
Abstract
Purpose:
Diabetic retinopathy (DR) is a microvascular retinal disease associated with chronic diabetes mellitus, characterized by the damage of blood vessels in the eye. It is projected to become the leading cause of blindness, given the increasing burden of the diabetic population worldwide. The diagnosis and management of DR pose significant challenges for physicians because of the involvement of multiple biochemical pathways and the complexity of ocular tissues. This review aims to provide a comprehensive understanding of the molecular pathways implicated in the pathogenesis of DR, including the polyo pathway, hexosamine pathway, protein kinase C (PKC), JAK/STAT signaling pathways, and the renin–angiotensin system (RAS).
Methods:
Academic databases such as PubMed, Scopus, Google Scholar and Web of Science was systematically searched using a carefully constructed search strategy incorporating keywords like “Diabetic Retinopathy,” “Molecular Pathways,” “Pharmacological Treatments,” and “Clinical Trials” to identify relevant literature for the comprehensive review.
Results:
In addition to activating other inflammatory cascades, these pathways contribute to the generation of oxidative stress within the retina. Furthermore, it aims to explore the existing pharmacotherapy options available for the treatment of DR. In addition to conventional pharmacological therapies such as corticosteroids, antivascular endothelial growth factors, and nonsteroidal anti-inflammatory drugs (NSAIDs), this review highlights the potential of repurposed drugs, phyto-pharmaceuticals, and novel pipeline drugs currently undergoing various stages of clinical trials.
Conclusion:
Overall, this review serves as a technical exploration of the complex nature of DR, highlighting both established and emerging molecular pathways implicated in its pathogenesis. Furthermore, it delves into the available pharmacological treatments, as well as the promising repurposed drugs, phyto-pharmaceuticals, and novel drugs currently being evaluated in clinical trials, with a focus on their specific mechanisms of action.
Introduction
Diabetic retinopathy (DR) is a serious comorbidity of diabetes mellitus (DM), which remains the top reason of visual impairment in working age population. 1 At present, diabetes is considered to be the fourth most prevalent metabolic disorder affecting 13% of the total world population and is closely related to DR that can compromise the quality of life. Insulin insufficiency, owing to damaged pancreatic β cells, results in a surge of blood glucose level during diabetes. DR, diabetic neuropathy, and diabetic nephropathy are the 3 most prominent comorbidities in hyperglycemia.2,3
This microvascular disease severely affects the retina, characterized by retinal hemorrhage, microaneurysms, neovascularization, hard exudates, and retinal detachment. Based on its severity, it has been characterized as nonproliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR). 4 Of the total 13 million DR patients in India, 6.5 million are considered to be on the verge of vision loss. 5 Indirect ophthalmoscopy, fundus imaging, and optical coherence tomography are some of the common techniques applied for preliminary diagnosis of DR.6,7
DR is a multifactorial metabolic disorder that encompasses a plethora of complex biochemical pathways; some of which are explored, whereas other remains a mystery till date. Conventional pharmacotherapy of DR involves several drawbacks such as single pathway concentric, improper drug delivery strategy including side effects that further progresses to blindness. A number of novel pathways have been discovered recently that play vital roles in the progression of DR. In addition to the combination strategy of traditional therapeutic molecules, several novel molecules are under preclinical and clinical trials to curb the alarming rate of growth in DR suffering patients.8,9
In the present review, we have summarized the recent advancements in the pathways involved in DR along with its management.
Pathophysiology
The etiology of DR revolves around the activation of multiple complex biochemical pathways in response to hyperglycemia, which significantly impact the retinal microvasculature. Several key pathways contribute to the pathogenesis of DR, including the polyol pathway, hexosamine pathway, oxidative stress, protein kinase C (PKC) activation, JAK/STAT pathway, RAS signaling pathways, advanced glycation end products (AGEs), TRX/TXNIP redox signaling, PPAR pathway, and other apoptotic factors. These pathways interact and synergistically exert detrimental effects on normal retinal cells. Collectively, the dysregulation of these pathways and the interplay between them contribute to the complex pathogenesis of DR, leading to microvascular abnormalities, retinal dysfunction, and potential vision loss. Understanding these underlying biochemical processes is crucial for developing effective therapeutic strategies to mitigate the progression of DR. Some of the above-mentioned pathways are given diagrammatically in Fig. 1.
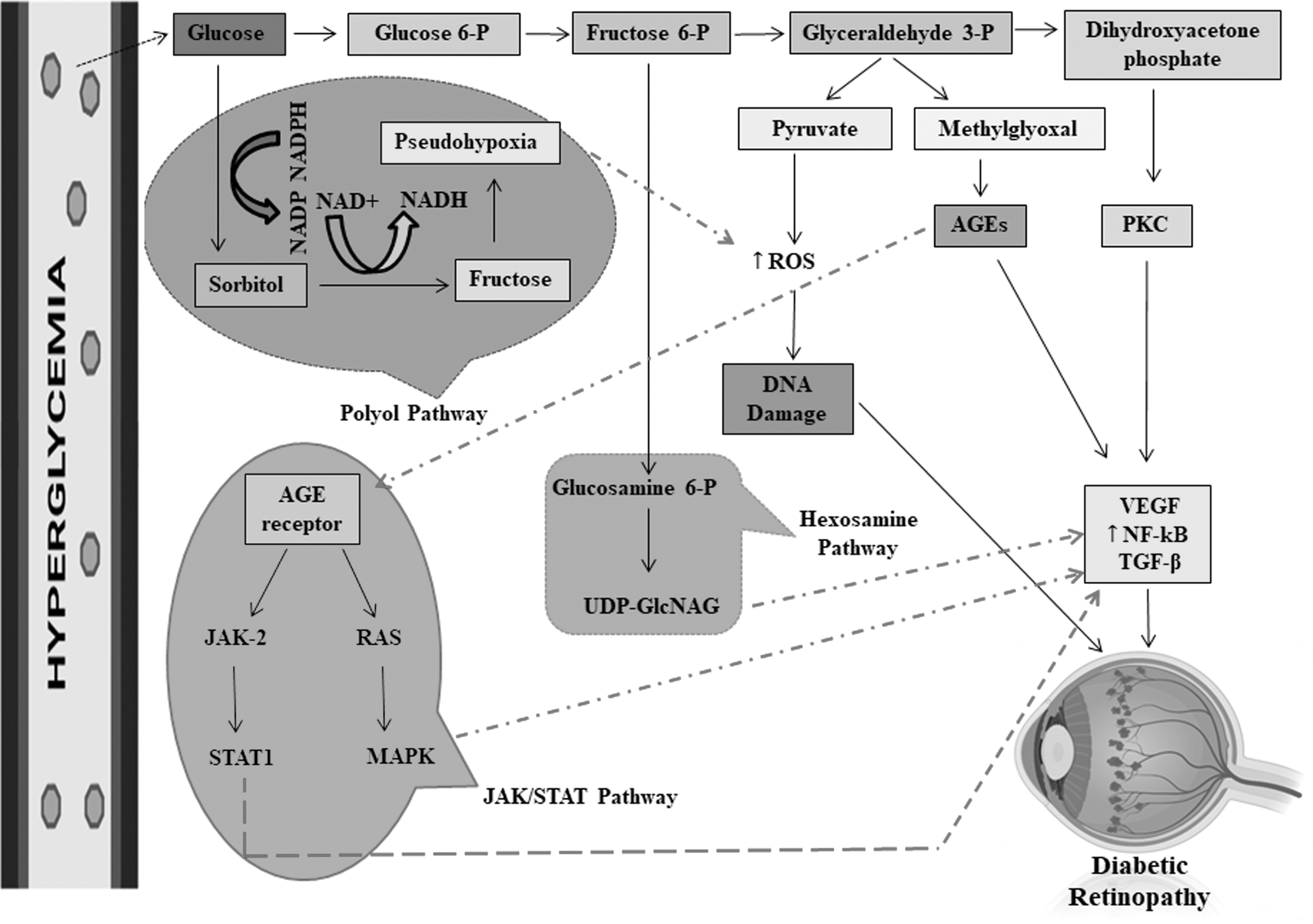
Polyol pathway, JAK/STAT pathway, hexosamine pathway, PKC, AGEs. In DR, hyperglycemia triggers a cascade of molecular pathways, including the activation of the polyol pathway, JAK/STAT pathway, hexosamine pathway, PKC, and the formation of AGEs. These processes contribute to the generation of ROS within the retina. In addition, hyperglycemia leads to increased levels of inflammatory molecules such as VEGF, NF-κB, and TGF-β. Collectively, these interconnected mechanisms play a significant role in the development and progression of DR. AGEs, advanced glycation end products; DR, diabetic retinopathy; JAK, Janus kinase; MAPK, mitogen-activated protein kinases; NADP, nicotinamide adenine dinucleotide phosphate; NADPH, nicotinamide adenine dinucleotide phosphate; NF-κB, nuclear factor-light-chain-enhancer of activated B cells; PKC, protein kinase C; RAS, rat sarcoma virus; ROS, reactive oxygen species; STAT, Signal transducer and activator of transcription; TGF-β, transforming growth factor-β; VEGF, vascular endothelial growth factor.
