold the sclera in position during the permeation experiments. All formulations were tested in 3 replicate permeation experiments. The receptor cell was filled with 5 mL PBS buffer (pH 7.4) containing 20% ethanol to maintain sink conditions. The solubility of difluprednate in the receptor medium was 30.5 μg/mL. The scleras were placed on the receptor cell with the outer surface of the sclera facing up, the microneedle patch was then pressed into the sclera using tweezers and the donor cell was placed on top of the sclera and both half cells were clamped together. In a separate experiment, the eye drop formulation (generic Durezol, 50 μL) was applied on the sclera after assembling the diffusion cells.
In the preliminary experiments, it was verified that all the microneedles of the patch penetrate the scleral tissue by the pressure applied. The 50 μL of simulated tear fluid (STF) was added. The receptor cell was sampled (1 mL) at 2, 4, 8, 12, and 24 h and replenished with a fresh receptor medium. Ethanol was added to ensure the sink condition of the experiment due to the poor solubility of difluprednate in the PBS. The scleral permeation samples were analyzed for the drug content by HPLC.
Extraction of difluprednate from scleras
At both the 12- and 24-h time points, microneedle patches or eye drop formulation (0.05% difluprednate ophthalmic emulsion) were removed from the scleras, and the scleras were subsequently removed and cleaned with PBS buffer (pH 7.4) containing 20% ethanol using cotton swabs. The active diffusion area of the sclera was cut, weighed, minced, and placed in individual vials with 2 mL of the HPLC mobile phase [10 mM phosphate buffer (pH = 6): Acetonitrile 40:60]. The vials were then sonicated for 30 min and left to sit for 24 h at 4°C to extract any drug that is retained in the sclera.
Following the 24-h extraction period, the vials were sonicated again for 30 min and then the supernatant was filtered through 0.45 μm Nylon membrane filter and assayed by HPLC. The microneedles were reserved for scanning electron microscopy (SEM) analysis at both 12- and 24-h time points.
Statistical analysis
