
Abstract
Keratitis is a disease characterized by inflammation of the cornea caused by different pathogens. It can cause serious visual morbidity if not treated quickly. Depending on the pathogen causing keratitis, eye drops containing antibacterial, antifungal, or antiviral agents such as besiloxacin, moxifloxacin, ofloxacin, voriconazol, econazole, fluconazole, and acyclovir are used, and these drops need to be applied frequently due to their low bioavailability. Studies are carried out on formulations with extended residence time in the cornea and increased permeability. These formulations include various new drug delivery systems such as inserts, nanoparticles, liposomes, niosomes, cubosomes, microemulsions, in situ gels, contact lenses, nanostructured lipid carriers, carbon quantum dots, and microneedles. Ex vivo and in vivo studies with these formulations have shown that the residence time of the active substances in the cornea is prolonged, and their ocular bioavailability is increased. In addition, in vivo studies have shown that these formulations successfully treat keratitis. However, it has been observed that fluoroquinolones are used in most of the studies; similar drug delivery systems are generally preferred for antifungal drugs, and studies for viral and acanthameba keratitis are limited. There is a need for new studies on different types of keratitis and different drug active substances. At the same time, proving the efficacy of drug delivery systems, which give promising results in in vivo animal models, with clinical studies is of great importance for progress in the treatment of keratitis.
Introduction
The eye is a complex organ that can be divided into 2 parts, the anterior segment and the posterior segment, and both can be affected by various diseases. 1 Keratitis is a corneal disease caused by bacteria, fungi, viruses, or amebae. If the infecting pathogen is not removed promptly, it can cause severe ocular morbidity, corneal scarring, and vision loss. Keratitis is rarely seen in a healthy eye because defense mechanisms of the eye create a barrier against keratitis. However, the use of contact lenses, corneal injuries and traumas, or other diseases that may occur on the surface of the eye can create various weaknesses in the defense mechanism and make the cornea vulnerable to keratitis.
Different active pharmaceutical ingredients are preferred in the treatment of keratitis types caused by different pathogens.2–4 But the common point for all types of keratitis is the necessity of starting the treatment as early as possible. If the treatment is delayed, corneal opacification and serious corneal ulcers can be observed, and severe vision loss may occur. 5
Conventional eye drops, which are most commonly used in treatment, have some disadvantages. The most important one of these is the rapid removal of the eye drops from the eye surface with nasalacrimal drainage as a result of the dilution of the eye drops with the tear film. Ocular bioavailability may decrease to 5% due to this situation. Due to the low ocular bioavailability, the frequency of application is increased to provide an effective treatment, but this reduces patient compliance and may cause various side effects. 6 For this reason, research studies are carried out on new drug delivery systems. Formulations of different active substances are developed using different methods. The purpose of this review is to discuss some new drug delivery systems that have the potential to increase the success of keratitis treatment.
Ocular Anatomy and Physiology
The eye is a remarkable structure with a peculiar and intricate arrangement within the eye sockets, and contains complex tissues that allow for vision. 7 It measures ∼2.5 cm in diameter and has a volume of 6.5 mL. The eye can be separated into 2 parts physiologically; the anterior segment, which is comprised of the cornea, conjunctiva, ciliary body, iris, aqueous humor, lens, and lachrymal system, and the posterior segment, which is comprised of the retina, vitreous humor, choroid, and sclera. 8
Anterior segment of the eye
The cornea is an opaque, veinless, and nearly dehydrated tissue. It is more permeable to cations at physiological pH due to its negative surface charge. Conjunctiva is a thin opaque layer containing mucus that covers and lubricates the eye's surface, and due to its high vascularity, also nurtures the cornea. 9 Aqueous humor is a transparent, moist substance that fills the space behind the cornea. 10
Posterior segment of the eye
Retina is the eye's innermost tissue and composed of 2 layers: an outer layer (pigment epithelium) and an inner layer (neuroepithelium), which controls the light-receiving and light-transmitting functions. 11
Factors limiting ocular bioavailability of drugs
Tears
Tears contribute to the maintenance of proper eye function and are produced by tear glands. Three layers form the tear film: an outer lipid layer (0.1 μm length, secreted by meibomian glands), a middle hydrophilic layer (7–10 μm), and an inner mucous layer (0.2–1.0 μm). While these tear factors significantly contribute to visual function, they have damaging outcomes on ocular drug bioavailability. 12 Given that a cul-de-sac could contain ∼30 μL and individual tears comprise ∼7 μL, tears tend to have a significant diluting impact on topical drugs. 12 Another factor influencing bioavailability is the presence of proteins and mucins in tears that adhere to drug compounds, reducing the amount of drug in contact with the cornea. 13
Conjunctiva
By developing mucus and antimicrobial peptides, the conjunctiva helps in both eye surface preservation and lubrication. Since tight junctions occur on the outer side of its cells, the conjunctiva has a high degree of vascularization and plays a major role as a defense barrier on the ocular surface. 14
Cornea
Cornea is mostly composed of epithelium, stroma, and endothelium. Besides providing ocular safety, cornea provides about two-thirds of the eye's optical capacity. However, owing to its structure, it acts as a physical obstacle, preventing permeation of drug molecules. Epithelial and endothelial membranes, with their abundant lipid content, function as barricade to the transport of hydrophilic compounds. In addition, the presence of tight junctions among corneal epithelial cells restricts the paracellular permeation of drugs, which causes a decrease in the corneal permeation to hydrophilic drugs.
The stroma formed by a highly aqueous extracellular matrix composed of a lamellar structure of collagen, which causes the cornea to become more impervious to lipophilic drugs. 15 The endothelium of the cornea is a single cell membrane that is connected to the aqueous humor. Because the corneal endothelium is composed mainly of phospholipids, lipophilic substances can move through it, whereas hydrophilic substances are difficult to pass. To summarize, for a drug to penetrate through the cornea, it should possess an amphiphilic disposition, defined as the existence of both hydrophobic and hydrophilic structures within the same framework. 16
Blood-ocular barriers
Blood aqueous barrier points to the tight junctions of the ciliary body's unpigmented epithelium, the iris tissues' junctions, also the iris blood vessels. As a result of its anatomic location, this obstacle prevents drug substances from reaching the anterior part of the eye. 17
Microbial Keratitis: Disease and Treatment
Physiological and pathological changes in the cornea due to keratitis
The first deterioration due to infections developing in the cornea is corneal ulceration. This is followed by stromal infiltration by polymorphonuclear and lymphomononuclear cells. This infiltration causes destruction of Bowman's layer and subsequent stromal necrosis, which may result in occlusion of the vessels feeding the cornea. In case of exacerbation of these necroses, Descemet's layer may be exposed as a result of focal corneal thinning called Descemetocele. At the same time, the immune response of the body causes superficial corneal vascularization and epithelial regeneration to prevent necrosis in the layers of the cornea.
