
Abstract
Purpose:
Diabetes mellitus has been associated with increased dry eye disease (DED) and exacerbates DED's pathology. This preliminary short-term study aimed to evaluate the effects of 3% Diquafosol Sodium ophthalmic solution (DQS) on ocular surface inflammation and corneal nerve density in diabetic dry eye (DDE) patients.
Methods:
In this perspective, participants used 1 drop of 3% DQS (Diquas; Santen Pharmaceutical Co., Ltd., Osaka, Japan) 6 times daily for 8 weeks. Non-invasive tear breakup time (NITBUT), tear film lipid layer (TFLL), conjunctival hyperemia [redness score (RS)], corneoconjunctival staining (CFS), corneal sensitivity (CS), Meibomian gland quality (MGQ) and Meibomian gland expressibility (MGEx), corneal nerve fiber density (CNFD), and Standard Patient Evaluation Eye Dryness (SPEED) questionnaire were assessed at baseline, at weeks 4, and up to 8 weeks. Matrix metalloproteinase-9 (MMP-9) of tear samples was measured at baseline and weeks 8.
Results:
The mean age was 61.27 ± 11.68 years. At baseline NITBUT = 5.89 ± 2.81 s, tear meniscus height = 0.17 ± 0.05 mm, TFLL = 2.74 ± 0.51, CFS = 4.35 ± 0.68, CS = 53.83 ± 9.63 mm, MMP-9 = 49.10 ± 10.42 ng/mL, RS = 1.65 ± 0.44, MGEx = 1.85 ± 0.72, MGQ = 2.65 ± 0.50, CNFD = 20.36 ± 8.20 no./mm2, and SPEED = 12.62 ± 3.91. At week 4, significant improvements were found in all parameters except RS (1.59 ± 0.46, P = 0.172) and CNFD (21.46 ± 8.41, P = 0.163). Finally, at week 8, all parameters had significant improvements.
Conclusion:
Preliminary short-term findings suggest that treatment of DDE patients with DQS was found to be safe and efficacious in improving dry eye parameters. In addition, inflammatory marker and corneal nerve density were significantly improved. This study was registered with ClinicalTrials.gov (NCT05193331).
Introduction
Type 2
Dry eye disease (DED) is characterized by a loss of tear film homeostasis and is accompanied by ocular symptoms, with tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities. 10 The prevalence of DED in people with diabetes is 54%, which is higher than in the average population. 11 The consensus revolves around the damaging role of DM in the microvasculature of the lacrimal gland and corneal nerve sensation that decreases homeostasis of the tear film, resulting in ocular surface insult and, consequently, signs and symptoms of DED.8,12 Furthermore, conjunctival goblet cell loss has been linked to decreased tear quantity and quality in T2DM patients.13,14 In animal models, goblet cell loss disrupts immune tolerance on the ocular surface and increases the production of inflammatory cytokines in the conjunctiva.15,16
Diquafosol Sodium is a potent purinergic P2Y2 receptor agonist and a stable synthetic derivative of the naturally occurring nucleotide uridine 5′-triphopsphate; conjunctival goblet cells and conjunctival epithelial cells are stimulated to secrete mucin and tear fluid.17–20 It stimulates mucin secretion from conjunctival goblet cells and tears secretion from conjunctival epithelial cells.19,21,22 Various studies have concluded that Diquafosol Sodium ophthalmic solution (DQS) is beneficial for the treatment of DED.23–26
In our previous pilot study, 3% DQS treatment improved the tear film and symptoms of DED in diabetic dry eye (DDE) patients. 27 Studies have revealed the number of nerves, the density of nerves, and inflammatory cell density were improved after treatment with 3% DQS in DE patients with Sjögren's syndrome (SS).28–30 Since hyperglycemia leads to a decrease in the density and sensitivity of corneal nerves, which may have hampered the tear secretion reflex and lowered tear production. 31 In addition, DED exacerbates existing diabetic corneal damage due to tear film instability and inflammation. 32 Therefore, this preliminary short-term study aimed to explore the effects of 3% DQS on ocular surface DE parameters, inflammation, and corneal nerve fiber density (CNFD) in DDE patients.
