
Abstract
Corneal injuries from chemical burns, mechanical trauma, infections, immunological rejections, surgical complications, and some diseases are commonly associated with persistent epithelial defects (PED), neurotrophic epitheliopathy, scarring fibrosis, corneal neovascularization (CNV), and/or corneal endothelial damage that lead to vision loss. Several Food and Drug Administration (FDA) approved medications have recently become available, are currently in clinical trials, or are likely to enter clinical trials in the near future. For example, a 2-week course of topical human recombinant nerve growth factor is frequently an effective treatment for corneal neurotrophic epitheliopathy associated with PEDs. Topical losartan, an angiotensin converting enzyme II receptor antagonist that also inhibits TGF beta signaling, has been shown to effectively decrease myofibroblast generation and scarring fibrosis in alkali burn injury and Descemetorhexis rabbit models. Small molecule topical tyrosine kinase inhibitors, such as sunitinib and axitinib, FDA approved as chemotherapeutic agents to treat specific cancers, have also been found to be effective topical inhibitors of CNV in animal and human trials. Rho-kinase inhibitors, such as ripasudil and netarsudil, that are currently approved agents for the treatment of glaucoma in some countries, have been shown to stimulate corneal endothelial proliferation in animal studies and human trials, and may accelerate the regeneration of Descemet's membrane. These agents, as well as other drugs in development, will be used in targeted combinations to treat corneal pathophysiology associated with epithelial healing disorders, stromal scarring fibrosis, CNV, and corneal endothelial injury during the next decade.
Introduction
Corneal pathological changes due to injuries, such as chemical burns, mechanical trauma, microbial keratitis, immunological rejections, or surgical complications, commonly lead to vision loss. 1 Persistent stromal opacity in each of these injuries commonly occurs by the same myofibroblast-related mechanism in humans as they do in rabbits and other species.2–4 Depending on the type and severity of injury, corneas in humans and other species may also develop persistent epithelial defects (PEDs),5,6 corneal neovascularization (CNV),7,8 and/or corneal endothelial dysfunction, along with stromal fibrosis (Fig. 1).2,5,9

Cornea after alkali burn with 1N NaOH. At 1 month after a 15 s 5 mm diameter alkali burn with 1N NaOH, a rabbit cornea that had duplex immunohistochemistry for alpha-smooth muscle actin (red), keratocan (green), and cell nuclei staining with 4′,6-diamidino-2-phenylindole (DAPI, blue) shows evidence of a neurotrophic cornea with friable central epithelium and a PED (large arrowhead). There is also both anterior stromal and posterior stromal corneal fibrosis (small arrowheads, F) with myofibroblasts staining red for alpha-smooth muscle actin. Peripheral neovascularization (NV, small arrows) is noted on the left side of the cornea, with pericytes of the neovascularization also staining for alpha-smooth muscle actin. Most of the central cornea is devoid of endothelial cells and Descemet's membrane was artifactually detached from the posterior stroma during sectioning. Mag 100X. PED, persistent epithelial defect.
Most of these opacity-producing corneal injuries are currently treated with modalities such as penetrating or lamellar keratoplasty, 10 phototherapeutic keratectomy, 11 conjunctival flaps, 12 stem cell transplantation, 13 amniotic membranes,13,14 or keratoprosthesis. 15 Pharmacological interventions are typically limited to topical corticosteroids, which may be effective in reducing inflammation, but are commonly ineffective in controlling the development of corneal scars or neovascularization. Recent developments in several areas, however, provide hope that effective pharmacological treatments for many corneal injuries will soon be available. This article will review new developments for both drugs that have received Food and Drug Administration (FDA) approval and those that have shown promise in animal models.
Nerve Growth Factor for the Treatment of Neurotrophic Keratopathy
Among the most frustrating disorders in humans and animals to treat are corneal neurotrophic epitheliopathies, often with PEDs, that are caused by many disorders, including diabetes mellitus, 16 herpes infections,17,18 and chemical injuries (Fig. 2).5,9 In these corneas, the epithelium is often thinner than normal and friable, with surface irregularity (Fig. 1).5,9,16–18 The epithelium typically has punctate epithelial erosions detected with rose bengal or lissamine green dye. Frequently, PEDs develop with rolled leading edges and exposed epithelial basement membrane (EBM) or stroma stains with fluorescein. PEDs commonly lead to stromal melting and fibrosis that may be accompanied by stromal neovascularization (Fig. 1).5,9,16–18 The corneal epithelium is dependent on trophic factors released by the corneal sensory nerves for normal viability and function.19–21 One of these trophic factors that has been identified and found to be efficacious in treating the symptoms and signs of neurotropic epitheliopathy is nerve growth factor (NGF).