Depending on the resistance of the pathogen causing the disease and the low resistance of the body at that moment, the entire cornea may be surrounded by the pathogen. The resulting corneal epithelial defects allow pathogens to invade the inner parts of the eye. Progressive pathogens block the iris and pupil, but also affect the thin fibrous tissue of the conjunctiva, resulting in the formation of a false cornea (pseudocornea). Perforations and opacification of the cornea, depending on the course of the disease, cause a decrease in vision or even its complete loss. Since corneal opacification and perforations are mostly irreversible, corneal transplantation is required to restore the cornea to its former function. 18
Microbial keratitis
Microbial keratitis is an acute disease of the cornea due to bacteria, fungal, viral infection, or ameba. 18 Microbial keratitis has an incidence of 11/100,000 in the United States, 19 while it has 799/100,000 persons in a year in developing countries. 20 Corneal epithelium mucins and antibodies are the primary ocular protection against microbial keratitis.21,22 As a result, conditions that disrupt corneal epithelial membrane, such as physical/chemical trauma, scarring, and contact lens use, contribute significantly to the risk of developing microbial keratitis.23,24
Bacterial keratitis
The most frequent form of microbial keratitis is bacterial keratitis, and it is responsible for 90% of all cases. 25 The pathogens that cause bacterial keratitis are highly variable based on the geographic position of the patient. Nevertheless, Pseudomonas, Streptococci, Staphylococci, and Serratia species are the most often identified bacteria in cases of bacterial keratitis.26–28
Bacterial keratitis may have various clinical symptoms. In patients with bacterial keratitis, blurred vision, excessive tearing, photophobia, eye discharge, redness, and pain are common symptoms.29–31
Per the American Academy of Ophthalmology (AAO), topical antibiotic treatment improves the vast majority of cases of bacterial keratitis.32,33 Table 1 contains the protocol based on the AAOs 2018 Preferred Practice Pattern study for bacterial keratitis.
Antimicrobials for Treatment of Keratitis
Fewer gram-positive cocci are resistant to gatifloxacin, moxifloxacin, and besifloxacin than other fluoroquinolones.
Besifloxacin 6 mg/mL; ciprofloxacin 3 mg/mL; gatifloxacin 3 mg/mL; levofloxacin 15 mg/mL; moxifloxacin 5 mg/mL; ofloxacin 3 mg/mL, all commercially available at these concentrations.
For resistant Enterococcus and Staphylococcus species and penicillin allergy. Vancomycin and bacitracin have no gramnegative activity and should not be used as a single agent in empirically treating bacterial keratitis.
Systemic therapy is necessary for suspected gonococcal infection.
The AAO 2018 report provides significant and reliable evidence that just fluoroquinolone treatment is almost equally effective as combined therapy with strengthened drops. 33 Fluoroquinolones are a class of antibiotics with a wide range of activity. They block the DNA gyrase (topoisomerase II) but also topoisomerase IV enzymes. 34 U.S. Food and Drug Administration (FDA) has approved fluoroquinolone antibiotics such as ciprofloxacin 0.3%, levofloxacin 1.5%, and ofloxacin 0.3% to be used in bacterial keratitis treatment. Due to development of tolerance to second-generation fluoroquinolones, fourth-generation fluoroquinolones such as moxifloxacin and gatifloxacin are being utilized in bacterial keratitis treatment.
While FDA has not approved moxifloxacin or gatifloxacin about this indication yet, they have already been considered for bacterial keratitis treatment. 33 Whereas moxifloxacin tolerance was found in 33.6% of all Staphylococcus aureus’ 1,695 isolates, methicillin-resistant S. aureus (MRSA) was detected in 72.8% of all 621 isolates. 35 Similar studies show increased tolerance to fourth-generation fluoroquinolones.36,37 Nevertheless, besifloxacin 0.6%, a recent marketing ophthalmic fluoroquinolone, was found to be advantageous to other ophthalmic fluoroquinolones in in vitro research against methicillin- as well as ciprofloxacin-resistant S. aureus and Staphylococcus epidermidis. 38 Besifloxacin was found significantly effective than gatifloxacin and moxifloxacin at decreasing MRSA or Pseudomonas aeruginosa keratitis.39–41
Fungal keratitis
Fungal keratitis is prevalent corneal disease with ∼1 million incidence each year and responsible for 1%–45% of infectious keratitis cases. 42 Infected individuals are commonly healthy, young farmers or outdoor employees who suffer injuries from organic material.43–45 Besides, former ocular surgery, ocular surface disorder, contact lens usage, and past topical or systemic corticosteroid usage disorders have been identified as risk factors for filamentous fungal keratitis. 46
