
Abstract
Purpose:
Prostaglandin-associated periorbitopathy in patients with glaucoma is reportedly not caused by EP2 agonist, but it has been a cosmetic problem with prostaglandin F receptor (FP) agonists. In this study, patients with prostaglandin-associated periorbitopathy on FP agonists were switched to EP2 agonist and changes were investigated.
Methods:
Patients complaining of prostaglandin-associated periorbitopathy were included. The FP agonist was switched to EP2 agonist (omidenepag isopropyl), and patients were followed up for 7 months. Frontal photographs were taken at every visit, and objective changes in deepening of the upper eyelid sulcus were assessed by three observers. Subjective questionnaires (self-awareness of deepening of the upper eyelid sulcus, eyelid/peri-eyelid skin pigmentation, eyelash elongation, and conjunctival hyperemia) were acquired at the start and the endpoint. Factors associated with the change of prostaglandin-associated periorbitopathy were investigated using logistic regression analysis.
Results:
Included were 23 eyes of 23 patients (17 women; 60.6 years). At 7 months, objective deepening of the upper eyelid sulcus improved by 76%. The subjective questionnaires showed that deepening of the upper eyelid sulcus improved in 95%, eyelid/peri-eyelid skin pigmentation in 76%. The less extent of myopia was a significant factor in the eyes with improved eyelid/peri-eyelid skin pigmentation. After switching, no change in intraocular pressure or visual acuity was observed (P ≥ 0.22).
Conclusion:
Switching to omidenepag isopropyl increased patient satisfaction and might be the first step to lightening deepening of the upper eyelid sulcus and eyelid/peri-eyelid skin pigmentation. It was suggested that pigmentation may be more easily improved in nonmyopic eyes.
Introduction
Currently, glaucomatous optic neuropathy is only actively treated by lowering intraocular pressure (IOP). There are several methods for lowering IOP, which include pharmacology, laser, and surgery. 1 The first choice among these is generally antiglaucoma eye drops. Prostaglandin F receptor agonists (FP agonists) lower IOP mainly through stimulating aqueous humor outflow from the uveoscleral outflow tract, 2 and as single agents, they have the most powerful IOP-lowering effect among several glaucoma eye drops. 3
Local ocular cosmetic side effects 4 such as conjunctival hyperemia, eyelash elongation, eyelid pigmentation, and deepening of the upper eyelid sulcus (these are so-called prostaglandin-associated periorbitopathy) 5 have been reported to affect glaucoma patients, although there are no major systemic adverse effects associated with FP agonists. The development of fast-onset prostaglandin-associated periorbitopathy has been reported as early as within a month of starting treatment with FP agonists. 5
Prostaglandin-associated periorbitopathy is an unwanted side effect that has recently received attention, because it can significantly change the appearance of the area around the eyes. 6 Deepening of the upper eyelid sulcus includes orbital fat atrophy (ocular retraction), ptosis, and skin retraction. A total of four available FP agonists are reported to cause deepening of the upper eyelid sulcus, 7 but the frequency of onset varies depending on the drug.
