
Abstract
Purpose:
Intravitreal injection has become a popular treatment for various retina disorders and dramatically increased over the past few years. In traditional preintravitreal injection, the preparation steps are time consuming for practitioners who perform a significant number of injections per day. Besides, lidocaine gel (L-Gel) shows a potential absorption barrier on the antibacterial effect of povidone iodine (PI).
Methods:
In this study, we describe a L/PI gel system as an alternative approach to address these issues for traditional preinjection drug administration. Lidocaine and PI are loaded in a thermoresponsive gel instilled as a liquid to the lower fornix that transitions to a stable, solid gel depot.
Results and Conclusion:
The gel demonstrated decrease in conjunctival touch sensitivity and sufficient bacteria killing with a single step, suggesting a significant decrease in the time required and less potential for drug inhibition due to sequential administration.
Introduction
Intravitreal injection is a common procedure used to administer medication to the posterior segment of the eye to treat a variety of ophthalmic conditions. The estimated annual number of intravitreal injections has dramatically increased over the past few years, largely in part due to the expanded availability and utility of antiangiogenic drugs, including antivascular endothelial growth factor (VEGF) for treating neovascular macular degeneration.1,2 The number of yearly intravitreal injections was consistently below 5000 before 2001; however, this number increased to over 5.9 million injections in 2016 alone due primarily to these angiogenesis inhibitors. 2
The most common intravitreal injections are intravitreal triamcinolone acetonide and VEGF antagonists, including pegaptanib, bevacizumab, and ranibizumab. 3 Initially, intravitreal injections were available only in an operating room setting but they have since become routine in the clinic. Indeed, several studies across different regions have confirmed that this procedure most frequently takes place in an office setting.4,5
Despite the ease of administering drugs through this route, complications after intravitreal injection can occur, including infectious and noninfectious endophthalmitis, retinal detachment, transient increase in intraocular pressure, and iatrogenic injury to the eye. 1 Endophthalmitis is a purulent inflammation of the intraocular fluids and tissues often caused by coagulase-negative Staphylococci, Staphylococcus aureus, and Streptococcus species after intraocular surgery. 3 Although recent studies suggest endophthalmitis rates following intravitreal injection are low, ranging from 0.019% to 0.052%,1,6–9 it remains a major concern for ophthalmologists due to its severity and the vast number of patients receiving injections. 10
Povidone iodine (PI) prep of the eye is a 2-step process, the eyelid prep followed by the injection site PI reapplication. 11 The use of preoperative PI eyedrops before intravitreal injection is associated with a significant reduction in endophthalmitis rates.12,13 However, PI can be very irritating to the ocular surface, therefore a topical anesthetic like lidocaine gel (L-Gel) is typically administered before PI. This combination of lidocaine and PI is standard practice to prepare a patient for intravitreal injection. It is worth noting that several studies have demonstrated a potential absorption barrier of L-Gel on the antibacterial effect of PI,14,15 possibly due to L-Gel preventing free molecular iodine from reaching the bacterial cell membrane and working as a cytotoxic agent.
One study suggested that using 2% L-Gel before PI is a risk factor for postoperative endophthalmitis. 16 In contrast, other studies conclude that the endophthalmitis rates are not affected by the sequence of preoperative drug administration.17,18 While at least 1 study 19 suggests that lidocaine does not prevent a significant physical barrier, this effect has been reported widely enough to warrant consideration in emerging preparation procedures such as the one described in this study.
The complete intravitreal injection procedure commonly lasts between 10 and 15 min, 20 most of which is required to prepare the eye for injection. These preparation steps involve instillation of topical anesthetic drops and 5%–10% PI solution, followed by a waiting period of ∼2–5 min for the drops to take effect.21–23 The amount of time required per injection is problematic for practitioners who perform a significant number of injections per day, in 1 example estimated to be 50–100 procedures per week. 24 Furthermore, ranibizumab is typically readministered about 10 times per eye over a 2-year period, thus necessitating a substantial time commitment from patients as well as providers. 25
To address concerns with both effectiveness and timing of traditional preintravitreal injection drug administration, we have developed a unique, thermoresponsive gel loaded with lidocaine and PI capable of autonomously delivering the full course of medication with a single drop. Our previous studies have demonstrated that the thermoresponsive and rheological properties of the polymerization of N-isopropylacrylamide (pNIPAAm) gel are well suited to topical, long-term use in the conjunctival fornix26,27 and that it is nontoxic. While other approved materials, such as poloxamers, have been used similarly, the gel/sol transition behavior is incompatible with the approach described herein. 28
The lidocaine and PI are simultaneously released to ensure efficacy of both drugs, both in preventing infection and maintaining proper anesthesia throughout the procedure. The efficacy in this study refers to that of the PI and lidocaine are not the intravitreally injected therapeutic. The results presented herein suggest that this novel combined drug delivery system may be an attractive alternative to the multiple preparation steps currently required before intravitreal injection drug administration while also addressing potential issues with efficacy caused by sequential drug administration.