The most common pathogenic fungi causing keratitis are commonly Aspergillus and Fusarium.47,48 Men were observed to have a greater rate of fungal keratitis morbidity than women, by a rate of 1.6:1.49,50 The frequency of fungal keratitis varies considerably between species and geographic locations.51–53
The presence of infiltration with uneven feathery edges accompanied with an overlying epithelial deficiency, stellate ulcers, and conjunctival hyperemia indicates clinical signs for fungal keratitis.43,54
Management of fungal keratitis presents a serious challenge since delaying diagnosis, inadequate therapy, or negligence might enable and accelerate progression of fungal growth. Fungi progressively infiltrate the cornea's flexible layer and finally produce endophthalmitis that may result in eyeball enucleation.55–57
Natamycin 5% suspension, available on the market, is the first-line treatment for fungal keratitis in medical care. It is currently the only authorized medication by FDA for management of fungal keratitis.58,59 Antifungal polyenes work by attaching to ergosterol found on the fungal cell surface. This interaction is hypothesized to cause porosity in membrane, altering membrane permeability and ultimately resulting in fungal cell death, possibly due to the outflow of essential intracellular chemicals. 60
For the treatment of fungal keratitis, topical ophthalmic solutions of 0.1% voriconazole, 0.2% posaconazole, 1% miconazole, 2% econazole, and 2% fluconazole have also been utilized.61,62 Voriconazole is efficient toward Candida, Aspergillus, and Fusarium, while fluconazole is more efficient for Candida. 63 Completed and ongoing investigations evaluating the performance of certain azole antifungals compared with natamycin have revealed mixed results; the majority confirming superiority of natamycin.62,64
Other drugs for fungal keratitis are Echinocandins, which include caspofungin, micafungin, and anidulafungin, are a novel family of antifungal drug molecules.65,66
Another option is Micafungin (Mycamine™; Astellas Ireland, Killorglin, Ireland), which is also injected intravenously in doses ranging from 100 to 150 mg per day.67,68
Viral keratitis
Keratitis caused by herpes simplex virus (HSV) has affected ∼500,000 persons in the United States and 1.5 million worldwide. Although less frequently, varicella-zoster virus and cytomegalovirus can also cause keratitis.69,70 In developed countries, the prevalence of ocular HSV infection is also estimated at 150 cases per 10,000 persons and 5–20 cases per 10,000 persons annually.71,72
In contrast to bacterial and fungal keratitis, HSV keratitis could be chronic and intermittent. Light sensitivity, tears, conjunctival injection, a foreign body sensation, and impaired vision are possible symptoms.73,74
Antivirals have been used to treat HSV epithelial keratitis either topically or systemically, depending on the severity of the disease.75,76 At the present time, topical drugs such as trifluridine, ganciclovir, and acyclovir are accessible. 73 Trifluridine is available as an ophthalmic solution in a market, whereas ganciclovir is available in a gel form.73–78
Acanthameba keratitis
Acanthameba is protozoa that can be found easily in the environment, air, soil, and water. 79 In the occurrence of corneal infection, Acanthameba is initially connected to the epithelial cells of the cornea through the mannose-binding lectin.80–83
In the 1970s, the first cases of acanthameba keratitis were reported.84–86 The primary risk factors are prolonged contact lens wear, contact lens wear while bathing, and contact lens washing with tap water.86,87
Around 75%–90% of patients with acanthameba keratitis are misdiagnosed at early stages of the disease since it is hard to relate characteristic acanthameba keratitis signs.85,88 Clinical symptoms of acanthameba keratitis include pseudodendritiform epitheliopathy, epithelial microerosions, microcysts, multifocal stromal infiltrates, and ring infiltrate.89,90
Acanthameba keratitis is usually misdiagnosed and treated as herpetic, bacterial, or mycotic keratitis due to the similarity of several clinical signs and symptoms. Diamidines such as propamidine-isethionate (Brolene), hexamidine-diisethionate (Hexacyl), and dibromopropamidine are administered at a concentration of 1%. Biguanides have been used in 0.02% concentrations, like polyhexamethylene-biguanide (Lavasept) and a chlorhexidine (Curasept).91,92 Neomycin is another treatment option. 93 Miconazole, clotrimazole, and voriconazole have traditionally been topically used in treating acanthameba keratitis.94,95
Novel Antimicrobial Drug Delivery Systems for Keratitis
Over the last 2 decades, ocular drug delivery systems such as nanoparticles, lipid nanocarriers, microemulsions (MEs), liposomes, niosome, cubosome, dendrimers, in situ forming hydrogels, ocular inserts, contact lens, microneedles (MNs), carbon quantum dots (CQDs), and iontophoresis have been developed to improve the treatment of keratitis (Fig. 1).
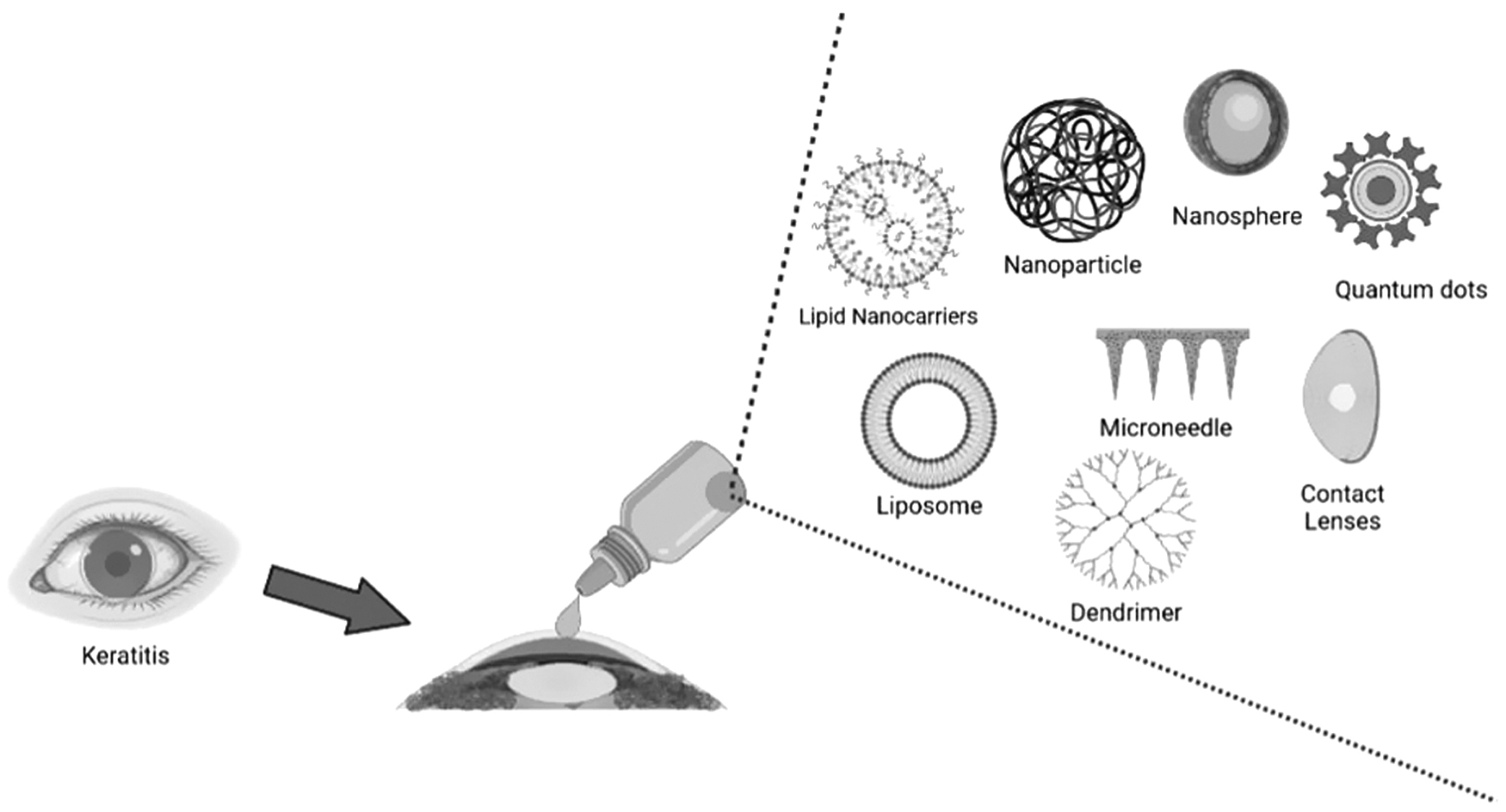
Some of the novel drug delivery systems for the treatment of keratitis.