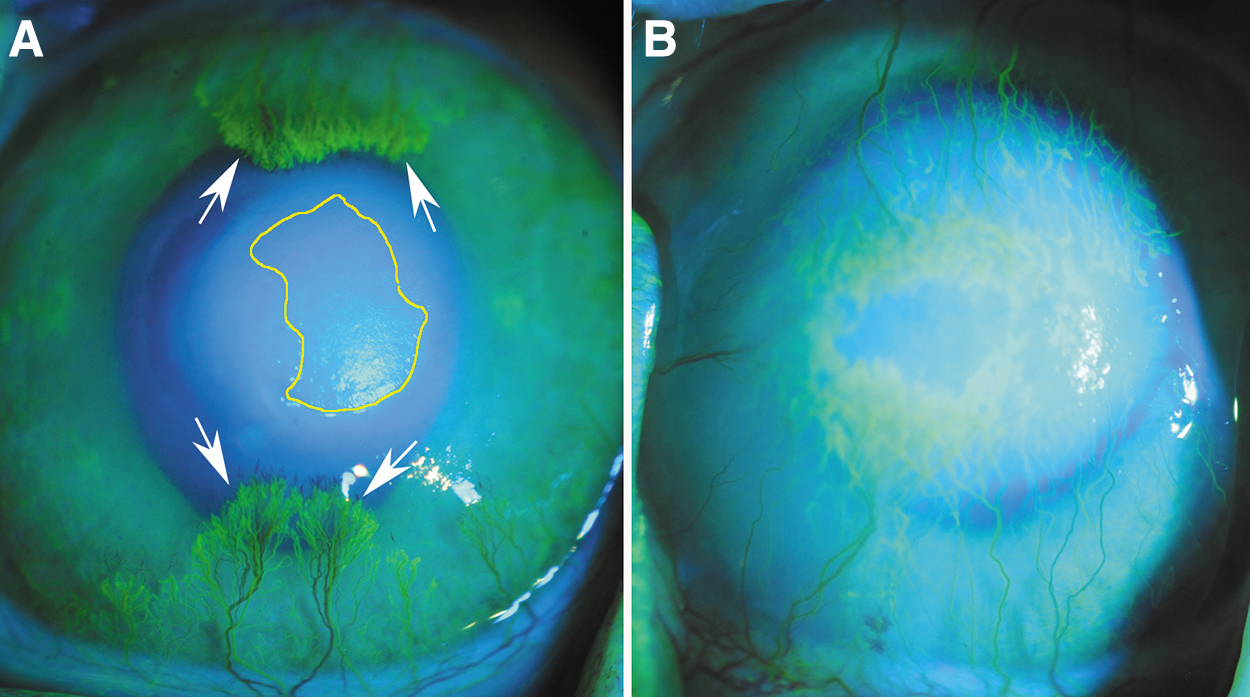
Persistent epithelial defect and corneal neovascularization after alkali burn injury. Corneal angiography following intravenous sodium fluorescein injection at 1 month after 1N NaOH burn.
In early studies, murine NGF (at 200 μg/mL) was applied at intervals from every 2 h to six times per day, with marked improvement in neurotrophic epitheliopathy in most patients.22,23 More recently, human recombinant NGF (hrNGF, Cenegermin) was developed and found to be safe and efficacious in treating symptoms and signs of neurotropic epitheliopathy caused by several disorders (herpetic eye disease, ocular surgery-induced epitheliopathy, dry eye, etc.) in a phase III clinical trial when applied as 35 μL of a 20 μg/mL solution six times per day for 2 weeks (Table 1). 24 hrNGF was approved by the FDA for neurotrophic corneas in 2018 and is available commercially as a 20 μg/mL solution (Oxervate, DOMPE’ FARMACEUTICI S.P.A., Boston, MA, USA). hrNGF is typically applied one drop six times per day for 2 weeks, and the application can be repeated, if necessary, to effectively treat neurotropic epitheliopathy.
Corneal Disorders, Pathology, and Topical Pharmacological Agents approved, in Trials and Preclinical Studies
ABK, aphakic bullous keratopathy; CNV, corneal neovascularization; DMEK, Descemet membrane endothelial keratoplasty; DSAEK, Descemet stripping automated endothelial keratoplasty; DWEK, Descemetorhexis without endothelial keratoplasty; PBK, pseudophakic bullous keratopathy; PED, persistent epithelial defect; PKP, penetrating keratoplasty; PRK, photorefractive keratectomy.
