
Abstract
Purpose:
Proliferative vitreoretinopathy (PVR) is currently treated surgically. Reliable pharmaceutical options would be desirable, and numerous drugs have been proposed. This in vitro study is intended to systematically compare and determine the most promising candidates for the treatment of PVR.
Methods:
A structured literature review was conducted in the “PubMed” database to identify previously published agents proposed for medical treatment of PVR -36 substances that met the inclusion criteria. Toxicity and antiproliferative effects were evaluated on primary human retinal pigment epithelial (hRPE) using colorimetric viability assays. The seven substances with the widest therapeutic range between toxicity and no longer detectable antiproliferative effect were then validated with a bromodeoxyuridine assay and a scratch wound healing assay using primary cells derived from surgically excised human PVR membranes (hPVR).
Results:
Among 36 substances, 12 showed no effect on hRPE at all. Seventeen substances had a significant (P < 0.05) toxic effect of which nine did not have an antiproliferative effect. Fifteen substances significantly reduced hRPE proliferation (P < 0.05). The seven most promising drugs with the highest difference between toxicity and antiproliferative effects on hRPE were dasatinib, methotrexate, resveratrol, retinoic acid, simvastatin, tacrolimus, and tranilast. Whereof resveratrol, simvastatin, and tranilast additionally showed antiproliferative and dasatinib, resveratrol, and tranilast antimigratory effects on hPVR (P < 0.05).
Conclusion:
This study presents a systematic comparison of drugs that have been proposed for PVR treatment in a human disease model. Dasatinib, resveratrol, simvastatin, and tranilast seem to be promising and are well-characterized in human use.
Introduction
Proliferative vitreoretinopathy (PVR) is a serious complication of retinal detachment. Up to 10% of the patients develop PVR within a few weeks following surgical retinal reattachment.1,2 Sadly, it often leads to multiple subsequent surgical interventions, resulting in a poor visual outcome. 3 The standard treatment remains a surgical one. However, a reliable pharmacological alternative or adjuvant therapy to avoid PVR onset would be desirable. This could potentially reduce the need for repeated surgeries and might result in a better visual outcome. 4
PVR causes epi-, intra-, and subretinal membranes by a proliferation of cells that detach the retina through tractional forces. Different approaches to explain the pathological mechanism exist, but the exact one remains unclear. 4 Retinal pigment epithelial (RPE) and glial cells are proposed to play a significant role. The common approach involves excessive proliferation, migration, epithelial to mesenchymal transition, and differentiation driven by cytokines and growth factors such as transforming growth factor (TGF)-β. 5
Different cellular targets and pathways to affect PVR cells have been identified and can be used as targets that can be influenced pharmacologically. Thus far, there is currently no drug to treat PVR in clinical routine. 6 Examples of drugs are immunomodulators (tacrolimus, dexamethasone, retinoic acid), cytostatics (fluorouracil), or kinase inhibitors (ranibizumab, dasatinib, sorafenib).1,7
The necessary conditions and requirements for a drug to be applicable are currently challenging. First, the substance must affect the pathological processes, without causing significant toxicity and biocompatibility issues in other ocular tissues. 8 A sufficient concentration needs to be ensured at the location needed over a given period. 9 In addition, clinical study goals, surgical treatment, and disease classification have not yet been standardized to design comparable study endpoints. 10 Finally, there is very little evidence on direct comparisons of these substances to identify those with clinical potential.
To this end, we systematically compared and determined the most promising and biocompatible candidates. For this purpose, we used in vitro proliferation, migration, and toxicity assays to detect their efficacy in inhibiting cell growth without showing toxic effects in two PVR models—primary human RPE (hRPE) cells, as well as primary human PVR (hPVR) cells derived from surgically excised PVR membranes.
Methods
Literature search
Several potential drugs have been described to mitigate the assumed pathological bases of PVR. The database “PubMed” was used to search for the proposing articles, using the following search queries: “vitreoretinopathy, proliferative [MeSH Terms] OR (“vitreoretinopathy”[All Fields] AND “proliferative”[All Fields]) OR “proliferative vitreoretinopathy”[All Fields] OR (“proliferative”[All Fields] AND “vitreoretinopathy”[All Fields])”. The substances were then selected according to the following inclusion criteria: (1) Approval by the U.S. Food and Drug Administration or European Medicines Agency for other purposes; (2) Genotoxicity or mutagenic effects must be excluded; (3) genetic information should neither be altered nor be transferred; (4) Safe handling and use in cell culture in the laboratory is obligatory; (5) the proposed article must be written in English language.
