
Abstract
Losartan is an angiotensin II receptor blocker (ARB) that impedes transforming growth factor (TGF) beta signaling by inhibiting activation of signal transduction molecule extracellular signal-regulated kinase (ERK). Studies supported the efficacy of topical losartan in decreasing scarring fibrosis after rabbit Descemetorhexis, alkali burn, and photorefractive keratectomy injuries, and in case reports of humans with scarring fibrosis after surgical complications. Clinical studies are needed to explore the efficacy and safety of topical losartan in the prevention and treatment of corneal scarring fibrosis, and other eye diseases and disorders where TGF beta has a role in pathophysiology. These include scarring fibrosis associated with corneal trauma, chemical burns, infections, surgical complications, and persistent epithelial defects, as well as conjunctival fibrotic diseases, such as ocular cicatricial pemphigoid and Stevens–Johnson syndrome. Research is also needed to explore the efficacy and safety of topical losartan for hypothesized treatment of transforming growth factor beta-induced (TGFBI)-related corneal dystrophies (Reis–Bu¨cklers corneal dystrophy, lattice corneal dystrophy type 1, and granular corneal dystrophies type 1 and type 2) where deposited mutant protein expression is modulated by TGF beta. Investigations could also explore the efficacy and safety of topical losartan treatments to reduce conjunctival bleb scarring and shunt encapsulation following glaucoma surgical procedures. Losartan and sustained release drug delivery devices could be efficacious in treating intraocular fibrotic diseases. Dosing suggestions and precautions that should be considered in trials of losartan are detailed. Losartan, as an adjuvant to current treatments, has the potential to augment pharmacological therapeutics for many ocular diseases and disorders where TGF beta plays a central role in pathophysiology.
Introduction: The Long Road to Discovery
When I opened my first research laboratory as an assistant professor at UT Southwestern in 1990, I decided to focus my future work on cell and molecular biological investigations of growth factors, cytokines, and their receptors' expression and functions in the cornea since I had become fascinated by the recently published (1989) transforming growth factor (TGF) beta-1 work of Plouët and Gospodarowicz 1 and realized little work had been reported on the expression and functions of any growth factors in the cornea. Our first articles on corneal expression of TGF beta in the cornea soon appeared in the literature.2–6 For a time, we became preoccupied with other growth factor–cytokine systems in the cornea besides TGF beta, including hepatocyte growth factor (HGF, also called scatter factor), keratinocyte growth factor (KGF, also fibroblast growth factor-7), and Fas ligand, and the receptors in these systems, 7 but remained interested as the work of other investigators and their teams, such as Gregory S. Schultz, Scheffer C.G. Tseng, James V. Jester, M. Elizabeth Fini, Shigeru Kinoshita, and others, was presented at meetings and appeared in the literature.8–14
Around this same time, beginning in 1987, James V. Jester, Winston W. Kao, Sandra Masur, and their colleagues, published works on corneal myofibroblasts.15–17 There was a clear overlap between the corneal TGF beta and myofibroblast areas of research because of the demonstrated importance of TGF beta in the biology of myofibroblasts, and work from many laboratories that is beyond the scope of this review to detail, mushroomed in the literature.
In 1998, Jester and his coworkers published a fascinating study in rabbits showing that a neutralizing antibody to TGF beta applied topically to injured corneas reduced keratocyte activation and myofibroblast transformation and stromal fibrosis. 18 I was intrigued by the work, but remember concluding it was not likely to be of great clinical benefit because antibodies are large molecules that were unlikely to penetrate into the corneal stroma when the epithelium was intact. It would be over a decade later, in 2011, before Bela K. Ambati and I collaborated to find that plasmid vectors that express genetically altered receptors that bound TGF beta and included a KDEL endoplasmic reticulum retention signal, which interfered with normal signaling of the bound growth factors, decreased stromal haze and myofibroblast density compared with control vectors in the corneas after haze-generating irregular phototherapeutic keratectomy (PTK) in mice. 19 That same year, as a devoted reader of weekly issues of Science, I came upon an article that demonstrated in a mouse aortic aneurysm Marfan's syndrome model that losartan, an angiotensin II receptor blocker (ARB), attenuated canonical TGF beta signaling in the aorta by inhibiting activation of the extracellular signal-regulated kinase (ERK). 20
The article especially intrigued me because I was (and still am) taking oral losartan for hypertension. I remember being irked (pun intended) at the time that I did not know even more about signal transduction pathways, so I fully understood all the complexities of the article. I was busily funded by NEI for other studies at the time, including many studies on epithelial basement membrane (EBM) regeneration and the role of the EBM in modulating TGF beta in the stroma,21–29 but I tucked that tidbit of information away in my hippocampus and cerebral cortex.
Around the spring of 2017, while still funded by the same NEI grant I nurtured for 28 years (up until 2021), but anxious about my funding future, I decided for the first time to submit a grant to the Department of Defense (DOD) Vision Research Program (VRP). Several of my postdoctoral fellows and I had worked on a series of experiments where we demonstrated that when an 8 mm disc of corneal endothelium and Descemet's membrane was excised (Descemetorhexis), severe posterior corneal scarring fibrosis and myofibroblasts developed by 1 month after injury in rabbits. 30 I decided to focus the aims of that grant on studying the longer-term healing response after Descemetorhexis in rabbits (out to 6 months), 31 and then to determine whether topical, oral, or combined topical and oral losartan would decrease that posterior scarring fibrosis. 32 I proposed also to evaluate the efficacy of the losartan, with or without corticosteroids, in corneal scarring fibrosis that occurs after severe alkali burn injuries. 33
We were fortunate that DOD grant, VR180066 “Corneal basement membranes and injury-related scarring” was funded. In the second year of those studies, I still remember the excitement my postdoctoral fellows and I experienced at seeing the obvious topical losartan effect on the Descemetorhexis scarring fibrosis in rabbits (Fig. 1), 32 but then not being able to talk about it, present it, or publish it until provisional patents covering the invention were submitted by the Cleveland Clinic.

Images from representative corneas from the first experiments on the efficacy and safety of topical losartan used to treat stromal scarring fibrosis, in this case in rabbits, supported by a Department of Defense grant because of interest in posterior corneal injuries that could occur in military personnel in combination with anterior corneal trauma or chemical exposures.
32
One month was chosen as the treatment time because that is when prior studies showed stromal fibrosis peaked in this rabbit model.