The amino acid sequence of NGF, especially in the domain responsible for the biological activity, has been highly conserved between different species during evolution.25–27 Thus, murine NGF has been shown to be effective in humans in several studies.22,23,28 Similarly, hrNGF 29 and murine NGF 30 have been found to be effective in rabbits. The mechanism is thought to be action of the drug as a neurotropic factor to both promote viability and normal physiology of the corneal epithelium and as a tropic factor to stimulate regeneration of the stromal nerves after injury.22–29 Due to the size of the NGF protein, penetration into the corneal stroma would be expected to stop after closure of any PED, but tropic effects on the epithelial cells themselves would be expected as long as the treatment continues.
Given the efficacy of topical hrNGF or murine NGF in neurotrophic epitheliopathy caused by herpetic eye disease, ocular surgery, and dry eye disease,22–24 it is likely that NGF would also be effective in neurotrophic epitheliopathy and PEDs caused by chemical burns produced by agents such as sodium hydroxide 5 and sulfur mustard. 9 Future studies should explore the use of NGF to facilitate treatment of these severe corneal injuries that are often associated with epitheliopathy and PEDs.
Stromal Fibrosis Treatment with Topical Losartan and Other ACEII Receptor Inhibitors
Myofibroblast-mediated stromal fibrosis with scarring frequently develops after trauma, normal and complicated surgeries, microbial infections, chemical burns, and other injuries to the anterior, posterior, and/or peripheral cornea (Fig. 1).2,3,5 Myofibroblasts develop from keratocytes via corneal fibroblasts in the stroma and bone marrow-derived fibrocytes that enter the stroma via the limbal blood vessels after injury. Frequently, CNV enters the stroma from the periphery in fibrotic corneas.2,3,5
Losartan (Table 1) is an angiotensin converting enzyme II receptor inhibitor that is commonly used for the treatment of hypertension, renal diseases, and heart failure.31,32 Renin–angiotensin–aldosterone system (RAAS) blockade by oral angiotensin-converting enzyme (ACE) II receptor inhibitors has been used in clinical and research studies for decades to treat diseases associated with fibrosis. For example, losartan was found to decrease progressive soft tissue fibrosis associated with a genetic skin blistering disease dystrophic epidermolysis bullosa when given to mice. 33 The mechanism, through which losartan was thought to modulate fibrosis, was by inhibition of TGF beta signaling, with TGF beta-1 and TGF beta-2 being critical modulators of myofibroblast development from precursor corneal fibroblasts and bone marrow-derived fibrocytes.34–39
Myofibroblasts, once developed, are critically dependent on ongoing and adequate levels of TGF beta-1 and/or TGF beta-2, or they undergo apoptosis.34–39 The first demonstration of the efficacy of losartan in modulating TGF beta-driven myofibroblast development and stromal opacity in the cornea was a study in rabbits where topical, but not oral, losartan given at a dosage of 0.4 mg/mL six times per day for 1 month (Fig. 3) inhibited scarring fibrosis after central removal of the corneal endothelium and Descemet's membrane (Descemetorhexis). 40 In another rabbit study, 6 combined topical 0.8 mg/mL losartan and 1% prednisolone acetate six times per day was more effective than topical vehicle, or either 0.8 mg/mL losartan or 1% prednisolone acetate alone, in decreasing stromal myofibroblasts and stromal fibrotic opacity. Thus, this combination addressed both inflammation (due to alkali-induced cellular and matrix necrosis) and myofibroblast generation better than either agent alone.

Losartin (Los) in Descemetorhexis-induced scarring fibrosis.
40
Bone marrow-derived fibrocytes enter the stroma from the corneal limbal blood vessels after injury and serve as TGF beta-driven precursors to myofibroblasts,41,42 in addition to corneal fibroblasts that develop locally from keratocytes.2,5,41 Corticosteroids have been found to have two effects on fibrocytes that decrease generation of myofibroblasts from these precursors. First, corticosteroids inhibit the proliferation of fibrocytes that is needed for the generation of large numbers of myofibroblasts.42,43 Second, corticosteroids also trigger fibrocyte apoptosis 44 and thereby decrease the number of precursor cells available to develop into myofibroblasts in the tissue. Thus, topical corticosteroids probably augment losartan inhibition of myofibroblast development from both corneal fibroblasts and fibrocytes.