Methods
All materials and reagents were obtained from Sigma (St. Louis, MO) unless otherwise specified.
Hydrogel fabrication
Free radical PNIPAAm was reported in our pervious study. 26 Briefly, 100 mg of PNIPAAm monomer was mixed with 2 mL of an 0.5 mg/mL solution of ammonium persulfate (APS) in MilliQ water. Five microliters of tetramethylethylenediamine (TEMED) initiator was added to the solution mixture and polymerization proceeded for 12 h at 4°C. Residual TEMED and APS were removed from the synthesized poly(N-isopropylacrylamide) (PNIPAAm) through repeated phase transition cycling (T > 37°C) in excess MilliQ water. The purified polymer was lyophilized for 48 h and stored at 4°C before rehydration.
Five milliliters of L/PI gel (L/PI-Gel) was prepared by rehydration of 400 mg lyophilized PNIPAAm in 1.05 mL of MilliQ water, then 0.45 mL of polyethylene glycol (MW 200 kDa) was added as an excipient. Two hundred milligrams of lidocaine hydrochloride monohydrate from Spectrum Chemical MFG Corp (Gardena, CA) was dissolved in 1 mL water and mixed with 2.5 mL of 10% w/v PI from Aplicare INC (Meriden, CT).
Hydration of the gels proceeded for 3 days with intermittent mixing and centrifugation at 4°C, 1,000 RPM (106 RCF). Samples were stored at 4°C until use. The final concentration of lidocaine and PI in 5 mL gel are 4% w/v and 5% w/v, respectively. The same procedure was used to fabricate other gels as listed here: blank gel without lidocaine and PI (E-Gel), L-Gel, and PI-Gel. Two different gels with higher lidocaine concentration of 6% w/v and 8%w/v were made and are identified hereafter as 6% lidocaine/PI gel (6% L/PI-Gel) and 8% lidocaine/PI gel (8% L/PI-Gel)
In vitro PI and lidocaine release study
To determine the amount of each PI and lidocaine being released from the gel matrix over time, 100 μL of L/PI-Gels were suspended in 400 μL of phosphate-buffered saline (PBS) from Fisher Scientific Company LLC (Pittsburgh, PA) and rotated at 37°C for a total of 30 min. After intervals of 2, 5, 10, 15, and 30 min (consecutively for a total release time of 62 min), the samples were spin down and the supernatant removed for analysis of lidocaine and PI content. The supernatant was then replaced with fresh PBS and samples were again rotated at 37°C.
PI concentration in supernatant samples was determined through UV/Vis absorption using a microplate reader set to a wavelength of 370 nm. Gel containing no PI was used as a blank, in which the supernatant was separated and analyzed to determine the contribution, if any, to the background signal for UV/Vis analysis. The thermoresponsive gel carrier becomes a solid when it reaches body temperature in the incubator. The drug is released in the supernatant from 1 continuous gel phase that does not break up into smaller pieces. The supernatant is removed at each time point and analyzed, and the gel is discarded at the end of the experiment.
Lidocaine concentration was measured by HPLC. The analyses were performed on the 1220 infinity LC (Agilent Technologies) system equipped with a dual gradient pump, integrated degasser, autosampler, column oven, variable wavelength detector (210 nm), and Agilent Open LAB CDS ChemStation for data acquisition.
Lidocaine concentration in supernatant was measured by running through a C18 reverse-phase column (InfinityLab Poroshell 120 EC-C18, 4.6 × 150 mm, 4 μm) at room temperature. Degassed solution of 0.1% aq phosphoric acid and acetonitrile were used as mobile phase A and B, respectively. The gradient program started at 10%B and ends at 90%B over 10 min followed by a 10 min return ramp to 10%B to wash the column before the next chromatographic run. The mobile phase flow rate was 0.8 mL/min with an injection volume of 5 μL.