31
In 1 eye of rabbits in surgery groups, an 8 mm diameter removal of the central Descemet's membrane and the attached corneal endothelium (DMR) was performed. Standardized slit lamp photographs of representative unwounded sham surgery corneas and corneas at 1 month after the DMR and treatment with topical and/or oral losartan solutions or the vehicle solutions beginning after surgery are shown. The sham unwounded control (Con) cornea groups were treated with
In some ways, God smiled upon us. The funding was only sufficient to study the results of losartan application until 1 month after the injury (research rabbits now cost ∼$400 each and per diem care is now $5.42, and steadily increasing), but it turned out that was enough time to demonstrate efficacy. 32 Also, when deciding on what topical dosage of losartan to use in the rabbit experiments, we performed losartan solubility studies in balanced salt solution (BSS) using tablets we ground up with a mortar and pestle. It turned out that powder was soluble to ∼1 mg/mL before precipitation occurred. Knowing that TGF beta regulates many normal functions in corneal cells, I decided on a lower concentration of 0.4 mg/mL for the initial experiment, not realizing until later that those pills were only 25% losartan and 75% “excipients,” so the actual losartan concentration was 0.1 mg/mL in the Descemetorhexis experiment 32 and 0.2% in the alkali burn study where we doubled the concentration after seeing no toxicity in the first series. 33 But it worked!
However, we did not realize the true concentration of losartan used in those experiments until the articles were published for 8 and 4 months, respectively (we subsequently published corrigendums for both articles correcting the actual dosage of losartan that was used). We also fortunately decided to monitor EBM component collagen type 4 protein in those corneas using immunohistochemistry, which provided strong evidence (to be described in more detail later) that the topical losartan penetrated through the intact epithelium and EBM, and into the stroma, all the way to the posterior surface of the cornea.
Several of my former Brazilian fellows, now back home in practice in Rio de Janeiro and Sao Paulo, Brazil, where oral losartan is also extensively used to treat hypertension, saw the early publications, and began to use topical losartan to treat corneal scarring fibrosis in a small number of patients. The compounding pharmacies the Brazilians worked with, obtained pure losartan powder and prepared actual 0.8 mg/mL losartan in BSS (1.27 M NaCl, 30 mM NaH2PO4.H2O and 70 mM Na2HPO4.7H2O, adjusted to pH 7.0) or normal saline (O.9% NaCl adjusted to pH 6.7–7.0) with treatment given 6 times per day for at least 6 months; and again, it worked! 34
Additionally, it worked without any signs of toxicity, putting topical losartan on the road to clinical usage in the cornea and eye. So, that is a brief history of the development of topical losartan. More of the details will come out, however, in the following sections.
Corneal Haze Fibrosis Pathophysiology: TGF Beta Sources and Activation
A brief discussion of the pathophysiology of corneal haze fibrosis will facilitate understanding of the effects of losartan in injured corneas. The EBM and Descemet's basement membrane are critical guardians of TGF beta effects on keratocytes and corneal stroma in the normal, unwounded transparent cornea.25–33,35,36 After corneal injury, depending on the type and extent of injury, TGF beta-1 and TGF beta-2 enter, and are activated 37 in the corneal stroma, with major sources of the growth factors being the epithelium, tears, aqueous humor, and residual endothelial cells, although invading bone marrow-derived cells that enter the stroma after injury may also contribute.32,33,35
This influx and activation of TGF beta isoforms (including TGF beta-3, 37 although the in vivo effects of TGF beta-3 remain controversial37,38), trigger the keratocytes proximate to the site of injury to commence their developmental transition into myofibroblasts, 39 along with infiltrating bone marrow-derived fibrocytes. 40 A competition of sorts ensues in the affected tissue, between the efforts of residual keratocytes–corneal fibroblasts and the developing myofibroblast precursor cells.
If the EBM (and/or Descemet's membrane) regenerates in a timely manner, typically a few weeks to a month, depending on the injury and the species, then stromal entry/activation of TGF beta-1 and TGF beta-2 declines, and the precursors undergo apoptosis and/or revert to their original phenotype. If, however, the EBM and/or Descemet's membrane does not regenerate, then the precursors and mature myofibroblasts persist and the latter excrete large amounts of disordered extracellular matrix (ECM) that, along with the relatively opaque myofibroblasts themselves, 41 forms the haze or scarring fibrosis (Fig. 1) seen at the slit lamp or with anterior segment optical coherence tomography.
Losartan, after it enters the stroma, rallies as it were to support the corneal fibroblasts that are striving to cooperate with the epithelium in regenerating the EBM (or Descemet's membrane)25–33,35,36 and to produce non-basement membrane collagen type 4 that directly binds TGF beta-1 and TGF beta-2 and prevents the growth factors from binding their cognate receptors expressed by keratocytes, corneal fibroblasts, fibrocytes, and myofibroblasts.31,32,42 Thus, as was mentioned earlier, losartan was shown to inhibit the activation of ERK. 20 Losartan could have other effects on TGF beta signal transduction yet to be characterized, but regardless of the global effects of angiotensin II receptor inhibition of that signaling, the end result is the myofibroblast precursors and mature myofibroblasts are deprived of requisite TGF beta stimulation and either die by apoptosis or revert to corneal fibroblasts.
Topical losartan also impedes corneal fibroblast production of non-BM collagen type 4 since TGF beta upregulates that expression too, 32 but that downregulation of tissue collagen type 4 does not appear to compromise the disappearance of the myofibroblasts or their precursor cells.32,33 However, the decrease in collagen type 4 expression that can be detected all the way to the posterior surface of the cornea by immunohistochemistry,32,42 provides direct evidence of losartan's effects on the full-thickness stroma after topical surface application, even if the epithelium and EBM are intact.
Myofibroblast Biology
Myofibroblasts, 43 the cells that produce fibrosis, are fascinating cells that have functions in all organs that include contracting wounds, like lacerations in the cornea, and buttressing injured tissues that would otherwise compromise organ integrity. 16 Functions of corneal myofibroblasts also include production of collagenases and metalloproteinases involved in tissue remodeling, the expression of toll-like receptors that likely have critical roles in the clearance of bacteria and viruses causing corneal infections, and the production of various growth factors, cytokines, and chemokines that regulate stromal cells, including other myofibroblasts. 43
Myofibroblasts are dependent on ongoing and adequate levels of TGF beta, or they undergo apoptosis. 43 Some in vitro work has suggested reversion back to corneal fibroblasts. 45 IL-1alpha or IL-1beta triggers the death of myofibroblasts in vitro and TGF beta-1 reduces this IL-1 effect on cell death. This is another example where TGF beta-1 and IL-1 have opposing effects in the cornea 44 —in this case on myofibroblast viability. The working hypothesis is that paracrine IL-1 produced by other stromal cells, such as corneal fibroblasts, or autocrine IL-1 produced by the myofibroblasts themselves, triggers myofibroblast apoptosis when that signaling is unopposed by sufficient TGF beta-1 or TGF beta-2 signaling.43,44 Interference with TGF beta signaling and resulting myofibroblast apoptosis is thought to be the primary mechanism through which losartan effects on myofibroblasts and tissue fibrosis is mediated.32,33,46
Fibrotic tissue in the cornea is not static in terms of cellularity. 30 Rather, precursor cells and mature myofibroblasts continually undergo mitosis and apoptosis within and surrounding the area of fibrosis in the cornea and it appears to be the ratio of mitosis/apoptosis that determines whether myofibroblasts and fibrosis are increasing, persisting unchanged, or decreasing in a particular fibrotic cornea. 30 Fibrosis that has persisted in a cornea for many months following injury is populated with myofibroblasts, which maintain the fibrosis and prevent reabsorption and remodeling by corneal fibroblasts and keratocytes, 43 although further investigation is needed to demonstrate this is true of corneal scars that have persisted for years or decades. This dynamic nature of the corneal fibrotic scar is why topical losartan could potentially impact scarring fibrosis that has been present for years in a particular cornea, regardless of the original inciting injury or disease.