Methods
Study design and participants
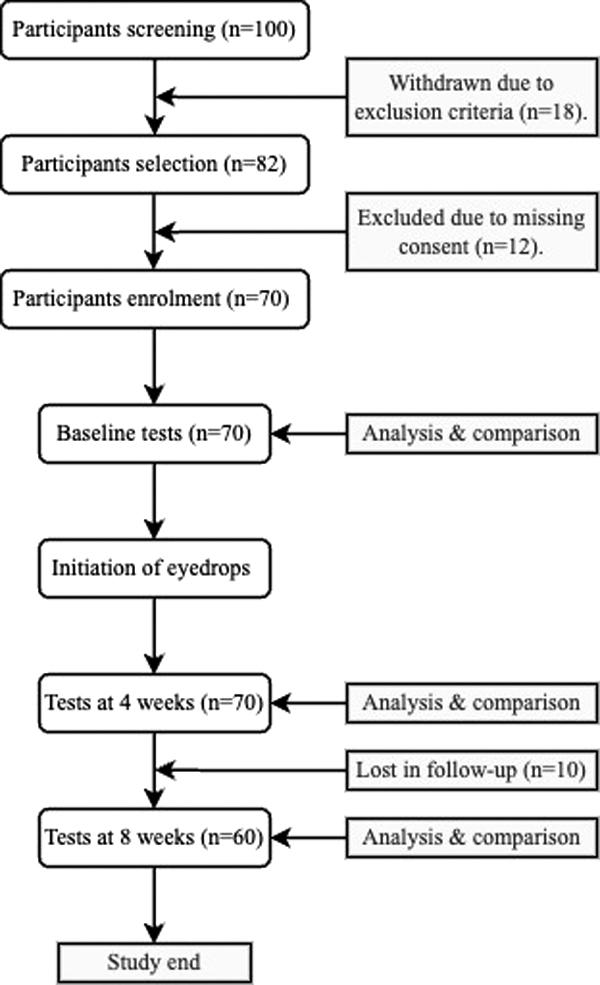
This prospective, single-arm, assessor-blinded, single study initially recruited 140 eyes of 70 diabetic patients diagnosed with DED and consecutively assigned to the study between August 2022 and March 2023 (Fig. 1). The study was conducted at the Department of Ophthalmology, He Eye Specialist Hospital, Shenyang, China, approved by the Ethics Committee of He Eye Specialist Hospital [IRB (2022) K002.01] and adhered to the tenets of the declaration of Helsinki. All subjects signed informed consent forms before they participated in the study. Patients or the public were not involved in our research's design, conduct, reporting, or dissemination plans.
Study design.
The study had an 8-week treatment period in which all participants used 1 drop of 3% Diquafosol Sodium (Diquas; Santen Pharmaceutical Co., Ltd., Osaka, Japan) 6 times daily for 8 weeks. All examinations were conducted at baseline, weeks 4, and up to 8 weeks. MMP-9 of tear samples was collected and measured at baseline and weeks 8. The clinical assessment, data collection, and team were unaware that the participants used 3% Diquafosol Sodium.
Inclusion criteria comprised the following: (1) age ≥18 years, (2) clinically diagnosed and confirmed with T2DM for 1 year or more, (3) able and willing to adhere to the therapy and follow-up plan, (4) participants were diagnosed with DE according to the TFOS DEWS II diagnostic criteria: (1) Standard Patient Evaluation Eye Dryness (SPEED) Questionnaire >6, (2) Noninvasive tear breakup time (NITBUT) <10 s, (3) ocular surface staining >5 corneal spots, >9 conjunctival spots. The presence of 2 or more criteria were used to establish a positive DE diagnosis.
The exclusion criteria were as follows: (1) systemic immune-mediated illnesses, such as secondary SS or graft-versus-host disease; (2) active ocular infection, such as infectious, viral, chlamydial, or immunologic conjunctivitis; (3) intraocular, corneal refractive surgery, keratoplasty, or ocular laser surgery within 6 months; (4) glaucoma, systemic, or ocular disease that might interfere with tear film production or function other than diabetes; (5) long-term contact lens wearers and artificial tears users; (6) any ocular severe systemic disease or uncontrolled medical condition; (7) exposure to any investigational drug within 30 days of study start; (8) pregnant and lactating women or those planning a pregnancy throughout the study.
Data collection
Age (years), sex (male or female), duration of diabetes (years), and fasting blood glucose (FBG, mg/dL) were collected from the participant's medical records.
Clinical evaluations
Noninvasive tear breakup time (NITBUT) and tear meniscus height (TMH) were assessed using the DE diagnostic system (MediWorks, Shanghai, China). Three consecutive measurements were taken, and the median value was entered as the final reading.
Using the DR-1, tear film lipid layer (TFLL score) interferometry was evaluated (Kowa, Nagoya, Japan). According to Hosaka et al. 33 grading method, TFLL quality was categorized, and a lower number indicates higher TFLL quality.