Bacteria killing study
Tryptic soy agar plates were inoculated with Staphylococcus epidermidis, the predominant organism in case of postsurgical endophthalmitis. The blood plates (Remel™ Blood Agar [TSA w/5% Sheep Blood]) were fully covered with 100 μL of 1 × 108 bacteria. Each group was layered with different gels (Fig. 2). Also, 5% PI was applied on some agar plates (Fig. 2D, F). Then agar plates were incubated overnight at 37°C. Microbial growth was evaluated after 24 h.
Conjunctival touch sensitivity measurement
All animal protocols were approved by the Institutional Animal Care and Use Committee (IACUC) of the University of Pittsburgh and conducted according to the Association for Research in Vision and Ophthalmology (ARVO) Statement for Use of Animals in Ophthalmic and Vision Research. The study was performed on 3 healthy male New Zealand white rabbits per group. Rabbits were housed individually in approved, standard cages. While group housing was not utilized, environmental enrichment was provided daily in the form of exercise, novel items, and other methods. All rabbits were under resection of nictitating membrane in their right eye to facilitate gel drop retention.
This procedure was performed 2 weeks before installation of gels and the rabbits were closely monitored to control inflammation and infection. The 0.1 mL gels were instilled in the lower conjunctival fornix of the right eye for each rabbit through syringe. Animals were randomized to one of the following groups: (1) E-Gel, (2) 0.1 mL of 3.5% lidocaine hydrochloride ophthalmic gel (Akten®, Switzerland) (Akten Gel), (3) L-Gel, (4) 0.1 mL 5% PI was added for 2 min then 0.1 mL of L-Gel was placed, (5) L/PI-Gel, (6) 6% L/PI-Gel, or (7) 8% L/PI-Gel.
Conjunctival touch sensitivity measurements, referred to as conjunctival touch threshold (CTT) were recorded at 5, 10, 15, 25, 40, or 60 min after instillation of gels. Measurements were taken temporally on the bulbar conjunctiva. CTT was assessed using a Cochet–Bonnet esthesiometer with a nylon filament diameter of 0.12 mm, similarly to corneal esthesiometer but adapted to match the intravitreal injection site.
Briefly, the filament was brought into contact with the conjunctiva to evaluate the presence or absence of a blink response. The 5.5 cm filament was gradually decreased in length by 0.5 cm intervals until a blink reflex was observed (defined as at least 3 blinks out of 5 touches). The recorded length was the shortest length that did not induce a blink response. CTT was recorded as 0 when no blink reflexes were observed at 0.5 cm, indicating the maximum measurable depth of anesthesia induced by lidocaine. Baseline CTT was measured in the right eyes of each rabbit at time 0 before any treatment. The solidified PNIPAAm gels were easily removed after 5 min of instillation using sterile cotton swabs.
Results
The release kinetics of PI and lidocaine are shown on Fig. 1A and B, respectively. The necessary time frame of release to be appropriate for the preinjection procedure is confirmed with results for our L/PI-Gel eyedrop, with most of the lidocaine and PI released over ∼17 min. The total amount of drug released after 17 min was much less, if any, suggesting that the eyedrop has exhausted its drug release at that time and the drop could be removed without compromising efficacy.