A limitation of both of these studies was that the treatment was given for only 1 month—the peak of fibrosis in rabbit injury models.2,5,40 It is likely that longer applications of losartan in both of these injury models would further decrease myofibroblasts and stromal opacity. Also, even after the disappearance of myofibroblasts, considerable time, usually measured in months to years, is needed for corneal fibroblasts and keratocytes to migrate into the affected stroma and reabsorb and remodel necrotic extracellular matrix (ECM) and/or disordered ECM produced by myofibroblasts and corneal fibroblasts.2,3,5
There is a large family of ACE II receptor inhibitors that could be effective in decreasing scarring fibrosis in the corneal stroma after injury. The advantage of losartan is that it is soluble up to ∼0.9–1.0 mg/mL in balanced salt solution vehicle. In preliminary studies (Shiju TM and Wilson SE, unpublished data, 2021), it was found that telmisartan and candesartan were only soluble to 0.3 and 0.1 mg/mL, respectively. Other ACE II receptor inhibitors tested, including valsartan, olmesartan, irbesartan, azilsartan and losartan metabolite EXP-3174, were insoluble in balanced salt solution. Thus, while these other ACE II receptor inhibitors might be effective in decreasing myofibroblast generation and stromal fibrosis, or increasing myofibroblast apoptosis, when treating established stromal fibrosis, alternative vehicles would be needed to utilize these alternative ACE II receptor inhibitors.
This problem is similar to the issues noted with topical cyclosporine A applications to the eye. Losartan also clearly penetrates the corneal epithelium and into the deepest stroma since after Descemetorhexis injury, it was found to inhibit collagen type IV production by corneal fibroblasts extending to the posterior stromal surface in corneas with normal epithelium. 40 This epithelial penetration has not been studied for the alternative ACE II receptor inhibitors.
Importantly, these studies found no evidence of losartan-induced toxicity in either injured or control uninjured rabbit corneas.6,40 Further rabbit studies evaluating more frequent dosing with topical losartan, as well as treatments of longer duration, are needed. Future clinical trials in humans with a variety of injuries will also be needed to prove the efficacy and safety of losartan or other ACE II receptor inhibitors. It is likely, however, that topical losartan can effectively decrease corneal scarring fibrosis when given as an adjuvant treatment in disorders commonly associated with stromal scarring fibrosis, such as trauma, chemical burns, microbial corneal infections, neurotrophic epitheliopathy with PEDs, and surgical complications.
Although this needs to be verified in clinical trials, topical losartan would likely need to be continued, possibly with lower frequency of application, for at least several months after resolution of stromal fibrosis, regardless of the underlying etiology, to allow the time needed for complete repair of the EBM and/or Descemet's membrane, depending on the triggering injury, for restoration of normal corneal control of TGF beta penetration in the anterior and posterior cornea, respectively.
Topical losartan may also have applications in inhibiting fibrosis in other anterior segment tissues where myofibroblast development has a role in the fibrosis pathophysiology. For example, it could be a useful agent for conjunctival scarring disorders such as trachoma 45 and the fibrosis of conjunctival blebs after glaucoma filtering surgeries. 46
CNV and Inhibitors
CNV is a serious complication that frequently is noted after trauma, chemical burns (Figs. 1 and 2), infections, allergies, hypoxia, limbal stem cell deficiencies, transplant rejections, complicated surgeries, or diseases of the cornea because it not only severely affects the transparency of the cornea, and thereby vision, but also greatly increases the chance of rejection if corneal transplantation is needed. 47 CNV can be difficult to prevent, and treat once it develops, and topical corticosteroid treatment alone is frequently ineffective.
Both angiogenesis and vasculogenesis are thought to be involved in CNV.48,49 Vasculogenesis is the de novo formation of vessels from vascular endothelial precursor cells, such as hemangioblasts and angioblasts, derived from mesodermal precursors (via mesodermal induction).48,49 Angiogenesis, on the contrary, is the process by which vascular endothelial cells of preexisting blood vessels proliferate and form new vessels.49,50 In the normal transparent cornea, avascularity is maintained by a balance of proangiogenic and antiangiogenic factors. 50 Thus, the cornea releases proangiogenic growth factor (VEGF), platelet-derived growth factor (PDGF), fibroblast growth factor-2, and interleukins that are sequestered in the ECM, including the EBM, that are counterbalanced by local antiangiogenic factors.8,50
Antiangiogenic factors include angiostatin, pigment epithelium-derived factor, soluble vascular endothelial growth factor receptor-1, tissue inhibitor of metalloproteinase-3, collagen XVIII (endostatin), angiostatin, restin, arrestin, endostatin, canstatin, tumstatin, and thrombospondins.8,50 Imbalance of these factors in pathological conditions triggers the abnormal proliferation of preexisting blood vessels (hemangiogenesis) and lymph vessels (lymphangiogenesis) into the corneal stroma to produce CNV. Blood and lymph vessels are normally absent from the central cornea.