Polyol pathway
The polyol pathway is a glucose metabolic pathway that becomes active under diabetic conditions and occurs in 2 steps. In the first step, glucose is reduced to sorbitol, and in the second step, sorbitol is converted into fructose. When intracellular glucose levels rise, the polyol pathway is activated. 10 The key rate-limiting enzyme in this pathway is aldose reductase (AR). AR utilizes NADPH as a co-factor to convert glucose to sorbitol. Sorbitol is then further metabolized to fructose by the enzyme sorbitol dehydrogenase, with NAD+ serving as the co-factor in the conversion process. 11
In addition to its role in sorbitol and fructose conversion, the polyol pathway has other implications. NADH, which is produced during the polyol pathway, participates in the methylation of glyceraldehyde 3-phosphate by the enzyme glyceraldehyde 3-phosphate dehydrogenase. This process ultimately contributes to the generation of advanced glycation end products (AGEs). 11 Through increased AR activity and ion flux, the polyol pathway modulates other signaling pathways. It has implications in altering cellular functions and contributes to the development and progression of diabetic complications.12–14
Hexosamine pathway
Elevated glucose levels in hyperglycemia lead to the activation of the hexosamine pathway, which has been observed to be upregulated in retinal tissues of diabetic patients. In the hexosamine pathway, glucose is phosphorylated, resulting in the formation of fructose-6-phosphate. Fructose-6-phosphate is then converted to glucosamine-6-phosphate by the enzyme fructose-6-phosphate aminotransferase. Glucosamine-6-phosphate can undergo acetylation and isomerization, leading to the formation of N-acetyl glucosamine-6-phosphate. This compound serves as a precursor for the synthesis of UDP-GlcNAc (diphosphate uracil-N-acetyl glucosamine), which is utilized as a primary substrate for the addition of glycosyl side chains during post-translational modifications of proteins and lipids.15–17
The hexosamine pathway plays a role in mediating the toxic effects of reactive oxygen species (ROS) in hyperglycemia. The elevated levels of glucosamine produced through this pathway contribute to ROS generation in mitochondria, resulting in impaired mitochondrial respiration, oxidative stress, and promotion of angiogenesis. This cascade of events has a detrimental effect on cellular function and contributes to the pathogenesis of DR.16,18,19
AGE pathway
Hyperglycemia leads to a significant increase in the nonenzymatic glycation of proteins, involving glucose, fructose, and other saccharides. This process results in the accumulation of AGEs through a series of reactions known as the AGE formation. 20 Glycation occurs when reducing sugars react with proteins or other macromolecules, forming an unstable Schiff base that rearranges to generate glycosylation products, mainly carbonyl compounds. These carbonyl compounds undergo oxidation, dehydration, and cross-linking with proteins, leading to the formation of irreversible and stable AGEs. The formation of AGEs involves the production of large amounts of free radicals, further promoting AGE accumulation. Nonenzymatic cross-links between glucose and amino groups within proteins lead to structural and functional damage. 21 The engagement of AGEs with their receptor RAGE (receptor for AGE) triggers nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) activation, leading to apoptosis of retinal pericytes and increased vascular endothelial permeability.
In addition, the interaction between AGEs and RAGE activates NADP oxidases, increasing the generation of ROS during the process. Other studies suggest that AGEs can stimulate ROS production through the mitochondrial electron transport chain. The enhancement of ROS levels further promotes the formation of AGEs and the expression of RAGE, exacerbating the detrimental effects mediated by AGEs in DR.8,22,23
PKC pathway
The PKC pathway plays a crucial role in the pathogenesis of DR induced by oxidative stress. Multiple isoforms of PKC, including PKC-α, PKC-β, PKC-δ, and PKC-ɛ, are activated during the development of DR.24,25 PKC is a serine/threonine kinase involved in signal transduction. Elevated glucose levels in hyperglycemia lead to increased flux through the glycolysis pathway, resulting in augmented diacylglycerol synthesis. Accumulated DAG activates PKC within cells.26,27 Preclinical and clinical studies have demonstrated that diabetes leads to DAG accumulation and hyperactivation of PKC. The initiation of PKC involves the buildup of DAG.28,29 Activation of PKC has several consequences. First, it reduces the activity of Na+/K+-ATPase in smooth muscles, resulting in the inhibition of transient receptor potential ion channels (TRPV1) and subsequent restoration of nerve conductivity.12,30,31
In addition, PKC inhibits the enzyme responsible for nitric oxide (NO) synthesis in blood vessels, thereby diminishing endothelial NO production. Furthermore, PKC promotes the secretion of proinflammatory cytokines, vasoconstriction, and tissue hypoxia by upregulating endothelin-1. Activation of PKC-δ can lead to excessive collagen formation, leading to thickening and stiffening of blood vessels.16,32–34
JAK/STAT pathway
The Janus kinase–signal transducer and activator of transcription (JAK-STAT) signaling pathway involves several key STAT protein subunits. In addition to STAT proteins, this pathway comprises ligand-receptor conjugates and JAK (Janus kinase). The JAK family includes tyrosine kinase 2, JAK1, JAK2, and JAK3 (TYK2).
35
The JAK-STAT signaling cascade occurs as follows:
Inhibitors (IFNs), interferon-6 (IFN-6), interleukin-6 (IL-6), and somatostatin (GH) bind to receptors located on the cell membrane, forming ligand-receptor conjugates. Ligand-receptor binding activates the receptors, leading to the activation of JAK, which phosphorylates the JAK protein. Phosphorylated JAK, in turn, phosphorylates STAT proteins. Phosphorylated STAT proteins form homodimers or heterodimers and translocate to the nucleus as part of the transcription factor complex. In the nucleus, these dimers regulate the transcription of inflammatory genes, including IL-1, IL-6, and tumor necrosis factor-alpha (TNF-α), influencing cellular biological functions.36,37
STAT proteins play essential roles as signaling molecules and transcriptional regulators for various cytokines, hormones, and growth factors. Dysregulation of STAT levels has been observed in the serum and ocular tissues of individuals with diabetes. 38 Of note, ocular surface tissues in patients with type 1 diabetes mellitus (T1DM) showed significantly elevated levels of STAT proteins in conjunctival impression cytology samples. Furthermore, emerging evidence indicates that STAT proteins are upregulated in DR. Increased glucose variability in individuals with type 2 diabetes mellitus (T2DM) predicts the development of PDR and diabetic macular inflammation, serving as a risk factor for diabetes complications. The JAK-STAT pathway is associated with a higher number of genes related to glucose fluctuation. 39
Gene prioritization analysis using the Toppergene system CCHMC and protein–protein interaction network analyses have revealed a strong correlation between STAT3 and glucose variability, underscoring the critical role of STAT proteins in glucose fluctuation. Furthermore, abnormally elevated expression levels of STAT1, STAT3, and STAT5 have been identified in the serum of patients with DR. Of note, the levels of STAT3 in the serum were significantly higher in subjects with DR compared with healthy controls and individuals with diabetes but without DR, after ruling out other systemic and ocular conditions.40,41
Oxidative stress
The excessive production of ROS leads to the oxidation of biomolecules, including DNA, proteins, carbohydrates, and lipids. Hyperglycemia raises intracellular glucose levels, which promotes several biochemical pathways involved in ROS generation. The polyol pathway is one such example, in which excess glucose is converted into sorbitol by the enzyme AR. 11 Increased Ang II levels in hypertension, which is frequently associated with diabetes, contributes to ROS generation within the retina. Hypertension causes vascular damage and weakens the blood–retinal barrier, allowing inflammatory cells to infiltrate and exacerbating oxidative stress. 42 In addition, the local RAS within the retina, as well as Ang II's stimulation of NADPH oxidase (NOX), play critical roles in initiating the oxidative stress cascade that contributes to retinal damage in DR. 43 This oxidative stress occurs when endogenous antioxidant defense mechanisms become overwhelmed.