Primary hRPE
After removal of the corneoscleral disc for transplantation purposes, 20 human donor globes of 10 eye tissue donors were provided by the cornea bank of the University Hospital Munich and processed within 72 h postmortem. Donors were aged between 51 and 78 years at the time of death. Informed consent for scientific tissue donation and approval by the institutional review board of the Ludwig Maximilian University of Munich (LMU Munich; project No. 73416) were obtained. All procedures complied with the tenets of the Declaration of Helsinki. A modified protocol was used as described previously to harvest hRPE cells. 11
In brief, for the dissociation buffer 7.8 mL phosphate-buffered saline (PBS; Biochrom GmbH, Berlin, Germany) was mixed with 16 μL 0.5 M ethylenediaminetetraacetic acid (EDTA; Invitrogen, Grand Island, NY, USA), 92 μL cystamine dihydrochloride 41 mg/mL in H2O (MilliporeSigma, Darmstadt, Germany), 80 μL 1:1000 w/v bovine serum albumin in H2O (BIOMOL GmbH, Hamburg, Germany), and 8 μL papain suspension (Worthington Biochemical Corp., Lakewood, NJ, USA). The anterior segment was removed from the globes, and subsequently, the retina together with the vitreous body was separated from the choroid with a sharp incision posterior to the ora serrata and cropped from the optic nerve. The RPE was then exposed to 1:500 PBS-EDTA at room temperature to dissolve retinal remnants. After 15 min, the solution was replaced with the dissociation buffer and left at 37°C for 23 min.
The suspended cells were obtained by centrifugation, suspended in Dulbecco's modified Eagle's medium (DMEM; Bio&SELL GmbH, Nuernberg, Germany) +20% fetal calf serum (FCS; Biochrom GmbH), plated to the cell culture plastic, and incubated for about 1 week without any disturbance. The epithelial phenotype was confirmed by immunofluorescence staining using the following reagents: Alexa Fluor 488 goat anti-mouse IgG (Invitrogen, Eugene, OR, USA), Hoechst 33342 (Invitrogen), and mouse monoclonal anti-cytokeratin peptide 8 (MilliporeSigma).
Primary hPVR cells
To obtain primary hPVR cells, a procedure already prepublished was used.12,13 Informed consent for scientific tissue donation and approval by the Institutional Review Board of the LMU Munich (project No. 47114) were obtained. All procedures followed the tenets of the Declaration of Helsinki. Membranes that required surgical removal anyway were donated by the patients for research purposes, stored in a balanced salt solution, and further used for cell culture within 1 h. Using a surgical microscope, the membranes are pinned onto the cell culture plastic by entomological pins (ENTO SPHINX s.r.o., Pardubice, Czech Republic). Subsequently, the pinned membranes were cultured with Minimum Essential Medium Earl's (MEM, Bio&SELL GmbH) containing 10% FCS until cells grew down from the membrane and could now be cultured as a separate cell line.
Cell culture
Both hRPE and hPVR were cultured in uncoated cell culture flasks (SARSTEDT AG, Nuembrecht, Germany) at 37°C and 5% carbon dioxide, examined under a microscope, and the medium exchange was performed every 2–3 days. The medium used was DMEM and MEM for hRPE and hPVR, respectively, both containing 10% v/v FCS and 2% v/v penicillin and streptomycin (resulting in 200 IU/mL penicillin and 0.2 mg/mL streptomycin; MilliporeSigma). Upon 80%–90% confluence, cells were subcultured with Versene (Gibco by Life Technologies, Paisley, United Kingdom) enriched with 0.25% w/v trypsin (Gibco by Life Technologies).
Dye reduction assay for drug activity screening in terms of cell proliferation and viability
A screening assay as previously described was used to estimate cytotoxicity and antiproliferative potential in hRPE. 14 For toxicity testing, the cells were grown to full cell coverage and starved of serum for 24 h to further lower proliferative activity and induce a stationary layer of cells. Cells were then incubated with different concentrations of the drug until the maximal solubility of the substance in cell culture was reached. For analysis of cell growth, cells were allowed to proliferate in 10% FCS-supplemented medium and treated once 25% of cell confluence was reached. Concentrations that showed toxicity in previous experiments were excluded. The estimated cell number and viability were measured with dye reduction assays: XTT (2,3-bis-(2-methoxy-4-nitro-5-sulfophenyl)-2H-tetrazolium-5-carboxanilide, MilliporeSigma) and WST-1 (4-[3-(4-Iodophenyl)-2-(4-nitro-phenyl)-2H-5-tetrazolio]-1,3-benzene sulfonate, Roche, Mannheim, Germany). Measurements were taken according to the manufacturer's instructions with treatment over 72 h in toxicity testing and 96 h for cell proliferation.
