
Abstract
Dry eye disease (DED) is a multifactorial disease affecting 5% to 50% in different populations. The most severe cases of DED are often caused by aqueous deficient dry eye disease (ADDE) due to lacrimal gland (LG) hypofunction. Many patients with severe ADDE do not experience adequate symptom relief from topical treatment, severely reducing their quality of life. The focus of this review is to describe the surgical interventions presently being used or investigated when topical treatment with eye drops is insufficient. The conventional surgical approach is to proceed to punctal occlusion or partial or total tarsorrhaphy. However, novel surgical procedures have been reported to have higher efficacy and patient satisfaction than conventional treatments. These procedures include amniotic membrane transplantation, transposition or transplantation of the salivary glands, and cell-based injections into the LG, each with strengths and weaknesses. Further development of these treatment modalities might prove pivotal in treating dry eye patients in the future.
Introduction
Dry eye disease (DED) has been reported to affect as much as 50% of the population. 1 Symptoms of DED include a variety of ocular discomfort and blurred vision, which has a negative impact on the visual function and quality of life. 2 As concluded in the Tear Film and Ocular Surface Society (TFOS) Dry Eye Workshop (DEWS) II report from 2017, DED is a multifactorial disease, in which hyperosmolarity of the tear fluid, tear film instability, and inflammation on the ocular surface leads to damage, and neurosensory abnormalities.
This further deteriorates the integrity of the tear film, leading to a vicious cycle. DED can be subdivided into evaporative dry eye (EDE), which is characterized by a decrease in tear film quality and aqueous-deficient dry eye (ADDE) characterized by a decrease in tear fluid quantity from the lacrimal gland (LG). 3 The most common causes of severe ADDE are Sjögren's syndrome (SS), which is a chronic autoimmune disorder affecting the exocrine glands, and graft-versus-host disease (GvHD), and Steven Johnson syndrome (SJS). 4
Although nonsurgical treatments are typically the first line of approach, surgical interventions may be considered for severe and refractory cases of DED that do not respond adequately to conservative therapies. 5 Novel surgical procedures might prove pivotal for the future treatment of ADDE. In this review, we aim to present the current treatment strategies for surgical management of treatment refractive ADDE by primarily focusing on up-to-date human studies.
Eyelid Procedures
Punctal occlusion
In patients with ADDE, conservation of tears on the ocular surface can be achieved by blocking the drainage of tear fluid in the lacrimal puncta. 6 This procedure can be performed either unilaterally or bilaterally, on the upper or lower punctum or both, and by using either punctal plugs or more permanently by surgical occlusion.7–10 This treatment modality, however, is most likely to be successful when combined with other treatments of DED. 11 A Cochrane review updated in 2017 included 18 clinical trials aimed at elucidating the efficacy of punctal plug occlusion as a treatment of DED. The authors concluded that even though punctal plugs was considered a relatively safe treatment, few studies had reported punctal plugs to be effective in the treatment of DED; the aggregate evidence was inconclusive mainly due to the extensive heterogeneity in trial methodology. 12