Corneoconjunctival staining (CFS score) measures corneal and conjunctival epithelium damage using the methods proposed by Arita et al. 34 A preservative-free solution containing 1% lissamine green and 1% sodium fluorescein was instilled in the conjunctival sac with 2 mL of a double vital staining approach. The ocular surface was sectionalized into three equal sections (temporal conjunctiva, cornea, and nasal conjunctiva). Each region was given a maximum staining score of 3 points and a minimum staining score of 0. The combined scores from all 3 parts were then recorded on a scale ranging from 0 (normal) to 9 (severe).
Central corneal sensitivity (CS) was measured using a Cochet–Bonnet esthesiometer (Luneau Technology Operations, France), which stimulates the cornea with a nylon monofilament. The stiffness of the filament is adjusted by altering the length (5–60 mm) of the filament with a slider on the side of the pen. 35
MMP-9 was measured using an immunochromatography assay after 1 μL tear samples were collected from the lateral canthus with a capillary tear collector. A commercial reagent card (S05B; Seinda Biomedical Corporation, Guangdong, China) based on colloidal gold and immunochromatographic analysis was used to determine the concentration of MMP-9 in the tear samples. One microliter of tear sample was placed in the sampling hole on the reagent card, followed by 3 drops of diluent in the dilution hole. The reagent card was loaded into the proprietary analyzer (S03A; Seinda Biomedical Corporation), and the MMP-9 concentration was measured 15 min later. 36
Conjunctival hyperemia [redness score (RS) score] was assessed by Keratography 5M (Oculus, Germany), and the score can range from 0.0 (normal) to 4.0 (severe).
Meibomian gland quality (MGQ) and expressibility were assessed under a slit-lamp: (1) MGQ was evaluated by rating each of the 5 meibomian glands in the middle of the eyelids on a scale from 0 to 3 (0 represented clear meibum; 1 represented cloudy meibum; 2 represented cloudy and granular meibum; and 3 represented thick, toothpaste-like consistency meibum). (2) Meibomian gland expressibility (MGEx) was assessed on a scale of 0 to 3 for 8 meibomian glands in the center (0 denoted that all glands were expressible; 1 denoted that 3 to 4 glands were expressible; 2 denoted that 1 to 2 glands were expressible; 3 denoted that no glands were expressible). The mean scores of these 8 glands were used to get the final score.
The in vitro confocal corneal microscopy images were obtained by HRT III RCM (Heidelberg Engineering GmbH, Dossenheim, Germany) and were used to examine corneal nerve change. For each eye, 3 central corneal subbasal nerve plexus images that were nonoverlapping, high-contrast, and high-quality chosen for analysis. The measurement of corneal nerve morphology was carried out using fully automated analysis software (ACCMetrics). 37 The number of main nerve fibers/mm2: CNFD.
Safety evaluation
Best corrected visual acuity (BCVA), intraocular pressure (IOP), endothelial cell count (ECC), and corneal and conjunctival examinations with a slit lamp microscope were performed during all test visits. The ocular surface and periorbital abnormalities were evaluated.
Assessment of symptoms
A validated SPEED Questionnaire provided a quantifiable assessment of DE symptoms. The 8 items of the questionnaire can be tabulated to obtain an individual score ranging from 0 to 28 (no symptoms to severe symptoms) points. Patients answered 2 SPEED questionnaires based on left and right ocular symptoms. 38
Statistical analyses
The data were reported in terms of mean and standard deviation. The statistical analysis was conducted using SPSS version 24 (SPSS, Inc., Chicago, IL, USA). The data were determined to have a nonnormal distribution through the use of the Shapiro–Wilk test (P < 0.05), necessitating nonparametric testing. The study employed a linear mixed model along with Bonferroni posthoc analysis to assess the repeated measurements of continuous variables such as NITBUT, TMH, CS, CNFD, BCVA, ECC, and IOP. The study employed a generalized linear mixed-model analysis to examine repeated measurements of discrete variables such as TFLL score, CS score, RS score, Meibomian gland (MG) assessments, and SPEED score. Additionally, a Bonferroni posthoc analysis was conducted. The statistical significance level was established at a threshold of P < 0.05. At a significance level of a = 0.05, the power of (1 − b) was 0.90, indicating that the sample size of 30 eyes in each group was adequate.
Results
Patient demographics
The final analysis included 60 patients (120 eyes). The mean age of participants was 61.27 ± 11.68 years and comprised 60 participants (38 females, 63.3%, and 22 males, 36.7%). The mean duration of T2DM was found to be 9.03 ± 5.61 years, and the mean FBG was analyzed to be 7.80 ± 2.03 mg/dL. All participants included in this study had signs and symptoms of DED after being diagnosed with T2DM. The demographic characteristics of participants in the study are presented in Table 1.
Participant Demographics
DM, diabetes mellitus.
