
Abstract
Purpose:
To identify 24-h changes in ocular biometric parameters in subjects with ocular hypertension (OHT), and to determine if an intraocular pressure (IOP)-lowering drug alters these parameters.
Methods:
Thirty volunteers with OHT (58.6 ± 9.2 years of age) were enrolled in this randomized, double-masked, placebo-controlled, crossover study. Participants self-administered 0.2% brimonidine or placebo 3 times daily for 6 weeks. Measurements of seated and supine IOP, central cornea thickness (CCT), anterior chamber depth (ACD), axial length (AXL), and lens thickness were made at 8 am, 3 pm, 8 pm, and 3 am. Statistical tests were Student's 2-tailed paired t-tests or 2-way analysis of variance (ANOVA) followed by one-way ANOVA and post hoc testing.
Results:
Time of day had a significant effect on IOP, CCT, ACD, and AXL. In placebo-treated eyes, CCT was greater at 3 am than at any other time (P < 0.01), ACD and AXL were greater at 3 am and 8 pm than at 3 pm (P < 0.01). Daytime IOPs were higher than nighttime (seated, P = 0.007; supine, P = 0.018), and supine IOP at night was higher than seated IOP during the day (P < 0.001). Brimonidine did not lower IOP at night nor did it alter the 24-h patterns of CCT, ACD, and AXL.
Conclusions:
Ocular biometric parameters exhibit characteristic 24-h fluctuations in patients with OHT. At night compared with day, the supine IOP increases, the cornea thickens, the anterior chamber deepens, and the AXL increases. Brimonidine does not alter these parameters at times when it lowers IOP (day) nor when it does not (night). Clinical Trial Registration number: NCT0132419.
Introduction
Accurate biometric measurements are vital to the algorithms and formulas used in cataract and refractive surgery to achieve precise outcomes. 1 Diurnal variation in biometric parameters can be a source of error in measurements of the same. It has been established that diurnal variations occur in central cornea thickness (CCT).2,3 Diurnal variations in axial length (AXL) and anterior chamber depth (ACD) are less well characterized and the mechanisms underlying these changes, if any, are not well known.4,5 This exploratory study of the diurnal variability of these parameters attempts to quantify these changes. If the variability is found to be significant, such data may be helpful in presurgical discussions with the patient as to how much variability can be expected in their refractive outcomes based on physiological diurnal variations in ocular biometrics alone.
The intraocular pressure (IOP) with its own well-documented 24-h rhythm6,7 is a potential candidate mediator for these changes in biometric parameters. 8 An evaluation of the correlation between IOP and biometric changes during a 24-h period can help confirm or refute its role as a mediator. With IOP as a potential mediator for diurnal biometric changes, it is of further interest to study how these changes are affected by ocular hypotensive medications in ocular hypertensive patients. Patient complaints of blurry or fluctuating vision with ocular hypotensive drops may be owing to the secondary effect of these drugs on ocular biometrics and thereby the patient's refractive error. 9
This study describes changes in IOP and ocular biometric parameters during the day and night in subjects with ocular hypertension (OHT). The study also examines whether these changes differ in subjects with IOPs lowered by an ocular hypotensive medication viz. brimonidine 0.2%. Finally, the study evaluates the possibility of a direct causal relationship between diurnal IOP variation and changes in these biometric parameters.
Methods
This study is ancillary to a study evaluating the daytime and nighttime changes in aqueous humor dynamics in subjects using brimonidine 0.2% three times daily at ∼8 am, 2 pm, and 8 pm. 10 Thirty patients (58.6 ± 9.2 years of age, mean ± standard deviation) with a diagnosis of OHT (IOP ≥21 mmHg on 2 separate occasions) were enrolled in the study. One patient was withdrawn before the study finished because the IOP increased to 35 mmHg during the placebo treatment phase (as determined after unmasking). This single-center study was approved by the University of Nebraska Medical Center Institutional Review Board and informed consent was obtained from all participants before enrollment. After a screening visit to determine eligibility and obtain consent, participants were scheduled for 2 daytime and 2 nighttime study visits.