All results are presented as mean ± standard error of mean. The calibration curve for difluprednate was tested up to a concentration of 400 μg/mL. (slope: y = 18,005x; R = 0.9998). The cumulative amount of drug permeated through unit area of sclera was plotted as a function of time. In vitro steady-state flux was calculated from the slope of the permeation plot. The amount of drug (mg) retained in the sclera was normalized to 1 g of sclera. Analysis of variance was performed to determine the level of significance between the means. Mean differences with P < 0.05 were considered significant.
Results
Fabrication and characterization of biodegradable microneedles
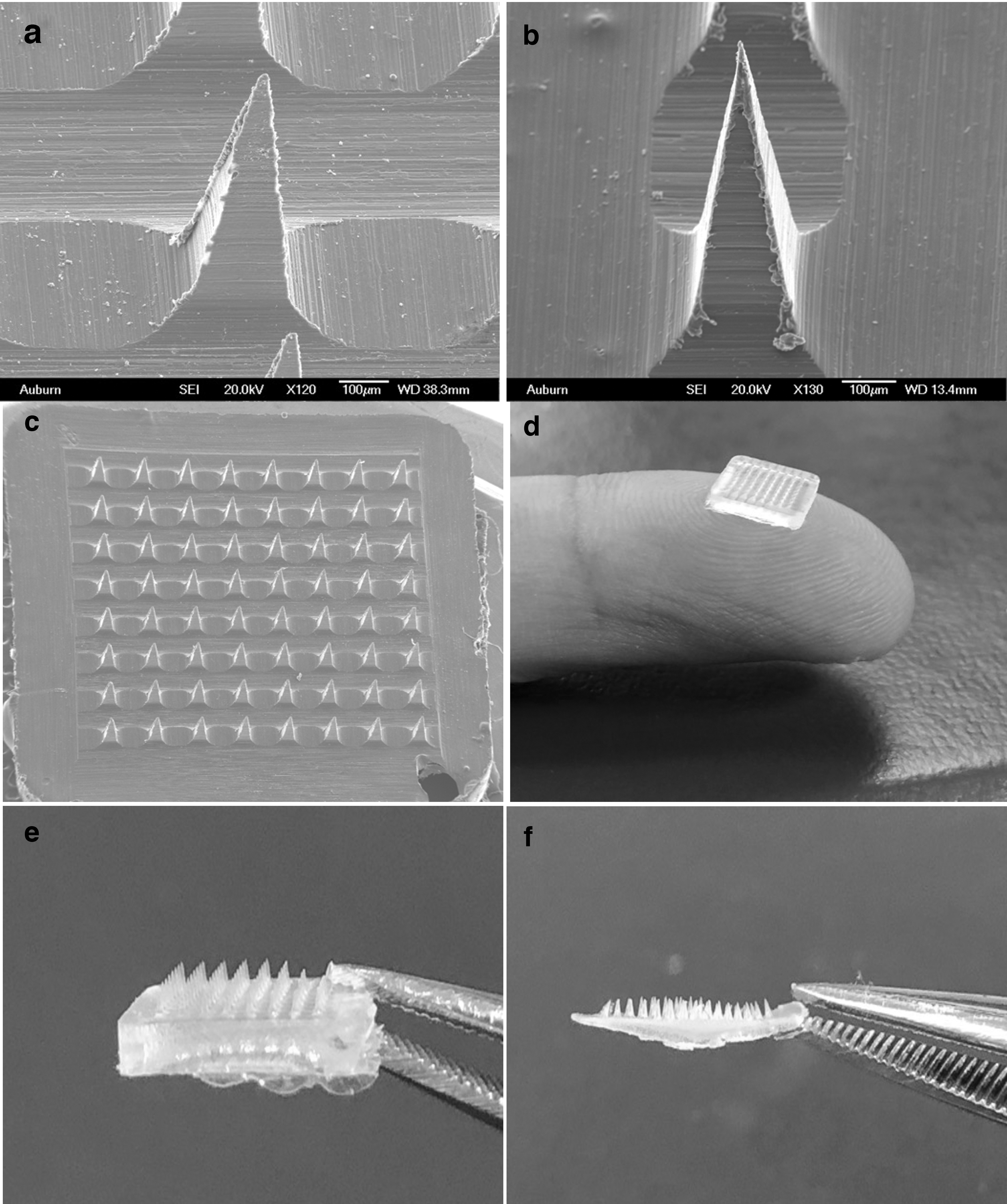
The microneedle array patch (8 × 8 needles) contained a total of 64 individual microneedles, with a needle length of 800 μm and base height of 200 μm (Fig. 1). The microneedle tips were 20 μm in diameter, and the needle pitch, the distance between each needle tip, was 680 μm. The final weight of the microneedles was ∼35 mg, and each array contained 1 mg of difluprednate. The compositions of each microneedle array are shown in Table 1.
SEM images
Percent Composition of Each Microneedle Array
L:G, lactide:glycolide; MW, molecular weight.
SEM analysis of the microneedles revealed that the arrays were uniform, and all microneedles appeared sharp without the presence of any cracks, fractures, or broken tips (Fig. 1a–c). The PAA microneedle backing dissolved completely in ∼40 min after being submerged in PBS pH 7.4. After the first inspection, the PAA backing began to transition into a gel, and at each remaining time point, the backing had continued to thin, meaning there was slow wicking of the PAA backing. Finally, at the 40-min time point, the backing was completely dissolved. Images before and after the dissolution of PAA are shown in Fig. 1d–f.
The microneedle failure force, or force required to break the microneedles, is evident by the sharp decrease in applied force in Fig. 2. The x-axis corresponds to the distance displaced by the upper stage after initial contact with the microneedle tips; the stage is then lowered until a preset distance of 1 mm is reached. After the microneedles are fractured, the applied force dips and then begins to increase again as it continues pressing against the microneedle backing until the preset distance is reached (data show ends after microneedle failure). The microneedle strength of each array is in the following order: C > B > A, which is directly proportional to the MW of the polymer(s) used.