In the context of the diabetic retina, oxidative stress plays a crucial role in initiating, modulating, and interconnecting the complex network of pathogenic events observed in DR.44,45 Antioxidants have the potential to mitigate the generation of ROS, scavenge free radicals, and reinforce the antioxidant defense system, thereby slowing down the progression of DR. Effective reduction of oxidative stress can lead to detoxification of oxidants in the diabetic retina. 46
In DR, the overproduction of intracellular free radicals, coupled with impaired antioxidant defense mechanisms, including mitochondrial manganese superoxide dismutase (MnSOD) and reduced glutathione (GSH), contributes to oxidative imbalance and mitochondrial dysfunction in the retina. Certain biomarkers associated with oxidative stress have shown altered concentrations in patients with DR, suggesting their potential utility in facilitating early and accurate diagnosis. The retina's response to oxidative stress and its antioxidant defense system resemble those of other susceptible cell types and neurons, which are particularly vulnerable to excessive ROS levels owing to weak or absent antioxidant protection mechanisms.17,47
Thioredoxin interacting protein
Thioredoxin (TRX) interacting protein (TXNIP), also known as vitamin D3 upregulated protein 1 (VDUP1), is known to be upregulated in patients with diabetes and plays a critical role in the pathogenesis of diabetes.48,49 TXNIP, a homodimer connected by a disulfide bond, belongs to the arrestin family. TRX, an antioxidant protein acting as a secondary line of defense, interacts with inactive or reduced TXNIP, thereby suppressing its antioxidant activity. Under normal conditions, TXNIP binds to TRX2 in the nucleus and TRX1 in the cytoplasm. However, during oxidative stress, translocation of TXNIP to the mitochondria triggers activation of apoptosis signaling cascades, including apoptosis signaling kinase-2 (ASK-2) and caspase-3–dependent cellular pathways. Furthermore, TXNIP disrupts TRX reductase enzyme function by forming a cysteine 247-TRX conjugate through oxidative means. The movement and accumulation of TXNIP are crucial for maintaining redox equilibrium within cells.50,51
Elevated glucose levels result in the oxidation and S-nitrosylation of TRX-1 at cysteine-73, mediated by excessive ROS production and prolonged TXNIP expression. Consequently, TXNIP initiates and activates the assembly of the NOD (nucleotide oligomerization domain)-like receptor pyrin domain containing protein-3 (NLRP3) inflammasome. This intricate molecular cascade is necessary for managing redox balance and orchestrating inflammatory responses within cells. 52 An overview of the pathway is given in Fig. 2.
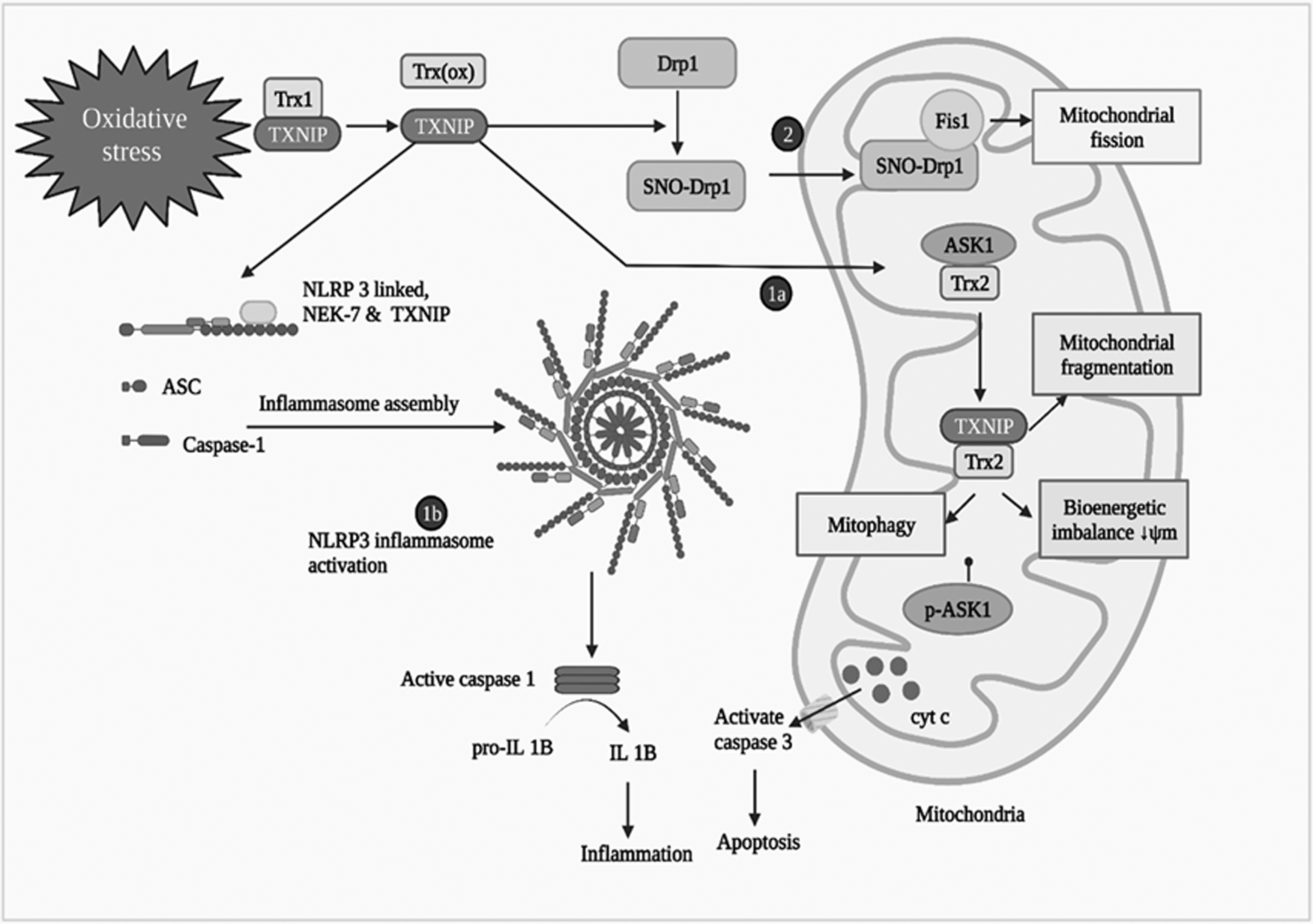
Role of TXNIP in diabetic retinopathy (reprinted with permission from doi.org/10.1016/j.phrs.2022.106292). Elevated glucose levels and oxidative stress upregulate TXNIP expression in retinal cells. TXNIP contributes to retinal inflammation and vascular dysfunction by promoting the production of ROS, activating inflammatory signaling pathways, and inducing endothelial cell apoptosis. , ASK-2, Apoptosis signaling kinase-2; NLRP3, NLR family pyrin domain containing 3; NOD, Nucleotide oligomerization domain; TRX, thioredoxin; TXNIP, thioredoxin interacting protein; VDUP1, vitamin D3 upregulated protein 1.
