
Abstract
Purpose:
Sustained intraocular drug delivery devices are being developed to lower intraocular pressure (IOP) and improve adherence in patients with glaucoma. The purpose of this study was to assess the IOP and eyedrop usage reduction effects of intracameral bimatoprost implants.
Methods:
We retrospectively reviewed the records of 46 eyes from 38 patients who received an intracameral implant containing 10 μg of bimatoprost as a replacement or addition to their existing eyedrop regimen and investigated IOP, eyedrop usage, and adverse effects.
Results:
Patients were followed for an average of 274 ± 104 (mean ± standard deviation) days after implant. Mean reduction in IOP (mmHg) at 3 months ±30 days, 6 months ±60 days, and 12 months ±90 days postoperation compared to baseline was 1.26 ± 2.53 (P = 0.002), 0.93 ± 4.71 (P = 0.098), and 1.35 ± 5.24 (P = 0.053), respectively. Reduction in eyedrops at 3 months ±30 days, 6 months ±60 days, and 12 months ±90 days postoperation compared to baseline were 0.62 ± 0.49 (P < 0.001), 0.55 ± 0.73 (P < 0.001), and 0.51 ± 0.71 (P < 0.001), respectively. Fifteen eyes (32.6%) experienced implant failure, defined as either restarting IOP-lowering eyedrops or undergoing surgical intervention, at an average of 260 ± 122 days after implant.
Conclusions:
While some patients eventually experienced implant failure, intracameral bimatoprost implants may result in fewer adverse reactions and successfully lower IOP and eyedrop burden over a longer period than previously reported.
Introduction
Open angle glaucoma (OAG) affects about 3 million individuals in the United States and is a leading cause of blindness. 1 It is a chronic disease that causes damage to the optic nerve, potentially leading to blindness without the proper treatment. 2 The first line of treatment includes intraocular pressure (IOP)-lowering topical medications such as prostaglandin analogs (PGA), which are often used due to their efficacy, excellent tolerance, and safety profile. 3 Numerous studies have demonstrated that topical PGAs are effective in lowering IOP if patients adhere to prescribed medications.3,4 However, patients must use these eyedrops daily to obtain maximum benefit.
One study found that patients were nonadherent with daily PGA eyedrops for an average of 63% of days in a 1-year period. 5 Early management and medication adherence are important in preventing negative outcomes with glaucoma progression, including decreased quality of life and increased economic costs associated with inadequate control and progression of glaucomatous disease.6,7
Sustained drug delivery devices are being developed to help address issues with adherence. 8 These devices include punctal plugs, conjunctival/subconjunctival inserts, and contact lenses with real-time IOP monitoring.9–13 All these devices are currently in clinical trials or seeking approval by the Food and Drug Administration.
The prostaglandin analog implant (Durysta; Allergan, Inc., Dublin, Ireland) was approved by the Food and Drug Administration (FDA) in March 2020 to lower IOP in patients with OAG and ocular hypertension. 14 The biodegradable implant, containing 10 μg of bimatoprost, slowly releases the active ingredient over 3–4 months, but has been shown in some studies to be effective up to 24 months.15,16 Clinical trials of intracameral bimatoprost (10 mg) have demonstrated IOP-lowering effects that are noninferior to topical timolol and approach those for topical bimatoprost.15,17
The aim of our study was to track the effectiveness and side effect profile of intracameral bimatoprost implants in patients at a single academic center. We hypothesized that intracameral bimatoprost implants would be more efficacious in the management of OAG and ocular hypertension than topical medications alone, demonstrated either by lower IOP or decreased drop burden postimplantation.
Methods
Approvals
This study adhered to the tenets of the Declaration of Helsinki and was approved by the Baylor College of Medicine Institutional Review Board. Informed consent was waived by the Institutional Review Board since the data were collected retrospectively.
Study population
This retrospective study included patients aged 18 years and older who received an intracameral bimatoprost implant at our academic center between November 1, 2020 and December 31, 2021 and had at least one follow-up visit. More recent patients were assumed to have insufficient follow-up data. The current procedural terminology code 66030 was used to identify patients who had received the intracameral bimatoprost implant. We manually confirmed that patients received the implant by reviewing each chart in the electronic health record.