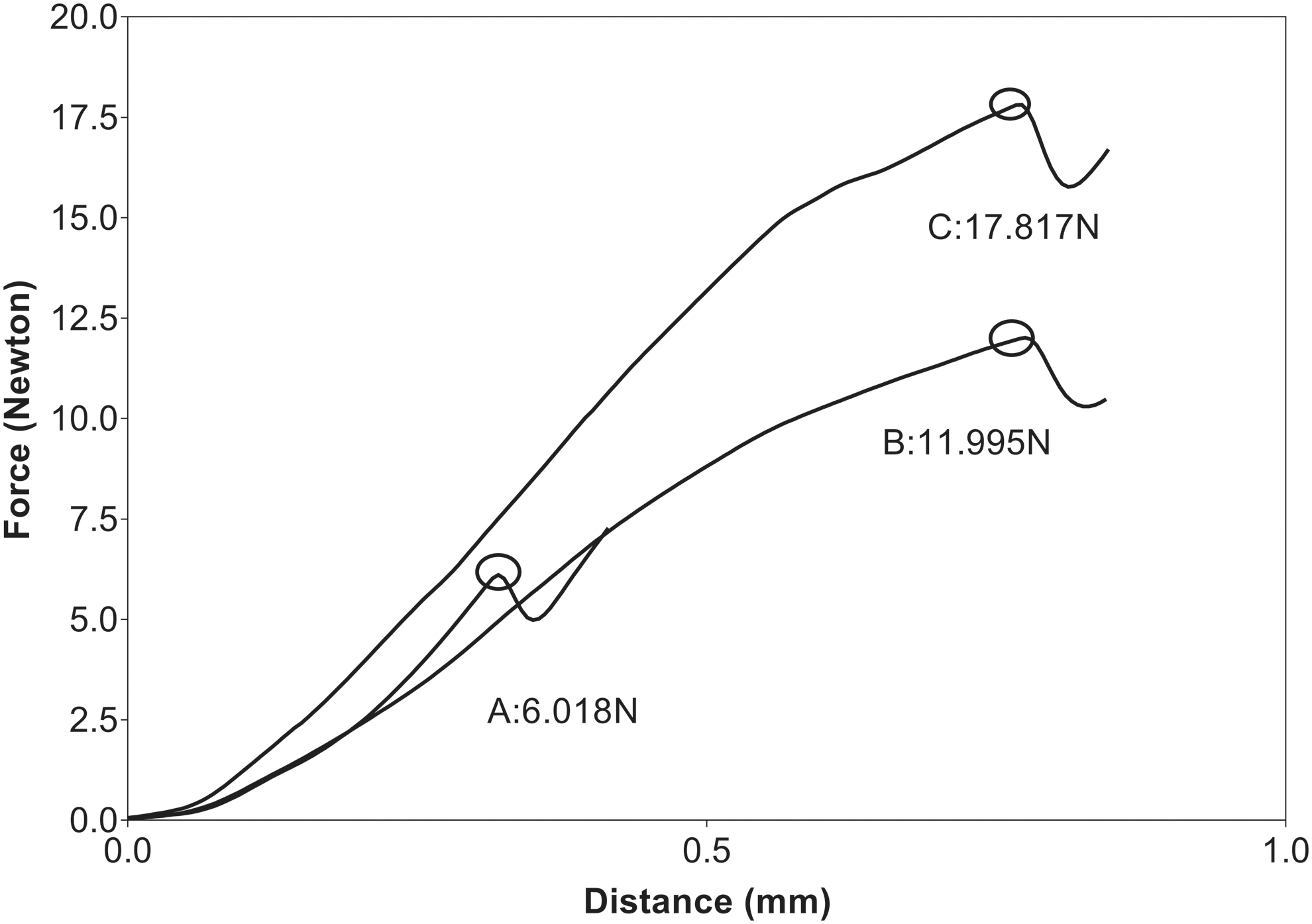
Stress–strain curves resulting from Texture Analyzer analysis. Plot shows data until microneedle failure point (dip in curve).
Furthermore, the lowest MW array, A, broke at a shorter distance compared with the higher MW patches, B and C. Needle breakage was confirmed using microscopy following texture analysis (data not shown). The force required for the insertion of microneedles in the sclera is shown in Fig. 3. A force of 2.57 ± 1.14 N, 6.83 ± 1.04 N, and 4.36 ± 0.26 N was required for the insertion of microneedle formulations A, B, and C, respectively, and these values were much lower than the force required to break the respective microneedles. Figure 4 shows the confocal images of optical sections of the sclera from the surface to a depth of 550 μm in the sclera after the insertion.