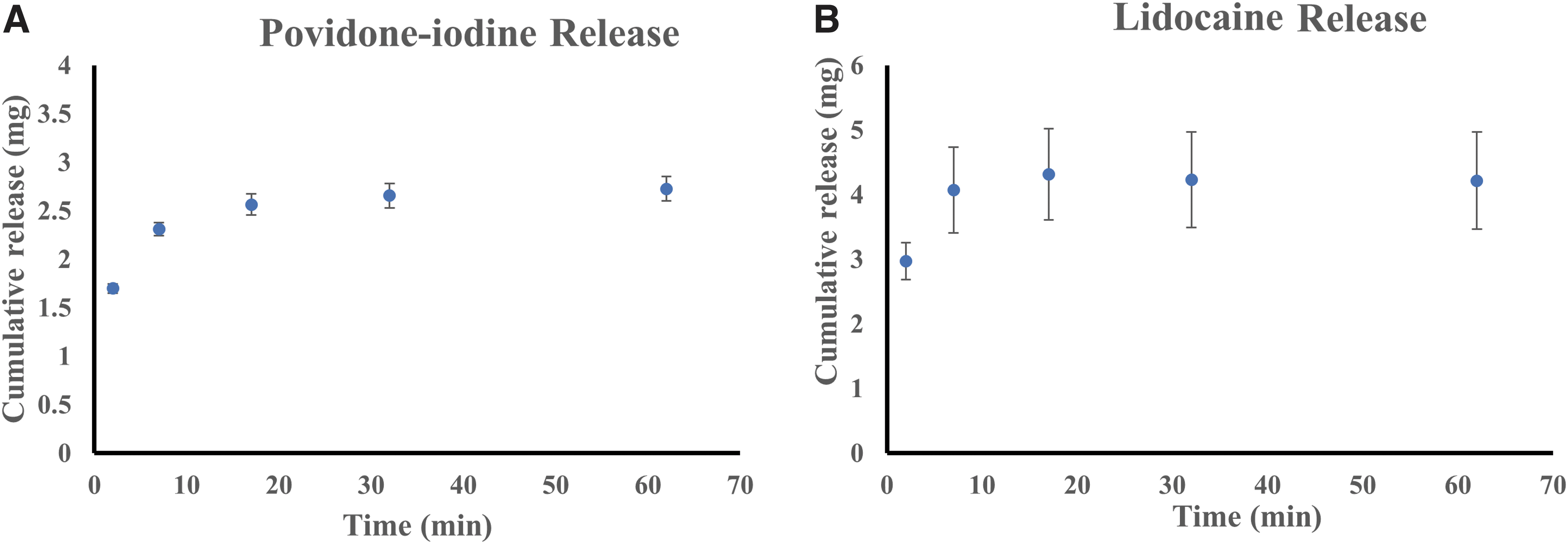
Lidocaine and PI release kinetics from L/PI-ge1.
The results of the in vitro bacteria killing study are shown in Fig. 2. Figure 2A shows the presence of bacteria in a control sample layered with E-Gel, while Fig. 2B, C shows they were covered with gels containing lidocaine. Significant bacterial growth was observed under all 3 of these testing conditions because they lacked an antiseptic agent. In contrast, S. epidermidis bacteria are killed by incorporating PI as an antiseptic agent, as shown in Fig. 2D and E. The plate in Fig. 2F was treated with Akten Gel for 1 min followed by application of 5% PI solution. The result indicates that the free iodine molecules could not pass the lidocaine barrier to kill the bacteria. However, the simultaneous administration of the experimental L/PI-Gel (Fig. 2G) shows no bacterial growth.

Evaluation of the antiseptic effect of L/PI-gel. In samples
CTT was measured in a healthy rabbit model following resection of the nictitating membrane. We used corneal touch threshold procedure presented in many publications29–31 to measure the conjunctival touch sensitivity with the difference that esthesiometer filament touched conjunctiva in our measurement. This measurement technique is a necessary step to better simulate human ocular anatomy and clinical use of the gel eye drop.
Mean ± standard deviation basal CTT for L/PI-Gel was 4 ± 0.5 cm and reduced to 0.5 cm after 5 min application of the gel. By increasing the concentration of lidocaine from 4% in L/PI-Gel to 6% and 8%, the CTT was reached to the maximal anesthesia effect (CTT = 0) and remained at zero CTT for 10 min. The same behavior was observed for applying Akten Gel, L-Gel, and traditional technique of using 5% PI followed by L-Gel (Fig. 3). All CTT measurements reached the basal CTT after 60 min of treatment.