The assays came into use according to the absorbance of the drug and due to delivery shortages of XTT. Photometric measurements were taken after 60 min. A statistically significant reduction in absorbance in comparison to the control was regarded as either toxic or antiproliferative depending on the experimental protocol.
Cell proliferation
The substances with the highest potential from the previous models have been tested on hPVR cells. Therefore, a colorimetric 5-bromo-2’-deoxyuridine (BrdU) assay was performed on hPVR cells using the following substances: dasatinib, methotrexate, resveratrol, retinoic acid, simvastatin, tacrolimus, and tranilast. A measure of 4000 cells per 100 μL was plated with 10% FCS in a 96-well plate. Three concentrations were tested, all close to the previously determined efficient concentration that caused a 50% reduction in cell growth of the maximum possible reduction (EC50). After 96 h of exposure, evaluation was performed according to the manufacturer's instructions except that we added the labeling solution simultaneously with the drugs and therefore lowered the concentration of the “anti-BrdU POD working solution” from 1:100 to 1: 1000.
Scratch wound healing assay
Completely confluent hPVR was scratched with a 100 μL pipette tip (Brand, Lippstadt, Germany). Subsequently, cell-free areas at 0, 8, and 24 h were documented using an inverted phase contrast microscope (Zeiss Axiovert 35, Jena, Germany) and a digital camera (Nikon D31000, Minato, Japan). ImageJ 1.81 (National Institutes of Health, Bethesda, MD, USA) was used to evaluate the repopulated area as a percentage of cell-free area at 0 h.
Statistics
The EC50 was defined as the molar concentration of the drug that results in a 50% reduction in optical density (parameter for cell viability and growth) in between the highest and least effect measured. A four-parameter logarithmic sigmoidal dose–response curve fit was performed to estimate the EC50 using Prism 9 (GraphPad Software, San Diego, CA, USA). Statistical comparison between more than two was done using a one-way analysis of variance and a subsequent Bonferroni post hoc test using SPSS 27 (IBM, Armonk, NY, USA). For all analyses a P < 0.05 was considered statistically significant. All graphs, if not stated otherwise, were plotted in Prism 9 or Excel 365 (Microsoft, Redmond, WA, USA) showing the standard deviation as error bars.
Results
Literature review
The search criterion described above yielded 2859 results on October 30, 2017. After a manual screening of the abstracts, 112 possible substances were identified to potentially mitigate PVR in any type of study. Thirty-six of the substances met the inclusion criteria and were tested in further experiments (Table 1).
Summary of the Literature Review and the Experiments
The following substances did not meet the inclusion criteria: 3-(benzyloxy)cinnamaldehyde, aclarubicin, AG1295, alpha-crystallin B chain siRNA, antiepithelial membrane protein 2 diabody, beta-lapachone, bis-(2-cyanethyl)-amin, bovine vitreous-derived lipid factor, c-fos antisense oligonucleotide, c-myc antisense oligonucleotide, calcitonin gene-related peptide, camptothecin, chebulagic acid, chebulinic acid, chelerythrine, cis-hydroxyproline, colchicine, concanavalin A, connective tissue growth factor inhibitor, cyclic adenosine monophosphate, cyclo(RGDfV), cyclosporin A, cytarabine, daunomycin, doxorubicin, etoposide, fas ligand, fluoroorotic acid-containing liposomes, fluorouracil, geldanamycin, genistein, ginkgo biloba extract EGb761, gold nanoparticle, herbimycin, human recombinant galectin 1, human recombinant galectin 3, intraocular beta-irradiation, JSM6427, low molecular weight heparin, LY-364947, lycopene, mammalian target of rapamycins siRNA, merlin, miR-29 microRNA, miR-34a microRNA, mitomycin C, neuropeptide Y, nuclear antigen chimeric ribozyme, ocriplasmin, p53 lentiviral mediated shRNA, paclitaxel, paromomycin, PD98059, perfluorocarbon liquid, platelet-derived growth factor, platelet-derived growth factor aptamer, porfimer sodium, prinomastat, proliferating cell nuclear antigen antisense oligonucleotides, protein kinase C alpha siRNA, pyrrolidine dithiocarbamic acid, quinotrierixin, ras-related C3 botulinum toxin substrate 1, roundabout protein 1 siRNA, sapanisertib, secretoneurin, semaphorin-3A, SU9518, substance P, teniposide, thiotepa, thrombin, transferrin-ricin A chain toxin, transforming growth factor beta antibody, vasoactive intestinal polypeptide, Y27632.