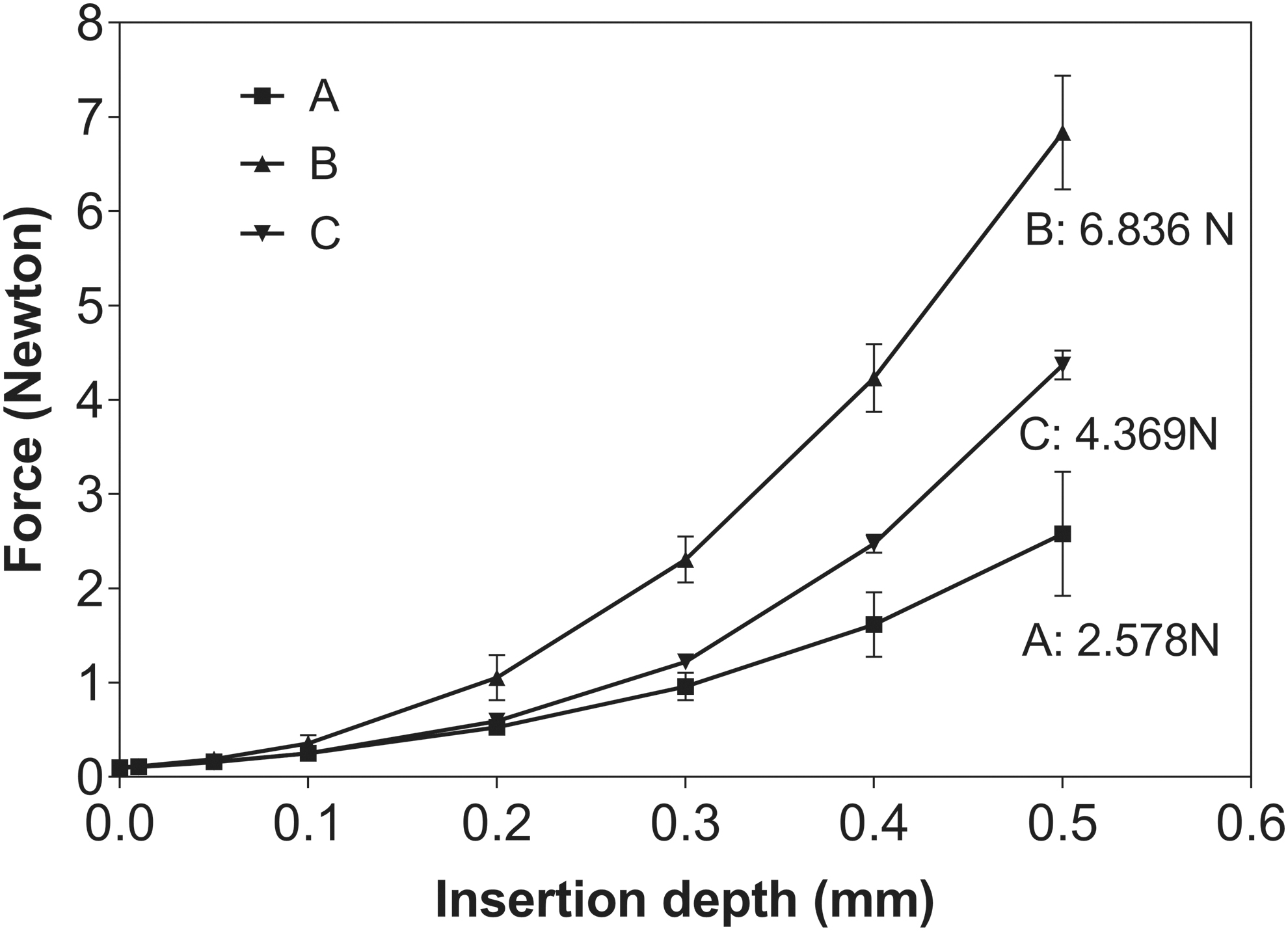
Graphical representation of force versus depth for the determination of insertion force into sclera. Data represent mean ± standard deviation, n = 3.