In a series of small cases regarding Japanese patients with open-angle glaucoma (OAG), ∼60% of patients were reported to have developed deepening of the upper eyelid sulcus as early as 4 months after switching from latanoprost to bimatoprost. 8 The decrease in the eyelid and orbital adipose tissue volume has been verified histologically 9 and via orbital magnetic resonance imaging, 10 respectively. The FP agonists act on the adipose progenitor cell receptors, activating mitogen-activated protein kinases. Subsequent phosphorylation and inactivation of peroxisome proliferator-activated receptor gamma are believed to inhibit adipocyte differentiation, resulting in decreased fat accumulation in adipocytes. 11
In clinical practice, we often encounter some cases in which IOP measurement using Goldmann applanation tonometry is difficult because of severe deepening of the upper eyelid sulcus where the eyelid skin is not retractable due to eyelid fat loss, which makes obtaining an accurate IOP measurement difficult. 12 In addition, poor IOP control after filtration surgery has been reported in deepening of the upper eyelid sulcus. 13
The FP agonist discontinuation is the only solution to prevent further worsening of deepening of the upper eyelid sulcus, but FP agonists are sometimes difficult to discontinue from the viewpoint of IOP control. However, omidenepag isopropyl, which is a new selective prostaglandin E2 receptor agonist (EP2 agonist) that first became available in Japan in 2018, was seen to be noninferior to latanoprost in terms of its IOP-lowering effect 14 and does not cause adipogenesis suppression, which in turn would cause deepening of the upper eyelid sulcus, 15 eyelash elongation, 16 and eyelid/peri-eyelid skin pigmentation.17,18
We conducted a prospective cohort study that included patients suffering from FP agonist-induced prostaglandin-associated periorbitopathy and reported that switching from FP agonists to omidenepag isopropyl improved deepening of the upper eyelid sulcus in over 70% of patients with glaucoma in 3 months. 19 This time with an extended follow-up period of 7 months, we investigated the changes not only deepening of the upper eyelid sulcus but also eyelid pigmentation, eyelash elongation, and conjunctival hyperemia after switching from FP agonists to omidenepag isopropyl and examined the factors associated with the changes. This report would be the first questionnaire survey of patients' subjective impressions of changes in prostaglandin-associated periorbitopathy.
Methods
This prospective cohort study included clinical data from the records of Japanese patients from Yotsuya Shirato Eye Clinic (Tokyo, Japan) with glaucoma who were recruited between May 2019 and March 2020. All procedures were conducted following the ethical standards of the responsible committees on human experimentation (institutional and national) and with the Helsinki Declaration of 1964, revised in 2013; the protocol was approved by the Medical Corporation TOUKEIKAI Kitamachi Clinic ERB (No. STS06405). Written informed consent was obtained from all patients. The registered UMIN ID is UMIN000036705.
The inclusion and exclusion criteria were described in the interim report. 19 To put it briefly, patients with glaucoma or ocular hypertension who wished to change their glaucoma medication because of complaints of decreased quality of life (QOL) due to FP agonist-induced deepening of the upper The FP agonists were switched to omidenepag isopropyl without a drug holiday after patients had provided written informed consent. Patients were asked to apply one drop of omidenepag isopropyl once daily (morning or evening). Patients using multiple drugs were advised to continue all drugs except for the FP agonists.
Ophthalmological examinations
The IOP was measured five times: day 0 (baseline), 1 month, 3 months, 5 months, and 7 months (last day). Topical anesthesia was applied at each clinic visit (at approximately the same time on the examination day), and two measurements were obtained by Goldmann applanation tonometry (Haag-Streit, Germany) by a well-trained examiner (R.S.). A third measurement was taken if the difference between the two measurements was greater than 2 mmHg. The average value of the two measurements within 2 mmHg was used in the analysis.
Central corneal thickness was measured at baseline and on the last day using a specular microscope (Tomey, Japan). Interpupillary distance was automatically calculated at baseline and on the last day using an autorefractor keratometer (NIDEK, Japan). Best-corrected VA was obtained at baseline and on the last day by Landolt C ring. The presence or absence of macular edema (focal or diffuse) at baseline and on the last day was determined using a fundus optical coherence tomography (macular; Cirrus 6000, Carl Zeiss Meditec, Jena, Germany).
The Humphrey visual field Swedish Interactive Testing Algorithm 30-2 (Humphrey visual field analyzer, Carl Zeiss Meditec) result was adopted for the baseline visual field (fix loss <15%, false-positive <15%, and false-negative <15%).
Frontal photography including eyelids
A frontal face photograph without makeup on the eyebrows or lower eyelids was taken without flash (Sony Cyber-Shot, DSC-WX300, Sony Inc., Tokyo, Japan) with the same settings (shooting mode: auto, distance to the patient: 2 m = 6.56 feet). The baseline photograph served as the baseline; all successive photographs (1, 3, 5, and 7 months) were taken using the same semidark room by the same examiner (R.S.).