Nanoparticles
During the last 2 decades, nanoparticle drug delivery has demonstrated promising outcomes in ocular drug delivery. Nanoparticles are a viable choice for ocular drug delivery due to their small size, and their sustained release characteristic that minimizes the need for repeated administration. Nanoparticles are described as particles with a diameter <1 μm, and their hydrodynamic diameter is generally optimizes pharmacokinetic parameters. A tiny size typically has a higher renal clearance, while a bigger size may be ingested by phagocytosis. However, since nanoparticles have a higher surface area to volume ratio, they could carry enormous payloads of drug substances.
Due to their small size, the nanoparticles are rapidly absorbed by the cells and appropriately deliver relatively much drug payload. Drug molecules can be loaded into nanoparticles by several methods: attachment to the surface, conjugation, entrapment, and encapsulation. This coupling enables improved adjustment of tissue distribution and sustained release. In various particle sizes and characterizations, materials have been utilized to generate nanoparticles, such as metals, nonmetals, semiconductors, polymers, and lipids.7,96,97 Preclinical developments of various nanoparticle-based formulations targeting keratitis are summarized in Table 2.
Some of the In Vitro and In Vivo Application Studies of Nanoparticle-Based Ocular Drug Delivery Systems for Keratitis Disease
β-CD, β-cyclodextrin; AC, Acanthameba castellanii; Ad-MMP-S PEPs, matrix metalloproteinase-9-sensitive peptides terminated with adamantane; API, active pharmaceutical ingredient; Ce6, chlorin e6; CS, chitosan; DL, drug loading; EE, encapsulation efficiency; MMP, matrix metalloproteinase; NA, nonavailable; NPs, nanoparticles; PDT, photodynamic therapy; PLA, poly(lactic acid); PS, particle size; SBE, sulfobutylether; ZP, zeta potential.
For ocular drug delivery formulations, different polymers have been utilized to generate nanoparticles, such as poly(ɛ-caprolactone), chitosan, alginate, hyaluronic acid, eudragit, carbopol, gelatin, poly-(butyl)cyanoacrylate, and poly(lactic-co-glycolic acid).98,99 Nanoparticles containing therapeutics might be in the form of nanocapsules or nanospheres. The drug is entrapped within the polymeric shell for nanocapsules, whereas the drug is dispersed throughout the matrix material for nanospheres. Numerous researchers have sought to establish drug-loaded nanoparticles for delivery to both anterior and posterior ocular regions during the last few decades. However, common problems with nanoparticles are low-drug loading and particle aggregation, burst release and lack of scale-up techniques.100–102
Lipid nanocarriers
The first-generation lipid nanoparticles are nanoparticle-encapsulated solid lipids, and thus called solid lipid nanoparticles (SLNs). Because of some recognized disadvantages of SLNs such as drug leakage through the matrix during preservation and low-drug loading rate, nanostructured lipid carriers (NLCs) were designed. The NLC formulation idea is based on the encapsulation of the drug into variable proportions of solid and liquid lipids. NLCs were developed to achieve less crystalline matrix with a solid core to resolve the constraints associated with the crystal structure of SLNs' core. The formulation parameter that distinguishes both is content of the core/matrix. Drugs are dissolved or encapsulated into the solid lipids in SLNs.
On the contrary, in NLCs, the drug is dissolved or melted in the liquid and solid lipid mixture, and distributed into aqueous phase consisting of surfactants. The lipid core preserves the drug from degrading, prolongs the drug's ocular residence period, and improves adhesion to the tear lipid layer. In addition, the lipid core is mainly covered by an emulsifier interface that functions as a penetration enhancer to elevate ocular bioavailability even more. However, the major disadvantages of SLNs are insufficient loading capacity, drug expulsion on long-term storage, and possible cytotoxic effects associated with the nature and concentration of the matrix.115–117 Preclinical developments of various lipid-based formulations targeting keratitis are summarized in Table 3.
Some of the In Vitro and In Vivo Application Studies of Lipid-Based Ocular Drug Delivery Systems for Keratitis Disease
MIC, minimum inhibitory concentration; NLCs, nanostructured lipid carriers; PLA, poly(lactic acid); Vis, viscosity.