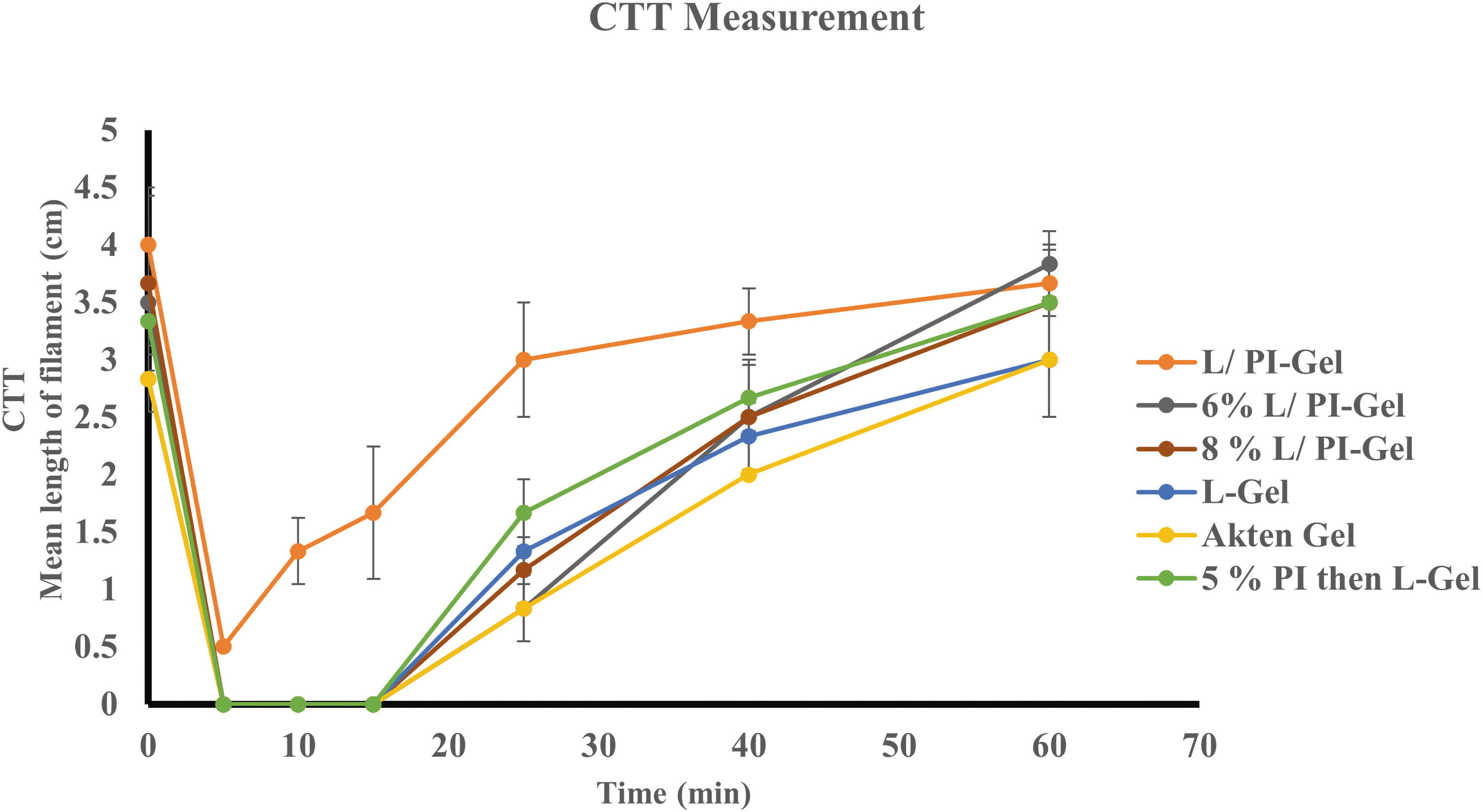
Compare different CTT measurements. Evaluate anesthetic effect of L/PI-Gels compare with different control conditions. CTT, conjunctival touch threshold. Color images are available online.
Discussion
Our gel is a simpler and more efficient format compared with the multiple preparation steps currently required before intravitreal injection. While these results are promising, additional in vivo safety and efficacy need to be done before use in humans, and to confirm the full translational potential of this treatment. The drug release property of the gel eye drop demonstrates a fast-acting and efficient delivery of the payload, with 74% of lidocaine (Fig. 1B) being released within 2 min of exposing to the body temperature (37°C). This amount of lidocaine is enough to significantly decrease the touch sensitivity of conjunctiva and at 5 min to reach to the maximal anesthetic effect.
PI 10% commercial formulation is a water-soluble polymer consisting of 90% water, 8.5% povidone, and 1% iodine. 32 Iodine has been known to be an effective antiseptic agent since the 18th century. 33 Therefore, the disinfectant property of PI is dependent on the amount of free iodine coming into contact with the surface to be treated.