Peroxisome proliferator–activated receptor
Peroxisome proliferator–activated receptors (PPARs) are nuclear receptors that respond to fatty acids and play a role in regulating glucose and lipid metabolism through various mechanisms. There are 3 types of PPARs: PPAR-α, PPAR-β/δ, and PPAR-γ. 53 PPAR-γ is a nuclear receptor that binds to unsaturated fatty acids and hypolipidemic medications. Activation of PPAR-γ improves mitochondrial function and energy metabolism, although there are currently no medications specifically targeting PPAR-γ. Several synthetic ligands have been developed to broaden the therapeutic applications of PPARs. PPAR activation in endothelial cells (ECs) plays a role in NO production and the antioxidant response.54,55
PPAR activation has been shown to prevent diabetes-induced retinal leukostasis and microvascular leakage by increasing endothelial nitric oxide synthase (eNOS) activity, reducing oxidative stress, and suppressing apoptosis, inflammation, and angiogenesis. Research indicates that PPARs are downregulated in diabetic eyes, and their disruption contributes to the development of DR. Pharmacological activation of PPARs has demonstrated therapeutic effects against various ocular degenerative diseases. Decreased PPAR expression has been associated with retinal inflammation and neovascularization. 56
In conditions of oxidative stress induced by 4-hydroxynonenal (4-HNE), fenofibric acid, an active metabolite of fenofibrate that acts on PPARs, has been reported to reduce oxidative stress and cell death in retinal neuronal cell lines. In diabetes, PPAR activation enhances retinal NADH (nicotinamide adenine dinucleotide + hydrogen) oxidation, suggesting that PPAR activation may reverse mitochondrial dysfunction caused by oxidative stress.57,58
TGF-β in DR
The TGF superfamily encompasses a collection of >30 members, which include prototypes like TGF-1, activins, nodals, and bone morphogenetic proteins. TGF-ligand signaling relies on type II receptors, such as TGF-β receptor 2, in conjunction with BMP receptor 2, as well as type I receptors referred to as activin receptor-like kinases (ALKs 1–7).59,60 Upon ligand engagement, activated receptor complexes utilize Smad nuclear shuttling transcriptional effectors as the primary signaling mechanism. However, there are also instances of Smad-independent mechanisms, such as the MAPK and PI3-kinase Akt pathways, through which signals can be transmitted. TGF-β induces ALK5 activation, resulting in the phosphorylation of Smad 2/3, subsequently facilitating their relocation to the nucleus and control over gene expression.
Although TGF-β signaling is known to play a role in the pathophysiology of DR, its precise molecular basis remains unknown. The widely expressed type I receptor ALK5 inhibits EC growth and migration by activating Smad 2/3. However, the endothelial-specific type I receptor ALKI, in conjunction with its coreceptor endoglin, generates Smad 1/5/8-dependent transcriptional messages that promote EC proliferation and angiogenesis.61,62 In the vascular system, TGF-β can either promote or inhibit angiogenesis. A study specifically examining TGF signaling in retinal microvasculature ECs and pericytes revealed that pericytes exhibited higher responsiveness to TGF-β–induced Smad 2 activation and increased fibronectin generation, whereas ECs displayed increased sensitivity to Smad 1/5/8 activation, leading to proangiogenic effects in isolated pericytes. Consequently, elevated levels of TGF-β in the vitreous of PDR patients appear to be another critical factor in the progression of DR. 63
TNF-α in DR
Patients diagnosed with PDR or proliferative vitreoretinopathy (PVR) exhibit elevated levels of lipid peroxides and myeloperoxidase activity within their vitreous and epiretinal membranes. The activation of leukocytes triggers an increase in the production of cyclooxygenase and lipoxygenase enzymes, which convert arachidonic acid into peroxide metabolites. 64 Subsequently, these peroxide metabolites induce the release of cytokines through a positive feedback mechanism. During ischemic conditions, phagocytic cells become activated and release TNF, interleukin 1, and interferon, among other chemical mediators.65,66 These substances promote neovascularization (formation of new blood vessels) and the adhesion of leukocytes to ECs. In addition, TNF-α stimulates retinal pigment epithelial cells to produce monocyte chemotactic protein, further amplifying the self-stimulatory nature of the process. The involvement of inflammatory cells significantly contributes to the pathogenesis of PVR. Consequently, this heightened stimulation plays a significant role in the progression of PVR.67–69
Aldosterone role in DR
Aldosterone has emerged as a pivotal mediator in the pathogenesis of DR, with evidence suggesting that blocking the mineralocorticoid receptor (MCR) can effectively halt the onset and progression of this condition.70–72 Intriguingly, studies have revealed that hyperglycemia stimulates the expression of cytochrome P450 family 11 subfamily B member 2 (CYP11B2), consequently elevating renal aldosterone levels. The production of aldosterone by mesangial cells in the kidney, triggered by angiotensin II (ANG II), leads to the accumulation of extracellular matrix (ECM), contributing to DR. 73 Of note, there is a localized aldosterone system implicated in podocyte damage among individuals with diabetes. In addition, ANG II has been identified as a mediator of renal impairment in diabetes, further emphasizing the pathogenic role of ANG II within the renin–angiotensin–aldosterone system (RAAS).74–77
Another key component of the RAAS that holds potential importance and is implicated in the development and progression of DR is aldosterone. Studies have demonstrated that aldosterone induces kidney damage by modulating the expression of plasminogen activator inhibitor-1 (PAI-1). Furthermore, aldosterone synthesis in diabetic kidneys promotes inflammation and the formation of matrix. By inhibiting the production of growth factors and ROS, aldosterone also accelerates the breakdown of the ECM. Therefore, using aldosterone antagonistic therapy may represent a promising treatment approach for DR, effectively mitigating its progression.78–81
Role of adenosine in DR
Adenosine receptors are classified into 4 subtypes associated with G proteins: A1, A2A, A2B, and A3. The A1 receptor, which exhibits the highest affinity for adenosine, utilizes Gi and Go proteins.82–87 Activation of the A1 receptor leads to the inhibition of adenylate cyclase, activation of phospholipase C, and opening of ATP-sensitive potassium channels (K+ATP) channels. The A2 receptors, coupled to the Gs-protein, activate N-type Ca2+ channels and stimulate adenylate cyclase. 88 The transduction system involves the activation of phospholipase C/D and inhibition of adenylate cyclase. The A3 receptor is coupled to Gi and Go proteins. Ecto-5'N is the primary source of adenosine (CD73) in most tissues.84,85