Microemulsions
ME is a mix of oil and water that are often prepared using a surfactant along with a cosurfactant. It is an opaque, thermodynamically robust liquid with typically 20–200 nm droplet size range. 121 Either oil-in-water (O/W) or water-in-oil (W/O) might be used to design these MEs. Generally, O/W MEs have a high water phase ratio, while W/O MEs have a higher oil phase ratio. In conditions with similar volumes of water and oil, a bicontinuous ME could occur. 122 It consists of aqueous and oiled components that could use to entrap both hydrophilic and lipophilic drugs. In addition, the extended drug release capacity of MEs renders these carriers highly desirable to the eye since they could minimize the frequency of administrations of eye drops daily. MEs may cause ocular irritation due to the surfactant used to increase their stability. 123
Shanni and Karthikeyan (2017) designed Moxifloxacin-loaded MEs to be used in the treatment of bacterial keratitis. ME was formulated using Tween 80, Span 20 (nonionic surfactants), isopropyl myristate, and acetate buffer by the pseudoternary phase diagrams. A ME with a droplet size of 36.25 nm was obtained, and no significant change was observed during 3 months stability study. The developed formulation showed sustained release compared with marketed product, and it has been shown that increasing the water content in formulation results in decreased drug release. Moreover, bacteria growth was efficiently inhibited, and the required treatment time was significantly decreased, as well as administration frequency. No ocular irritation was observed. 124
Liposomes
Liposomes are round-shaped vesicles composed of one or more phospholipid bilayers. They are nontoxic and biodegradable, likely because they consist of lipids similar to biological membranes. The liposomes are capable of entrapping both hydrophilic and lipophilic molecules in aqueous core or lipid layers due to their amphiphilic structure. Liposomes might have a positive, negative, or neutral charge on their surface reckon with their structure. Surface charge is a critical feature that contributes to liposome stability by affecting the aggregation and fusion of liposomes throughout storage period. Positively charged liposomes appear to be essential when considered the corneal epithelium's thin coating of mucin that is negatively charged.125,126
In a study, siRNA-loaded liposomes were developed for use in treatment of Acanthameba keratitis that has no specific treatment. Liposomes designed using DOTAP:DOPE:DSPE-PEG by nanoprecipitation with solvent displacement, by film hydration with high-pressure homogenization, and by film hydration with membrane extrusion methods. Among these production methods, the membrane extrusion method was found to be suitable, and liposomes with a particle size of 225 ± 13 nm and a zeta potential of +44.5 ± 3.5 mV were obtained. Also no significant ocular irritation was observed. 127
Although liposomes seem to be suitable systems for the administration of ocular drugs, they have some problems such as lack of scalability potential due to their low stability, very high production cost, and drug leakage during storage. 128 For this reason, it does not seem possible to replace conventional drugs in the short term without eliminating these problems.
Niosomes
Niosomes are bilayered structures that are composed of biodegradable, nonionic surfactant vesicles. Similar to liposomes, they contain 2 layers of surfactant. They have the ability to entrap both lipophilic and hydrophilic molecules, and they are chemically more robust than liposomes. In addition, they cause less toxicity due to their nonionic structure. 7 However, their main limitations are leaching of encapsulated drug and inefficient drug loading. 128
In a study, El-Nabarawi et al. developed natamycin-loaded niosomes by reverse-phase evaporation technique and incorporated them into ketorolac tromethamine gel formulations that were prepared with different mucoadhesive polymers (sodium carboxymethyl cellulose and hydroxypropyl methylcellulose) for fungal keratitis. Designed niosomes had between 181.75 and 498.95 nm particle size, −52.90 to −73.75 mV zeta potential, 90.99%–96.43% entrapment efficiency, and 14.68%–14.75% drug loading. Compared with marketed products, designed formulations demonstrated prolonged in vitro release up to 24 h. Also, formulations exhibited greater corneal infiltration, ocular bioavailability, and hypopyon level in rabbit corneas. 129
Cubosomes
Cubosomes, also known as liquid crystalline nanoparticles, resemble the cubic structure produced by the self-assembly of certain surfactants such as monoglyceride glycerol monoolein (MO). MO is a nontoxic, biodegradable, and biocompatible surfactant frequently utilized to generate cubosomes. Cubic phases provide several advantages, including the capacity to dissolve lipophobic, lipophilic, and amphiphilic compounds; easier biodegradation; and sustained drug release. Also, it is highly bioadhesive and is believed to increase skin penetration. 130 Also, in cubosomes, the loading capacity of hydrophilic drugs is higher than that of hydrophilic drugs. 128
In a study, sertaconazole nitrate-loaded cubosome formulation was designed against fungal keratitis. Optimal formulation had 216.55 ± 2.33 nm particle size and 34.00 ± 6.93 mV zeta potential. Also, it showed better mucoadhesive characteristics, longer storage stability, and enhanced corneal permeability with no ocular irritation in rabbits. 131
In another study by Nasr et al., cubosome formulations containing fluconazole with 48.17 ± 0.65 nm particle size, −31.90 ± 0.56 zeta potential, and 85.70 ± 2.56 entrapment efficiency were developed. It exhibited enhanced permeability (slightly >2-fold) through rabbit cornea compared with the solution of fluconazole. Besides, it showed a better antifungal efficacy and safety profile in rats than fluconazole solution. 132
Dendrimers
Dendrimers are nanosized structures that resemble trees. Due to nanoscale sizes and low particle size dispersity, this delivery system is suitable for the ocular administration. Their spherical structure consists of 3 parts: core, branches, and terminal groups. The inner part, the core, is the center of the structure, and could be an atom or molecule. The branches are covalently linked, and a considerable number of branching sites are gathered in several substantially concentric layers termed generation.
The terminal groups, the outer parts, are functional agents placed on the dendrimer's surface. 133 Dendrimers have a hydrophobic characteristic. New-generation dendrimers are cationic charged and may be hazardous when used for ocular administration. The old generation of dendrimers is anionic or neutral charged, and more biocompatible for ocular delivery. 1 However, dendrimers involve multiple steps while producing, and the chemicals used during these production steps may cause cytotoxicity.
In a study, chlorhexidine digluconate combinations with ammonium or guanidine carbosilane dendrimers had developed to treat acanthameba keratitis. In vitro results showed that developed formulations have a synergistic impact against Acanthameba polyphaga and significantly reduced the minimal trophozoite concentration. Furthermore, some formulations showed meaningful activity against cyst resistance. 134
In situ forming hydrogels
Natural or synthetic polymers could absorb enormous quantities of water and form 3-dimensional crosslinked gels, which are specifically called hydrogels. The significantly high viscosity of the hydrogel prevents it from being removed more easily on the eye surface, which prolongs the residence time and therefore provides a longer drug release time. Hydrogels' drug release could be modified by altering their porosity or crosslinking level based on polymers used for manufacturing. Another advantage of hydrogels is preventing peptide-based drugs from enzymatic degradation. 135 Although natural polymers are harmless and biodegradable, they have lower physical strength, greater variability, and higher immunogenicity.