The 2 major precursors for corneal myofibroblasts that have been best characterized are keratocytes/corneal fibroblasts 47 and bone marrow-derived fibrocytes.40,48 There are potentially other precursors for myofibroblasts in the cornea that have been better characterized in other organs, including nerve-associated Schwann cells49,50 and blood vessel-associated pericytes.51,52 Finally, epithelial mesenchymal transition53–55 and endothelial mesenchymal transition56,57 have been reported in some studies.
Why are there so many potential precursors for myofibroblasts in the cornea and other organs? Myofibroblasts from different precursors are not created equal even though they are all TGF beta dependent for survival. In a proteomic study of proteins expressed by myofibroblasts derived from corneal cells compared with those derived from bone marrow-derived cells, 673 differentially expressed proteins were identified and assessment with Ingenuity Pathway Analysis suggested progenitor-dependent functional differences between these 2 types of myofibroblasts. 58
In an in vitro study of mouse myofibroblasts derived from corneal fibroblasts or bone marrow-derived cells, it was found that the percentage of alpha-smooth muscle actin (α-SMA)-positive myofibroblasts generated was higher when both cells were cocultured together (juxtacrine) as compared with when bone marrow-derived cells and mouse corneal stromal fibroblasts were cocultured in different compartments of the Transwell System (paracrine). 59 This suggests that interaction between myofibroblasts derived from different precursors may augment the fibrosis response and the ratios of myofibroblasts derived from alternative precursors in different individuals or organs could differ.
Losartan and Other ARBs: Corneal Pharmacokinetics, Mechanism of Action, and Potential Toxicity
There are several other ARBs that have been identified besides losartan, including telmisartan, valsartan, olmesartan, candesartan, irbesartan, eprosartan, azilsartan, and the active losartan metabolite EXP-3174. 60 These alternative antagonists have differences in their pharmacokinetics and other properties, and their differing potential effects on myofibroblasts and fibrosis could be exploited in studies on the prevention and treatment of myofibroblasts and fibrosis associated with many disparate corneal disorders and diseases. Just one example of these differences will illustrate this heterogeneity for the purposes of this review. Losartan is a competitive antagonist of angiotensin II receptor. 60 EXP-3174, the metabolite of losartan, however, is a noncompetitive antagonist of angiotensin II receptor with a potency estimated to be 33-fold greater than losartan in the antagonism of the angiotensin II receptor-mediated contraction of rabbit aortic strips in vitro. 61 So, the overall effects of these 2 inhibitors could be different. EXP-3174, however, is insoluble in BSS or normal saline, and would, therefore, require alternative vehicles.
We have performed some unpublished preliminary studies on other drugs in this group, but differences in solubility in BSS, in vivo safety profiles, and other factors led us to focus on losartan for the early experiments. Additional investigations to explore these differences between losartan and other members of this group may lead to important insights into the pathophysiology of corneal fibrosis.
As was mentioned previously, originally losartan was found to attenuate canonical TGF beta signal transduction in the aorta by inhibiting activation of ERK through phosphorylation. 20 Some studies have explored losartan effects on other signal transduction molecules related to TGF beta-signaling, including P-Smad2/3, Smad7, Smurf2, and Smurf1,62–65 but the precise mechanisms for losartan or the other ARBs remain enigmatic, with the majority of studies in different organs merely referring to losartan's “inhibition of TGF beta signaling.”
With regard to losartan treatment of corneal fibrosis, desirable characteristics include high solubility in BSS (up to over ∼500 mg/mL, as the solution becomes increasingly more viscous), efficacy at low concentration (0.1 mg/mL, 32 0.2 mg/mL, 33 and 0.8 mg/ml 34 ), penetration of the intact corneal epithelium and EBM into the stroma to the most posterior cornea, 32 and no apparent ocular surface toxicity in either animal models32,33 or the first human case report. 34 Importantly, losartan can cause serious (possibly fatal) harm to an unborn baby if used during pregnancy, so potential patients must be screened for the possibility of pregnancy.
In both initial rabbit studies of topical losartan treatment of corneal fibrosis, the drug solution was applied 1 drop (50 μL) 6 times per day for the 1-month duration of the studies.32,33 Similarly, in the human case report 1 drop of 0.8 mg/mL losartan was initially applied 6 times per day for several months before being decreased to 4 times a day for the duration of treatment after complete resolution of the scarring fibrosis was noted. The question always arises as to whether increasing the dosage of losartan or the frequency of administration might augment the efficacy of topical losartan in treating corneal scarring fibrosis? I ardently recommend against such increases until they are thoroughly evaluated in animal models and clinical trials because such increases are likely to augment penetration of losartan into the eye. While it is apparent that TGF beta modulates the pathophysiology of corneal myofibroblasts and fibrosis, it also likely regulates normal cellular functions in many tissues and impeding these functions could theoretically lead to unforeseen effects and complications in the trabecular meshwork, lens, retina, and other ocular tissues.66–70
Conversely, it is possible that losartan could have a role in the treatment of TGF beta-mediated pathophysiology in these other ocular tissues, but animal testing followed by clinical trials would be prudent.66–70
How long should topical losartan be continued in a treated eye? As of yet, there is no definitive answer to that question. However, the underlying pathophysiology of corneal scarring fibrosis provides some clues. In many cases, the development of corneal scarring fibrosis is related to defective regeneration of the EBM and/or Descemet's membrane.32,33,35,36 Thus, while topical losartan may decrease myofibroblasts and fibrosis rather quickly in a particular eye, it likely will take much longer for the defective EBM and/or Descemet's membrane to fully regenerate. If the basement membrane(s) have not regenerated, then I hypothesize that scarring fibrosis is likely to recur once the losartan is stopped since TGF beta-1 and/or TGF beta-2 will continue to pass into the stroma and drive myofibroblast development. It has, therefore, been my recommendation to continue the topical losartan, perhaps at decreased frequency, for 6 months after there has been substantial clearing of the scarring fibrosis, and then to observe the cornea over time by slit lamp examination. If the scarring fibrosis begins to recur, then longer treatment with topical losartan will likely be necessary.