Questionnaire of subjective symptoms of FP agonist-related local adverse effects and QOL
A questionnaire was completed by the study participants at baseline and on the last day, which consisted of four items: subjective deepening of the upper eyelid sulcus symptoms, eyelid pigmentation, eyelash elongation, and conjunctival hyperemia. Participants were asked whether they were overly concerned, slightly concerned, or not concerned regarding these items. The participants were asked at the end of the follow-up to rate the degree of change in their condition as follows: much improved, slightly improved, unchanged, and worsened.
Study participants also completed a questionnaire of QOL on the last day that consisted of the following items: appearance (better or worse), eye drop comfort (better or worse), burden (e.g., wiping the eye area clean after eye drops, etc.) associated with eye drops (less or more complicated), and eyedrops can be released into the conjunctival sac with less force (yes or no). Then, at the end of the study, they were asked whether or not the switch in eye drops made them feel motivated to continue treatment well, and whether they would choose to continue treatment with the pre-switch eye drops or omidenepag isopropyl.
Sample size and power analysis
Approximately 85% of patients with deepening of the upper eyelid sulcus who switched from bimatoprost 0.03% to latanoprost 0.005% showed a reduction in deepening of the upper eyelid sulcus at 6 months. 20 We did not specify the FP agonist used in the present study before the switch. There was no information on deepening of the upper eyelid sulcus reduction after switching from FP agonist to omidenepag isopropyl. We established 30 cases in this study to estimate the 95% confidence interval (CI) in the range of 63%–90% assuming an 80% disappearance rate of deepening of the upper eyelid sulcus.
Statistical analysis
We selected the eye with stronger objective deepening of the upper eyelid sulcus judged by the primary care physician in patients for whom both eyes were eligible for analysis. We enrolled the eye with higher IOP at baseline if the degree of deepening of the upper eyelid sulcus was the same, but if the IOP was the same, the right eye was selected. If only one eye was eligible, that eye was enrolled.
The method used to evaluate objective deepening of the upper eyelid sulcus followed that of previous reports.7,8,20,21 The three independent observers (M.A., M.H., and T.F.) compared the 1-, 3-, 5-, and 7-month frontal photographs with the baseline photographs; observers were blinded to the chronologies of the photograph sequences. Changes in deepening of the upper eyelid sulcus were evaluated on a three-point scale (improved, no change, or worsened).
The final judgment was decided through discussion among the observers when the assessment was not unanimous. The percentage of reproducibility between the judgments (among the three observers) was calculated from Fleiss' kappa. The physician in charge of examining a particular patient did not participate in the evaluation.
The number of subjective symptoms was calculated (deepening of the upper eyelid sulcus, eyelid pigmentation, eyelash elongation, and conjunctival hyperemia) at the switching point and at the follow-up's end. The degree of subjective improvement was binarized (either improved or not), and logistic regression analysis was adopted to examine the factors associated with the improved prostaglandin-associated periorbitopathy symptoms.
The explained variables were set as the deepening of the upper eyelid sulcus self-awareness improvement, eyelid pigmentation, eyelash elongation, and conjunctival hyperemia. Gender, age, spherical equivalent, mean deviation, pattern standard deviation, the use of FP agonists duration, central corneal thickness, and interpupillary distance were factors that were adopted as response variables. The IOP at 1-, 3-, 5-, and 7 months were evaluated as compared with the baseline IOP by analysis of variance based on the mixed model.
A paired t test was used to evaluate the change in visual acuity, central corneal thickness, and interpupillary distance. Fundus optical coherence tomography was used to determine the presence or absence of macular edema.
The software used were JMP Pro (version 16.0; SAS Institute, Cary, NC) and IBM SPSS Statistics (version 23.0; IBM Corp., Armonk, NY). The significance level was set at 5%, unless otherwise mentioned.