On the contrary, synthetic polymers have superior reproducibility, changeable mechanical features, and longer stability, though they may not be biocompatible and biodegradable. 136 In situ hydrogels facilitate liquid or preformed gel application, depending on their gelation feature. In situ gelation could be succeeded through temperature, pH, or ion changes related to its composition. In situ gel also has the disadvantages of being more susceptible to stability problems resulting in chemical degradation and requiring a high level of liquid, which leads to deterioration during storage. 137
A study was conducted to evaluate the effectiveness of gatifloxacin-loaded, ion-sensitive hydrogel systems prepared by sodium alginate or gellan, and their combinations with sodium carboxymethylcellulose to treat experimental bacterial keratitis in rabbit eyes. Developed hydrogel systems showed longer precorneal durations and improved ocular bioavailability than marketed solutions due to their nonirritating higher mucoadhesive character. 138
In a study by Díaz-Tomé et al., econazole nitrate-loaded ion-activated hydrogels and hyaluronic acid hydrogel systems were developed to treat fungal keratitis. Various cyclodextrins were used to make inclusion complex to increase econazole's solubility, demonstrating that α-cyclodextrin was most efficient. Although both hydrogels showed controlled release, it was found that both did not show ocular irritation in the hen's egg test. According to ex vivo studies, econazole has similar corneal permeability from both inclusion complex solution and hydrogels. Although, positron emission tomography exhibited that hydrogels have higher residence time on the eye surface. 139
In another study, Mohammed et al. developed a moxifloxacin-loaded or gentamicin-loaded in situ chitosan/β-glycerolphosphate hydrogel to treat microbial keratitis. It was stated that developed formulations showed no cytotoxicity on the fibroblast cells and exhibited sustained release. Furthermore, any bacterial colony development was not observed along with hydrogel implementation. 140
In another study by Soliman et al., fluconazole-loaded niosomal gel (117.13 ± 8.85 nm particle size and −45.37 ± 5.15 mV zeta potential) and ME (59.93 ± 2.00 nm particle size and −31.90 ± 0.99 mV zeta potential) formulations were designed for fungal keratitis treatment. While all formulations provided over 12 h of release, this release time was further increased in niosomal gel formulations. Also, niosomal gels demonstrated ∼2-fold greater ocular bioavailability than ME in rabbits. 141
Ocular inserts
Ocular inserts are sterile formulations with a solid or semisolid composition, which have been specifically sized and shaped for ophthalmic use. Inserts are generally put in the lower fornix but may also be put in the upper fornix or cornea. 142 Ophthalmic inserts may provide many benefits, including extended ocular residence, greater bioavailability contrary to other standard vehicles, possible sustained release, decreased systemic absorption, reduced dose frequency, enhanced patient compliance, omitting preservatives, escalated shelf life, and opportunity of targeting internal ocular tissues. Because ocular inserts are rigid, they can cause eye irritation and adversely affect vision. At the same time, the application of some devices and attachments to the eye can be quite challenging. 143
In a study by Ustundag-Okur et al., ofloxacin-loaded nanostructured lipid carriers (NLC)-based ocular insert formulations were developed for bacterial keratitis treatment. NLC was developed by the high-shear homogenization method, and inserts were designed with the solvent casting evaporation method. Ocular residence time was extended up to 24 h, and cmax was ∼6-fold of commercial product. Bacterial keratitis-infected rabbits recovered in 7 days without any major side effect and corneal opacity. 144
Besifloxacin HCl or besifloxacin HCl-hydroxypropyl-beta-cyclodextrin (HP-β-CD) complex containing poly(caprolactone)/polyethylene glycol fibrous inserts were designed through electrospinning method by our research group. The fibrous inserts were covered with sodium alginate or thiolated sodium alginate (TSA), and bioadhesive characteristics of formulations were increased (Table 4).
Characteristics of Insert Formulations A–D′
+, present; −, absent.
HP-β-Cyc, hydroxypropylbeta-cyclodextrin; PCL, poly(ɛ-caprolactone).
In vitro release studies exhibited that insert formulations had a burst release in the first 2 days ensued by controlled release. All of the insert formulations had ≥93% encapsulation efficiency. Formulation C (TSA coated) and Formulation D (HP-β-CD complex containing insert formulations) were chosen for use in in vivo studies because of their high efficiency in bioadhesion and ex vivo studies. Developed Formulation C or Formulation D efficiently ameliorated bacterial keratitis in rabbits after single-dose administration compared with marketed product (Fig. 2). 145

Clinical examinations of rabbit eyes at 1, 3, 5, and 7 days postinfection, respectively.
Terreni et al. have developed synthetic antimicrobial peptide (hLF 1–11), loaded inserts by the freeze-drying method. As a model drug molecule, vancomycin was loaded into matrices with various polymers at different concentrations to obtain optimal formulation. Hydroxypropyl methylcellulose/trehalose/sodium hyaluronate/hLF 1–11fd contained formulation chosen due to enhanced chemical stability up to 6 months. Moreover, optimal matrix facilitated drug release in simulated biological conditions associated with an ideal hydration time, and antimicrobial impact of the peptide had maintained for up to 15 months. 146
Moxifloxacin-loaded ocular insert formulations that demonstrated the controlled release were designed by Sebastian-Morello et al. to treat corneal keratitis. All inserts were prepared using bioadhesive polymers (hydroxypropyl methylcellulose, polyvinylpyrrolidone K30, polyethylene glycol) with different ratios by solvent casting method.
Moxifloxacin solution showed no significant difference between frozen (−20°C and −80°C) rabbit corneas for accumulation of moxifloxacin. However, the difference between fresh and frozen corneas was significant. Also, the difference between the corneal stroma thickness of the frozen groups was not meaningful, while the difference between fresh and frozen groups was notable. Besides, no substantial differences in epithelial thickness were found among the 3 groups. Based on ex vivo results, the developed optimum insert formulation showed better permeation and greater ocular concentrations than marketed product. 147
In another study to treat fungal keratitis, voriconazole-loaded proniosomes were developed by the coacervation phase separation method. These niosomes were incorporated into inserts by film casting method that utilizes polymers, hydroxypropyl methylcellulose, and carbopol 940. The optimum niosomes formulations had an entrapment efficiency of 87.4% ± 2.55%, particle size of 209.7 ± 8.13 nm, and zeta potential of −33.5 ± 1.85 mV. The niosomal voriconazole-loaded ocular insert formulation exhibited biphasic drug release for 8 h; while rapid release occurred in the first half hour due to the burst effect, controlled drug release was achieved in the remaining time. Designed insert formulation at a concentration of 1% w/w showed superior antifungal activity to marketed product. 148
Contact lenses
Contact lenses are mainly comprised of hydrogel substances and provide prolonged contact with the cornea without any adverse effect on eyesight. As a result of broad usage of contact lenses by individuals, their biocompatibility and usage safety have been thoroughly studied. Following these advantages, a significant number of studies have been conducted on contact lenses for delivering antimicrobial drugs into the eye. Researchers have investigated various ways to do this, such as soaking traditional contact lenses in drug solution, merging 2 hydrogel lenses to form a drug reservoir, surface functionalization, and embedding the substance into the contact lens.149,150 Preclinical developments of contact lenses formulations targeting keratitis are summarized in Table 5.