BrdU, 5-bromo-2’-deoxyuridine; EC50, effective concentration that caused a 50% reduction in cell viability or growth; [M], Molar; max., maximal.
Toxicity
In the prescreening, 17 out of the 36 substances showed a potentially toxic effect below the maximal solubility in cell culture (Fig. 1, Table 1). The concentrations detected were excluded from further investigation, as a potentially toxic effect on other ocular cells must be expected and the pharmacological effect of the substance should not be explained by toxicity. Nineteen substances did not show a reduced optical density within the range of solubility in cell culture (Supplementary Fig. S1).

Seventeen substances showed toxic effects on hRPE in our screening assay. Substances without toxic effects can be found in detail in Supplementary Fig. S1. Data were obtained by WST-1 or XTT assays on hRPE following 72 h of treatment with the substance or the associated solvent of the drug serving as Co. The OD as measured is plotted against the logarithmic concentration in pM. The control was set as 100%, and all tested concentrations were calculated relative to the control. The concentrations showing a statistically significant reduction are depicted in grey color (P < 0.05; for exact P values refer to Table 1; n = 3–5 depending on the substance tested). Co, control; hRPE, human retinal pigment epithelial; OD, optical density; WST-1, 4-[3-(4-Iodophenyl)-2-(4-nitro-phenyl)-2H-5-tetrazolio]-1,3-benzene sulfonate; XTT, 2,3-bis-(2-methoxy-4-nitro-5-sulfophenyl)-2H-tetrazolium-5-carboxanilide.
Proliferation
In the WST-1 prescreening test, 15 substances showed a statistically significant antiproliferative effect (Fig. 2, Table 1). Furthermore, 9 substances were found to have only toxic and no growth inhibitory effects, and 10 showed no statistically significant effects in terms of proliferation. Interestingly, the two vascular endothelial growth factor antibodies, bevacizumab and ranibizumab, reproducibly showed a significant increase in optical density (Supplementary Fig. S2). The seven substances with the broadest therapeutic range, that is, the highest difference between the lowest toxic concentration and the highest concentration that did not yield antiproliferative effects (Fig. 3), were retested using hPVR and a BrdU assay to evaluate their potential in an additional setting.