Study design
All study data for this retrospective chart review were obtained from the electronic health record. For every patient, the following data were collected: age, sex, race, type of glaucoma, severity, affected eye, and date of the intracameral bimatoprost implant. The IOP, eyedrop regimen, and slit-lamp examination findings were recorded for each patient before the intracameral bimatoprost implantation and at each visit afterward. For every visit in the postoperative period, we also documented the visit date and adverse reactions. Baseline IOP was defined as the average of IOP measurements obtained at the 2 most recent clinic visits in the 6-month period before implantation. If any new IOP-lowering medications were introduced during these 2 visits, then only the most recent measurement would be recorded.
Durysta was used according to the FDA approved label which does not allow repeat implantation. During the sterile procedure, the bevel of the needle is inserted adjacent to the limbus and positioned completely within the anterior chamber. 14 Topical proparacaine 0.5% and postinjection antibiotics were given and do not result in long-term IOP changes. Topical PGAs were discontinued at the time of implant, while other IOP-lowering eyedrops were continued. The intracameral bimatoprost implant was considered a failure if there was readdition of topical PGA, addition of any new IOP-lowering medications, or the need for surgical intervention. The readdition of eyedrops was up to the surgeon's discretion, but was usually restarted if IOP had significantly increased from the prior visit. For every patient, we collected postimplantation data from each visit up until the time of data collection or implant failure, whichever came first.
Measurement of outcomes
Our aim was to determine (1) if intracameral bimatoprost implant lowers IOP; (2) if intracameral bimatoprost implant reduces eyedrop usage; and (3) how long intracameral bimatoprost implant is effective. For the first 2 outcomes, we compared the IOP and number of eyedrops from a patient's baseline to that of each postoperative visit. Postoperative visits were organized into follow-up periods consisting of 3 months ±30 days, 6 months ±60 days, and 12 months ±90 days follow-up for comparison. At each follow-up period, a decrease in mean IOP and/or a decrease in the number of eyedrops in follow-up patients would suggest that the intracameral bimatoprost implant is an effective alternative to topical IOP-lowering medications alone. For the third outcome, we averaged the length of time between the implantation date and implant failure to evaluate the effective lifespan of intracameral bimatoprost implant.
Data analysis
A paired t-test was performed to compare mean IOP and mean number of eyedrops in the preimplantation and postimplantation periods. The same analysis was repeated when excluding those who were not on any IOP-lowering eyedrops preimplantation due to drop intolerance.
Results
A total of 46 eyes from 38 patients were included in the analysis. The mean age of the population was 76.1 ± 6.8 years, and females comprised 52.2% of the study population. Subjects were Caucasian (73.9%), Asian (15.2%), African American (8.7%), or Hispanic (2.2%). Most eyes were diagnosed with primary OAG (84.8%) or ocular hypertension (6.5%), and 23 left and right eyes were studied. The severity of glaucoma ranged from mild to severe. The number of postoperative visits by patients ranged from 1 to 11 visits, with an average of 3.5 ± 1.9 postoperative visits per patient. Mean IOP before implantation for all study eyes regardless of follow-up period, was 16.58 ± 3.91 mmHg. At baseline, the mean number of IOP-lowering drugs used in all study eyes was 1.11 ± 0.71 drops (Table 1).
Baseline Demographics
IOP reduction
Thirty-seven eyes were followed up at 3 months ±30 days after implant. The mean IOP at these visits was 15.19 ± 3.49 mmHg, with a mean IOP reduction of 1.26 mmHg (CI: 0.42–2.09; P = 0.002) compared to these patient's baseline (Table 2).