Some of the In Vitro and In Vivo Application Studies of Contact Lenses Ocular Drug Delivery Systems for Keratitis Disease
ACV, acyclovir; CHX, chlorhexidine; CLs, contact lenses; D, 10−7 cm2/s; DXM, dexamethasone; GFL, gatifloxacin; GO, graphene oxide; HEMA, 2-hydroxyethyl methacrylate; HTCC, quaternized chitosan; kD, 10−7 cm2/s; LVF, levofloxacin; MAA, methacrylic acid; MF, moxifloxacin; MS, mucoadhesive strength; OFL, ofloxacin; PLA, poly(lactic acid); PLGA, poly(lactic-co-glycolic acid); SI, swelling index; T, transmittance; VACV, valacyclovir; Vit E, vitamin E.
Traditionally, the straightforward technique of immersing commercial contact lenses in a drug solution has been regarded to have a minimal effect due to the quick release of the drug from these drug-immersed lenses.
Molecular imprinting is a relatively new technique for producing sustained therapeutic delivery through contact lenses. This approach employs a prepolymer combination of hydrogels and one or more monomers to interact with the given drug. The polymerization reaction is subsequently begun, resulting in the formation of the hydrogel surrounding the therapeutic agent. The kind and proportion of monomer units in the polymeric matrix could be changed to customize the drug release pattern. Nevertheless, after a specific concentration, increased crosslinking might have a detrimental effect on the hydrogel's clarity, water capacity, and oxygen transport, rendering the molecularly imprinted lens insufficient for in vivo usage. 150
Although contact lenses have many advantages over eye drops, they have drawbacks such as potential safety risks, low patient compliance, and manufacturing difficulties. In addition to these, attention should be paid to the changes in oxygen permeability and optical properties that may occur during production. 151
In a study, a contact lens formulation loaded with oriconazole and diclofenac was produced to be used in the treatment of acanthameba keratitis. Acuvue TruEye, a commercial contact lens, was used to manufacture the formulation. In this context, Acuvue TruEye contact lenses were first dipped in deionized water and then dried at 60°C, thereby removing moisture from the surface. Then, these dry contact lenses were placed in 10 mL of 1% voriconazole solution or 1% voriconazole and 0.5% diclofenac solution, and they were both rehydrated and saturated with the drug solution.
After 1 day, the contact lenses were removed from the solutions and dried. With these drug-loaded contact lenses, extended drug release was provided to the cornea (∼6 h), and the release values obtained during this period were found to be above the minimum inhibitory concentration value of Acanthameba castellanii. In the MTT analysis, it was determined that the system did not show any toxic effects, and also showed reasonable cell proliferation and repopulation at the drug doses used in the in vitro scratch wound study. 152
Microneedles
MNs are polymeric or metallic devices with a size ranging between a few micrometers and 200 μm. MNs have microdimensional structures that make them minimally invasive. Not only are these MNs capable of overcoming the limitations associated with currently utilized traditional drug delivery methods, but they also have the ability to penetrate ocular barriers, allowing medicines to be selectively targeted at the desired location.162–164
In a study, Roy et al. designed free or liposomal amphotericin B-loaded MNs to treat fungal keratitis. Liposomes containing amphotericin B were produced using the thin-film hydration technique. MNs were fabricated utilizing a soluble polymeric matrix containing polyvinyl alcohol and polyvinyl pyrrolidone. Ex vivo corneal permeation tests indicated that MNs' usage substantially increases amphotericin B corneal penetration compared with nonapplication of MNs. Designed MNs formulation quickly dissolved after the 5 min of administration in the ocular surface. Amphotericin B-loaded MNs exhibited efficiency in suppressing infection in both ex vivo and in vivo rabbit models.
Also, it was observed that amphotericin B-loaded MNs formulation ameliorated infection-related epithelial and stromal changes. However, rabbit model's results interestingly showed that liposomal amphotericin B-loaded MNs were less efficient than free amphotericin B-loaded MNs. 165
In another study, Lee et al. had fabricated a hybrid device with a drug-loaded biodegradable tip and a supportive base. This biodegradable MN has a 150 μm length that could be applied into cornea for sustained drug release, allowing long-acting and less invasive ocular drug delivery. Polyhexamethylene biguanide-loaded MN was utilized to ascertain in vivo therapeutic applicability in the mouse eye model with acanthameba keratitis. In vitro studies revealed that 93% of the drug was released within 4 days; the remaining drug was released for ∼9 days. MNs loaded with polyhexamethylene biguanide demonstrated their safety, and decreased keratitis progression by a single application. 166
Carbon quantum dots
CQDs can be defined as small-sized (typically <10 nm) nanomaterials, which have different surface passivation with optical characteristics and photocatalytic capabilities, similar to semiconductor-based quantum dots. Some CQDs display superior water solubility, excessive fluorescence, robust photostability, and minimal cytotoxicity. 167 These advantageous properties enable CQDs to be frequently used in sensor and medicinal applications, such as fluorescence sensing, cellular image analysis, drug targeting, and antibacterial therapeutics. 168 However, it has been observed that in vivo applications have cytotoxic effects of quantum dots, and stability problems occur due to interaction with proteins at the application site. 169
In a study, CQDs of biogenic spermine and dopamine mixture were prepared by a simple heating method. CQDs of spermine and dopamine mixture's antimicrobial activity was 17- and 7-fold higher than only spermine and only dopamine contains CQDs, respectively. Prepared CQDs displayed superior biocompatibility as demonstrated by in vitro cytotoxicity results, hemolysis tests, and in vivo study. Furthermore, outcomes exhibited that CQDs containing a mixture of spermine and dopamine could restrain the development of bacterial keratitis in a rabbit model. 170
Iontophoresis
An electrical field is created at the ocular surface with a slight current, crossing through to posterior segments in the ocular iontophoresis method. The movement of charged particles is facilitated by the effect of this electric field. Ionic drug molecules or drug delivery systems that are placed into this field may ensure much higher ocular drug concentrations than those that would be obtained by using conventional eye drops. 171
In a study, 3 different voriconazole formulations (cyclodextrin inclusion complex, liposome, and chitosan-coated liposome) were designed to treat fungal keratitis, and the iontophoresis method was utilized for increasing their corneal permeability. Liposome and chitosan-coated liposome formulations had ∼134.6 ± 1.7 and 139.2 ± 1.3 nm particle size, −8.2 ± 3.0 and +3.3 ± 1.5 mV zeta potential, respectively. Drug inclusion complex and both liposomal formulations were stable under the electrical field of iontophoresis. Ex vivo studies showed that the iontophoresis application increased corneal retention and penetration of voriconazole for all formulations (45.4 ± 11.2, 30.4 ± 2.1, and 30.6 ± 2.9 μg/cm2 for cyclodextrin inclusion complex, liposome, and chitosan-coated liposome, respectively). 172
Discussion
The therapeutic doses of conventional drug drops used in the treatment of bacterial keratitis are high and require frequent use. This is due to the unique anatomy and physiology of the eye. The eye protects itself from external effects owing to its protective structures, but this unique protective structure also makes it difficult to treat diseases. Especially the tear, corneal barriers, and conjunctival barriers are the 3 structures that make the treatment of diseases to occur in the anterior part the most challenging. These protective structures in the eye reduce the ocular bioavailability of eye drops to <5%. Due to this low ocular bioavailability, eye drops are produced in high doses and used with frequent application to achieve the desired efficacy.