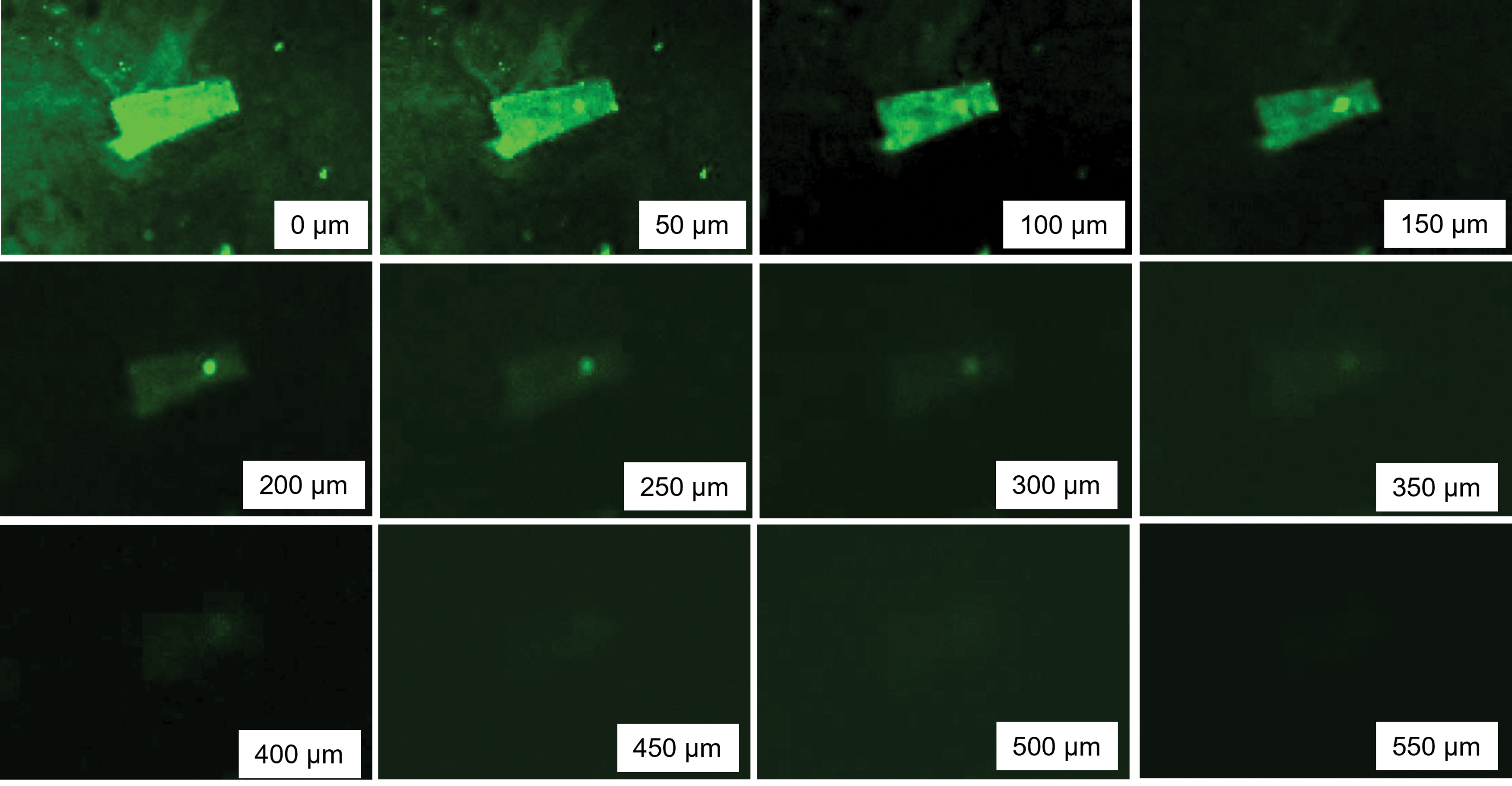
Confocal micrographs of optical sections of sclera from the surface (0 μm) to 550 μm inside the sclera created by the insertion of FITC-loaded microneedles. FITC, fluorescein isothiocyanate. Color images are available online.
Drug release and scleral permeation from microneedles
The release of the drug from microneedles was studied over a 7-day period, as shown in Fig. 5. The overall drug release from the microneedle patches was between 20% and 25% of the initial drug concentration. Array C had a slightly lower release compared with Array A and B. Furthermore, there was no significant difference in the release rates for the microneedle patches A (lowest MW) and C (highest MW). All the patches displayed a sustained-release profile, with a minimal occurrence of burst effect.