Studies using enzymes and immunohistochemistry have revealed that glycoprotein 5'N is present in specific domains of Müller cells in both adult and developing retinas of humans, mice, and dogs. Adenosine, which is the primary product of 5'N, serves as an intercellular signaling molecule in the retina.82,83,86 Adenosine regulates blood flow in the retina and is released in response to ischemia in adults and newborns. Research indicates that activation of the A1 receptor protects against the detrimental effects of ischemia/reperfusion (I/R), whereas A2A receptor stimulation may exacerbate those effects.87,88
Cannabinoid receptor in DR
The 3 most prominent cannabinoids derived from marijuana are tetrahydrocannabinol (THC), cannabinol (CBN), and cannabidiol (CBD). 89 These cannabinoids possess well-established therapeutic properties in terms of antioxidation and anti-inflammation. The biological effects of cannabinoids are mediated through at least 2 receptors, namely CB1 and CB2.90–92 The CB1 receptor, found in the brain and retinal neurons, is responsible for the psychoactive effects, whereas the CB2 receptor is expressed in immune cells, cerebral microglial cells, and the retina of the eye. These receptors interact with Gi/Go proteins to inhibit immediate early gene signaling pathways and adenylyl cyclase activity.93,94 In addition, the CB1 receptor, through Gi/Go proteins, activates potassium channels and inhibits voltage-sensitive calcium channels.93,95
CBD demonstrates potent ROS scavenging capabilities, making it effective in combating oxidative stress. It exhibits stronger antioxidant effects than α-tocopherol and ascorbate, as it can scavenge ROS and inhibit NOX. In the presence of CBD, human coronary ECs exhibit a reduced inflammatory response and enhanced barrier integrity when exposed to high glucose levels. Moreover, CBD has been shown to reduce the incidence of diabetes in nonobese diabetic mice. Tetrahydrocannabinoids, such as CBD, have the potential to inhibit ENT1 absorption in murine microglia. 93 CBD can enhance adenosine signaling through noncannabinoid receptor mechanisms and by inhibiting uptake. Furthermore, CBD possesses anti-inflammatory properties and can mitigate inflammation induced by endotoxins.96–98
Renin–angiotensin system in DR
Angiotensinogen serves as the sole precursor of angiotensin peptides within the renin–angiotensin system (RAS) enzyme-mediated cascade. The initiation of this cascade involves the conversion of pro-renin, an inactive form of renin, into active renin. Renin, in turn, degrades angiotensinogen to generate angiotensin I (ANGI).Various enzymes play a crucial role in the conversion of angiotensin I (ANG I) into angiotensin II (ANG II). These enzymes include angiotensin-converting enzyme 1 (ACE1), tonin, trypsin, kallikrein, cathepsin G, and chymase. Together, they facilitate the transformation of ANG I into ANG II.42,99 Of interest, apart from ANG I, there is evidence suggesting the existence of an upstream precursor called angiotensin-(1–12). This precursor can directly generate ANG II through the action of the serine protease chymase, providing an alternative non-ACE pathway.43,100
The primary targets of ANG II, the main effector peptide of the RAS, are the angiotensin type 1 (AT 1) and angiotensin type 2 (AT 2) receptors. Among these receptors, the angiotensin type 1 receptor, a 7-transmembrane domain G protein–coupled receptor, mediates the majority of ANG II's known activities. It is expressed in various tissues, including the heart, prostate, eye, and vasculature.101,102 Elevated plasma pro-renin levels have been observed in patients with DR, indicating an activation of the RAS. The severity of DR may be associated with plasma pro-renin levels.103–105
Although pre-PDR (pre-PDR) may cause an increase in plasma pro-renin, its levels may not change significantly during the progression from no retinopathy to background retinopathy.106,107 Although the retina produces relatively low levels of renin compared with other tissues, the eye may serve as an extra-renal source of plasma pro-renin in diabetes. Studies have found higher levels of pro-renin in the vitreous fluids of PDR patients compared with nondiabetic patients experiencing spontaneous retinal detachment.108,109
The concentrations of pro-renin and renin in ocular fluids exhibit variations, with the posterior vitreous showing the highest levels, followed by the anterior vitreous and then the aqueous humor. This suggests that the posterior segment of the eye primarily contributes to the ocular fluid's pro-renin content.110,111 Figure 3 provides a diagrammatic representation of the insulin signaling pathways in DR, specifically mediated by angiotensin-converting enzyme (ACE II).

Role of angiotensin-converting enzyme (ACE II)–mediated insulin signaling pathways in DR. In diabetes, the RAS is dysregulated, leading to increased levels of angiotensin II (Ang II) and activation of its receptors. Ang II promotes vasoconstriction, inflammation, oxidative stress, and the release of pro-inflammatory cytokines. These effects contribute to endothelial dysfunction, increased vascular permeability, and the formation of retinal micro aneurysms. Furthermore, Ang II stimulates the production of VEGF, a key driver of abnormal angiogenesis and retinal neovascularization in DR. GLUT4, Glucose transporter protein type-4; IL-6, interleukin-6; IRS-1, insulin receptor substrate 1; JNK, Jun N-terminal kinase; PI3K, phosphoinositide 3-kinase; PKB, or Akt, protein kinase B; PIP2, phosphatidylinositol-4, 5-bisphosphate; PIP2, phosphatidylinositol (4,5)-bisphosphate PIP3; phosphatidylinositol (3,4,5) trisphosphate; SOCS, suppressor of cytokine signaling.
Matrix metalloproteinases
Except for collagen, almost all types of extracellular matrix components are degraded by zinc-dependent endopeptidases known as matrix metalloproteinases (MMPs). In pathological conditions, MMPs are induced in the retina, leading to the remodeling of the extracellular matrix. The activity of MMPs is regulated by endogenous inhibitors called tissue inhibitors of metalloproteinases (TIMPs), including macroglobulins. Among the 4 members of the TIMP group, TIMP-1 preferably inhibits MMP-9, whereas TIMP-2 has a higher affinity for MMP-2.112,113 The MMP-9 promoter contains several functional cis-regulatory regions that are regulated by multiple transcription factors. Regulating active MMPs can protect retinal capillary cells from apoptosis by preserving mitochondrial ultrastructure and function, as well as reducing DNA damage. This suggests that targeting MMPs could be a potential therapeutic approach for treating DR.114,115
In DR, MMP-9 is released by cells, directly contributing to angiogenesis and impairing the blood–retinal barrier, thereby diminishing retinal neuroprotection. MMPs, along with NF-κB, are activated in hyperglycemic conditions, leading to apoptosis in retinal capillary cells.116–118 An outline of the pathway along with the inflammatory molecules is given in Fig. 4.