Thanks to the novel drug delivery systems that were produced by considering the barriers of the eye, the removal of the active substances on the eye surface with tears has been prevented, and their residence time on the eye surface has been substantially increased (especially solid systems such as inserts and colloidal systems prepared with positively charged polymers and surfactants have much higher adherence). At the same time, it has been determined that the corneal and conjunctival permeation of these systems are more than conventional systems. In addition, the burst effect of the new drug delivery systems, as a result of the rapid release of the active substance in high doses, enabled the rapid onset of the effect and the continuation of these effects with the controlled release that followed.
Ocular bioavailability of active substances has been increased with the new drug delivery systems, and efficiency has been ensured by producing at lower doses compared with conventional systems. In a study by Ustundag-Okur et al., 144 they applied the inserts they had developed (containing 0.3% ofloxacin) once a day and the commercial preparation (containing 0.3% ofloxacin) twice a day to rabbits. At the end of the seventh day, they determined that the amount of ofloxacin passed into the aqueous fluid from the ocular inserts they prepared increased by 6 times that of the commercial preparation. They also determined that the ocular insert reduced corneal opacity by 20 times.
In another study, Shi et al. 160 compared gatifloxacin-loaded contact lenses (∼11 μg drug loaded) with the market preparation (0.3% gatifloxacin containing) in an in vivo experiment. They found that rats with contact lenses were almost healed (corneal abscess was healed) at the end of the 48th hour, and the market preparation did not show the same effect in the same time period. In another study, Mahmoud et al. 107 produced chitosan nanoparticles loaded with euconazole. When the results of the in vivo rabbit study were examined, it was determined that the antifungal activity of the nanoparticles on the eye surface was >8 h, while the solution form showed activity for 4 h. In addition, it was determined that the activities of the nanoparticles during this time were much higher than those in the solution form.
However, nanodrug carriers must overcome many challenges to reach clinical trials. The biggest hurdle in the production of nanodrug carriers is large-scale production following Good Manufacturing Practice standards and quality control experiments for the characterization of these systems. The marketed product must be within acceptable limits for safety, efficacy, stability, and patient acceptance. At the same time, the methods used during the production of the formulation should be within certain standards, and the production specifications obtained should be reproducible.
Although nanodrug carriers give superior results in in vivo animal experiments, traditional eye drops are still preferred due to difficulties in determining production standards, very high R&D and production costs, and problems in reproducibility. However, advances in scale-up technology and Quality by Design concepts could pave the way for commercialization processes of nanodrug carriers and innovative drug delivery systems.
Conclusion and Future Direction
Drug delivery into the eye is still very challenging task owing to highly impervious structure of the eye. Conventional dosage forms such as solutions, suspensions, and ointments cannot provide optimal therapy due to new diseases and antibiotic resistances occurring today. Depending on the diseases and drug molecules used in treatment, different drug delivery approaches are being tried, and their superiority over conventional systems has been demonstrated in many publications.
In the treatment of keratitis, the pathogen causing keratitis is of great importance, and it is vital to use the appropriate formulation and treatment method to prevent antibiotic resistance, especially in bacterial keratitis. When the literature is examined, it has been observed that formulations developed for fungal keratitis are generally lipid based due to the low water solubility of antifungal drugs. In the treatment of bacterial keratitis, it has been observed that fluoroquinolone antibiotics have been studied quite frequently. Therefore, trying different and new antibiotics may create new opportunities for keratitis treatment.
When in vivo models were evaluated, it was observed that the treatment time of keratitis was reduced with the addition of corneal permeability enhancer agents such as cyclodextrin to the formulations or application of corneal permeability enhancer methods such as iontophoresis. Also, the use of contact lenses increases the treatment efficiency by prolonging the contact time of formulation with the cornea.
Within the scope of this review, different formulation approaches developed against keratitis diseases have been shown to have encouraging results based on in vitro and in vivo studies. However, for these systems to be used in treatment instead of conventional systems, their efficiency should be increased while their costs are reduced. Also, their efficacy needs to be proven with large-scale clinical studies.
Footnotes
Authors' Contributions
H.K.P., N.K., E.A., S.B.P., and S.C. approved the idea/concept and design. S.B.P. contributed to supervision/consultancy. H.K.P., N.K., and E.A. contributed to data collection, and/or processing and writing of the article. S.B.P., S.C., and E.A. performed analysis and/or comment. H.K.P. and N.K. performed source scan. S.Ç. and S.B.P. contributed to critical review and resources and funding.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.