It has been demonstrated that PI solution has rapid bacteria killing time at low concentrations (0.05%–0.1%) in vitro. The bacteria can be killed in less than 30 s in these dilute concentrations rather than more conventional 5%–10% solutions due to a greater availability of free iodine. 34 However, in vivo it has been shown that as the initial bacteria load increased, 5% PI more effectively reduced the bacteria on the ocular surface than 1%. 35 Additional studies support the use of 5% PI concentration before ocular surgery to decrease the bacterial flora of the ocular surface.36–38
In our in vitro study, PI was loaded in the gel matrix at a minimum of 5% and compared with various control groups. As is standard for such studies, bacteria killing was observed at 24 h, much longer than the time period over which bacteria killing would occur clinically. Therefore, future studies may examine at the immediate effect on a much smaller, more clinically relevant bacterial load.
The in vitro results, however, demonstrate significant killing bacteria activity as compared with standard PI solution suggesting the potential efficacy of this method in vivo. The need for free iodine to contact the surface containing bacteria is readily apparent in Fig. 2F, indicating that the L-Gel acts as a barrier on antibacterial action of PI when it is applied first. This observation agrees well with previous studies,14,15 thus supporting the finding that both concentration and availability of free iodine are critical in proper antiseptic activity of PI solution in any form. In our experiment, thermoresponsive gel eye drop system, PI with or without lidocaine, was shown to effectively kill bacteria, presumably due to ease of access to the bacteria cell membrane.
Lidocaine and free iodine molecules are simultaneously released from our thermosensitive gel when is reached to the body temperature, and there is no viscus gel barrier to prevent free iodine from reaching the bacteria. The combination of L-Gel with PI was reported elsewhere. 39 The novelty of our lidocaine/PI system compared with this previously reported combined mixture is our drugs (PI/lidocaine) are loaded in a thermoresponsive gel. The results of our study suggest that there may be a significant advantage in prep time while maintaining the proper efficacy for sequential drop administration.
The advantages of using topical L-Gel versus lidocaine subconjunctival injection before an intravitreal injection are patient comfort and lack of clinical or histopathological adverse effects on ocular tissues.40,41
In our experimental combined L/PI-Gel eyedrop, CTT was nonzero (indicating incomplete depth of anesthesia) compared with higher concentrations of lidocaine in the same system. The interaction between lidocaine with free iodine may have reduced available lidocaine molecules to block voltage-gated Na+ channels in the neuronal cell membrane, thus necessitating a higher percent lidocaine in the gel upon initial loading. Although using L-Gel and 5% PI solution separately can make conjunctiva numb as effectively as our optimized gel combinations of 6%L/PI-Gel and 8%L/PI-Gel, the free iodine in PI solution might not reach the bacteria. Furthermore, applying PI solution before lidocaine can cause discomfort and irritation. 35
The results of our in vivo study suggest that, while a slightly higher concentration of lidocaine may be needed, the benefit of combining both drugs to avoid concerns about the order in which to administer them is unique to this novel gel eye drop.
Conclusion
By increasing the annual number of intravitreal injections, having a fast and effective preintravitreal injection procedure feels as an essential need. Our thermosensitive gel loaded with lidocaine and PI can be a better alternative to the traditional use of these drugs in preintravitreal injection. The L/PI-Gel system can simultaneously release lidocaine and PI without interfering the lidocaine barrier in bacterial activity of PI. The conjunctival touch sensitivity can be significantly decreased by our fast-responsive gel.
The other unique aspect of our gel system is the ease of use and replace during the procedure. The solidified gel can easily be removed from the corner of the eye after 5 min of installation. This fast-acting and more streamlined format may reduce the preparation steps before intravitreal injection and may benefit both clinicians and patients with a more consistently effective infection prophylaxis method.
Footnotes
Acknowledgment
The authors are grateful to Dr. Robert M.Q. Shanks's assistant for the bacteria killing study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by NIH CORE Grant P30 EY08098 to the Department of Ophthalmology, the Eye and Ear Foundation of Pittsburgh, funding from an unrestricted grant from Research to Prevent Blindness, New York, NY, and funding from UPMC Immune Transplant and Therapy Center (IPA 2019 No. 17).