Visits and dosing
The screening visit included a medical and ophthalmic history, visual acuity measurement, a slit lamp examination, gonioscopy, tonometry, and a dilated fundus examination. Exclusion criteria were history of glaucoma, history of intraocular inflammation, current (or within 3 months) use of topical or systemic steroid, previous ocular surgeries, anterior chamber angle Schaffer grade 2 or less for 180 degrees or more on gonioscopy, 11 a cup-to-disc ratio >0.8, or IOP >35 mmHg at any time during the study.
The study had a double-masked, placebo-controlled, randomized, crossover design, with 2 daytime and 2 nighttime visits. Six weeks before study visit 1, subjects stopped using their prescribed IOP lowering medication, if any, and started self-administering study drops of 0.2% brimonidine (Allergan, Inc., Irvine, CA) or placebo to both eyes (Artificial Tears; Alcon, Fort Worth, TX) 3 times daily. They returned for visit 1 (daytime visit). Dosing continued until the evening of visit 2 (nighttime visit 2 days later). At the completion of visit 2 the subjects switched to the alternate drops (brimonidine or placebo) for another 6 weeks, at which time patients returned for visit 3 (second daytime visit). Dosing continued for 2 more days until the evening of visit 4 (second nighttime visit). It was assumed that the effect of the first treatment was gone and the effect of the second treatment was maximal at 6 weeks. 12 If the treating physicians had any concerns about significant IOP elevation during the study (based on history and current IOP targets), safety visits were included at weeks 1–4 after the initiation of each study treatment to monitor IOP.
Measurements
At each daytime visit (visits 1 and 3), after administration of one drop of 0.5% proparacaine (Akorn, Inc., Lake Forest, IL), CCT was measured by ultrasound pachymetry, and ACD, AXL, and lens thickness (LT) by A-Scan ultrasonography (Pacscan Series 300; Sonomed, Lake Success, NY) at 8 am and 3 pm (Table 1). A pneumatonometer (Model 30 Classic; Ametek, Inc., Berwyn, PA) was used to measure IOP at 9 am, 11 am, 1 pm, and 3 pm with the participants in the seated position and then 5 min after changing to the supine position. At each body position, 2 measurements were taken in quick succession and averaged. If the difference between duplicate measurements was >2 mmHg, a third measurement was taken. In this case, the median value was used for the analysis. Two days later the participants returned for the nighttime measurements (visits 2 and 4). These measurements were carried out in a 2-room suite of a hospital-based hotel on campus. At 8 pm and 3 am CCT, ACD, AXL, and LT were measured in the seated position.
Study Schedules and Procedures
Times are approximate.
ACD, anterior chamber depth; AXL, axial length; CCT, central cornea thickness; IOP, intraocular pressure; LT, lens thickness.
The IOP was measured at 9 pm, 11 pm, 1 am, and 3 am in the dimly lit hotel room with the patients in a supine position and then at least 5 min after rising to a seated position. The light in the room was kept as dim as possible while still allowing the investigator to see the instruments and safely collect the measurements. It has been reported that a short period of light exposure at night does not affect IOP, 13 therefore, the room light intensity was not measured during this study. This light setting was consistent throughout this study and a previous study. 10 The mean daytime IOP is the average of 9 am, 11 am, 1 pm, and 3 pm measurements and the mean nighttime IOP is the average of 9 pm, 11 pm, 1 am, and 3 am measurements. Participants were instructed to return to sleep between readings. Vitreous chamber length (VL) was calculated by subtracting CCT, ACD, and LT from the AXL.
Statistical analyses
Both eyes of each participant were included in the data analysis unless one eye did not meet eligibility criteria. In one subject, only one eye was included in the analysis. The fellow eye experienced irritation after the first 2 measurements; thus further measurements were stopped. Data are presented as mean ± standard deviation. Student's 2-tailed paired t-tests were used to compare daytime versus nighttime IOPs in the seated position, daytime versus nighttime IOPs in the supine position, and daytime seated versus nighttime supine IOPs (habitual positions). Two-way analysis of variance (ANOVA) and one-way repeat-measures ANOVA followed by Tukey post hoc test where appropriate were used to compare CCT, ACD, AXL, and LT during the day on treatment with brimonidine or placebo.