Results
A total of 23 patients with OAG were enrolled. Of these, 21 were followed up for 7 months. One patient stopped coming to the clinic after the first visit due to the COVID-19 pandemic, and the other patient requested an eye drop other than omidenepag isopropyl at 3 months. Table 1 shows the details of the patients' backgrounds and subjective symptoms at the time of switching. The breakdown was as follows: bimatoprost (n = 9) as prostamide F2α analog, 22 travoprost (n = 9), latanoprost (n = 4), and tafluprost (n = 1) as FP agonists. Self-reported adherence to eye drop use after switching to omidenepag isopropyl was 100% for all patients during the course.
Demographics and Clinical Characteristics of Patients in the Current Study
n = 22.
Acquired from the questionnaire (the results were obtained from 22 cases).
dB, decibel; IOP, intraocular pressure; SD, standard deviation.
Objective deepening of the upper eyelid sulcus improved in 12 eyes (57%; 95% CI, 37% to 76%) at 1 month, in 16 eyes (73%; 52% to 87%) at 3 months, in 17 eyes (81%; 60% to 92%) at 5 months, and in 16 eyes (76%; 55% to 89%) at 7 months. The percentage of judgment reproducibility at 7 months between the three independent observers was 0.47 (95% CI, −0.45 to 1.38). Figure 1 presents one representative improved case.
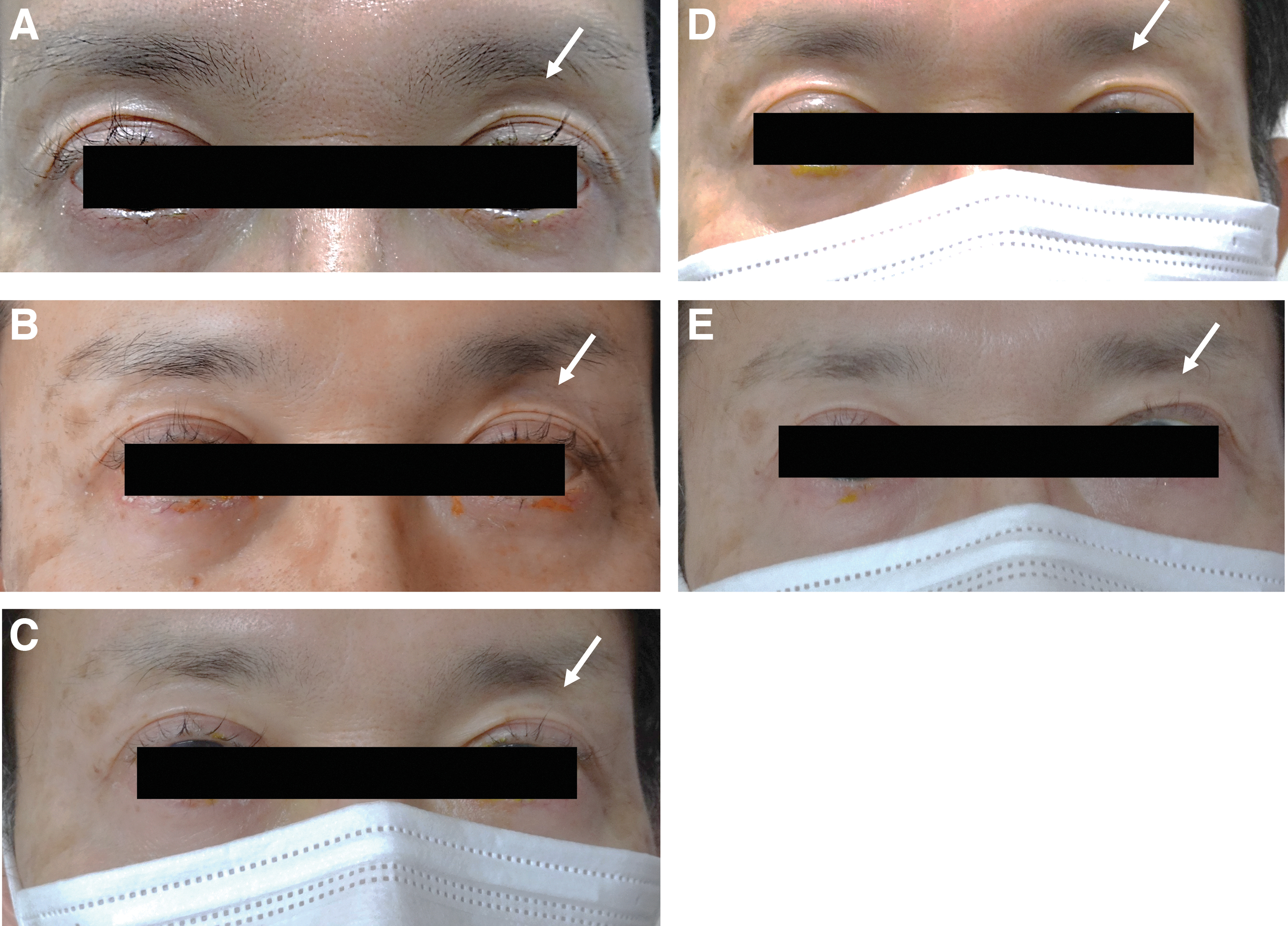
A 58-year-old man experienced alleviation of deepening of the upper eyelid sulcus after switching treatment to omidenepag isopropyl (left eye). This patient showed deepening of the upper eyelid sulcus, especially in his left eye with the use of travoprost ophthalmic solution