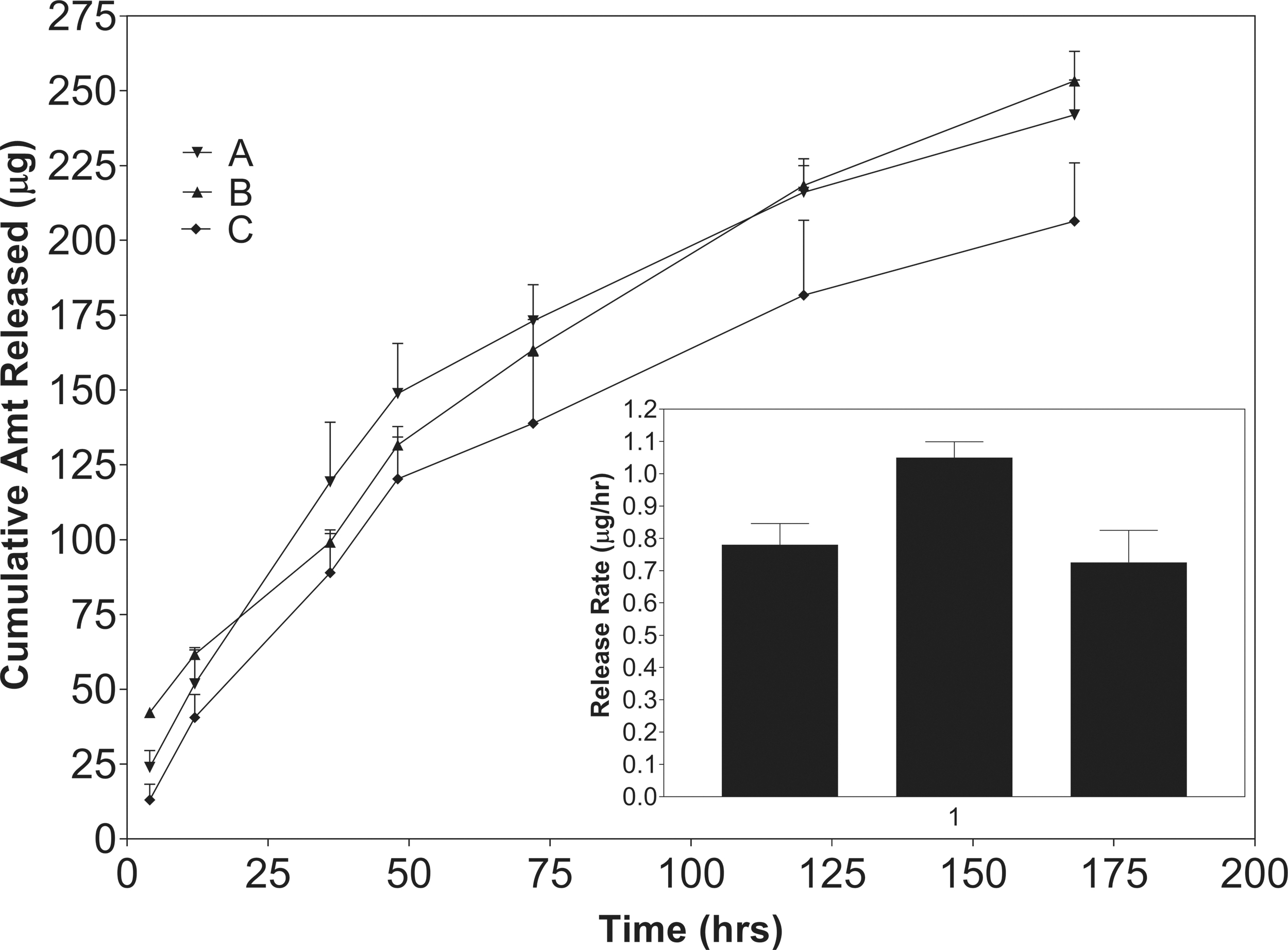
Sustained release of difluprednate from microneedle patches over a 7-day period. Data represent mean ± standard deviation, n = 3.
The kinetic profiles are indicative of diffusion-controlled drug release as the difluprednate release is proportional to the square root of time (Fig. 6). By fitting the experimental data to the Higuchi equation [Eq. (1)], the apparent diffusion coefficient, D, was determined for Arrays A–C: 9.164E-09, 9.13E-09, and 6.22E-09 cm2/s, respectively. The corresponding correlation coefficients were 0.92, 0.96, and 0.86 respectively.

Experimental data was modeled to the Higuchi equation [Eq. (1)] as shown by the solid line. The data were plotted as a function of the square root of time to display the linear relationship of release to time, as described by the Higuchi equation.