The most common complication related to punctal plugs is spontaneous plug displacement, occurring in as many as 70% of cases, whereas infection, conjunctivitis, subconjunctival hemorrhage, chemosis, epiphora, discomfort, and foreign body sensation were less frequent.13–15 One concern regarding tear conservation approaches is that retention of tear fluid containing pro-inflammatory cytokines on the ocular surface could worsen the inflammatory process, driving the vicious circle of DED. One study, however, contradicts this notion as punctal occlusion resulted in reduced corneal fluorescein staining (CSF) and DED symptoms without a rise in matrix metalloproteinase 9 levels. 16
Permanent surgical occlusion of the lacrimal punctum is typically reserved for patients who do not tolerate punctal plugs. The most common method is by thermal cautery; however, other options include diathermy and Argon laser. 17 Permanent punctum occlusion by cauterization has been found to significantly alleviate symptoms of DED, increase tear production and tear film break-up time (TBUT), and reduce CSF in patients with ADDE. To avoid epiphora after treatment, a partial occlusion technique has been shown to improve TBUT and CSF in patients with SS. 18
Tarsorrhaphy
Tarsorrhaphy is a surgical procedure in which partial or total closure of the eyelids is obtained using either sutures, adhesive tape or levator paralysis by Botulinum toxin A (BTA) injection. 19 The purpose of this treatment is to decrease ocular surface exposure to keep the ocular surface lubricated and protected. As this procedure impairs the visual function on the treated eye it is reserved for patients with persistent epithelial defects and in cases of severe DED that are refractory to previous treatment. With careful patient selection, however, it does have a high success rate (>90%) with only few complications such as trichiasis, premature opening of the tarsorrhaphy, and infection. 20 Interestingly, only 20% of patients have reported being unhappy with the cosmetic appearance of the tarsorrhaphy, which is possibly due to the fact that it is normally reserved for cases where all other treatments have failed. 21
Transplantations and Transpositions
Amniotic membrane transplantation
The amniotic membrane (AM) is the innermost layer of the placenta and consists of 3 layers: a monolayer epithelium, a thick basement membrane, and an avascular stroma. The AM contains various anti-inflammatory and anti-angiogenic cytokines and growth factors, which are involved in promoting epithelial wound healing. 22 Amniotic membrane transplantation (AMT) has been successfully used to treat various inflammatory ocular surface diseases, including epithelial keratitis in DED, corneal ulcers, persistent epithelial defects, and limbal stem cell deficiency. 23 Initially, AMT was performed by suturing the graft to the ocular surface (Fig. 1A). More recently, cryopreserved AM (CAM) has been used as a sutureless self-retained biologic bandage lens for the cornea (Fig. 1B).