I anticipate that the EBM and/or Descemet's membrane will never adequately regenerate in some eyes and that repeated recurrence will be noted. In such cases, the clinician will probably need to consider other treatments, including surgeries such as lamellar keratoplasty or penetrating keratoplasty, rather than permanent treatment with topical losartan.
Disorders and Diseases of the Cornea Where Topical Losartan Has Potential to Provide Clinically Effective Treatment
This discussion will begin with disorders where topical losartan is not likely to be effective and/or treatment is unnecessary. A prime example is corneal haze attributable to corneal fibroblasts, which are themselves opaque due to downregulation of corneal crystallins 41 and produce limited amounts of disordered ECM.42,43 This would include normal course photorefractive keratectomy (PRK), riboflavin–ultraviolet (UV) crosslinking surgeries, and other disorders where mild transient stromal haze is generated and typically resolves spontaneously over time. Also, disorders such as blepharokeratoconjunctivitis that tend to be highly responsive to topical corticosteroids and antibiotics would usually not need treatment with topical losartan. However, disorders such as these occasionally develop persistent epithelial defects (PEDs) or transition into more severe vision-compromising scarring fibrosis where topical losartan could be used for treatment.
Some corneal stromal fibrosis cases that are mediated by myofibroblasts might not respond to topical losartan treatment for some unknown pathophysiological reason. It is just as important to report these cases, so over time we can better understand the limitations of losartan treatments.
Using concentrations of losartan above the recommended 0.8 mg/mL in BSS could also affect TGF beta signal transduction in normal cells and tissues in an unpredictable way and even produce worsening of stromal fibrosis by unknown mechanisms. Clinicians should refrain from using concentrations of losartan that have not been tested in animal models or previously reported in human cases. Concentrations between 0.1 and 0.8 mg/mL have worked well in rabbits and humans. Using higher dosages in an attempt to further suppress TGF beta signaling is asking for trouble until those concentrations have been tested in animal models. Changes in the formulation of the losartan drops, including changes in pH to other than the pH 6.7–7.0 used in rabbit studies, could also affect the efficacy of treatment, trigger unforeseen complications, and/or produce discomfort on application to patient eyes.
For each of the diseases and disorders that will be discussed (Table 1), even if this is not repeated in each section, it is recommended that formal clinical trials with Investigational New Drug and Investigational Review Board approval be performed to establish efficacy and safety. Some of these conditions are relatively rare and will require multicenter cooperation for adequate number of patients to be studied. Study designs where vehicle control patients later become eligible for topical losartan treatment might be considered.
Topical Losartan Treatments for Ocular Fibrosis in Clinical Trials: Animal Studies or Human Case Reports, and Hypothetical Treatments for Ocular Disorders
Many other potential etiologies for corneal scarring fibrosis are not included in this table.
DMEK, Descemet's membrane endothelial keratoplasty; DSAEK, Descemet's stripping automated endothelial keratoplasty; EKC, epidemic keratoconjunctivitis; H, Hypothetical; HSV, herpes simplex virus; LASIK, laser-assisted in situ keratomileusis; PRK, photorefractive keratectomy; TGFBI, transforming growth factor beta-induced.
PRK late haze that develops typically 3–4 months after normal PRK in humans, has become much less common and problematic, since the use of mitomycin C at the time of surgery was adopted for routine care.71–73 However, despite mitomycin C treatment, infrequent patients develop vision-compromising “breakthrough haze.” 74 PRK late haze, including breakthrough haze, is mediated by the development of myofibroblasts 72 and is likely to be responsive to topical losartan treatment. The underlying abnormality in these patients is defective regeneration of the EBM.21,25,35,36 It is recommended, therefore, that topical losartan treatments continue for several months after clearing of fibrosis haze. The recurrence of haze would indicate the EBM remains defective and that topical losartan treatment must resume for a longer period of time. Thus, the clinical course in each case will dictate the duration of treatment. Topical losartan was found to be effective in decreasing corneal opacity and myofibroblasts in a rabbit study of high-correction PRK. 75
It is anticipated, however, that the majority of refractive surgeons will continue to use mitomycin C treatments at the time of surgery to remove patient compliance as an issue, especially since few, if any, complications have been noted following this use over the past 20 years.
Central corneal scarring fibrosis can also occur after other refractive and corneal surgical procedures, including complicated laser-assisted in situ keratomileusis (LASIK) and small incision lenticule extraction (SMILE). The first human case of successful treatment of corneal scarring fibrosis after LASIK surgery complicated by a free cap and severe diffuse lamellar keratitis was recently published (Fig. 2). 34 If the scarring fibrosis in a particular case is due to the development of myofibroblasts and the disordered ECM these cells produce, then topical losartan treatment could potentially be useful in decreasing or eliminating the scarring fibrosis and improving visual function.