Association between IOP and biometric parameters was evaluated using linear mixed-effects models. For the linear mixed models, biometric parameter was the outcome measure and IOP was entered as a covariate. In 2 candidate models, each subject or eye was allowed to have his own random intercept for the association. The model with better fit, as indicated by lower value of Akaike Information Criteria, was selected as the final model. P values <0.05 were considered statistically significant.
Results
Twenty-nine patients completed all study visits (Table 2). One patient completed one daytime and one nighttime visit and then withdrew when IOPs exceeded the inclusion limit. In the placebo arm, the mean daytime IOPs were higher than the mean nighttime IOPs when measured with the subject in the same body position at each measurement time (P = 0.007, seated; and P = 0.018, supine; Fig. 1). In the brimonidine-treatment arm, the seated IOPs during the day were higher than at night (P = 0.02) but the supine IOPs during the day were not different than at night (P = 0.44; Fig. 2). When considering natural body positions of seated during the day and supine at night, the habitual IOP was higher at night than day in both the placebo and brimonidine treatment arms (P < 0.0001; Figs. 1 and 2).
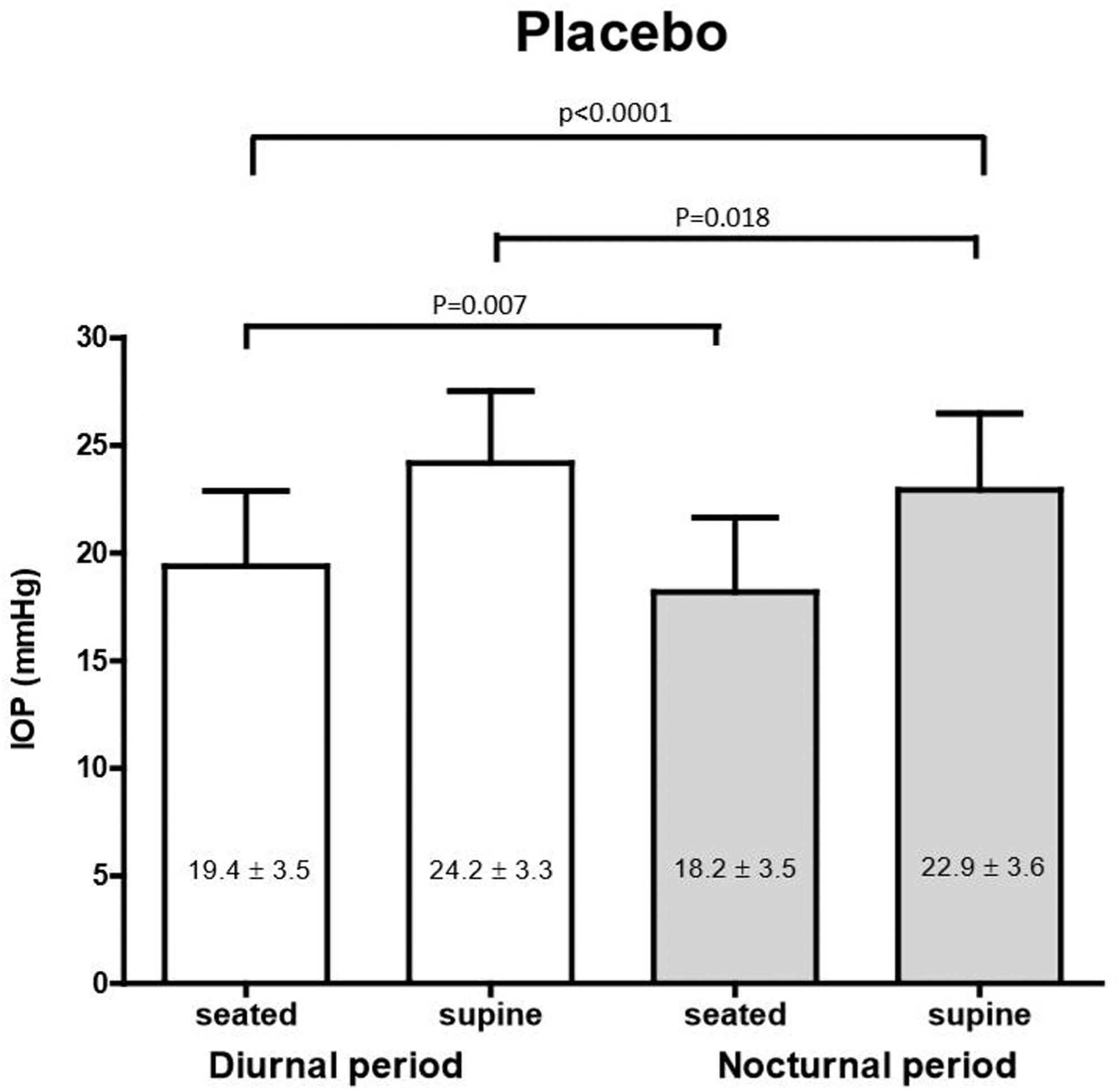