Inflammation, and its effects on the balance of angiogenic and antiangiogenic factors in the cornea, has a critical role in the development of CNV induced by infection, chemical injury, trauma, immune disorders, hypoxia, or limbal stem cell deficiency,8,50 and likely is a major cause of CNV in animal injury models.5,40 There is also an interplay between inflammatory cells recruited into the corneal stroma after injury, especially macrophages and neutrophils, and angiogenic growth factors, such as VEGF family members, in inflammation-induced CNV. VEGF-A-mediated recruitment of macrophages initiates the “immune amplification cascade” that promotes corneal hemangiogenesis and lymphangiogenesis. 51 Thus, inflammatory cells that are recruited by corneal injury, including macrophages, produce proangiogenic factors and proteolytic enzymes that promote limbal vascular endothelial cell proliferation and migration.51–54 Proinflammatory cytokines and chemokines are strong mediators of angiogenesis in humans and are overexpressed in inflamed corneas.55–63
Most existing models of CNV are related to corneal surface inflammation induced with chemical cauterization and/or suture placement.64,65 These models have an inflammatory component that mimics the complex nature of CNV in human diseases.64,65 Chemical cauterization models induce CNV by application of alkali (typically 1N NaOH) or silver/potassium nitrate to the center of mouse, rat, or rabbit cornea for a short time, followed by irrigation with saline. 66 However, CNV that develops after alkali burns, 6 corneal endothelial/Descemet's membrane damage,2,40 and other injuries, often include much deeper stromal vessels that may be more difficult to treat pharmacologically.
The main treatment for CNV has been to suppress the inflammatory response associated with these injuries with the administration of topical corticosteroids that suppress active growth of CNV through inhibition of cell chemotaxis, proinflammatory cytokine release, and prostaglandin synthesis. 67 However, their efficacy is typically limited in controlling CNV, and chronic use of corticosteroids is often associated with side effects, such as glaucoma, cataracts, and increased risk of infection, and better approaches to prevent and treat CNV are needed.
Bevacizumab, a recombinant monoclonal immunoglobulin G1 antibody directed against all isoforms of VEGF-A, has been used as an anti-VEGF agent for the treatment of CNV by inhibiting angiogenesis and vasculogenesis. 68 Although it is a large molecule, it has been successfully used topically to treat CNV in a mouse model and is a prototype drug to treat CNV. 69 However, smaller molecules are likely to have better epithelial penetration and be more efficacious if they target multiple modulators of CNV. 64
Sunitinib (Table 1), previously known as SU11248, is one of the most promising small molecules to prevent and treat CNV since it is a potent, multitarget tyrosine kinase inhibitor of VEGF receptors, PDGF receptors, c-KIT, and RET, and thereby inhibiting angiogenesis and vasculogenesis controlled by these receptors that modulate CNV via stimulation by their agonist cytokines and growth factors. 70 Sunitinib has been approved for the treatment of metastatic renal cell carcinoma and gastrointestinal stromal tumors. 70 VEGF exerts its effects through interaction with vascular endothelial growth factor receptors (VEGFRs) that are receptor tyrosine kinases.71,72 VEGFR1 and VEGFR2 are thought to be the major signal transducers of hemangiogenesis in CNV.71,72 Conversely, VEGFR-3 is likely the major contributor to lymphangiogenesis. 72
One study compared topical administration of sunitinib to topical bevacizumab. 72 Both treatments inhibited CNV in a rabbit suture model. However, sunitinib was found to be three-fold more potent than bevacizumab, possibly because of its inhibition of both the VEGF and PDGF pathways. 72 Another study supported sunitinib having greater potency over bevacizumab and indicated a greater inhibitory effect when administered topically at 0.5 mg/mL rather than subconjunctivally. 73 In a study in rats, 74 sunitinib in microspheres that were subconjunctivally injected inhibited suture-induced CNV. No significant toxicity was observed in vivo with topical sunitinib.71–74