Different methods used for amniotic membrane transplantation.
Further, a combination of AM transplantation kept in place using a symblepharon ring has proven effective in the acute phase of SJS (Fig. 1C). 24 Whereas sutured grafts gradually dissolve over the course of 12 months, sutureless AM grafts dissolve within a week. 25 The commercially available CAM, Prokera® (BioTissue, Doral, FL), seems to offer a promising treatment option for patients with moderate-to-severe treatment refractive DED. 26 However, 1 study investigated the effect of Prokera in patients with ADDE due to SS and found that all patients experienced a relapse of symptoms after a mean of 24.6 days after removal of the Prokera. 27 This suggests that the anti-inflammatory effect of AM transplantation in patients with ADDE might be temporary. In the future, topical treatment with AM extract eye drops might offer an alternative approach. 28
Transplantation of the salivary glands
The salivary glands (SGs) share many common morphological and physiological characteristics with the LG. The composition of SG and LG secretion is similar and contains antimicrobial peptides and surface immunoglobulins that provides mucosal immunity. Tears have a pH range of 6.5–7.6, whereas the pH of saliva ranges from 5.6 to 7.0.29,30 The similarities have led to the exploration of SG transplantation as a possible treatment of severe ADDE. The concept of using saliva to lubricate dry eyes was first employed in 195131 and since then, transplantation and/or transposition of the major SGs (parotid, submandibular, and sublingual gland) and the minor labial SGs has been explored (Fig. 2).
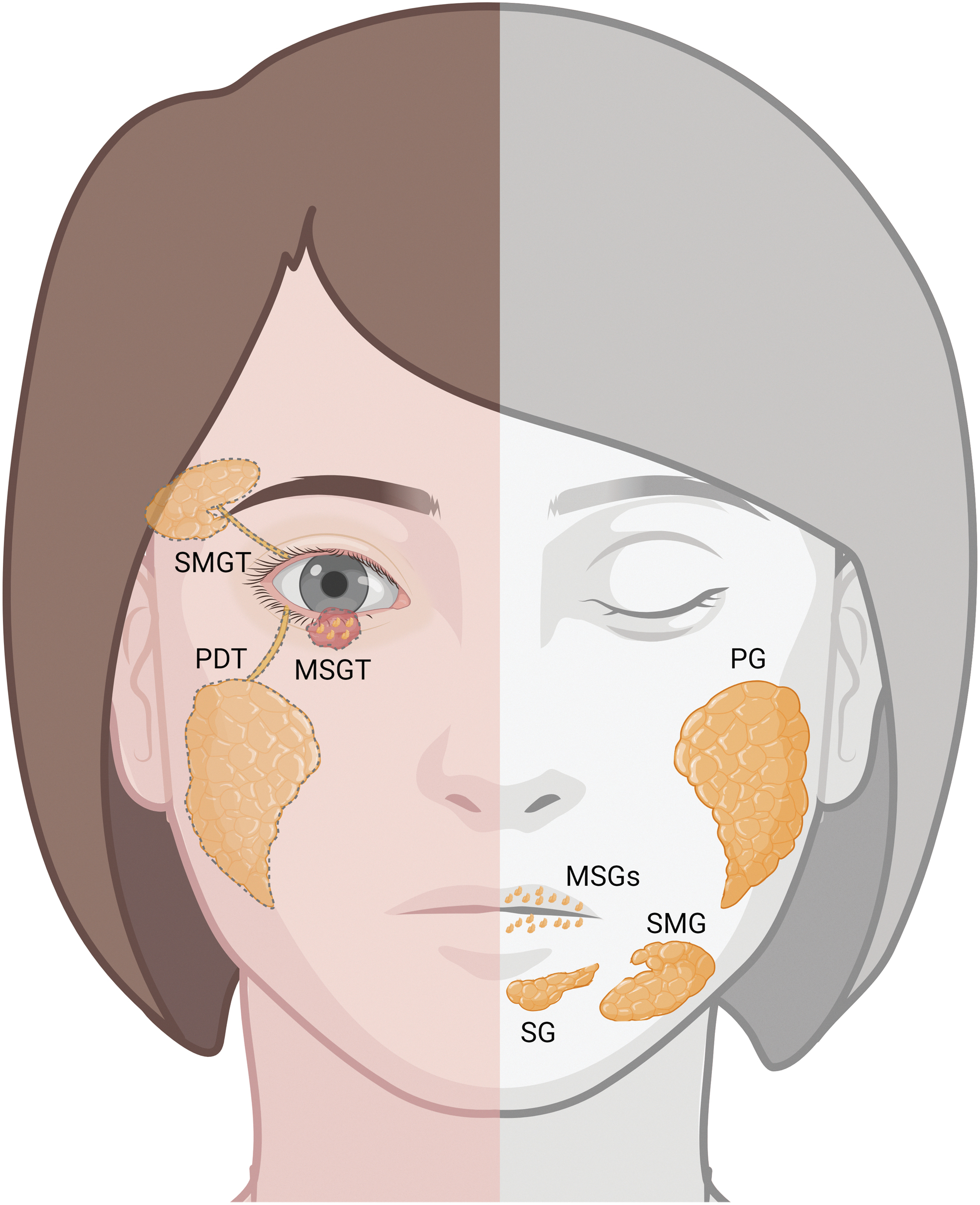
The various transplantations and transpositions of the salivary glands are illustrated on the left side of the figure. The right side of the figure shows the normal anatomic position of the salivary glands. PG, parotid gland; SMG, submandibular gland; SG, sublingual gland; MSG, minor labial salivary glands; SMGT, submandibular gland transplantation; PDT, parotid duct transposition; MSGT, minor labial salivary gland transplantation. Created using Biorender.com
The transplantation of SGs ultimately results in the establishment of functional exocrine tissue that serves as a source of lubrication and supplies various beneficial factors present in tears to alleviate DED. 32 The process of SG transplantation is intricate and challenging as it involves multiple steps such as graft harvesting, transfer, and microanastomosis. Thus, collaboration with a skilled oral surgeon or maxillofacial surgeon is required. SG transplantation should be reserved for patients with severe end-stage ADDE, which cannot be controlled by conservative means. Autologous SG transplantation is by far the most studied method.