There was no significant difference in the permeation rate among the 3 microneedle patches (Fig. 7). However, as compared with the eye drop formulation, the permeation by all 3 microneedle formulations was significantly higher as compared with the eye drop formulation (P < 0.05).

Permeation of difluprednate across porcine sclera; inset: permeation rates calculated from the slopes of the permeation plots. Data represent mean ± standard deviation, n = 6. *P < 0.05 vs Eye drops (Durezol).
This observation was expected since PLGA is known to degrade slowly (weeks to months), and our application is intended for much longer than 24 h. In contrast, we observed significant differences in the amount of difluprednate retained in the scleral tissue.
The amount of difluprednate retained in the scleras appears to increase according to the MW of the polymer: A > B > C (Fig. 8). Array A had significantly higher retention after 24 h compared with array C (P < 0.05). Furthermore, array A was the only array to have a significantly higher release after 24 h compared with the 12-h time point. Array B exhibited a slightly higher difluprednate retention in the sclera compared with array C due to the lower MW of the Resomer RG 503 polymer.

Retention of difluprednate in porcine sclera following 12-and 24-h removal of microneedles. Data represent mean ± standard deviation, n = 6.
However, the scleral retention by all microneedle formulations was dramatically higher as compared with the eye drop formulation (P < 0.001). These differences were not observed in the permeation rate results, as the drug did not have sufficient time to permeate the sclera due to the short duration of the study for sustained release polymer like PLGA. The SEM inspection of the C microneedle arrays at 0, 12, and 24 h is shown in Fig. 9. A visual difference can be seen among the 3 images, where the image captured after the 24-h permeation study shows blunt tips of the microneedles.

SEM images of microneedles at 0 h
Discussion
Microneedle arrays were fabricated using PLGA, as this is the polymer of choice due to the long degradation timescale and compatibility and ocular acceptability.20,35,36 Based on our preliminary trials, polyvinyl pyrrolidone provided quick dissolution in <5 min; however, these backings were brittle. Hence PAA backing was used. These microneedles can easily be inserted into the sclera to target drug release into the SCS, a space between choroid and sclera, without piercing the chorioretina.17,19,37
Targeting delivery to the SCS provides enhanced local drug concentrations to the choroid/retina as compared with intravitreal injections or topical formulations. 17 The microneedle sharpness (20 μm diameter), the needle pitch, and the distance between the needle tips (680 μm) enable easy scleral penetration. The uniformity and sharpness of the microneedles were confirmed by the SEM images, as shown in Fig. 1.
The failure force testing (force required to break the microneedles) was performed to determine the physical strength of the microneedles. 32 The ocular (scleral) penetration of the microneedles requires them to be strong enough to remain intact, enabling easy piercing and anchoring in the eye, and hence the failure force test was performed. The strength of the microneedle arrays was found to be directly proportional to the MW of the polymer(s) used. 25 The lower MW array, A, broke at a shorter distance compared with B and C.
The force required for insertion is higher for the porcine sclera than the human sclera due to the anatomical and physiological differences between the tissues making the porcine sclera to be 2-fold thicker38,39 with higher mechanical strength. 40 In addition to sclera, microneedles due to their conical shape, the diameter increases from tip to base, and therefore, force required to insert 8 × 8 microneedle array was proportional to the insertion depth. 20
There was no correlation between the insertion force and the compression force to break the needles. This can be due to biological variation in the scleral structures from the animals. The average insertion force required to fully insert single microneedle into the sclera is 0.16, 0.42, and 0.27 N for A, B, and C, respectively. The required insertion force per single microneedle in our study was higher than the reported values in the literature. 20 This can be attributed to the fact that microneedles in our study differed in the polymer type, MW, and preparation method.
In addition to the insertion forces, the depth of penetration of microneedles into the sclera was examined using confocal microscopy. Based on the confocal images of the z-stacking, around 550 μm height of fluorescein-loaded microneedle array was inserted into the porcine sclera, which is around 70% of the total microneedle height. This is similar to the previous report, where 75% of total height was inserted for microneedle array containing only 9 microneedles. 20
Based on our preliminary studies to obtain optimal needle strength and the release rate profiles, we decided to work with those 3 lactide:glycolide (L:G) ratios in the study. The eye drop (Durezol) formulation delivers 25 μg/50 μL (per dose in 1 drop) to the eye surface. The microneedle patch contains 1,000 μg per array, which is attached to the scleral tissue for slow delivery over several days. The drug release pattern from the PLGA microneedles over a 7-day period suggested a marginal influence of the type the PLGA polymer type used in constructing the microneedles.