Axitinib (Table 1), previously known as AG013736, is another small multitarget tyrosine kinase inhibitor that is highly selective for VEGFRs, and possibly PDGFRs. By blocking these receptors, it inhibits the angiogenesis and vasculogenesis controlled by the agonists of these receptors that modulate CNV. It is currently approved for treatment of renal cell carcinoma that has previously failed 1 year of systemic therapy. The constellation of receptors inhibited by axitinib, however, likely differs from sunitinib. 75 Topical application of 0.5 mg/mL axitinib produced a dose-dependent inhibition of CNV area in a rabbit suture-induced CNV model. 75 Finally, in an alkali burn injury model in rats, axitinib-loaded micelles inhibited CNV without apparent toxicity. 76
Since sunitinib and axitinib are small molecule inhibitors, it is expected that they would transition the epithelium into the stroma when there is an intact epithelium in the cornea. The clinical trials performed thus far on these agents support this likelihood.71–75
Thus, small molecule CNV inhibitors, such as sunitinib, axitinib, and others likely to be developed, are promising agents to inhibit and treat CNV. Future studies should aim to prevent and treat CNV in more complex models, such as CNV triggered by severe infections, alkali burns, or corneal transplant rejections, in both animals and humans. Future clinical trials should be designed to determine how long topical sunitinib or axitinib would need to be continued once CNV is under control after a particular injury.
It should be noted that rho-kinase (ROCK) inhibitors, which will be highlighted in the next section of this review, may also inhibit angiogenesis—at least to some extent. Treatment of vascular endothelial cells with ROCK inhibitor Y27632 was found to inhibit migration and tube formation induced by VEGF. 77 Y27632 also reduced hypoxia-induced angiogenesis in the lung in vivo.78,79 VEGF-induced angiogenesis was also suppressed by ROCK inhibitor fasudil both in vitro and in vivo.80,81 Thus, there could be combined effects of using ROCK inhibitors with more traditional inhibitors of CNV.
Corneal Endothelium/Descemet's Membrane Injury and ROCK Inhibitors
Many severe injuries to the cornea, including chemical burns,5,9 infections, 2 trauma, 82 and even surgeries, such as phacoemulsification, 83 Descemetorhexis without endothelial transplantation, 84 or lamellar corneal endothelial transplantation, 85 injure the corneal endothelium and Descemet's membrane (Fig. 1). These injuries are often associated with posterior stromal haze or scarring fibrosis, and stromal neovascularization may develop.2,5,9,82–84
Descemetorhexis models in rabbits, which tend to develop more fibrosis than humans after similar injuries, not only found severe posterior stromal myofibroblast and fibrosis development but also showed that regeneration of the endothelium and Descemet's membrane over time in rabbits led to a decrease in stromal myofibroblasts and scarring fibrosis.85,86 These observations led to the hypothesis that a pharmacological increase in the proliferation of human corneal endothelial cells could promote Descemet's membrane regeneration and subsequent decreases in myofibroblasts and fibrosis in human corneas with posterior injuries. 86
Corneal endothelial cells have been shown to have limited proliferative potential—with peripheral cells possibly having greater proliferative potential than central cells.87–90 However, several approaches have demonstrated that human corneal endothelial cells actually have considerable regulated proliferative potential that is stimulated by transfection or transduction of the cells with oncogenes, such as SV40 large T antigen or E6/E7.91–94 Expression of these genes in human corneal endothelial cells led to extended-life with the capacity for human corneal endothelial cell proliferation for more than 100 population doublings.91–94 Joyce et al87,88 demonstrated that human corneal endothelial cells are arrested in the G1-phase of mitosis. Studies also showed that TGF beta isoforms from the aqueous humor (or via corneal endothelial cell autocrine mechanisms) likely had a role in this mitotic arrest.88,95–100
Many studies suggested that different species of normal corneal endothelial cells have varied proliferative potential in culture. Thus, bovine, 100 rabbit,95,96,101 and rat 97 were found to grow in culture more readily, whereas cat, 102 monkey, 103 and human88,99,104,105 were reported not to culture as easily. However, Joyce 87 proposed that this difference between studies might be largely explained based on age differences, with laboratory animals tending to be younger. Likely, however, in vivo proliferation of CE cells in all species must be tightly regulated to prevent them from growing over the trabecular meshwork and other vital anterior segment tissues.