However, this treatment is controversial in patients with ADDE due to autoimmune disorders such as SS and GvHD, which might affect the SGs as well. Allogeneic transplantation, although technically feasible, is complicated as histocompatibility is a major concern. This requires lifelong immunosuppressive treatment, which often results in complications. 33 This leaves severe ADDE without affection of the SGs as the primary indications for autologous transplantation. The indications include ADDE due to chemical injuries, SJS, cicatrizing conjunctivitis, acquired alacrimia (after excision of LG tumor), congenital alacrimia, facial nerve palsy, and idiopathic keratoconjunctivitis sicca.31,32
Parotid duct transposition
In parotid duct transposition the secretory duct of the parotid gland (Stensen's duct) is moved from its original position in the mouth to the lower conjunctival fornix (Fig. 2). 34 As the innervation of the parotid gland is maintained, the ocular surface receives an exclusively serous secretion that is controlled by the gustatory reflex. As the present data mainly come from older retrospective case reports the success rate is questionable. 35 Complications such as gustatory reflex epiphora and complications related to the serous composition of the “salivary tears” have since led to the conclusion that techniques involving the other SGs are superior. 31
Submandibular gland transplantation
In transplantation of the submandibular gland, the gland along with a vascular pedicle and the secretory duct is implanted under the skin of the temporal region. An anastomosis from the facial vessels is performed and the duct is then sutured into the conjunctival fornix (Fig. 2). 35 Submandibular gland transplantation (SMGT) has several advantages compared with other transplantations of major SGs: The “salivary tears” from the SMG grafts resemble the mucoaqueous component of the normal tear film causing fewer complications such as reflex epiphora and graft ischemia.36,37 SMGT has been tested in several clinical trials in patients with severe ADDE and a viability in 85% to 100% of cases up to 5 years after transplantation has been reported with improvement in Schirmer test scores, TBUT, and CSF.38–41
However, epiphora remains a common complication, why partial SMGT has been investigated. In 1 study 86% (19/22 patients) with a total submandibular gland graft suffered from epiphora versus 30% (6/20 patients) with a partial transplant. 42 In these cases epiphora can be controlled either surgically by reducing the size of the SMG or by partial ligation of the excretory duct or pharmacologically with periglandular BTA injections or by applying atropine gel onto the skin overlying the graft.43–45 The most significant limitation of SMGT is the hypo-osmolarity of the salivary tears, which causes microcystic epithelial edema in up to 40% of the cases. 46
Minor labial SG transplantation
The minor labial salivary glands (MSGs) reside in the labial mucosa and has been used as a complex graft (a mucosal patch including MSGs) to the fornices, palpebral, tarsal, or bulbar conjunctiva in eyes with severe ADDE (Fig. 2). Minor labial salivary gland transplantation (MSGT) has resulted in an increase in Schirmer's test score and CSF with graft viability in up to 95% of cases. 32 In a larger study an improvement in visual acuity (VA) from 38% of cases with a VA ≥20/200 at baseline to 93% 3 years after MSGT was found. 47
This is in contrast to other SG transplantation methods which has not proven to improve VA. MSGT has generally been reported to carry low risk for complications; however, labial hypoesthesia at the donor site has been reported in about 2/3 of cases, whereas graft necrosis and epiphora are rare. 47 SMGT is a complex procedure, which requires collaboration with an oral maxillofacial surgeon, whereas MSGT is simpler with low surgical risk. The most significant limitation of MSGT is the limited lubrication provided. 48 In a rhesus monkey animal model, the efficacy of fluid production initially increased after transplantation, but showed a decrease during follow-up. 49
Injections
Periocular botox injection
Botulinum toxin A (botox, BTA) is a neurotoxin that blocks the release of acetylcholine at the neuromuscular junctions of cholinergic nerves, which reduces muscle contractions. 50 Although injection of BTA into the LG is a mainstay treatment of patients with hypersecretion from the LG, 51 periocular injection of BTA has also been investigated as a potential treatment of ADDE. In 1997, it was first reported that periocular injection of BTA in patients with SS resulted in an increase in Schirmer test scores and a decrease in DED symptoms. 52 It has since been proposed that injection of BTA into the medial part of the lower eyelid causes orbicularis muscle paralysis, which in turn decreases the amount of tear volume ejected at each blink. 53
More recently, 2 randomized clinical trials have demonstrated the efficacy of periocular BTA injection as a treatment of DED.54,55 However, in these studies the Schirmer test scores have inconsistently shown to be both lower and higher after treatment. A recent retrospective observational study of 28 patients with DED found significant improvements in the DED symptoms, tear osmolarity, Schirmer test scores, and tear meniscus height 1 month after treatment. 56 No data on long-term results have been published, but the effect of this treatment is presumed to be temporary. Interestingly, 1 previous study has compared BTA injection with punctal plugs and concluded, that of the 2, BTA was associated with fewer and milder complications and with higher levels of patient satisfaction. 57
Platelet-rich plasma
Platelet-rich plasma (PRP) is a reservoir of biologically active growth factors, which has been proven to be effective on tissue regeneration and wound healing. 58 These regenerative properties are related to the high content of growth factor from PRP, which supports cell proliferation. 59 In an effort to target the underlying cause of LG hyposecretion in patients with ADDE, injection of autologous PRP into (or around) the LG has been tested in 2 trials in patients with SS.60,61 In the first prospective clinical trial, 30 patients with ADDE due to SS were randomized to either (n = 15) repeated PRP injection (days 0, 30, 60, and 90) + hyaluronic acid (HA) eye drops or (n = 15) HA eye drops alone. The injections were performed transcutaneously into the external one-third of the orbital rim in the anatomical area corresponding to the location of the LG (Fig. 3B).