Mean IOP during the diurnal period (9 am, 11 am, 1 pm, and 3 pm), and the nocturnal period (9 pm, 11 pm, 1 am, and 3 am) of 29 patients with ocular hypertension (n = 57 eyes) who had self-administered placebo 3 times daily for 6 weeks. (P values were obtained using Student's 2-tailed paired t-tests, the T-bars represent standard deviation). IOP, intraocular pressure.
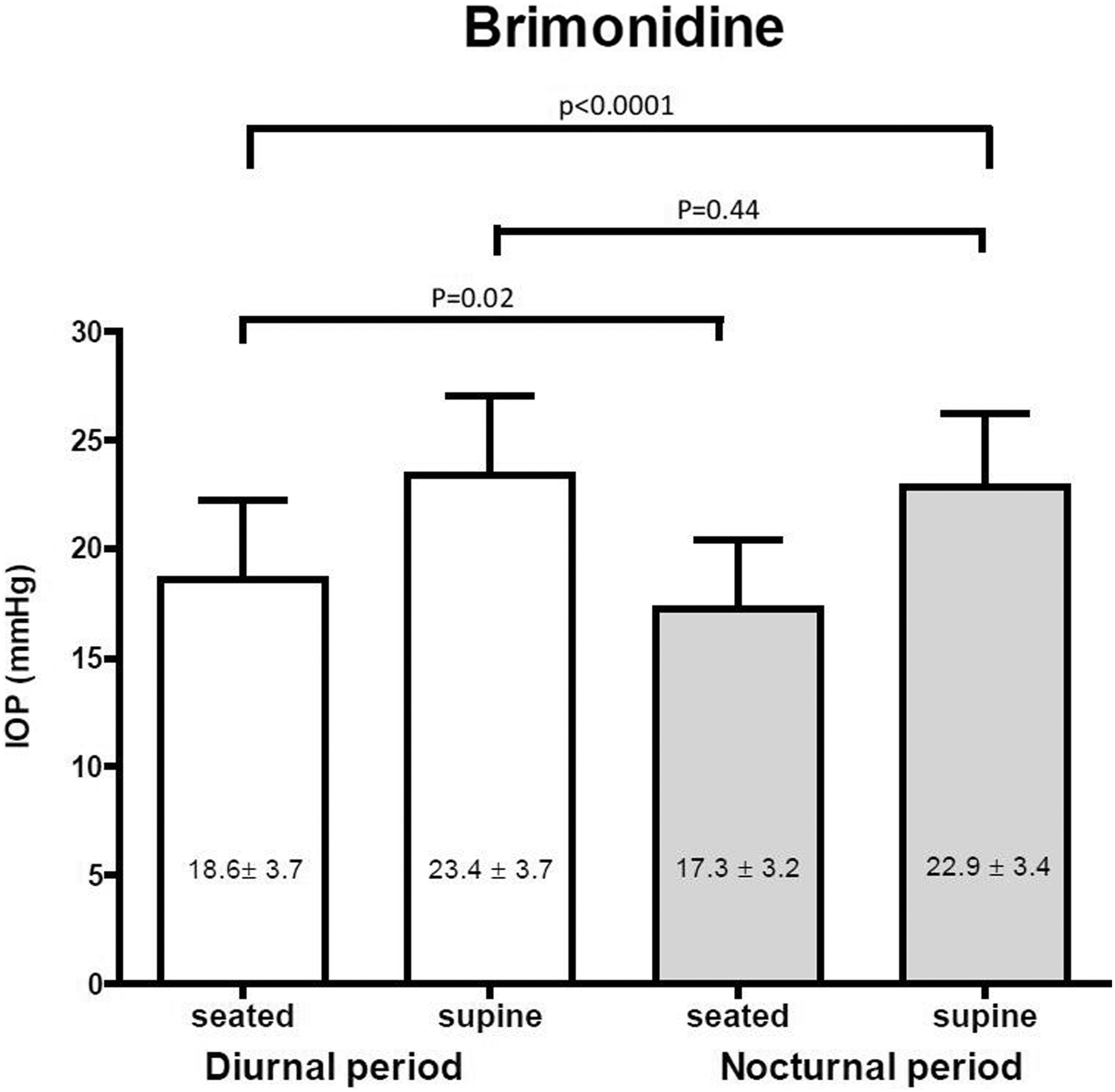
Mean IOP during the diurnal period (9 am, 11 am, 1 pm, and 3 pm), and the nocturnal period (9 pm, 11 pm, 1 am, and 3 am) of 29 patients with ocular hypertension (n = 58 eyes) who had self-administered brimonidine 3 times daily for 6 weeks. P values were obtained using Student's 2-tailed paired t-tests, the bars represent standard deviation.
Demographics
Central corneal thickness
On a 2-way ANOVA, the effect of time on CCT was statistically significant (P < 0.0001). In other words, while controlling for treatment, there was a significant change in CCT over time, that is, the average of at least 2 of the CCT time points was significantly different. The effect of treatment (placebo vs. brimonidine) on CCT was not statistically significant (P = 0.93), that is, CCT did not change at any time measured during treatment with brimonidine when compared with placebo. The interaction between time and treatment was not significant (P = 0.51), indicating that the effect of time on CCT was not affected by treatment (Table 3).
Central Corneal Thickness, Anterior Chamber Depth, Axial Length, Lens Thickness, and Intraocular Pressure Obtained During the Day and Night in Patients with Ocular Hypertension After 6 Weeks of 3 Times Daily Topical Brimonidine or Placebo
Values are given as mean ± SD.
P value obtained by 2-way ANOVA. p(time) indicates whether time affected the results. p(treat) indicates whether brimonidine affected the results. p(time*treat) indicates the interaction between time and treatment. The effect of IOP on biometrics was studied using linear mixed models, therefore those P-values (IOP on biometrics) are not included here.
On a post hoc pairwise comparison of all time points, CCT was higher at 3 am than at any of the other measurement times in both treatment arms (P < 0.01). The correlation between diurnal CCT and diurnal IOP change was evaluated using linear mixed models, with random intercepts model. The changes in CCT did not correlate with either the seated (subject in the seated position at all measurements, P = 0.45) or the habitual IOP (subject seated during the day and supine at night, P = 0.18).
Anterior chamber depth
A similar analysis evaluating the diurnal ACD variation showed that ACD was not affected by treatment (P = 0.87) but did show significant changes with time (P < 0.0001). The change with time was not affected by treatment (P = 0.76) (Table 3). On post hoc pairwise comparisons, ACD was less at 3 pm than either at 8 pm or 3 am in both treatment arms. Diurnal changes in ACD did not correlate with changes in either the seated (P = 0.72) or the habitual IOP (P = 0.74).