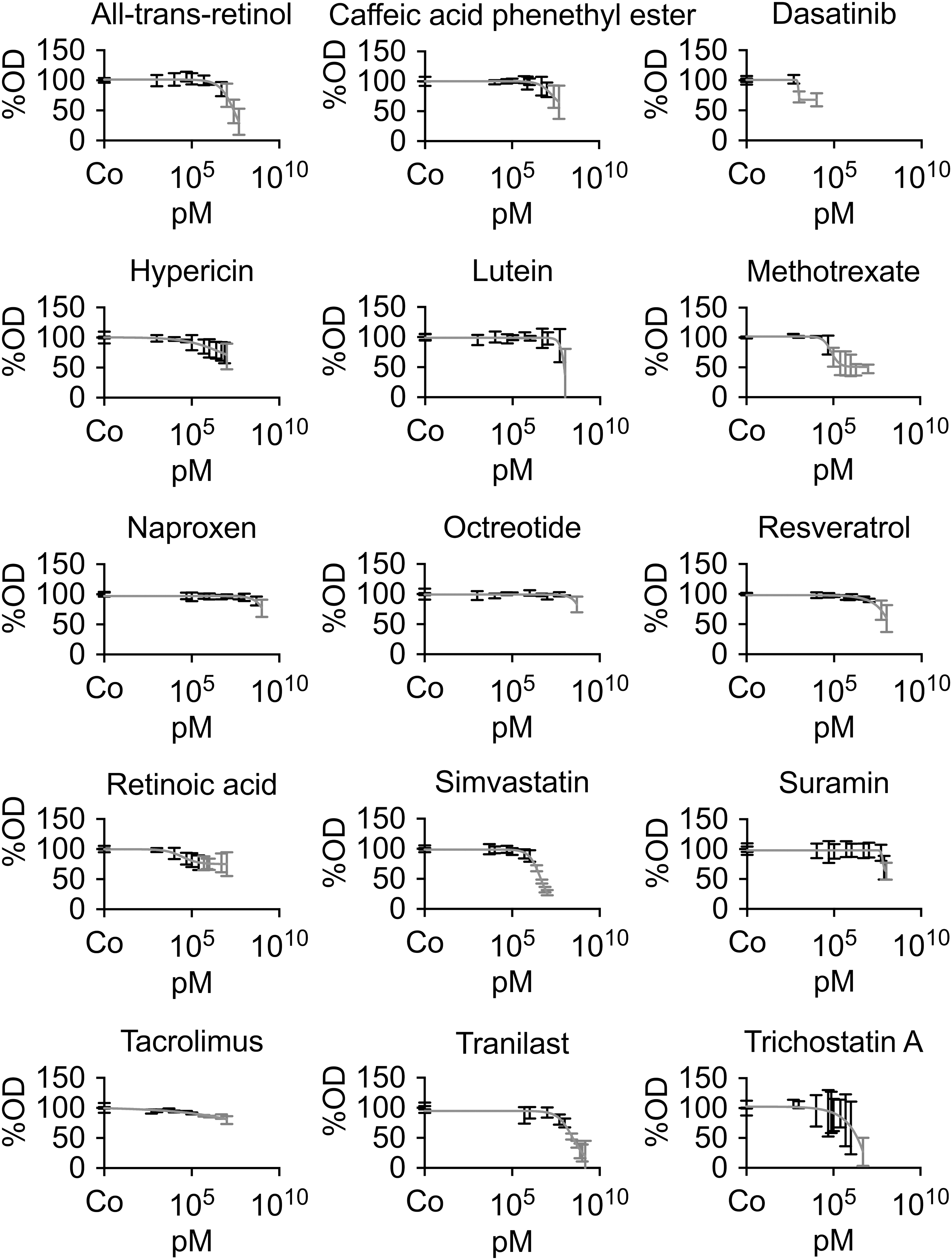
Fifteen substances showed a significant antiproliferative effect on hRPE. For all other substances Supplementary Fig. S2 can be consulted. The OD as determined by the dye reduction assay is plotted against the logarithmic concentration in pM. The Co was set as 100%, and all tested concentrations were calculated relative to the control. A four-parameter logarithmic sigmoidal dose–response curve fit was performed to estimate the EC50. The result of the curve fit is plotted in every graph as a grey line. The concentrations showing a statistically significant reduction are shown in grey color (P < 0.05; for exact P values refer to table 1; n = 3–5 depending on the substance tested).
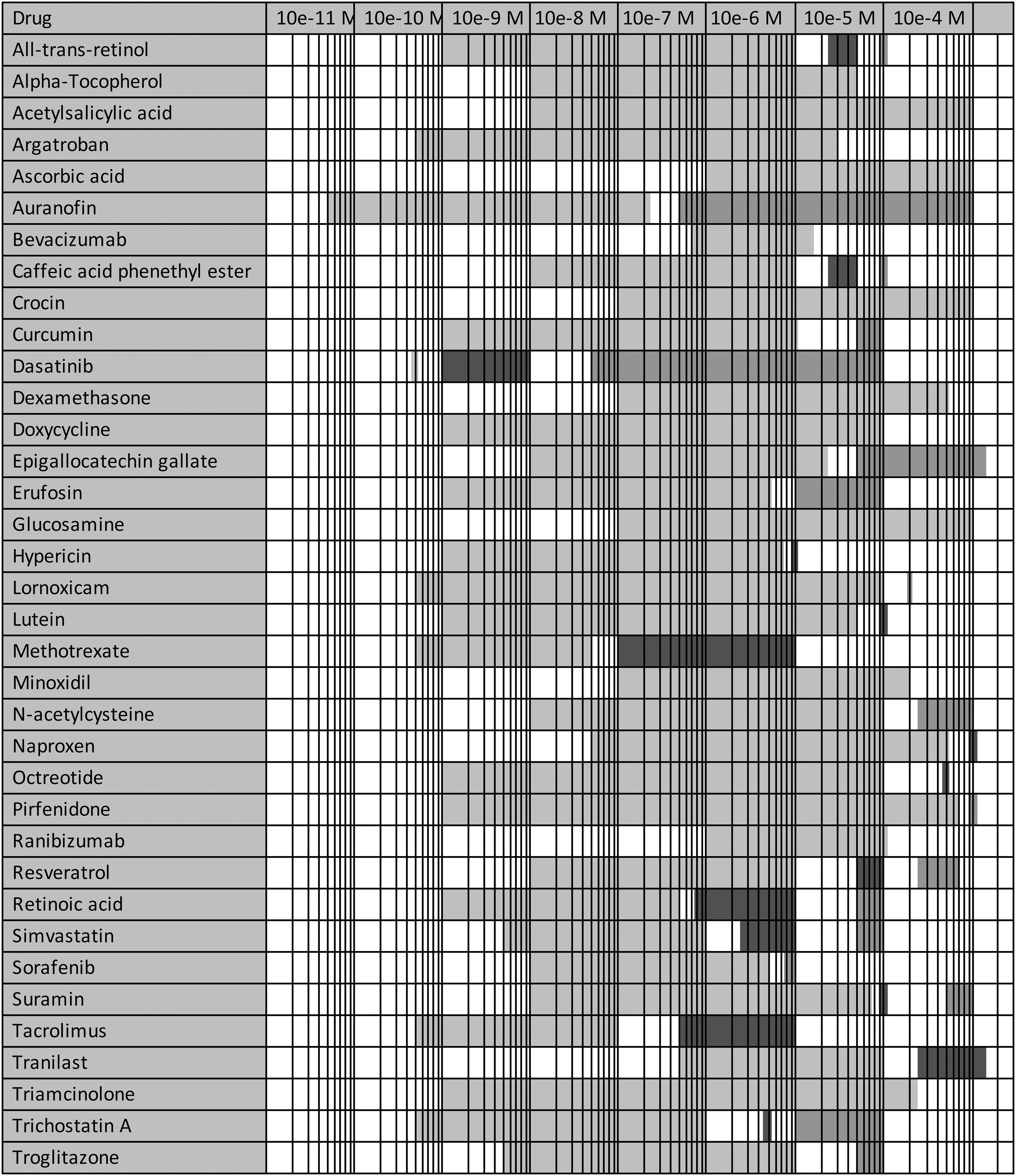
A direct comparison between the different substances in a tabular view is shown. A logarithmic scale was used to depict the tested molar concentrations (M). Toxicity was tested on hRPE for 72 h and measured with XTT or WST-1, respectively, whereas antiproliferative effects were tested on hRPE for 96 h and measured with WST-1. Light grey areas represent the concentration range without statistically significant toxic or antiproliferative effects (P > 0.05). Dark grey ranges are those with significant antiproliferative effects (P < 0.05) and no significant toxicity (P > 0.05). The concentration range that showed significant toxicity (P < 0.05) is depicted in medium grey. The concentration range in white color has not been tested in the experiments (n = 3–5 depending on the substance tested).
hPVR proliferation
Of the seven compounds reevaluated on the primary hPVR cells, we could determine three substances that showed reproducible antiproliferative effects in the BrdU assay. Those are resveratrol, simvastatin, and tranilast. Resveratrol showed significant effects at 10 μM (80% ± 9%; P = 0.027), 50 μM (63% ± 13%; P < 0.001), and 100 μM (52% ± 15%; P < 0.001). Simvastatin showed significant effects at 2.5 μM (74% ± 3%; P < 0.001), 5 μM (64% ± 9%; P < 0.001), and 7.5 μM (41% ± 8%; P < 0.001). Tranilast showed significant effects at 500 μM (82% ± 6%; P = 0.03). Methotrexate, retinoic acid, tacrolimus, and dasatinib did not demonstrate significant effects in the BrdU assay (Fig. 4).