PLGA releases the drug by diffusion-controlled mechanism and by hydrolytic degradation over several weeks. Within the study period of 7 days, ∼25% of the initial concentration was released. Array A and B had a slightly higher release versus C; as expected, the higher MW latter (array C) would have caused lower drug release. 25 It appears that MW plays a role in controlling the release of difluprednate.
The higher glycolide content of array B also could increase the drug release because the glycolide degrades more rapidly in a hydrophilic environment, while the inverse is true for lactide. 25 The drug release kinetics suggest a diffusion-controlled mechanism according to the Higuchi equation, which provided correlation coefficients of 0.92, 0.96, and 0.86 for the arrays A, B, and C, respectively. PLGA was not expected to display release kinetics related to degradation and subsequent dissolution since significant degradation would not have occurred in a matter of hours to days.33,41 Based on the release trends, we anticipate the microneedles to last for 3–4 weeks.
As PLGA is known to degrade slowly over a period of several weeks, and our application is intended for much longer than 24 h, we did not expect to observe the formulation influence on the difluprednate release within the 24-h study period. Array C provided very low levels of difluprednate release until the 4 h, which cannot be explained well, except our speculation that the Array C used the PLGA of high MW.
Furthermore, the scleral studies were not performed past 24 h, as the integrity of the tissues would be compromised. Viability studies conducted on the sclera reveal it to be viable for 4 h, but no studies have evaluated the viability past 4 h. 42 We chose to study the permeation past 4 h because very little difluprednate would be released at 4 h due to the slow degradation timescale of PLGA. The steady permeation profiles suggest that the barrier property of the sclera was not affected.
The difluprednate retained in the sclera was inversely correlated to the PLGA MWs, and these results are also inversely proportional to the microneedle failure force, meaning the softer needles have a higher drug release leading to scleral retention. Furthermore, the weaker microneedle tips could have broken off following the removal of the patches, leaving the needles embedded in the tissue to continue degrading/releasing the drug following the conclusion of the studies.
The higher drug retention by Array A can be explained by the fact that these microneedles were made with the PLGA of lower MW, failure force, and the highest lactide content (100%). In the SEM images, a visible difference can be seen among the 3 microneedle arrays; the microneedles were blunt after 24 h compared with 12 h. No significant degradation is expected on such a small time scale since PLGA is known to degrade over a period of months. 34
The high scleral retention of difluprednate with the microneedle formulations as compared with the eye drop formulation was due to the penetration of the needles in the sclera and slow release of drug inside the tissue over time. The loading of difluprednate in the microneedles was much higher for slow and controlled release at the effective concentrations as compared with the eye drop formulation.
Conclusion
Difluprednate was successfully loaded into biodegradable microneedles for sustained-release drug delivery. Three types of patches were formulated with PLGA of varying MWs. PAA was used to produce a backing that dissolved within 30–40 min upon interaction with tear secretions. Texture Analyzer studies revealed that the needle fracture force was proportional to the MW of the microneedles. The insertion forces were significantly below the force required to break the microneedles. The microneedles penetrated to a depth of 550 μm. Release studies revealed a diffusion-controlled release of difluprednate over 7 days, without the occurrence of a burst effect.
Permeation studies using porcine scleras revealed no significant difference in permeation rate; however, the amount of drug retained in the sclera increased according to the MW: A > B > C. These observations suggest that the MW of the polymers affects the microneedle strength, while the lactide content directly affects the scleral permeation and retention of difluprednate. Thus, PLGA-based biodegradable microneedles have a potential future use as a drug delivery system for the sustained release of difluprednate for posterior eye conditions.
Footnotes
Acknowledgment
The authors acknowledge Auburn University Lambert-Powell Meats Laboratory for providing us porcine eyeballs.
Author Disclosure Statement
A part of the work has been published in the electronic version of the dissertation titled “Formulation of Water Insoluble Drugs for Ocular Delivery” by H.S., the first author of this article. 43 Authors declare no conflict of interest with the data generated and published.
Funding Information
There is no funding to report for this work.