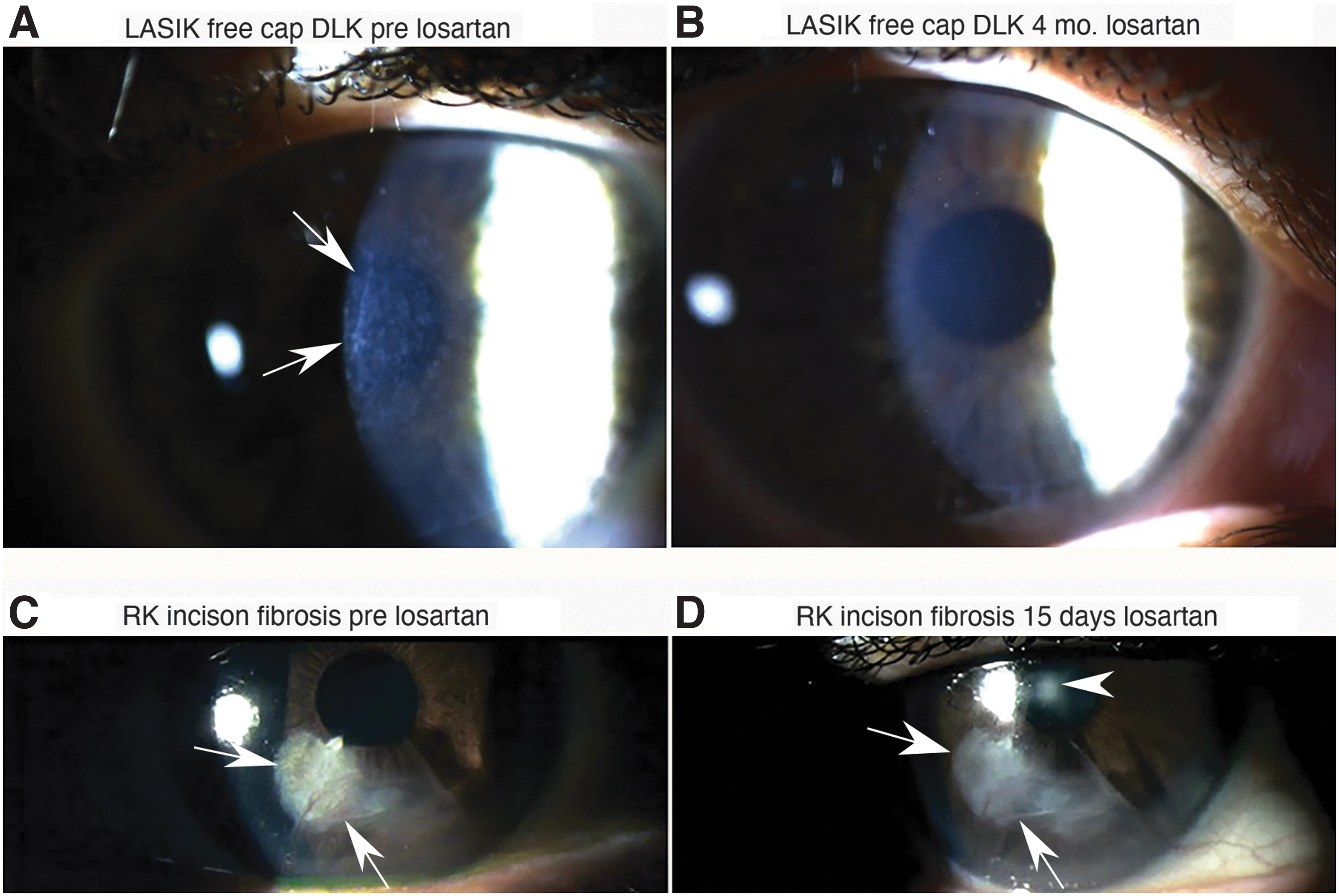
Losartan treatment of refractive surgery complications.
In some eyes, especially with very severe inciting injuries, EBM and/or Descemet's basement membrane may never regenerate, leading to repeated recurrence of scarring fibrosis. In such eyes, surgical treatments, such as lamellar keratoplasty or penetrating keratoplasty may be needed, although low-frequency topical losartan could be effective long term in these eyes if unforeseen toxicities are not noted as larger number of patients are treated. This reinforces the importance of future IRB-approved clinical trials and FDA approval for topical losartan treatments in PRK and other disorders and diseases.
PEDs, often associated with neurotrophic corneas from disorders such as herpes zoster virus ophthalmicus, herpes simplex virus (HSV) keratitis, trigeminal nerve injury, and diabetes mellitus, may benefit from topical losartan treatment. Although topical Oxervate (recombinant human nerve growth factor) is often effective to facilitate crucial closure of the epithelial defects, 76 these corneas are usually found to have vision-compromising scarring stromal fibrosis even after epithelial closure, especially since definitive treatment is often delayed for months. We have found that cases of spontaneous PEDs occurring after PRK in rabbit models have myofibroblasts populating the anterior stroma within the defect (Fig. 3). 77 Six more rabbit PEDs after PRK are being studied from a subsequent series and all have anterior stromal myofibroblasts in the PEDs (Unpublished data; Sampaio LP, Wilson SE, 2022).

PEDs and myofibroblasts in corneas.
The presence of myofibroblasts within PED may itself impede epithelial closure and maturation since these cells apparently do not produce HGF and KGF that are produced by corneal fibroblasts to modulate corneal epithelial proliferation, migration, differentiation, and apoptosis.6,78
Also, myofibroblasts have been shown to directly inhibit corneal nerve regeneration through TGF beta-mediated processes. 79 These findings suggest that combined topical Oxervate and topical losartan treatment could potentially provide the most effective treatment to both facilitate the closure of corneal epithelial defects and to decrease scarring fibrosis in corneas with PEDs, regardless of underlying etiology. Clinical trials are needed to demonstrate the efficacy and safety of this combined therapy.
Recurrent HSV keratitis is often associated with severe corneal scarring and vision loss. 80 These infections produce corneal damage that is a combination of direct viral cellular injury and the immune response to the viral agent. Currently, care is typically provided with topical or oral antiviral medications, such as acyclovir and valacyclovir, and judicious use of topical corticosteroids, and some of these eyes become dependent on at least low-frequency ongoing corticosteroids to control inflammation. 80 Despite treatment, corticosteroid-unresponsive corneal scarring often develops that is attributable to myofibroblast generation and persistence, 81 with possible underlying defective EBM regeneration. Topical losartan treatment could be an effective addition to antiviral and corticosteroid treatment based on the pathology of the corneal scarring in these corneas, and clinical trials are needed to investigate safety and efficacy of multidrug therapy for this troublesome malady.
Bacterial keratitis caused by numerous pathogens commonly generates corneal scarring fibrosis that impairs vision. 82 Myofibroblasts were prominent in scarred corneas in a Pseudomonas aeruginosa model in rabbits, 26 and likely myofibroblasts are associated with the corneal scarring associated with all bacterial corneal ulcers. The mainstay of initial treatment of these infections will continue to be appropriate antibiotics and prudent use of corticosteroids, but topical losartan could be a useful adjuvant to control scarring fibrosis typically noted after these infections. Since myofibroblasts commonly persist after the infection is controlled, topical losartan could be efficacious for treatment of scarring fibrosis months, or even years, after the microbial infections. Once again, future clinical trials and experience will help establish the timing of introduction and duration of treatment needed for optimal topical losartan therapy.
There are many other ocular infections where topical losartan could be a beneficial adjuvant to traditional antimicrobial therapies, including herpes zoster virus, fungus, acanthamoeba infections, and others. Topical losartan could be an effective adjuvant to treat corneal scarring fibrosis in each of these conditions and clinical trials and experience will be needed to establish the safest and most effective approaches. Importantly, after the infectious agent is eliminated by antimicrobials, corneal scarring is likely maintained by persistent myofibroblasts for months or years after all of these infections. Therefore, topical losartan could be beneficial in reducing scarring months or years after the corneal infection is eliminated.