Routes of injection into the LG.
Ninety days after treatment a significant improvement in Schirmer's test scores, CSF, TBUT, and DED symptoms was found. 60 Moreover, in a recent retrospective study of 14 patients with ADDE due to SS, injection of PRP demonstrated significant improvements of the treated eye compared with the fellow eye evaluated with noninvasive TBUT, tear meniscus height, lipid layer thickness, CFS, and Schirmer test scores. 61 No data on DED symptoms in the patients were reported in this study. Among the scarce clinical trials investigating PRP injection as a treatment of ADDE no long-term results have been published. Interestingly, no adverse events were reported in any of these trials.
Mesenchymal stem cells
Cell-based therapies aiming at regenerating the LG have been the topic of several investigations in preclinical studies. 62 Most of the previous research has been performed in animal models, in which the therapeutic effect of mesenchymal stem cells (MSCs) has been demonstrated.63–68 The regenerative effect of MSCs has been ascribed to their paracrine and immunomodulating properties—specifically it has been suggested that MSCs exert their effect by restoring the balance between pro-inflammatory Th17- and anti-inflammatory regulatory T cells. 69
In 2021, the results of the first study investigating injection of allogeneic MSCs into the LG as a treatment for ADDE in humans were published. 70 The purpose of this open-label clinical trial was to evaluate the safety and feasibility of injecting allogenic adipose-derived mesenchymal stem cells (ASCs) into the LG in patients with severe ADDE due to SS. Seven subjects received 1 transconjunctival injection of ASCs from a healthy donor into the LG in 1 eye (Fig. 3A). The primary outcome measure was safety evaluated as number of adverse reactions related to the study treatment.
Within the 4 months of follow-up in this study, no adverse reactions were observed. A significant improvement in ocular surface disease index (OSDI) score, tear osmolarity, TBUT, and Schirmer test scores in the treated eye suggest that injection of ASCs into the LG is a safe and feasible treatment of severe ADDE. To evaluate the therapeutic effect of this treatment, a randomized clinical trial using allogeneic ASCs as a treatment of ADDE due to SS was initiated in November 2020 and the results are underway. 71 In this trial, a transcutaneous injection into the LG using ultrasonic guidance is performed to assure delivery of the treatment within the LG (Fig. 3C). 72
Conclusion
In patients with severe dry eye and insufficient response to treatment with eye drops, a surgical procedure should be considered the next step. Novel treatments, including AM transplantation and autologous transplantation of the minor salivary glands, have been reported to be successful in selected patients, but each have their limitations. In patients with severe ADDE, cell-based injections into the LG targets the underlying inflammation in ADDE and have shown promising results in human studies. Further development of treatments with cell-based injections might prove pivotal for the treatment of dry eye patients in the future.
Authors' Contributions
M.M-H. contributed to conceptualization, methodology, writing—original draft, and visualization. S.T-P. carried out conceptualization, methodology, writing—review and editing. S.H. carried out conceptualization, supervision, and writing—review and editing.
Footnotes
Author Disclosure Statement
All authors met the ICMJE authorship criteria. No honoraria or payments were made for authorship. In collaboration with Rigshospitalet and the University of Copenhagen authors M.M-H. and S.H. has filed a patent application “Stem cell therapy for lacrimal gland dysfunction” to the European Patent Office (ref. 21943EP00). M.M-H. is a member of the advisory board for Abilion Medical Systems AB. T.P.H. is cofounder and co-owner of The Norwegian dry eye clinic and the Clinic of eye health, Oslo, Norway, which delivers talks for and/or receives financial support from the following: ABIGO, Alcon, Allergan, AMWO, Bausch & Lomb, Bayer and European school for advanced studies in ophthalmology, InnZ Medical, Medilens Nordic, Medistim, Novartis, Santen, Specsavers, Shire Pharmaceuticals, and Théa Laboratories.
Funding Information
This study was funded by grants from Simon Spies Fonden, Synoptik Fonden, and Fight for Sight, Denmark.