Resveratrol, simvastatin, and tranilast decrease proliferation in BrdU cell proliferation assay on primary human PVR cells. Following 96 h of treatment with DMSO/PBS (Co; PBS for methotrexate), dasatinib, methotrexate, resveratrol (significant Conc.: 10 μM; 50 μM; 100 μM), retinoic acid, simvastatin (significant Conc.: 2.5 μM; 5 μM; 7.5 μM), tacrolimus, or tranilast (significant Conc.: 500 μM). The control was set as 100% of the OD, and all tested concentrations were calculated relative to the control. (*P < 0.05; **P < 0.01; ***P < 0.001). Conc., concentration; DMSO, dimethyl sulfoxide; PBS, phosphate-buffered saline; PVR, proliferative vitreoretinopathy.
hPVR scratch wound healing assay
A wound-induced scratch assay was performed to determine an effect on cell migration in the seven most promising substances. After 24 h the relative area covered by cells was statistically significantly lower for dasatinib (P < 0.001), resveratrol (P < 0.001), and tranilast (P = 0.006) compared to the untreated control. All other substances did not reach statistical significance. A statistically significant difference at 8 h after inducing the scratch could not be determined for any of the substances (Fig. 5).

Results of the scratch wound migration assay are presented for each tested substance at 0, 8, and 24 h. The relative (rel.) area repopulated by cells after 24 h was significantly reduced when resveratrol (P < 0.001 represented as the lowest graph), dasatinib (P < 0.001 represented as the second lowest graph), and tranilast (P = 0.006 represented as the third lowest graph) were added to the culture medium for 24 h in comparison to the respective Co (represented as the second highest graph)
Discussion
Fifteen of the 36 investigated substances showed significant antiproliferative effects on hRPE. Among them, seven drugs were with a broad concentration range between toxicity and antiproliferative effect extending over more than one order of magnitude. Those seven are dasatinib, methotrexate, retinoic acid, tacrolimus, resveratrol, simvastatin, and tranilast. In addition, resveratrol, simvastatin, and tranilast reduced the proliferation of primary hPVR cells significantly. Dasatinib, resveratrol, and tranilast mitigated hPVR migration.