Corneal lacerations, both traumatic and surgical, generate stromal myofibroblasts. 16 Examples include traumatic lacerations and surgical incisions, such as radial keratotomy, LASIK flaps, and penetrating keratoplasty donor–recipient interfaces. A corneal laceration, depending on whether or not it was tightly sutured, is initially filled with an epithelial plug that over time is replaced with fibrotic tissue that includes myofibroblasts that contract the injury.83,84
In the early period after lacerations or incisional surgical procedures, topical losartan should probably be avoided so the myofibroblasts that are generated can perform this function. After a period of at least a few months following surgery, however, topical losartan might be useful in cases with hypertrophic scars that are affecting vision. Even a year later, a peripheral laceration or incision can develop progressive stromal fibrosis, with or without neovascularization. In these cases, topical losartan can be effective in decreasing fibrosis, and possibly associated neovascularization. The effect of topical losartan should be monitored carefully in these eyes and discontinued when sufficient improvement in vision is noted before the integrity of the scarred incision is compromised.
Descemet's membrane, among its other important functions, modulates the entry of TGF beta-1 and TGF beta-2 into the stroma from the aqueous humor and corneal endothelium. 85 After removal of a portion of corneal endothelial–Descemet's membrane complex (Descemetorhexis) massive posterior stromal fibrosis occurs in the rabbit by 1 month after the procedure.30,31 Admittedly, corneal injuries in rabbits tend to generate greater fibrosis than similar injuries in humans, but clinically significant posterior fibrosis has also been noted after Descemetorhexis without graft placement in humans. 86
The author has noted posterior stromal fibrosis after Descemet's stripping automated endothelial keratoplasty (DSAEK) and Descemet's membrane endothelial keratoplasty (DMEK), especially in areas where the transplanted tissue did not precisely cover the stromal defect left after removal of the recipient Descemet's membrane–endothelial tissue or became displaced postoperatively. Posterior fibrosis can also occur after phacoemulsification burns, HSV endotheliitis, and other posterior surface injuries, and these could also be treated with topical losartan if vision is compromised.
Descemetorhexis without graft placement in rabbits was the first animal model in which the efficacy and safety of topical losartan was demonstrated at a dosage of 0.1 mg/mL 6 times a day for 1 month (Fig. 1), the time at which scarring fibrosis peaks in rabbit corneas in response to this injury. 32 Therefore, in cases where clinically significant posterior corneal fibrosis occurs, topical losartan may effectively treat the scarring fibrosis. It is recommended that future studies use losartan 0.8 mg/mL 6 times per day, as has been used in multiple cases for the treatment of corneal fibrosis in Brazil without reported complications. 65
The second disorder where topical losartan was used to treat corneal scarring fibrosis was in severe 1 N NaOH alkali burns that also injured the corneal endothelium. 33 In that study, it was noted that the combination of topical losartan and the topical corticosteroid 1% prednisolone acetate provided a more consistent treatment for corneal scarring fibrosis than either agent alone. Thus, in highly inflammatory chemical burn injuries, the use of both agents is recommended, at least in the early stages of treatment. The duration of treatment in these cases could be determined by clinical observation of the corneal scarring and would likely be dependent on whether the corneal endothelium and Descemet's membrane were also injured. It is hypothesized that topical losartan with topical corticosteroid could be useful to decrease scarring fibrosis in a wide range of corneal chemical burns. For example, we hope to study the efficacy of this treatment in bioweapon sulfur mustard chemical burns, with and without corneal endothelial–Descemet's membrane injury, in the near future.
Losartan alone was almost as effective as losartan plus corticosteroid in the rabbit alkali burn study, but the treatments were not statistically identical. 33 Therefore, if there is severe inflammation in a cornea with an injury that produces scarring fibrosis, such as in severe alkali burns, then, if it is safe to do so, combined treatment may be considered. However, if the treating physician is concerned about the use of corticosteroids in a particular eye, then topical losartan alone can be administered and may be effective.
In the first two studies of topical losartan, there appeared to be an effect of the losartan on corneal neovascularization.32,33 TGF beta has been implicated in angiogenesis.87,88 However, this potential effect of topical losartan on corneal neovascularization needs to be directly studied in the future.
Finally, corneal stromal scarring is frequently noted in eyes with keratoconus, 89 and this scarring is commonly the reason for performing penetrating keratoplasty or deep anterior lamellar keratoplasty. Surprisingly, no studies have been published to show that the corneal scarring in keratoconus is caused by myofibroblasts, and, therefore, that topical losartan is likely to be effective in treating this scarring. A study is in progress at the Cleveland Clinic to explore this. However, since injury to the EBM is one of the earliest signs of keratoconus, 90 it is likely that myofibroblasts will be involved in the pathophysiology of corneal scarring in keratoconus.
Other Ocular Disorders Where Topical Losartan Could Hypothetically Provide Effective Treatments
TGF beta-induced corneal dystrophies
The transforming growth factor beta-induced protein (TGFBIp) is encoded by the transforming growth factor beta-induced (TGFBI) gene. 91 It is a 68 kDa ECM protein that has also been termed BIGH3, big-h3, bigh3, or keratoepithelin (KE) in various prior publications. TGFBIp contains a secretory signal peptide sequence found in all secreted proteins, a cysteine-rich EMI domain, 4 homologous fasciclin 1 (FAS1) domains (an ancient structural motif found in extracellular proteins) at the N-terminus, as well as an arginine–glycine–aspartate (RGD) motif at the C-terminus, which binds to integrins. 91 Interestingly, TGFBIp was initially isolated from an adenocarcinoma cell line and TGFBIp was found to be upregulated by TGF beta. 92 TGFBIp is expressed in many organs, such as skin, heart, pancreas, kidney, and tendons. 91 The specific functions performed by TGFBIp remain enigmatic but it is thought to have roles in mediating cell adhesion, migration, proliferation, and differentiation.91,93 In the cornea, TGFBIp is expressed primarily in the epithelium but also in keratocytes and corneal fibroblasts. 94
Mutations in TGFBIp are linked to nearly 40 corneal dystrophies, including Reis–Bu¨cklers corneal dystrophy, Thiel–Behnke corneal dystrophy, lattice corneal dystrophy type 1, granular corneal dystrophy type 1, and granular corneal dystrophy type 2 (Fig. 4).91,93 The phenotypic variation in these dystrophies is phenomenal considering they all involve the same protein. Most of these diseases demonstrate a conserved mutation in 1 of 2 hot spots: codon Arg124 in first FAS1 domain or Arg555 in fourth FAS1 domain of the TGFBIp protein.

Slit lamp photographs of the corneal deposits in a patient with granular corneal dystrophy, type 1, who would be a good candidate for a trial of topical losartan treatment since the mutant TGFBI protein is modulated by TGF beta-1 and losartan is a known inhibitor of TGF beta-1 signaling. TGF, transforming growth factor; TGFBI, transforming growth factor beta-induced. This image graciously provided by Jeffrey M. Goshe, MD.