Results
At 6 months ±60 days after implant, 44 eyes were followed up. The mean IOP at this follow-up period was 16.32 ± 5.96 mmHg, with a mean IOP reduction of 0.93 mmHg (CI: −0.50 to 2.36; P = 0.098) compared to baseline (Table 2). Forty-one eyes were seen at 12 months ±90 days after implant. The mean IOP at this follow-up period was 15.63 ± 4.22 mmHg, with a mean IOP reduction of 1.35 mmHg (CI: −0.29 to 3.00; P = 0.053) compared to baseline (Table 2).
Eight of the 46 eyes that received the intracameral bimatoprost implant were not on IOP-lowering eyedrops preimplantation due to drop intolerance. For patients on at least one drop, the mean IOP before implantation was 15.75 ± 3.58 mmHg. There was a mean IOP reduction of 1.00 mmHg (CI: 0.13–1.87; P = 0.014) at 3 months ±30 days (Table 3) compared to baseline. Mean IOP at 6 months ±60 days decreased by 0.42 mmHg (CI: −1.18 to 2.01; P = 0.30) (Table 3) compared to baseline. However, mean IOP at 12 months ±90 days increased by 0.42 mmHg (CI: −1.72 to 0.88; P = 0.26) compared to baseline. Nevertheless, this subset was consistent with our findings of a IOP reduction at only the 3 months ±30 days time period.
Results: Excluding Patients not on Preoperative Intraocular Pressure-Lowering Drops
Reduction in number of eyedrops
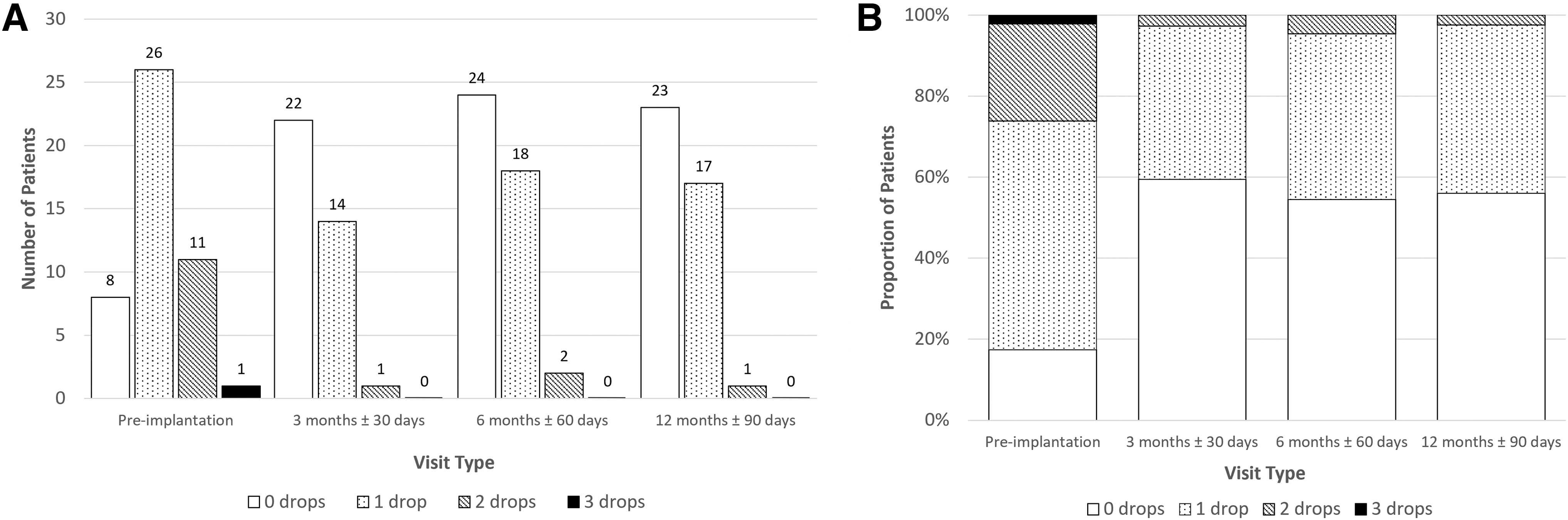
At 3 months ±30 days follow-up, the mean number of IOP-lowering eyedrops used in the 37 study eyes was 0.43 ± 0.55 drops, with a mean eyedrop reduction of 0.62 drops (CI: 0.46–0.78; P < 0.001) compared to baseline. At 6 months ±60 days follow-up, 44 patients had a mean eyedrop usage of 0.50 ± 0.59 eyedrops, with a reduction of 0.55 drops (CI: 0.32–0.77; P < 0.001) (Table 2) compared to baseline.