Axial length
AXL (P = 0.98) or its change with time (P = 0.62) were not affected by treatment. AXL did vary significantly with the time of measurement (P = 0.002; Table 3), being significantly shorter at 3 pm as compared with 8 pm in both treatment arms. Changes in AXL were not associated with changes in seated IOP (P = 0.18). However, diurnal changes in AXL were significantly associated with changes in habitual IOP (beta coefficient = 0.0036 ± 0.0016; P = 0.03).
Lens thickness
Unlike the other biometric parameters measured, LT did not differ among the different measurement times (P = 0.40) or between the 2 treatment arms (P = 0.80; Table 3). Evaluation of association between LT changes and diurnal IOP changes, did not reveal a significant association with either the seated (P = 0.98) or habitual IOP (P = 0.54).
Magnitude of changes in ocular biometric parameters in placebo group
In an analysis of diurnal change in biometric variables in the placebo group alone, changes in AXL, central corneal thickness, and ACD were statistically significant when comparing measurements at 3 am and 3 pm (Fig. 3).
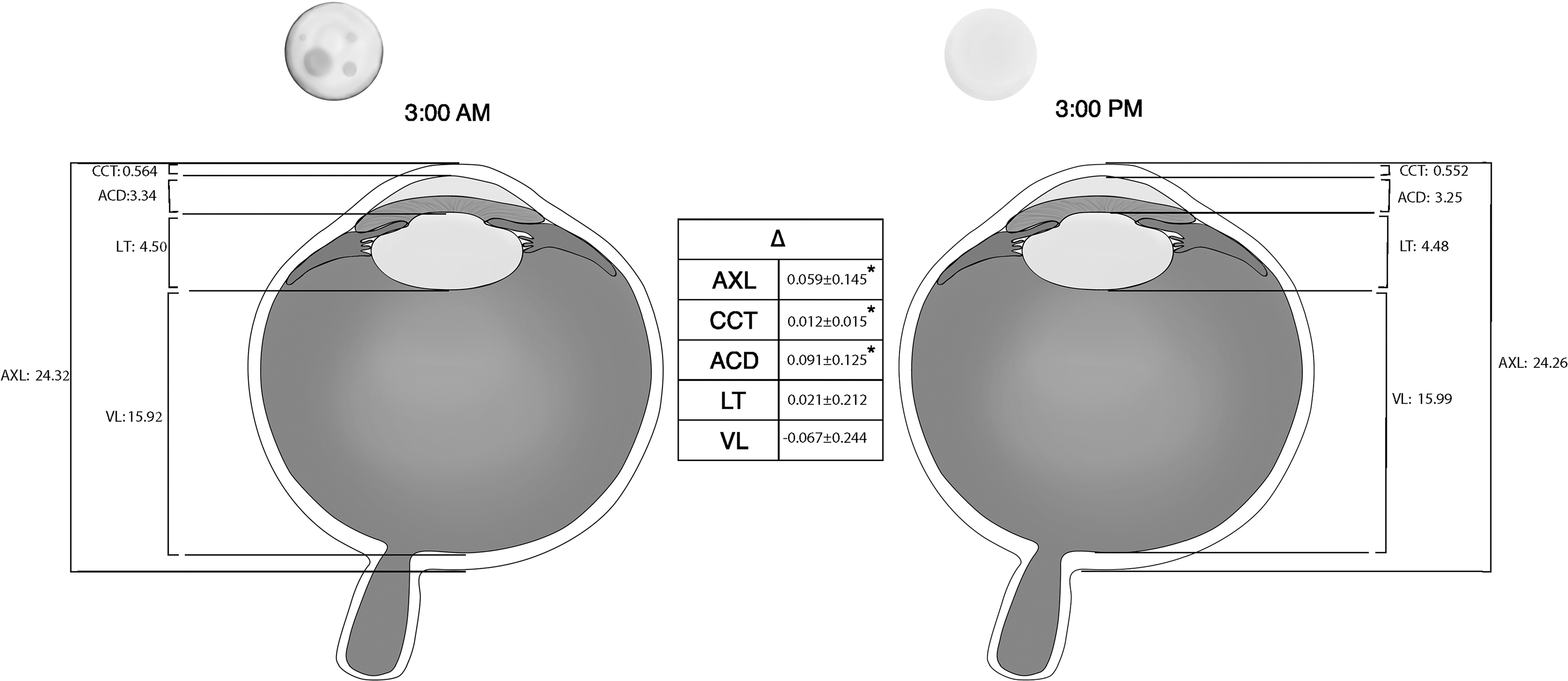
Changes in ocular biometric parameters between 3 am and 3 pm in patients with ocular hypertension who had self-administered placebo 3 times daily for 6 weeks. Values are given as mean ± SD. *Statistically significant differences between 3 am and 3 pm. AXL, axial length; CCT, central corneal thickness; ACD, anterior chamber depth; LT, lens thickness; VL, vitreous length. Permission was obtained from Cody McCalla who drew the figure.
Discussion
This study found numerous changes in IOP and ocular biometrics (CCT, ACD, and AXL) in a 24-h period. Other studies are also comparable in these parameters,2,8,14,15 as well as retinal 16 and choroidal thickness. 17 These patterns have been found in numerous animal models,18,19 and humans.15,20 Some of these diurnal changes could be endogenous, perhaps circadian, in some species.7,21 Several factors have diurnal rhythms that could impact ocular biometrics such as circadian clock genes, 22 sympathetic nerve activity, 23 fluctuating concentrations of melatonin, 24 norepinephrine, 25 and IOP itself.