Efficacy of treatment
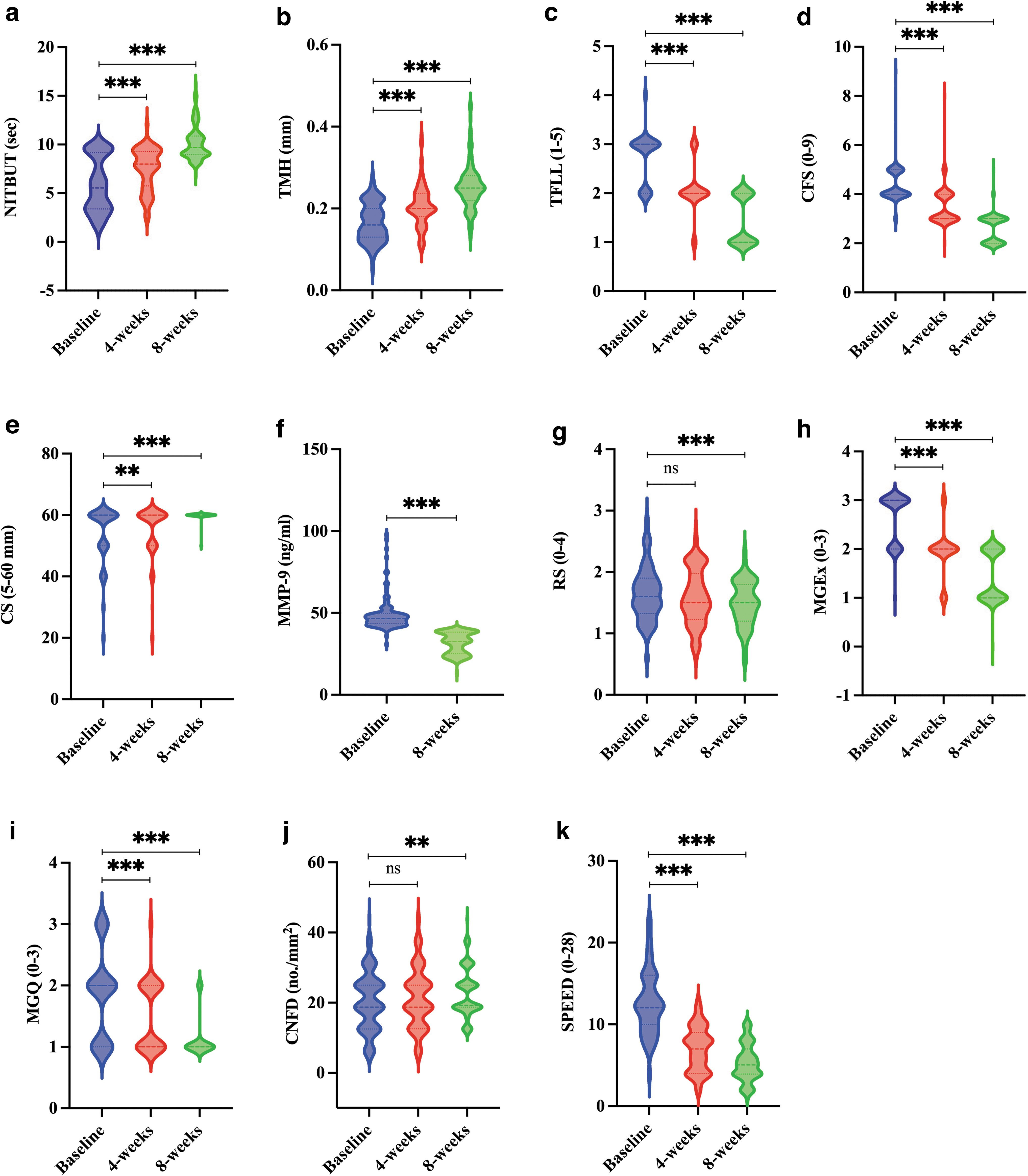
NITBUT (s) was significantly prolonged following the use of DQS (Baseline: 5.89 ± 2.81 s, 4 weeks: 7.49 ± 2.17 s, and 8 weeks: 10.17 ± 1.78 s) at all assessment time points. At 4 weeks, the within-group comparison revealed −1.60 s (Δ1) improvement and at 8 weeks, −4.28 s (Δ2) improvement was found (Table 2 and Fig. 2a).
Ocular Surface Characteristics of Participants Before and After the Treatment of Diquafosol Sodium
P value <0.05; P 1 -value: baseline versus 4 weeks; P2-value: baseline versus 8 weeks.