The 41 patients following-up at 12 months ±90 days after implant had a mean eyedrop usage of 0.46 ± 0.55, with a mean reduction of 0.51 drops (CI: 0.29–0.74; P < 0.001) compared to baseline. A chi-square test of independence showed that the distribution of eyedrops usage was significantly shifted toward zero at 3 months, χ 2 (2, n = 37) = 67.78 (P < 0.001), 6 months, χ 2 (3, n = 44) = 40.05 (P < 0.001), and 12 months, χ 2 (3, n = 41) = 29.50 (P < 0.001), compared to baseline (Fig. 1).
When excluding the 8 eyes that did not receive IOP-lowering eyedrops before the implantation, the findings of this subset were still consistent with a reduction in eyedrops usage. At baseline, the mean number of IOP-lowering drugs used was 1.34 ± 0.53. At 3 months ±30 days, patients had a mean eyedrop reduction of 0.72 drops (CI: 0.56–0.88; P < 0.001) compared to baseline. At 6 months ±60 days, patients had a mean eyedrop reduction of 0.75 drops (CI: 0.55–0.95; P < 0.001) (Table 3) compared to baseline. The patients who were followed up at 12 months ±90 days had a mean eyedrop reduction of 0.75 drops (CI: 0.48–1.02; P < 0.001) compared to baseline.
Implant failure and adverse reactions
Across all postoperative visits, 15 eyes (32.6%) had implant failure defined as either restarting IOP-lowering eyedrops (n = 8) or scheduling for surgical interventions such as Selective Laser Trabeculoplasty (n = 6) or glaucoma tube shunt placement (n = 1). In these patients, failure occurred at an average of 260 ± 122 days postimplantation. Mean IOP at the time of failure was 22.00 ± 6.78 mmHg and the average number of IOP-lowering eyedrops was 0.47 ± 0.64 drops (Table 4). When divided into follow-up periods, 1, 8, and 6 eyes experienced implant failure at 3 months ±30 days, 6 months ±60 days, and 12 months ±90 days, respectively.
Results: Intracameral Bimatoprost Implant Failure
Adverse events documented during all postoperative visits included dry eye (n = 9), conjunctival hyperemia (n = 8), blurry vision (n = 4), floaters (n = 2), iritis (n = 2), itching (n = 2), hordeolum (n = 1), headache (n = 1), and implant migration to the sulcus (n = 1).
Discussion
Our study demonstrated that an intracameral bimatoprost implant was effective at reducing IOP and drop burden at 3 months. However, IOP reduction was not statistically significant at 6 months and 12 months follow-up. Although IOP reductions at 6 and 12 months did not reach statistical significance, they were of similar magnitude to IOP reduction at 3 months. Furthermore, the reduction of eyedrop burden through 12 months suggests that an intracameral bimatoprost implant is effective at managing OAG and ocular hypertension in the short and long term.
When comparing data from our main cohort to our exclusionary subset, there appears to be worse IOP-lowering effects after excluding patients not on preoperative eyedrops. This suggests that patients unable to receive topical IOP-lowering eyedrops may benefit the most from intracameral bimatoprost.
Intracameral bimatoprost implant was intended to lower IOP over a 3- to 4-month period, but our findings suggest that it may have a longer duration of efficacy, confirming previous studies. A phase I/II trial studying the bimatoprost implant demonstrated that IOP was controlled without additional implants or rescue medication in 68% of eyes at 6 months, 40% at 1 year, and 28% at 2 years. 15 In 2 phase III trials investigating the efficacy of the bimatoprost implant, results also showed that the implant was noninferior in terms of IOP reduction compared to timolol twice a day through the first 12 weeks.17,18 Since the primary endpoint of the phase III studies were set at 12 weeks in eyes receiving only a single implant, no conclusions were made on the effective lifespan of the intracameral bimatoprost implant.