The subjective improvement ratio at the end of follow-up was as follows: deepening of the upper eyelid sulcus, 95% (77%–99%); eyelid pigmentation, 76% (55%–89%); eyelash elongation, 43% (24%–63%); and conjunctival hyperemia, 14% (5%–35%). The percentage of patients who were willing to continue treatment after switching eye drops was 52% (32%–73%), and 100% (83%–100%) of the patients preferred continuing omidenepag isopropyl rather than previous eye drops.
Figure 2 showed the subjective percentages for each symptom at the time of switching and at the end of follow-up. The percentage of no concern significantly increased in the end. Spherical equivalent (odds ratio 1.90, 95% CI, 1.17 to 4.72, P = 0.005) was a significantly positive associated factor in the improvement of eyelid/peri-eyelid skin pigmentation in logistic regression analysis (Table 2).
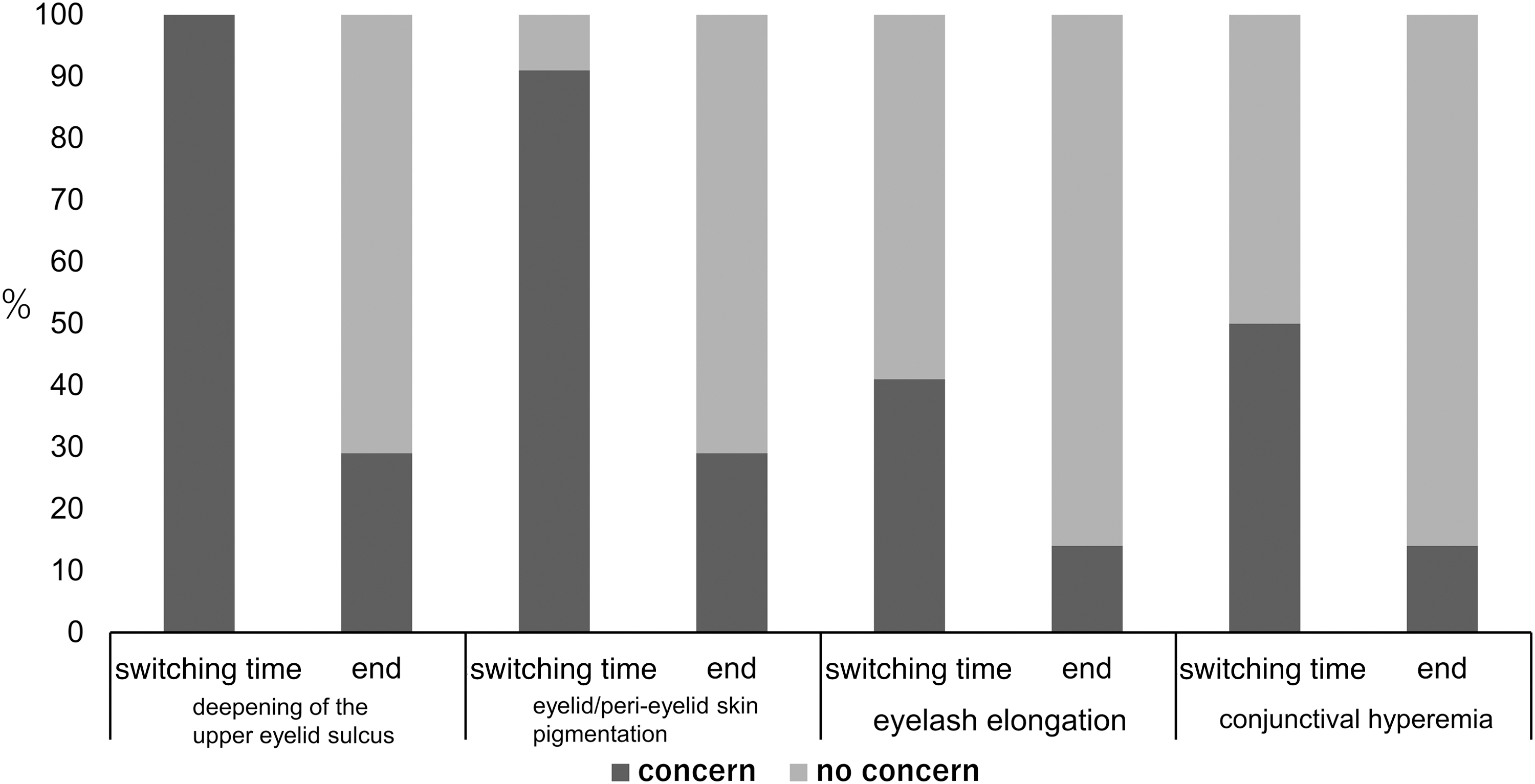
The subjective percentages for each symptom at the time of switching and at the end of follow-up. The subjective symptom of deepening of the upper eyelid sulcus decreased from 100% (black bar) to 29% at the end. Similarly, eyelid/peri-eyelid skin pigmentation decreased from 91% to 29%, eyelash elongation decreased from 41% to 14%, and conjunctival hyperemia decreased from 50% to 14%, respectively. Gray bar indicated as “not concerned.”
Univariate Logistic Regression Results Analysis of Subjective Improved Categories
FP, prostaglandin F receptor; MD, mean deviation; N/A, not available due to a complete separation; PSD, pattern standard deviation.