This study differed from other studies in 2 main ways. Compared with other studies, it measured the ocular biometric parameters more times throughout the day and night, and it tested the effects of reducing IOP on these parameters. In this study, brimonidine lowered IOP during the day and into the evening but did not change the 24-h patterns of CCT, ACD AXL, and LT. Other ocular hypotensive drugs with greater effects on IOP over a 24-h period might have found more significant changes.
Brimonidine was chosen as the IOP-lowering drug in this study for 3 reasons. (1) It was expected that brimonidine would lower IOP during the day and at night because of its mechanism of action. It improves uveoscleral outflow during the day10,26 and like latanoprost, 27 it was expected to increase uveoscleral outflow and lower IOP during the night. (2) Detailed analyses of 24-h brimonidine changes had not been carried out before, which would add new information to the literature. It would allow comparisons of the nighttime effects of this class of drug (alpha2 adrenergic agonist) with published findings 27 from other classes of IOP-lowering drugs (prostaglandin analogs, carbonic anhydrase inhibitors, beta blockers). (3) The actions of brimonidine could block sympathetic nerve activity and potentially modify the 24-h fluctuations in ocular biometrics.
Reported changes in AXL throughout 24 h are not consistent in the literature. One study 20 of young healthy adults (18–24 years of age) and another 28 of volunteers with a wide age range (7 and 53 years) reported that IOP played a minor role, if any, in generating AXL fluctuations. However, a later study 15 of healthy adults (20–27 years of age) reported a significant association between the change in IOP and the change in AXL. This study found fluctuations in both AXL and IOP over a 24-h period in older subjects with OHT (36–74 years of age). A previous study 10 found the time of lowest mean IOP during the day (3 pm) to coincide with the time of lowest measured values for AXL and ACD. The association observed between IOP and AXL may indicate a passive expansion of the globe in response to IOP. However, a formal robust analysis using linear mixed models found a significant association only between habitual IOP and AXL.