Kinoshita and collaborators106–109 pioneered the use of topical ROCK inhibitors, such as H-1152, Y-27632 and ripasudil (Table 1), which stimulate corneal endothelial cell adhesion and proliferation, and inhibition of apoptosis, of primate, porcine, and rabbit corneal endothelial cells in in vitro and in vivo models. For example, in an in vivo rabbit transcorneal endothelial cell freeze injury model, Okumura et al, 106 showed that there were significantly more mitotic corneal endothelial cells in corneas treated either with 50 μL of 0.4% ripasudil four times daily or 0.8% ripasudil two times daily, after the injury. Greater corneal transparency and higher corneal endothelial cell densities were noted in ripasudil-treated compared to vehicle-treated rabbit corneas.
These authors also noted that eyes treated with ripasudil expressed N-cadherin and Na/K-ATPase in almost all corneal endothelial cells, whereas this expression was decreased in corneal endothelial cells in the control eyes. Meekins et al 110 found that topical H-1152 was superior to Y-27632 in stimulating corneal endothelial cell proliferation after endothelial injury in a rabbit model. In that study, two 25 μL drops of H-1152 (1 mM; Enzo) were applied to the treated eyes topically four times daily.
A recent study found that ROCK inhibitor Y27632 also enhanced corneal nerve regeneration in a murine model. 111 Thus, ROCK inhibitors could also be useful in eyes with neurotropic keratopathy. However, further verification of this potential effect of ROCK inhibitors is needed.
Netarsudil 0.02% ophthalmic solution (Table 1) is another ROCK inhibitor that was approved by the FDA for the treatment of open-angle glaucoma or ocular hypertension in 2017. Some investigators have reported pilot studies on the use of netarsudil to treat corneal endothelial disorders through its demonstrated in vitro activity to stimulate corneal endothelial cell adhesion and proliferation, and inhibit corneal endothelial cell apoptosis. Thus, Davies et al 112 reported that the topical application of 0.02% netarsudil beginning after Descemetorhexis without endothelial keratoplasty at the time of cataract surgery significantly reduced the time to corneal clearing and increased corneal endothelial cell counts compared to eyes where the netarsudil treatment was delayed.
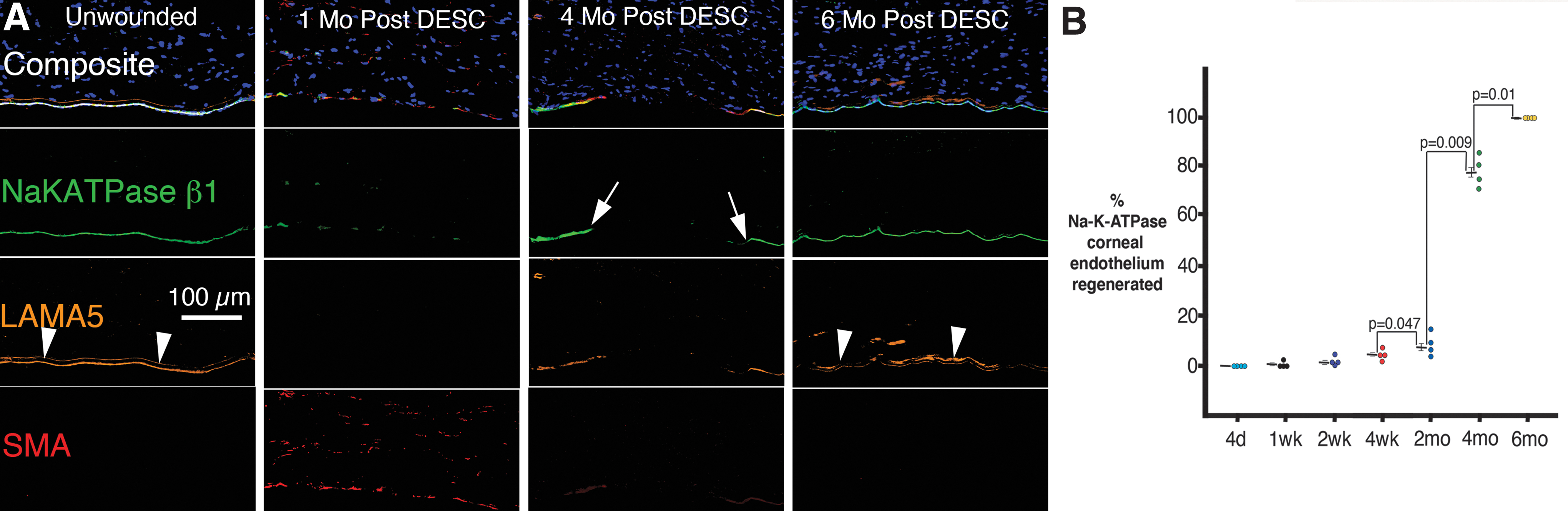
In a prospective clinical trial of topical 0.02% netarsudil versus vehicle once a day for 3 months in symptomatic Fuchs' dystrophy eyes, Price and Price 113 found a reduction in corneal edema and improvement in scotopic corrected distance visual acuity in eyes treated with the netarsudil. Thus, there is clinical evidence that topical ROCK inhibitors could be effective therapeutic agents to address diseases or injuries affecting the corneal endothelium. These modulators could be tested in animal models such as rabbits, where the corneal endothelium is thought to have greater proliferative potential than in humans, because 5–6 months are required for corneal endothelial cells and Descemet's membrane to completely regenerate and stromal fibrosis to decrease without treatment after an 8 mm Descemetorhexis without corneal endothelial transplantation (Fig. 4). 86 ROCK inhibitors could accelerate this regeneration of the corneal endothelium and Descemet's membrane, and thereby more rapidly decrease corneal scarring fibrosis.