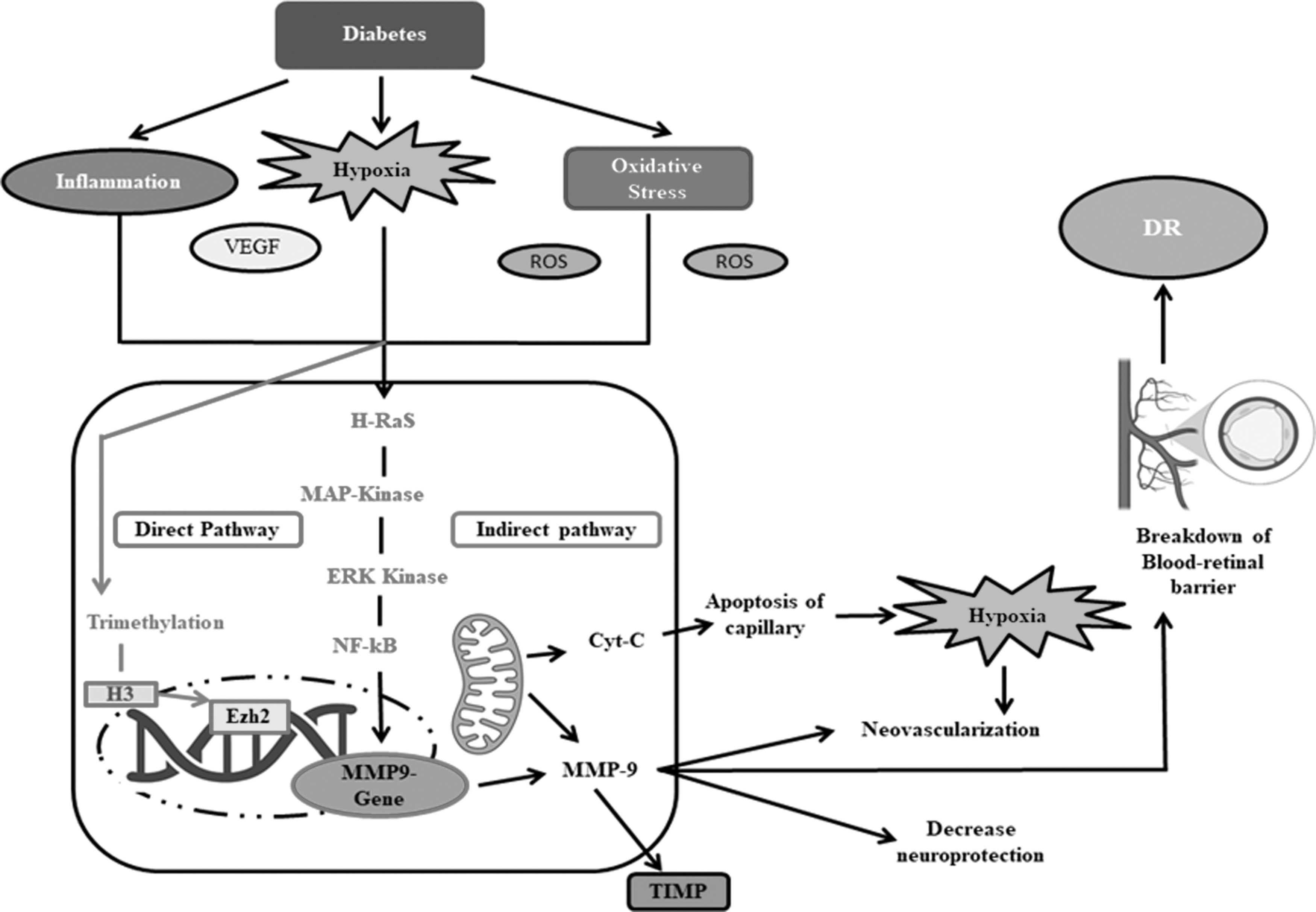
MMP9 in DR. The dysregulated expression and activity of MMPs contribute to the breakdown of the blood-retinal barrier, the development of retinal neovascularization, and the promotion of inflammation within the retina. MMPs, particularly MMP-2 and MMP-9, are implicated in the degradation of the extracellular matrix, leading to basement membrane dysfunction, and increased vascular permeability. These processes contribute to the progression of DR and its associated complications. EZH2, H3 histone, enhancer of zeste homolog 2; ERKs, extracellular signal–regulated kinases; HRas, Harvey Rat sarcoma virus; MAPK, mitogen-activated protein kinases; MMP-9, matrix metalloproteinase-9; TIMP, tissue inhibitor of metalloproteinases.
NADPH oxidase
NOXs are the primary producers of cytosolic ROS, and one of these enzymes, NOX2, plays a crucial role in ROS production within the retina.119,120 NOX2 is a multi-component protein that includes transmembrane and cytosolic proteins, as well as the miniature G-protein. The activation of NOX2-ROS and Rac1 has been associated with mitochondrial dysfunction and the development of retinopathy.121,122 NOXs catalyze the formation of free radicals by transferring an electron from NADPH to oxygen. Accumulation of free radicals leads to compromised structural and functional stability of mitochondria, resulting in the leakage of cytochrome c into the cytoplasm and the acceleration of capillary cell death.120,123 NOX-derived ROS contribute to the pathogenesis of DR by causing oxidative injury and acting as signaling molecules to regulate cellular activities. Suppression of inflammation may be a promising strategy for managing DR.124,125
The components of NOX are expressed in the retinal vasculature of the eye. Inhibition of NOX prevents diabetes-induced retinal inflammation and the early stages of retinopathy. Excessive production of ROS under conditions of oxidative stress is a primary cause of diabetes complications, including DR. 119 Given that the sole function of the NOX enzyme family is the generation of ROS, it is an interesting target for therapeutic intervention in DR. In oxygen-induced retinopathy, inflammatory cytokines such as TNF-α and IL-1β reduce retinal avascularity while suppressing revascularization. Administration of exogenous antioxidants, such as superoxide dismutase or pharmaceutical antioxidants, significantly improves ischemic retina revascularization. 126
Kinin–Kallikrein system
The kallikrein–kinin system (KKS) comprises 2 independent proteolytic pathways that generate bradykinin peptides and activate bradykinin receptors. 127 Tissue kallikrein and plasma kallikrein (PK) mediate these pathways. Bradykinin peptides play a crucial role in mediating the effects of the KKS on retinal vascular permeability. PK, a zymogen similar to trypsin, is present in the plasma, with its active site located in the light chain. The delicate chain of PK is stimulated by protease inhibitors.128,129
The KKS regulates several critical processes involved in the development of DR, including angiogenesis, innate immunity, thrombosis, and inflammation. The kinin receptors B1 and B2 are responsible for the breakdown of the blood–retinal barrier and increased plasma extravasation in DR. In the human eye, there are 4 carbonic anhydrase (CA) isoforms (CA I, II, IV, and XIV).130,131 CA I, found in retinal ECs, may contribute to increased retinal permeability. Activation of the retinal vasculature, particularly in the presence of molecules such as CA-1 and heparin, triggers the activation of the KKS pathway. Reducing the activation of the contact system may present opportunities to mitigate the effects of the KKS in DR. 110 A diagrammatic representation of the KKS is given in Fig. 5.

Role of KKS in DR. In diabetes, dysregulation of the KKS leads to increased activation of kinin receptors and excessive production of bradykinin. Bradykinin promotes vasodilation, inflammation, and increased vascular permeability within the retina. These effects contribute to the breakdown of the blood–retinal barrier and the formation of retinal edema. Moreover, bradykinin stimulates the release of VEGF, a key mediator of abnormal angiogenesis in diabetic retinopathy. ALK1, Activin receptor-like kinase 1; B1R, bradykinin receptor B1; B2R, bradykinin receptor B2; BK, bradykinin kinase; DABK, desArg9-Bradykinin; HK, histidine kinases; iNOS, inducible nitric oxide synthetase; KKS, kallikrein–kinin system; LRG1, leucine-rich α-2 glycoprotein 1; NADPH, nicotinamide adenine dinucleotide phosphate; NOS3, endothelial nitric oxide synthase 3; PLA, proximity ligation assay; PPK, pickpocket receptors, coagulation factor 12; SMAD, suppressor of mothers against decapentaplegic; TGF-β, transforming growth factor beta; TGF-βRII, transforming growth factor beta receptor 2.
Therapeutic Management of DR
To prevent vision loss/recovery of sight, current treatments for DR include laser surgery, medication, and vitrectomy surgery. 132 Intraocular pharmacotherapy, particularly anti-inflammatory [corticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs)] and anti-angiogenic (vascular endothelial growth factor [VEGF] inhibitors), has gained popularity among patients suffering from DR.133,134 Although the conventional therapeutic strategy reduces the therapeutic burden of DR among patients, yet a number of drawbacks exists for each class of drugs. Some of the recent research indicates that phytopharmaceuticals and repurposed drugs have promising therapeutic effect against amelioration of DR. 135 An overview of the currently used drugs and repurposed drugs for DR is given in Table 1 along with their mechanism of action and possible side effects.136,137
Currently Approved Drugs for the Management of Diabetic Retinopathy
ROS, reactive oxygen species; VEGF, vascular endothelial growth factor.
Corticosteroids
Prednisone, triamcinolone, 161 betamethasone, methylprednisolone, and dexamethasone 162 are chemically synthesized analogues of hydrocortisone and cortisone with reduced mineralocorticoid properties that allow them to be used for their anti-inflammatory properties. 163 Corticosteroids' anti-inflammatory effect suppresses angiogenesis and neovascularization (eg, VEGF, transforming growth factor) by limiting outer membrane disintegration (a step required for angiogenesis), EC migration, and growth factor production. Corticosteroids, dexamethasone, triamcinolone, and fluocinolone acetonide have been shown to be beneficial in the treatment of this condition, making them an appealing therapy option. 164 These medications inhibit VEGF and a number of cytokines.