A more detailed discussion of these TGFBIp-related corneal dystrophies and their phenotypes is beyond the scope of this review, but an exceptional and detailed review has been published by Han et al. 91 However, TGF beta-1 (and likely TGF beta-2) induces progressive accumulation of TGFBIp, along with other ECM proteins, including keratins, collagens, and fibronectin, in the corneal epithelium and stroma.95,96 Thus, in all the TGFBI-related corneal dystrophies, endogenous TGF beta-1, and likely TGF beta-2, expression and activation, although at low levels in unwounded corneas, potentially drives the accumulation of the mutant protein that deposits in the epithelium and/or stroma, depending on the specific dystrophy. As we have documented in earlier sections of this review, topical losartan penetrates the intact epithelium and stroma, and effectively inhibits TGF beta signaling. Therefore, it seems possible that topical losartan might decrease the production and deposition of TGFBIp in some or all of these vision-compromising and debilitating corneal dystrophies.
Given the lack of toxicity noted in rabbits or humans treated with topical losartan for conditions that trigger corneal stromal fibrosis, I believe clinical trials are indicated to evaluate the safety and efficacy of topical losartan in patients with the many different TGFBI-related corneal dystrophies. If efficacy is noted in at least some of these dystrophies, these trials can establish other parameters, such as the appropriate dosage of topical losartan, the optimal frequency of administration, the timing of treatment, and the duration of treatment. For example, is treatment most effective before significant accumulation of the protein in affected individuals or does treatment even impact already deposited TGFBIp? It is possible topical losartan could affect existing deposits of mutant TGFBIp and other deposited materials in some of these dystrophies if it slows down deposition to the point the keratocytes–corneal fibroblasts and epithelial cells are able to better handle elimination of the mutant TGFBIp in the diseased stroma and epithelium.
Corneal specialists often perform PTK to smooth the surface and debulk the corneal deposits in eyes with TGFBI dystrophies, when the only other alternative to improve vision is penetrating keratoplasty. However, the deposits routinely recur in these corneas over time. Perhaps long-term topical losartan treatment will delay the recurrence of the corneal deposits after PTK or in corneas that ultimately need penetrating keratoplasty to improve visual functions.
It may turn out topical losartan will not be effective in these dystrophies or it is only effective if started early upon diagnosis at a young age and used continuously. Well-designed clinical trials will provide these answers. I think most would agree it is at least worthy of investigation. It would indeed be exciting if we, corneal specialists, finally had some pharmacologic agent to impact these devastating corneal dystrophies.
Conjunctival fibrotic diseases
In the same way topical losartan penetrates the intact corneal epithelium and full thickness of the stroma, for example, after Descemetorhexis, 32 it is likely that it will penetrate the conjunctival epithelium into the underlying loose fibrovascular connective tissue substantia propria. The substantia propria consists of a meshwork of collagen and elastic fibers, in addition to fibroblasts, blood vessels, lymphatics, peripheral nerves, and inflammatory cells. There are a number of fibrotic conjunctival diseases, including trachoma, Stevens–Johnson syndrome, ocular cicatricial pemphigoid, ocular graft-versus-host disease, and other diseases.97–100 Drug-induced ocular cicatricial pemphigoid has been associated with the use of topical pilocarpine, epinephrine, dipivefrine, timolol, idoxuridine, ecothiopate, demecarium, benzalkonium chloride, and other drugs, in addition rarely to systemic drugs. 101 The development of myofibroblasts and conjunctival fibrosis are likely to have prominent roles in the pathophysiology of these diseases, although surprisingly little research has been undertaken to characterize the roles of myofibroblasts and fibrosis in some of these disorders.
Myofibroblasts in all tissues are dependent on TGF beta for development and survival.43,102,103 I hypothesize that topical losartan could be a useful adjuvant to current treatment modalities for each of these diseases and disorders to prevent progression and possibly even to decrease the level of conjunctival fibrosis. Multicenter clinical trials will likely be needed to explore the potential for topical losartan to augment current treatments for these diseases associated with conjunctival fibrosis as the conditions are somewhat rare.
Trachoma is worthy of special consideration. Trachoma is one of the most common blinding diseases in the world. 104 The pathogenesis of trachoma is related to recurrent conjunctival infection with Chlamydia trachomatis that typically begin in childhood. In the untreated or partially treated, the associated inflammatory and tissue injury components to the disease eventually lead to conjunctival fibrosis and trichiasis. 104 Ultimately, chronic rubbing of the eyelashes on the cornea triggers corneal fibrosis. Surprisingly little has been published on the histology of conjunctival or corneal fibrosis in trachoma. In fact, I have only discovered a single article in the literature that used α-SMA staining to partially explore myofibroblasts in conjunctival fibrosis in trachoma 105 and none studying myofibroblasts in trachomatous corneal fibrosis. However, I would be beyond surprised if myofibroblasts were not the primary mediators of fibrosis in both the conjunctiva and the cornea in trachoma. Chronic rubbing of anything on the corneal surface is the best method I can imagine for producing ongoing injury to the corneal EBM and promoting myofibroblast development and stromal fibrosis.
Antibiotics, such as azithromycin, will rightfully remain the primary treatment for prevention of trachoma. 106 However, many patients will unfortunately continue to develop the sequelae of chronic recurrent conjunctival infection with Chlamydia trachomatis due to antibiotic availability and distribution problems, as well as compliance issues. Topical losartan has the potential to treat conjunctival and corneal fibrosis after they have already developed. I hope that the World Health Organization and other interested parties will consider clinical trials to ameliorate the suffering of the millions of people already afflicted with this horrific disease.