Even then, the magnitude of estimated change was rather small as suggested by a coefficient of 0.0036 ± 0.0016 mm/mmHg. This means that a 10 mmHg change in IOP will be expected to be associated with an increase of only 36 μm in AXL. With all other variables held constant, this will translate to a refractive change of ∼0.1 diopter and will not likely be noticed by most individuals. However, the coefficient and hence the refractive error may be higher in eyes with violated structural integrity as in those having undergone incisional or refractive surgery. This speculation will need to be confirmed by future studies involving subjects with such clinical profiles.
In the placebo arm of this study, the mean ACD was 108 μm more at 8 pm than at 3 pm. Average AXL was 75 μm higher when comparing the same times in the same treatment arm. A slight backward movement of the natural lens (of ∼33 μm) will be required to reconcile the fact that the increase in ACD was in excess of the increase in AXL. A posterior movement of the lens (theoretical hyperopic shift) likely will have a compensatory effect on any increase in AXL (theoretical myopic shift) to minimize any variation in the refractive error. These interpretations of the data suggest that IOP changes might affect biometric parameters in such a way as to move compensatory mechanisms in a direction to counteract any significant refractive shifts.
This study is in agreement with others in that over a 24-h period IOP changes in a predictable manner in healthy humans 29 and in those with elevated IOP. 30 Change in episcleral venous pressure as a result of posture change is a likely cause. When changing from vertical to recumbent positions, body fluid is quickly redistributed causing increases in episcleral venous pressure followed rapidly by increases in IOP.31,32 Brimonidine treatment did not alter this effect. In the short term, one drop of brimonidine causes vasoconstriction, which is an explanation for its effects on aqueous flow 26 but in the longer term (6 weeks of dosing), the potential vasoconstrictor effects of brimonidine seem to be diminished as the effects on aqueous flow disappear. At the same time, effects on episcleral venous pressure are no longer measurable.
The finding that the central cornea was thicker at night than during the day agrees with previous studies.33,34 This increase in CCT during the night may be caused by numerous changes under the closed eyelid including hypoxia, increased lactate levels, and decreased osmolarity. 35 Topical administration of brimonidine has been reported to cause a reversible increase in CCT. The greatest swelling was reached within 2 days of twice-daily brimonidine 0.1% treatment and the CCT returned to near pretreatment levels after another 2 days of continued treatment. 36 This study did not find any effects of brimonidine 0.2% on CCT. The measurement was made at 6 weeks of treatment, thus any potential short-term effect would have been missed.
Significant changes in ACD were found in this study when comparing day and nighttime measurements. The anterior chamber was the deepest at night as also reported in rabbits 7 and normal healthy people. 37 The deeper anterior chamber at night could not be explained by nighttime changes in cornea or lens thickness. A thicker cornea might displace some aqueous humor and reduce rather than increase the depth and volume of the anterior chamber. Changes in the thickness of the lens also might displace aqueous humor but this did not happen as the lens did not change its nonaccommodative thickness from day to night. Others have reported a similar lack of change in lens thickness throughout a 24-h period.80
One factor that may change ACD is IOP. Mechanically, 38 pharmacologically, 39 or surgically 40 induced alterations in IOP can be associated with changes in AXL and ACD. Increased pressure expands the globe and the depth of the anterior chamber. This study demonstrated that the shortest AXL and ACD were temporally close to the lowest habitual IOP during the day, although statistically significant correlations were not found. Similar to another study, 41 this study demonstrated that brimonidine did not affect these 24-h fluctuation in ACD and AXL.
Conclusion
This study has identified numerous ocular biometric parameters that exhibit 24-h fluctuations in patients with OHT. The supine IOP at night increases compared with seated IOP during the day. Simultaneously, the cornea becomes thicker, the anterior chamber deepens, and the AXL increases, all to maintain visual acuity despite the IOP changes. Brimonidine does not alter any of these diurnal changes. A drug with greater effects on IOP during the day and night might produce different results.
Footnotes
Author Disclosure Statement
No conflicting relationship exists for any author.
Funding Information
The study was supported by AGS MAPS grant (VG); NIH K23EY023266 (VG) and an Unrestricted Departmental grant (UNMC) from Research to Prevent Blindness.