Unfortunately, because many disorders are chronic, numerous injections are frequently required, which reduces patient compliance and increases the risk of problems over time. 146 There is a risk of vitreous hemorrhage, cataract progression, and retinal detachment with each injection, among other complications. 148 Ocular hypertension is one of the most common side effects.140,165
Anti-VEGF
VEGFs play a critical role in the pathogenesis of choroidal neovascularization and the regulation of vascular permeability. The VEGF family encompasses 5 distinct molecules: VEGF-A, VEGF-B, VEGF-C, VEGF-D, VEGF-E, VEGF-F, and placental growth factor. 166 Among them, VEGF-A exhibits binding affinity to the pivotal receptors VEGF receptor 1 (VEGFR-1) and VEGF receptor 2 (VEGFR-2), which mediate its diverse physiological and pathological effects. These interactions contribute to the complex interplay between VEGF-A and its receptor signaling cascades, ultimately influencing angiogenesis and vascular permeability. 167 In response to hypoxia, various cells, particularly retinal ECs, pericytes, and retinal pigment epithelial cells, release the VEGF family of growth factors.168,169 Although VEGF-A is currently the primary target in treatments, VEGF-C and VEGF-D also play important roles in angiogenesis and vascular permeability. VEGF-C and VEGF-D upregulation can limit the efficacy of selective VEGF-A inhibition, resulting in resistance in some patients. OPT-302, a fusion protein developed by Opthea Limited, however, specifically binds to and neutralizes the activity of VEGF-C and VEGF-D, potentially improving treatment.167,170 The first anti-VEGF medication used to treat DME was pegaptanib, which targets the 165 isoform of VEGF. 171 Ranibizumab (Lucentis; Genentech USA) is a humanized, engineered recombinant antibody fragment (Fab) that is effective against all VEGF-A isoforms.142,171 Its half-life is shorter than other anti-VEGF drugs and lacks the Fc domain. Lucentis is an FDA-approved intravitreal agent intended to ameliorate wet age-related macular degeneration (AMD). 172 Abicipar pegol is a protein-binding molecule with a high affinity for soluble VEGF-A isoforms. When compared with ranibizumab (48 kDa), it has a lower molecular weight (34 kDa) and a higher binding affinity. These properties, combined with its longer intraocular half-life (>13 days in the aqueous humor), contribute to abicipar's expected durability, which outperforms currently available anti-VEGFs. 170 Pegaptanib is a 28-nucleotide RNA aptamer that is targeted to specifically bind to the VEGF-A165 isomer, that is considered as the main pathogenic VEGF protein in ocular tissues. Aflibercept (VEGF Trap-Eye) is a synthetic protein complex made up of the essential VEGF binding sites of human VEGF receptors 1 and 2. In 2011, the FDA granted approval to aflibercept as a therapeutic option for the management of neovascular AMD. Conbercept has not yet been subjected to a level I randomized clinical trial, but it has the potential to be the fifth most effective anti-VEGF agent. Bevacizumab, ranibizumab, and aflibercept were all equally effective in treating eyes with DME involving the center.152,173
Tarcocimab tedromer (KSI-301) developed by Kodiak Sciences is an investigational anti-VEGF drug administered through intravitreal route for the treatment of a variety of eye conditions, including DR. The drug candidate is a bioconjugate of 950 kDa made up of 2 parts. 174 The first component is a fully humanized recombinant monoclonal antibody that specifically targets VEGF. The second component is an optically clear branched phosphorylcholine biopolymer that is securely connected to the antibody. This biopolymer is designed to increase the stability and duration of the bioconjugate within the eye while maintaining its anti-VEGF activity. 143
Brolucizumab, developed by Novartis (Cambridge, MA), received FDA approval in 2019 for exudative AMD and in 2022 for diabetic macular edema (DME). Brolucizumab, weighing 26 kDa, is a recombinant monoclonal single-domain antibody that selectively binds to VEGF-A at a solitary binding site. Faricimab, developed by Roche in Basel, Switzerland, was FDA approved in 2022 for wet AMD and DME.175,176 Faricimab is a dual-mechanism antibody with a size of 149 kDa. It comprises 2 separate antigen-binding fragment regions, one specific to VEGF and the other to ANG II, both linked to a single Fc domain. However, both Brolucizumab and Faricimab are under clinical trials and yet remains to approved by FDA for DR. 177
Ensuring adherence to follow-up appointments for anti-VEGF injections is crucial in effectively managing DR and sustaining positive visual outcomes in the long run. From a pharmacokinetics perspective, maintaining adequate drug levels for continuous anti-VEGF therapy necessitates monthly injections. Discontinuation of monthly injections can lead to a prompt deterioration of the disease, even in patients who initially displayed rapid improvement and subsequently remained stable over an extended period. 177 However, there is concern about anti-VEGF therapy permeation and potential systemic side effects. Endophthalmitis and retinal detachment are common risks associated with intravitreal drug administration, in addition to the systemic side effects of anti-VEGF.138,178 There have been reports of corneal damage, chemosis of conjunctival tissues, lens damage, anterior uveitis, vitreous and retinal hemorrhages following intravitreal bevacizumab injection. 179
Nonsteroidal anti-inflammatory drugs
NSAIDs are well known for their excellent analgesic, antipyretic, and anti-inflammatory properties, 180 for which they are among the most commonly prescribed medications. NSAIDs inhibit the cyclooxygenase pathway (COX-1 and COX-2), restricting prostaglandin (PG) production and decreasing the release of indigenous PGs, promoting inflammation. 151 As NF-κB activity influences both iNOS and COX-2 activity, they are frequently produced during inflammation.150,181 iNOS products positively regulating COX-2 expression of its by products, such as PGE2, are dramatically increased in ocular cells of hyperglycemic rats exposed to high glucose levels. 182 COX-2 inhibition, on the contrary, reduces PGE2 synthesis in diabetic rat retinas and prevents leukostasis and ICAM-1 development. 183
These findings suggest that COX-2 may play a role in retinal inflammation and that NSAIDs may be beneficial for the treatment of DR. In ophthalmology, topical NSAIDs are primarily used to treat allergic conjunctivitis, cystoid macular edema and maintain pupil dilation during ocular surgery to reduce postoperative discomfort and inflammation (especially after refractive surgery).181,184 A growing body of research suggests that NSAIDs may help with DR, ocular malignancies, and AMD. 185 Aspirin therapy prevents capillary cell death and vascular degradation in diabetic rats. Specific blockers such as sulfasalazine, aspirin, and sodium salicylate reduce capillary cell death, vessel degradation, and capillary leakage. 149
Other antioxidants
Other antioxidants for treating DR include taxifolin, 186 zinc, sesamin, 187 tempol, 188 hesperetin, 189 resveratrol, 190 and others antioxidant therapy in combination (CAT). According to recent research, combined antioxidant therapy (CAT) is gaining popularity. Garcia-Medina conducted a 60-month trial in 105 T2DM patients with NPDR to assess the effects of antioxidant supplements (lutein, VC, alpha-tocopherol, niacin, beta-carotene, Zn, and Se). 191 This extended follow-up demonstrates that the treatment person's plasma antioxidant level was maintained and that the course of DR was slowed. Another study discovered that taking lutein and zeaxanthin supplements for 3 months improved visual acuity, contrast sensitivity, and foveal thickness in people with T1DM and T2DM. It is fascinating to see how CAT is linked to modern treatments such as anti-VEFG therapy. Lafuente spent 3 years studying 55 T2DM patients. They investigated the efficacy of combining ranibizumab with antioxidant therapy to treat DME. They discovered that the supplemental team's macular diameter was smaller compared with the control group.159,192
Vitamins
Pathological neurovascular diseases have been related to a general deficiency of several vitamins, including vitamin B complex and vitamin D deficiency. 193 UVB sunlight converts the precursor 7-dehydrocholesterol in the skin into vitamin D3, and vitamin D is a fat-soluble steroid hormone that can be absorbed in small amounts through food. 194 Vitamin D3 has been shown to improve DR by restricting ROS generation, the TXNIP/NLRP3 inflammation pathway, along with lowering the expression of VEGF. The antioxidant alpha-lipoic acid lowers GSH levels within cells by controlling the nuclear factor erythroid 2 connected factor ligase for 2-glutamate-cysteine catalytic component (Nrf2-Gclc-GSH). Thus it indirectly modulates the Nrf2-KEAP1 signaling pathway and inhibits NF-κβ. Trolox, a vitamin E derivative, reduces ROS generation and thus, structural damage in an oxygen-induced rat model. 195
Phyto-pharmaceuticals
The use of herbal medicine has grown significantly in recent decades. Traditional medical practices such as Ayurveda, Unani, and traditional Chinese medicine are practiced worldwide for therapeutic intervention of metabolic disorders, including DR. 196
Polyphenols
Polyphenols are a class of chemicals naturally present in plants with antioxidant, anticancer, and anti-inflammatory properties. 197 Polyphenols are also an essential source of anti-infective agents against antibiotic-resistant human pathogens. 198 Rutin is a quercetin-like rutinoside that acts as an antioxidant and a metabolite. Salix atrocinerea and Ficus virens contain rutin. Rutin administration to STZ-induced diabetic rats has been shown to decreases the amount of thiobarbituric acid reactive substances (TBARS), caspase-3, tumor necrosis factor-α, and VEGF while increasing the levels of GSH and Bcl-2, protecting the retina from oxidative and neurodegenerative damage.199–201
Flavonoids and phenolic acid
Flavonoids are bioactive substances found primarily in dietary plants, including those commonly consumed in the human diet, such as fruits, vegetables, cereals, and beverages. 202 Flavonoids have been found to be very effective against DR in numerous studies. 203 Anthocyanins, 204 arctiin, 205 carotenoids (Carotene), 206 chlorogenic acid, 207 baicalein, 208 curcumin, 209 cannabidiol, 93 astaxanthin, 210 naringenin, 52 plantaginis semen, 211 and other novel flavonoids has been reported in the literature to be effective against DR.