Conjunctival bleb scarring and shunt encapsulation following glaucoma surgery
Glaucoma patients with disease progression that is not controlled by medications or laser procedures are often treated with a variety of glaucoma filtration surgeries that include trabeculectomy to form a conjunctival filtering bleb or a tube shunt procedure, such as the Baerveldt implant or Ahmed Glaucoma Valve. 107 Unfortunately, each of these surgical approaches to the treatment of advanced glaucoma is all too often complicated by myofibroblast-mediated fibrosis that can result in bleb scarring or encapsulation of the tube shunt that cause the treatment to fail. 107 These fibrosis-related complications are often treated with topical corticosteroids or by “needling the bleb” and/or the use of antimetabolites like mitomycin C or 5-fluorouracil administered by subconjunctival injection or topical intraoperative application. 107 These approaches also frequently fail, with elevation of intraocular pressure and progression of the glaucoma. Antimetabolite treatments can also cause severe complications, such as scleral melting. 107
It is not surprising that this is a major problem with trabeculectomy or tube shunt procedures since the aqueous humor that percolates from the anterior chamber of the eye and into the substantia propria after these procedures contains TGF beta-1 and TGF beta-2.108–111 This is the same TGF beta source that triggers posterior corneal fibrosis after Descemetorhexis.30–32 This TGF beta is likely to drive resident fibroblasts in the substantia propria, as well as bone marrow-derived fibrocytes attracted to the injury,40,48 to transition into myofibroblasts. Topical losartan is an excellent candidate drug to inhibit the development of these myofibroblasts and possibly trigger their apoptosis through its TGF beta signaling blockade effects.20,62–65 One group reported that subconjunctival injection of 5 mg/mL losartan significantly decreased postoperative intraocular pressure and subconjunctival myofibroblasts compared with controls in a rabbit trabeculectomy model. 112
While subconjunctival injections of losartan at the time of filtration surgeries or reneedling of blebs could be beneficial to initially control myofibroblast-mediated scarring, this approach is unlikely to be successful in the long-term management of fibrosis and likely needs to be supplemented with ongoing topical administration of losartan to provide long-term therapeutic benefit. My recommendation is not to exceed 0.8 mg/mL losartan in BSS 6 × per day since that dosage is likely to be effective based on human corneal outcomes 34 without needlessly increasing the risk of potential complications from normal cellular TGF beta-signaling blockade. Future trials may confirm that ongoing topical losartan dosages as low as 0.1 mg/mL, with lower frequencies of application, are effective in controlling fibrosis after glaucoma filtration surgeries. Of course, sterility is essential when utilizing topical losartan in patients with filtering blebs and tube shunts, and it may be wise to provide the medication in daily use vials for these clinical studies.
Hypertrophic scars after skin trauma or surgery
The skin of the eyelids or periocular areas may heal with hypertrophic scars. There has been a report of topical losartan in cream or ointment formulations effectively decreasing hypertrophic healing of the skin in humans. 113 In a study in mice, 0.2% losartan urea cream was applied twice a day for 30 days and there was a decrease in scarring compared with the vehicle control group. 114 These studies suggest that topical losartan cream or ointment formulations might also decrease scar hypertrophy in the skin of the eyelids or periocular area.
Potential use of losartan to control intraocular fibrosis
This review concentrated on the treatment of anterior segment disorders and diseases where TGF beta mediates fibrosis or mutant protein expression to produce diseases where topical losartan may be effective prophylactically or therapeutically to treat the disorder or disease. Losartan, and other ARBs, through their inhibition of TGF beta signaling, could also be useful adjuvants for prevention and treatment of more posterior fibrotic diseases involving the retina, choroid, vitreous, optic nerve, and other organs or tissues of the eye, especially if a sustained release drug delivery device were used to provide continuous or regular intermittent delivery of the drug to the tissues. For example, I could envision a role for losartan in the prevention and treatment of proliferative vitreoretinopathy, a disease for which there is currently no effective medical therapy. 115 Further research is likely to reveal new and exciting potential for these powerful ARBs in the treatment of intraocular diseases.
What if Topical Losartan Is Not Effective in a Patient with a Disorder Where It Was Effective in Animal Studies or Human Case Reports?
There are many potential issues that could lead to lack of efficacy in a particular patient. First, the losartan is likely to be effective only if the scarring process is mediated by myofibroblasts (this would not apply to theoretical use in TGFBI-related corneal dystrophies), and not, for example, transient haze in the cornea produced by corneal fibroblasts after normal PRK or riboflavin–UV crosslinking. Patient compliance is also a concern. For sufficient TGF beta signaling blockade, it is likely consistent and ongoing losartan administration is needed. Each of the rabbit studies of topical losartan reported thus far utilized a frequency of 50 μL 6 times per day (∼8 am, 10 am, noon, 2 pm, 4 pm, and 6 pm) with 0.1–0.2 mg/mL losartan in BSS (1.27 M NaCl, 30 mM NaH2PO4.H2O and 70 mM Na2HPO4.7H2O, pH adjusted to 7.0) prepared from ground tablets (which were ∼25% losartan and 75% excipients included to constitute the tablet, so 0.4 or 0.8 mg/mL of the ground tablet was used to give these final losartan dosages).32,33,75
A similar dosing regimen of 0.8 mg/mL losartan in 0.9% sodium chloride, pH 6.7–7.0, was used for the first case report patient in Brazil. 34 Application for 4–5 months in a particular patient is recommended before deciding the treatment was not effective.
Another potential problem, however, is distribution of counterfeit losartan. In the United States, there were 2021 reports by the FDA of fake losartan distribution (https://baguiocityguide.com/fda-warns-public-against-fake-version-of-this-drug-product). There are dozens of recognized manufacturers of losartan potassium worldwide (partial list https://www.pharmacompass.com/listed-active-pharmaceutical-ingredients/losartan-potassium) and little information is available about the medication from different sources. Thus far, the losartan potassium that has been used successfully in rabbit studies or human cases are: Zydus Pharmaceuticals, Pennington, NJ; Bristol-Myers Squibb, Sao Paulo, Brazil; PCCA, Houston, TX; and Merck and Co., Kenilworth, NJ). Therefore, it is recommended that if there is a failure of treatment after 2 or 3 months in a patient thought to have a myofibroblast-mediated disease or disorder that treatment with losartan potassium from another distributor/manufacturer be evaluated.
Conclusions
Topical losartan has the potential to treat numerous diseases of the cornea and anterior segment of the eye that are mediated by TGF beta-dependent myofibroblasts because of its effects on TGF beta signal transduction. It theoretically could also be of benefit to decrease corneal deposits in TGFBI-related corneal dystrophies. Intraocular fibrotic diseases could potentially be treated with losartan and sustained-release drug delivery devices. Clinical trials are needed to explore the efficacy and safety of losartan in a wide range of ocular diseases and disorders where TGF beta has a role in the pathophysiology.
Footnotes
Acknowledgments
The author is grateful for diligent work of all of the residents and postdoctoral fellows who worked in the Wilson Laboratory and contributed greatly to the understanding of the potential efficacy of topical losartan in corneal diseases.
Author Disclosure Statement
S.E.W. and the Cleveland Clinic have submitted a patent on the use of topical losartan and other ARBs to prevent and treat corneal scarring fibrosis.
Funding Information
Supported in part by DOD grants VR210001 (S.E.W.); U.S. Public Health Service grant P30-EY025585 from the National Eye Institute, National Institutes of Health, Bethesda, MD; Research to Prevent Blindness, New York, NY; and The Cleveland Eye Bank Foundation, Cleveland, OH.