Ripasudil likely penetrates the intact corneal endothelium since it has been found to stimulate corneal endothelial cell motility and proliferation in animals with normal corneal epithelium.106–110 Netarsudil also likely penetrates the intact corneal epithelium because endothelial changes have been noted in patients receiving the medication topically.112,113 However, further study is needed to verify netarsudil corneal penetration.
If ripasudil or netarsudil was applied topically to the cornea to augment corneal endothelial cell density, then that density should be monitored with specular microscopy or confocal microscopy to determine when the medication could be discontinued. Ongoing monitoring of corneal endothelial density could be used to dictate whether additional treatment with ripasudil or netarsudil was needed.
Combined Corneal Treatment with Multiple Agents Modulating Epithelial Healing, Stromal Scarring Fibrosis, Neovascularization, and Endothelial Injury
Many small molecules that modulate corneal epithelial healing, myofibroblast-mediated stromal fibrosis, stromal neovascularization, and corneal endothelial cell proliferation are either currently available for clinical use in human eyes or likely to enter clinical trials in the near future. New agents that modulate each of these processes important in the pathophysiological responses to corneal injuries or diseases are also likely to be developed. Some of these drugs are likely to be useful as single agents—for example, ROCK inhibitors may be effective in the treatment of Fuchs' corneal dystrophy112,113 or human recombinant NGF has been shown to be effective in the treatment of eyes with PEDs associated with neurotrophic corneas. 24
Following severe injuries affecting the entire cornea, such as chemical burns or severe infections, however, it is likely that polydrug therapies will be required to address not only endothelial injury but also stromal scarring, CNV and PEDs. Some eyes will still require surgical treatments in addition to these pharmacological approaches to address associated disorders such as limbal stem cell deficiencies or total corneal endothelial destruction. In some of these eyes, penetrating keratoplasty will still be necessary, perhaps followed by pharmacological agents to address epithelial healing, CNV and/or endothelial insufficiency. Thus, it seems likely that many pharmacological agents will soon be available to add to the armamentarium of ophthalmologists for the treatment of corneal injuries and diseases.
Conclusions
Corneal injuries and diseases are commonly associated with pathophysiological processes that decrease vision such as epitheliopathy, PEDs, stromal scarring fibrosis, CNV, and endothelial cell injury. Several pharmacological agents that can be applied topically to the cornea to control these injury responses are either already available for clinical use or will soon enter clinical trials. It is likely that combinations of these medications will provide optimal treatment for these corneal disorders depending on the specific injury or disease.
Footnotes
Acknowledgment
The author is grateful to Lycia Pedral Sampaio, MD, Thomas Michael Shiju, PhD, and Guilherme S. L. Hilgert, MD for work that contributed to this review.
Author Disclosure Statement
The Cleveland Clinic and Steven E. Wilson submitted a provisional patent application for the use of losartan and other angiotensin converting enzyme II receptor inhibitors to prevent and treat scarring fibrosis after corneal injury, surgery, or disease.
Funding Information
Supported by the Department of Defense grant VR180066 (S.E.W.), U.S. Public Health Service grant EY025585 from NEI, and an Unrestricted Grant from Research to Prevent Blindness, New York, NY, USA.