Repurposed and pipeline drugs
Antihyperlipidemic drugs
It is well known that diabetic subjects with hyperlipidemia are more likely to develop retinal tough transude. Some antihyperlipidemic drugs lower LDL levels, triglyceride levels, and some others raise HDL levels. 212 Several drugs are demonstrating therapeutic effects in DR via different mechanisms of action. Atorvastatin154,213 and rosuvastatin, 2 statin medications, have been shown in numerous studies to lower diabetic patients' lipid levels and may be especially effective in the treatment of DR. 155
Fenofibrate is a PPAR-α agonist. Fenofibric acid binds to the nuclear hormone receptor PPAR after being transformed into fenofibrate. 214 The retinoid X receptor and the linked PPAR then combine to form a heterodimer, which then attaches to a specific transcription factor receptor—associated with stimulating the production of the target sequence via increasing lipoprotein lipase activity and decreasing apolipoprotein C-III activity via PPAR, 153 which together increase the breakdown of triglyceride-rich particles and extremely LDL. Fenofibrate has a positive effect on the retina of different people with DR, but it appears to be separate from its lipid-lowering actions. 215
Antidiabetic drugs
Antidiabetic medications are used to lower blood glucose levels in diabetic patients. Some diabetes medications, such as metformin and glibenclamide, 156 have been studied to reduce the risk of NPDR and sight-threatening DR. 157 Compared with other hypoglycemic treatments for patients with diabetes, metformin and glibenclamide significantly reduced the likelihood of several macrovascular and microvascular complications associated with diabetes. Compared with diabetic diet therapy, metformin and glibenclamide reduced the possibility of DR progression in obese patients with diabetes as one of the several outcomes. These 2 drugs have demonstrated a therapeutic effect in various studies, suggesting that they may help treat DR.216,217
Antihypertensive drugs
ACE inhibitors like Captopril and Candesartan are effective in lowering blood pressure and reducing the risk of DR by relaxing veins and arteries. These medications work by inhibiting the production of angiotensin II, a compound that constricts blood vessels in the body. 160 Numerous pathological conditions associated with DR, including angiogenesis, inflammation, and oxidative stress, are influenced by altered physiological mechanisms related to angiotensin II. 218 All these incidents eventually culminated in the major issue, oxidative stress.
Several studies have found that angiotensin II is one of the main initiators of oxidative stress, or the production of ROS, which is a known factor in the development of DR. 219 According to a study on produced retinal cells that demonstrated the role of angiotensin II type-1 receptor signaling in oxidative stress–induced retinal neurodegeneration, a key event in the pathogenesis of DR, the most obvious negative consequences of oxidative stress are detected in retinal tissue neuron. Endothelial dysfunction and inflammation are also caused. Animal models of DR have demonstrated that angiotensin II production triggers the formation of superoxide radicals and retinal leukostasis, further implicating angiotensin II–induced oxidative stress in the development of DR. 160
Pipeline drugs under preclinical trials
Several medications are being tested in preclinical and clinical trials with the purpose of treating DR are given in Table 2. Preclinical research is being conducted on OCX 063, a novel molecular entity. The medicine OCX 063133 inhibits retinal angiogenesis and is effective in treating wet AMD, glaucoma, and DME. Another experimental medicine known as AT003220 is being developed to treat DME. The drug has been developed by Applied Therapeutics and works as an AR inhibitor. The medication inhibits AR, an enzyme involved in the pathophysiology of many disorders, including DR.
Novel Molecules Under Phases of Clinical Trial Intended for Diabetic Retinopathy Treatment
NA, not applicable.
Discussion and Future Directions for Management of DR
The safety and efficacy of available therapeutic interventions for DR, as well as the timely diagnosis and management of the condition, pose significant challenges. This review focuses on understanding the molecular mechanisms that contribute to the progression of DR and explores potential therapeutic interventions, including molecules currently undergoing clinical trials. Given the time-consuming and uncertain nature of discovering novel molecules through conventional methods, a promising approach involves repurposing existing drugs in combination with novel agents to target multiple molecular pathways.
To summarize, the field of DR treatment is experiencing promising advancements through the development of slow-release systems that incorporate steroids, anti-VEGF agents, and repurposed drugs. Tarcocimab tedromer, brolucizumab, and abicipar pegol show potential as superior alternatives to aflibercept and ranibizumab, offering the advantage of reduced administration frequency. Moreover, alongside pharmacological interventions, the administration of phytopharmaceuticals has demonstrated positive effects in DR-related models. These natural compounds have shown the ability to alleviate various pathological conditions associated with DR, such as oxidative stress, inflammation, neurodegeneration, and vascular lesions. Nevertheless, more comprehensive studies are required to enhance our understanding of their efficacy and safety before considering their widespread use in managing DR.
Footnotes
Acknowledgment
The authors of this review work are thankful to The Director, CSIR-Central Drug Research Institute for providing all the support to complete the work. The authors acknowledge ![]() that was used for preparation of graphical abstract. Arpon Biswas expresses gratitude to the Indian Council of Medical Research for generously providing essential funding. CSIR-CDRI allotted communication number is 10649.
that was used for preparation of graphical abstract. Arpon Biswas expresses gratitude to the Indian Council of Medical Research for generously providing essential funding. CSIR-CDRI allotted communication number is 10649.
Authors' Contributions
Arpon Biswas conceived the topic, wrote the article, created tables and figures. S.K.V., A.D.C., S.A., A.B., S.N.S., M.K., A.M., S.K., M.C. performed proof reading along with preparation of graphical abstract. R.S.B. revised, edited and approved the final version of the draft.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work is financially supported by the Indian Council of Medical Research, Senior Research Fellowship. Fellowship Number: 3/1/3(2)/OPH/2020-NCD-II.