The mean IOP at switching was 15.3 mmHg (14.0–16.7 mmHg). The mean IOPs were 15.6 mmHg (14.2–16.9 mmHg) at 1 month, 15.6 mmHg (14.3–17.0 mmHg) at 3 months, 16.2 mmHg (14.8–17.6 mmHg) at 5 months, and 15.9 mmHg (14.6–17.3 mmHg) at 7 months (P ≥ 0.22 at each month; adjusted by Bonferroni correction). Changes from switching to the endpoint of ocular factors were as follows: Visual acuity (logMAR visual acuity, from −0.0075 to −0.0097, P = 0.33), central corneal thickness (from 518 to 530 μm, P = 0.003), and interpupillary distance (from 62.8 to 63.2 mm, P = 0.20); there were no cases of macular edema at the start and endpoint of the study.
Lastly, significant improvements in patients' QOL were observed, especially in terms of good appearance after changing eye drop (95%), good eye drop comfort of omidenepag isopropyl (95%), less burden associated with omidenepag isopropyl (75%), and ease of application of omidenepag isopropyl (100%).
Discussion
This study was the prospective FP agonists-related prostaglandin-associated periorbitopathy evaluation that may affect both cosmetic and functional aspects after switching from FP agonists to omidenepag isopropyl. We followed up with the patients for half a year after the switch in line with the previous report. 20 The study revealed that switching to omidenepag isopropyl in patients with FP agonist-induced deepening of the upper eyelid sulcus resulted in a 76% improvement in objective symptoms while maintaining IOP and visual function.