Results from our study showed that the intracameral bimatoprost implant can reduce drop burden even at 12 months postimplantation. Furthermore, the majority (67.4%) of our single center study population have yet to fail following implantation. Those that did experience implant failure received IOP-lowering eyedrops or were scheduled for surgical interventions after an average of 37 weeks (8–9 months) postimplantation.
The extended duration of the intracameral bimatoprost implant past 3 months is not well understood. In vitro assays measuring drug release determined that the contents of the implant were completely released after 3 months. 17 In addition, studies with beagle dogs showed bimatoprost levels to be undetectable after 4.2 months. 17 With drug levels likely undetectable, most of our patients continued to have controlled IOP well past that time point. While it is known that long-term treatment with prostaglandins expands the uveoscleral outflow pathways, the leading hypothesis is that the targeted intracameral delivery of bimatoprost leads to increased drug concentration at the iris-ciliary-body, causing a dose-dependent response.16,18,19 To determine the effective lifespan of the intracameral bimatoprost implant and the mechanism behind its extended duration, further long-term analysis and study are needed.
In addition to reducing drop burden, an intracameral implant offers an alternative treatment for those that are intolerant to eyedrops. Across 46 implants in our study, there was one reported case of implant migration causing severe inflammation. Most adverse outcomes, however, were minor reactions such as conjunctival hyperemia, dry eyes, and blurry vision. Seventeen percent of patients from our study reported conjunctival hyperemia (n = 8) during their postoperative visits. In a meta-analysis of multicenter studies, 49% of patients receiving topical bimatoprost 0.03% were reported to experience conjunctival hyperemia. 20 Hypertrichosis, which was experienced by 36% of patients on once-daily topical bimatoprost in a 6-month trial, was not reported with the intracameral implant. 21
Iris pigmentation, which was associated with 3.1%–5.2% of patients using latanoprost or travoprost, along with periocular skin pigmentation was not rigorously monitored and would not be adequately detected in our study if rates of occurrence are similar to reports in the literature. 22 Other adverse effects associated with PGAs such as cystoid macular edema were not reported during our study. 20 One theory explaining the decrease in adverse effects is that an intracameral implant bypasses the eyelid margins, bulbar conjunctiva, and periorbital fat. In contrast, topical administration of bimatoprost was found to deliver higher concentrations to those areas causing the adverse effects typically associated with topical PGA. 16 Patients who experience these effects may be more prone to nonadherence.
This study was a retrospective case review. One of its limitations is the small number of follow-up visits from patients who were recently treated. Although our goal was to track IOP across multiple visits, we still included patients with less than 12 months of follow-up. Other limitations of this study included the small sample size. To provide more adequate power, this study can be expanded in the future to include a greater number of patients. The study also included participants who were on average 76 years old; therefore, the data may not be generalizable to younger populations.
In summary, this study demonstrated that an intracameral bimatoprost implant is a safe and effective treatment option for OAG or ocular hypertension. The intracameral bimatoprost implant may help patients with poor adherence to topical medication by easing the burden of multiple regimens and from adverse effects associated with topical PGA. The lifespan of the intracameral bimatoprost implant may also be longer than previously investigated and should be further studied along with the mechanism behind its extended duration.
Footnotes
Authors' Contributions
W.X.: original draft (lead), review and editing (lead), and formal analysis (supporting). P.Z.: original draft (supporting), and review and editing (supporting). N.D.K.: conceptualization (equal), and review and editing (supporting). B.J.F.: formal analysis (lead) and review and editing (supporting). L.S.B.: review and editing (supporting) and methodology (supporting). P.T.C.: methodology (lead) and conceptualization (equal).
Author Disclosure Statement
P.T.C. has previously consulted for Allergan. All other authors declare no conflicts of interest.
Funding Information
This study was supported by an Unrestricted Grant from Research to prevent Blindness.