One of the substances which showed promising results in our setting is simvastatin. The 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor belongs to the group of statins and is widely used for the treatment of hypercholesterolemia. The substance was inhibiting proliferation significantly between 2.5 and 7.5 μM both in hRPE and hPVR. Toxicity became apparent at 50–100 μM. This is in keeping with the literature. A significant reduction of lipopolysaccharide-induced pro-inflammatory cytokines (interleukin-6 and 8, monocyte chemoattractant protein-1) by 5 μM simvastatin on ARPE19 cells was described and might be the explanation for a mitigative effect on PVR development. 15
In addition, 1–10 μM simvastatin was shown to be a dose- and time-dependent inhibitor of gel contraction of bovine hyalocytes and at 5 and 15 μM it decreased the formation of PVR in the rabbit model. 16 Five micromolar of simvastatin also inhibited TGF-β2-induced phosphorylation of myosin light chain, a mediator in the Rho-kinase signaling pathway and TGF-β2-induced collagen 1 protein in human RPE cells. 17 Clinical evidence was also found that suggested a positive mitigative effect against PVR after retinal detachment surgery. Levels of angiopoietin-2, vascular endothelial growth factor, and activity of metalloproteinase-2 were lower in the retinal detachment vitreous of patients with statin treatment at 1 month. Postoperative visual acuity gain was improved when systemic statins were administered.
A Finnish population-based cohort study of 1916 vitrectomized patients suffering from rhegmatogenous retinal detachment had a 28% lower risk of revitrectomy when systemic statins were used. 18 The intravitreal concentration of orally ingested simvastatin in another study (40 mg/day) was determined to settle between 0.064 and 0.17 nM, which is approximately equivalent to unbound statin at steady-state—consequently, only unbound statin can cross the blood–retinal barrier. 15 This is one order of magnitude lower than the determined EC50 in our study, and simvastatin has a short half-life of 1–5 h. 15 Therefore, another route of application might be necessary, also to avoid systemic toxicity. Intravitreal injection of up to 200 μM simvastatin produced no adverse effects in the mouse retina. 19
Resveratrol is found in cranberries and red currants. It has antioxidant and anti-inflammatory properties and is used for heart disease and cancer, as well as inflammatory and degenerative diseases. 20 Several studies have found evidence of a mitigative effect against PVR. 21 A significant decrease in proliferation and protection against H2O2-induced intracellular oxidation was shown at 50 and 100 μM on ARPE19. 22 These two concentrations are mentioned in other studies too and along with the observed toxicity at 200 μM are in line with our results.23,24
Furthermore, in the literature it is described that resveratrol might inhibit cellular responses that might lead to the development of PVR. Resveratrol has been shown to arrest or even reverse extracellular matrix contraction of ARPE19 and of fetal hRPE cells induced with TGF-β2, respectively. The expression of epithelial markers E-cadherin and zonula-occludens-1 was increased by resveratrol, while the mesenchymal markers smooth muscle actin and vimentin, as well as cell migration and gel contraction, were decreased in ARPE19 cells induced by TGF-β2.23,24
Proliferation, migration, and fibronectin synthesis were also reduced in resveratrol treated RPE cells following induction with platelet-derived growth factor. 24 Clinical trials were conducted, and one study found resveratrol to be abundant in different ocular tissues after vitrectomy and oral administration. Although the concentration of parent resveratrol was low in the eyes, its metabolites could be detected. 25 Resveratrol may well be considered a potential therapeutic agent against PVR formation. 26
Tranilast is an antiallergic drug that has also been used for keloidal scars or scar treatment and is becoming increasingly interesting for cancer treatment. It seems to interfere with several signaling pathways, namely TGF, mitogen-activated protein kinase, and protein kinase B (Akt/PKB), and further modulates cancer stem cells. 27 In our experiments tranilast revealed that antiproliferative effects without being toxic on hRPE in concentrations ranging from 250 μM up to 1.5 mM and 500 μM also showed a significant antiproliferative effect on hPVR cells. This is consistent with the literature. A measure of 300 μM on bovine RPE cells and rabbit dermal fibroblasts was antiproliferative, preventing gel contraction and decreased TGF-1 secretion. 28 Efficacy without toxicity of tranilast was demonstrated in a rabbit model of PVR. Five milligram per milliliter reduced the formation of PVR after 28 days, and the amount of TGF-β1 was significantly lower with tranilast than in controls. 29