There was a significant improvement in patients' QOL according to the results of the QOL questionnaire, in terms of “good appearance” and “ease of eye drop.” The switch to omidenepag isopropyl when taken together resulted in increased patient satisfaction with improvements in two items in particular: self-awareness of deepening of the upper eyelid sulcus and eyelid pigmentation. We discovered that eyelid pigmentation in nonmyopic eyes might be more likely to fade by switching to omidenepag isopropyl. These results demonstrated that switching from FP agonists to omidenepag isopropyl might be beneficial in terms of reducing the side effects of FP agonists-related objective and subjective prostaglandin-associated periorbitopathy.
Proper management of ocular local adverse effects in glaucoma medications is especially important in terms of maintaining medication adherence. The sooner side effects emerge, the less satisfied patients are with their treatment. This, in turn, leads to glaucoma progression. 23 Prostaglandin-associated periorbitopathy has a significant negative effect on the patient's appearance and the doctor's ophthalmic examination. Patients might find it difficult to maintain a positive attitude toward glaucoma treatment because of the drastic change in their appearance due to the atrophy of the orbital/eyelid fat.
On the medical side, the eyelids cannot be opened sufficiently because of nonretractable skin due to loss of peri-eyelid fat, including the upper eyelid. This not only increases the measurement error of Goldmann applanation tonometry on IOP but also makes it difficult to perform filtration surgery.12,13 Laser suture lysis and needling bleb revision after filtration surgery are also difficult to perform, which results in poor surgical outcomes. Previously, a nearly identical eye condition was termed tight orbit syndrome. 24 Essentially, it is the same medical condition in which obtaining stable IOP control is difficult in patients with glaucoma.
Glaucoma patients must continue IOP-lowering therapy throughout their lives. Prostaglandin-associated periorbitopathy is inevitable to some extent because FP agonists still exist at the core of current medical therapy, but some alternative treatments should be attempted before prostaglandin-associated periorbitopathy deterioration. However, β-blockers and other drugs that are used to avoid prostaglandin-associated periorbitopathy are less effective in lowering IOP than FP agonists.
Omidenepag isopropyl showed noninferiority to FP agonists (latanoprost) in lowering IOP, 14 and this new drug is a promising candidate as an alternative to FP agonists. In addition, it has been reported from the results of basic research that omidenepag isopropyl did not cause fat atrophy, 15 iris pigmentation, 17 and eyelash elongation. 16 These results provide support for the rationale for switching from FP agonists to omidenepag isopropyl in patients with troubling ocular local side effects.
Nearly three-quarters of the cases experienced an improvement in objective appearance at 3 months or later after the switch to omidenepag isopropyl, and surprisingly, subjective symptoms also markedly improved (>90%), even in some cases in which no objective improvement was observed. This was supported by the QOL results questionnaire, which showed that 95% of the patients had felt their appearance improved.
In addition, many patients felt that the omidenepag isopropyl eye drops were more comfortable and easier to use than the eye drops before the switch. This means that patient satisfaction with the treatment was greatly increased after switching. This is supported by the fact that 100% of patients wanted to continue treatment with omidenepag isopropyl rather than previous eye drops after the study period.
The major cosmetic problems are deepening of the upper eyelid sulcus, eyelid pigmentation, eyelash elongation, and conjunctival hyperemia. A thorough explanation is required when initiating the use of FP agonists as first-line drugs for all patients with glaucoma, especially in younger patients, female patients, and patients with unilateral ophthalmic drops. We found that deepening of the upper eyelid sulcus and eyelid pigmentation were highly improved in the present study, based on the patients' responses to the questionnaire survey.
The percentage of improvement in eyelash elongation and conjunctival hyperemia was relatively low, but we believe this was because the subjective rates of eyelash elongation and conjunctival hyperemia were not originally extremely high. It is known that the symptoms of conjunctival hyperemia gradually alleviate with the continued use of eye drops like FP agonists, although there are no reports on changes in eyelash elongation over time.
Conversely, none of our patients with severe deepening of the upper eyelid sulcus, such as a wide distance between the superior orbital bone and the upper eyelid at switching, showed objective improvement after half a year. Liang et al reported a semi-quantitative grading of sunken eyes, but the classification of deepening of the upper eyelid sulcus is difficult to determine quantitatively. 25 It may be difficult to evaluate qualitatively even when there is only a slight amount of change.
The moderate agreement (κ = 0.47) among the three observers in this study was thought to be due to the inclusion of some cases where the photographic judgment was difficult (Supplementary Table S1).
The results of the logistic regression analysis indicated that the decreased degree of myopia was a significant factor related to the improvement in eyelid pigmentation. Generally, the more myopic the patient, the more eyeballs tend to protrude forward. Consequently, the more myopic eye tends to have a thinner epidermis, and pigmentation may be more prominent. Pigmentation may become less noticeable after discontinuation of the FP agonist in low myopia more quickly than in high myopia.
In the present study, no patient showed a significant increase or decrease in IOP after switching. It is safe to assume that IOP was at least maintained without worrying about IOP changes after switching. It has been reported that less frequent side effects such as macular edema 26 and increased central corneal thickness 14 may occur with the use of omidenepag isopropyl. Further accumulation of knowledge is needed because intraocular lens and aphakia, including phakic eyes with a preexisting condition that predisposes the patient to macular edema (diabetic retinopathy, epiretinal membrane, etc.), are conceivable subjects, although there were no cases of macular edema in this study.
A small but significant increase in central corneal thickness (12 μm), which was considered to be within the range of diurnal variation of central corneal thickness, 27 was noted in this study. It is unknown why this variation occurs, but it is generally considered that a value of this magnitude has almost no effect on IOP values. Therefore, this study did not use central corneal thickness to correct the measured IOP values.
Several limitations should be discussed here. Some patients who receive FP agonists did not suffer from deepening of the upper eyelid sulcus or other ocular local side effects subjectively, whereas some patients did not care whether they have deepening of the upper eyelid sulcus. This resulted in a small number of recruited patients and possibly reduced power to detect relevant factors. Second, it was necessary to adjust as there is a difference in the evaluation standards among evaluators, in which there is no quantitative evaluation method. There were no such indicators as having been proposed in recent years. 28
Third, there is the essential question of whether prostaglandin-associated periorbitopathy had really existed at the time of switching. It must be said that it is impossible to know the true status in the absence of photographs when recruited patients originally started FP agonists several years ago. However, it should be noted that patients themselves had a strong dissatisfaction with their appearance (self-declared deepening of the upper eyelid sulcus, 100%) and eyelid hardening. Fourth, we believe that semi-quantitative photography in the examination room is a convenient method, although there is some controversy regarding photographic judgment.
The key to taking photographs with minimal error was thought to maintain the same distance from the patient, keep the same room lighting conditions, and keep a constant shooting mode.
In conclusion, switching to omidenepag isopropyl could improve these symptoms with a high satisfaction rate in patients with glaucoma who developed deepening of the upper eyelid sulcus and eyelid pigmentation by FP agonists. Eyelid pigmentation in nonmyopic eyes was found to be easily ameliorated. Our results suggest that switching to omidenepag isopropyl might be the first step toward a solution for lightening these cosmetic conditions objectively and subjectively while maintaining IOP and visual function.
Footnotes
Acknowledgments
The authors would like to appreciate the participants of this study and Editage for English language editing.
Authors' Contributions
Study conception and design: M.A., S.S.; Acquisition of data: R.S., T.F., H.S., N.N., M.H., S.S., and M.A.; Analysis of interpretation of data: R.S.; Drafting of article: R.S., M.A.; Critical revision: E.M., Y.Y., and M.A.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work, and have given their approval for this version to be published. The moderate agreement (k = 0.47) among the three observers in this study was thought to be due to the inclusion of some cases where the photographic judgment was difficult.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by Santen Pharmaceutical Co., Ltd, Osaka, Japan. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.