Our prescreening test showed several drugs, which have been suggested for the prevention of PVR in peer-reviewed articles but did not show an effect in our work. There are several possible reasons why we could not reproduce those results. Study endpoints and models varied widely across the literature, and results from PVR models in animal models 30 and different cell lines 31 might not yield comparable results. The same issue was apparent in our study. The hPVR cells, which already underwent typical pathobiological changes in the patient, could not reproduce the results of the cultured primary hRPE cells from healthy donors. This might be due to different cellular processes that are activated during the disease process. Another explanation for the varying results could be that there were substances that were already regarded as ineffective in follow-up or human trials. Examples are bevacizumab 32 and steroids. 33 Different definitions of toxicity might have led to exclusion of concentrations of certain compounds that were regarded as toxic in our study, but not in other studies. 34
Several future challenges need to be addressed before a clinical option becomes available. The most suitable dosage and route of application need to be further explored in cell and animal models before a clinical benefit can be foreseen. Eyedrops might not be able to reach the retina due to diffusion barriers in ocular tissue. Moreover, concentrations in the eye might be lower and systemic toxicity higher in medication administered orally. 15 A single administration to the eye during surgery is very feasible but might not be sufficient enough to halter the process as pharmacokinetics in the eye might cause a fast clearance of the drug. Multiple intravitreal injections might therefore be necessary. 35 To overcome the issue of multiple injections drug carriers with slow-release properties have been proposed and might be an option. 9
In addition, there are several options for when to administer medication against PVR in the course of the disease. First, a prophylactic treatment after surgery for retinal detachment would be possible but will be associated with a higher number needed to treat, as not all patients will develop PVR. 36 A therapy in this setting should have low side effects and good biocompatibility. Second, a prophylactic administration only in high-risk eyes, for example, after trauma or longer-standing retinal detachment, would possibly reduce the number of patients treated and therefore fewer patients get treated unnecessarily. The third option would be to treat when PVR has already developed to induce arrest of the membranes and contraction. 37
Limitations of the study include inherent problems that arise from the use of cell culture as a model for PVR. The hRPE cells used are a very simplified model for PVR and do not fully represent the pathological basis of PVR as the retina is a complex tissue with glial cells, neuro tissue medullary phages, and blood vessels. The transferability to humans must therefore be explored in further studies. The chosen cell culture conditions, including a high amount of serum, were used in an attempt to simulate the clinical situation in PVR eyes, including a breakdown of the blood–aqueous barrier. Other additions to the medium such as substances, cytokines, or growth factors might have led to different results. Testing and systematically comparing different substances considering their effect on PVR is a process of consuming many resources. We, therefore, opted for an easy prescreening method in a human model for PVR.
Most of the substances tested in this article are highly lipophilic and were not well soluble in the culture medium. After the maximum solubility, the substance precipitates in the medium and concentration does not increase. We could therefore only perform experiments up to the highest soluble concentration. It is not clear how solubility changes within the eye, and in vivo and clinical studies are needed to clarify this issue. Fibrotic contractile cells undergo epithelial–mesenchymal transition, cell invasion from different locations, migration, proliferation, and extracellular matrix production to form membranes which are able to contract and detach the retina. In this study, we did not investigate all of the cellular factors associated with PVR formation, and results might differ if other factors were chosen. A colorimetric test was used to estimate the effect on cell proliferation and toxicity by measuring metabolic reduction in the cells as an indirect indicator. Both the drug and other cellular factors could have influenced this metabolic reduction.
In summary, this study presents a direct systematic comparison of pharmacologic substances that have been proposed for PVR treatment in a human disease model. Dasatinib, resveratrol, simvastatin, and tranilast seem to be promising and are well-characterized in human and ocular use. Especially high-risk patients could benefit from a follow-up of these results in research, through improved visual acuity or reduced need for reoperation. Further studies, experimental and clinical, are warranted to determine the clinical potential of the findings of this article.
Footnotes
Authors' Contributions
N.T.: Writing—original draft, Writing—review and editing, Investigation, Methodology, Project administration, Formal Analysis. S.K.: Writing—review and editing, Formal Analysis. A.O.: Resources, Supervision. L.S.: Investigation. S.G.P.: Resources. D.H. and A.W.: Supervision. C.M.W.: Writing—original draft, Writing—review and editing, Conceptualization, Formal Analysis, Funding acquisition, Visualization.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Institutional funding from the Friedrich-Baur-Foundation, University Hospital, LMU Munich was available for this research project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.