NITBUT, noninvasive tear breakup time; TMH, tear meniscus height; TFLL, tear film lipid layer; CFS, corneoconjunctival staining; CS, corneal sensitivity; MMP-9, matrix metalloproteinase-9; RS, redness score; MGQ, Meibomian gland quality; MGEx, Meibomian gland quality expressibility; CNFD, corneal nerve fiber density; SPEED, Standard Patient Evaluation Eye Dryness.
TMH (mm) increased significantly following the treatment of DQS (Baseline: 0.17 ± 0.05 mm, 4 weeks: 0.21 ± 0.05 mm, and 8 weeks: 0.25 ± 0.05 mm). Δ1 at 4 weeks and Δ2 at 8 weeks were found to be −0.04 and −0.09 mm, respectively (Table 2 and Fig. 2b).
TFLL (1–5) increased from 2.74 ± 0.51 at baseline to 2.07 ± 0.48 at 4 weeks follow-up (P < 0.001), and at 8 weeks, TFLL further improved to 1.43 ± 0.50 (P < 0.001). The within-group comparison revealed that Δ1 at 4 weeks was 0.68, and Δ2 further improved to 1.32 at 8 weeks (Table 2 and Fig. 2c).
CFS (0–9) at baseline was recorded to be 4.35 ± 0.68, and it significantly improved to 3.50 ± 0.74 (P < 0.001) at 4 weeks and further reduced to 2.61 ± 0.58 at 8 weeks (P < 0.001). Δ1 and Δ2 were found to be 0.85 and 1.74, respectively (Table 2 and Fig. 2d).
CS (0–60 mm) measurement at baseline was 53.83 ± 9.63 mm, and at 4 weeks, it significantly improved to 55.17 ± 8.60 mm (P < 0.01) and was found to further improve to 59.75 ± 1.57 mm (<0.001) at 8 weeks follow-up. Δ1 and Δ2 were found to be −1.33 and −5.92, respectively (Table 2 and Fig. 2e).
MMP-9 (ng/mL) was tested at the beginning (baseline) and end of the study (8 weeks) (49.10 ± 10.42 and 31.61 ± 6.52 ng/mL, respectively) and a significant decrease in tear film MMP-9 levels was recorded (P < 0.001). Δ2 was found to be 17.49 (Table 2, and Fig. 2f).
RS (0–4) at baseline was 1.65 ± 0.44, and at 4 and 8 weeks, RS was recorded to be 1.59 ± 0.46 (P = 0.172) and 1.49 ± 0.37 (P < 0.001), respectively. Δ1 and Δ2 were found to be 0.06 and 0.16, respectively (Table 2 and Fig. 2g).
MGEx (0–3) at baseline was recorded to be 1.85 ± 0.72. At 4 and 8 weeks, MGEx was found to be 1.50 ± 0.57 (P = 0.181) and 1.13 ± 0.33 (P < 0.001), respectively. Δ1 was recorded to be 0.35, and Δ2 improved to 0.73 (Table 2 and Fig. 2h).
MGQ (0–3) at baseline, 4 weeks, and 8 weeks were recorded to be 2.65 ± 0.50, 1.94 ± 0.47, and 1.43 ± 0.51, respectively. Δ1 was recorded as 0.71, and Δ2 improved to 1.23 (Table 2 and Fig. 2i).
CNFD (no./mm2) at baseline was 20.36 ± 8.20 no./mm2, at 4 weeks was 21.46 ± 8.41 (P = 0.163), and at 8 weeks was 22.97 ± 6.98 no./mm2 (P = 0.001). Δ1 was recorded as −1.10, and Δ2 improved to −2.60 (Table 2 and Fig. 2j).
Standardized Patient Evaluation of Eye Dryness Questionnaire score (0–28) at baseline was 12.62 ± 3.91 and significantly improved to 7.03 ± 2.70 (P < 0.001) at 4 weeks. At 8 weeks, further improvement was recorded and was recorded to be 5.30 ± 2.29 (P < 0.001). Δ1 was recorded to be 5.59, and Δ2 improved to 7.33 (Table 2 and Fig. 2k).
Safety data
During the study, no systemic adverse events or adverse clinical signs and symptoms were detected. BCVA remained stable throughout all visits. No significant change was seen in either group at 4 or 8 weeks of follow-up time (Table 3).
Safety Evaluation
BCVA, best corrected visual acuity; ECC, endothelium cell count; IOP, intraocular pressure.
Discussion
This self-control, prospective, single-arm study compared the efficacy and safety of DQS (n = 120 eyes) on the signs and symptoms of DE in patients with T2DM. The findings demonstrated that DQS can improve the inflammatory maker (MMP-9) and increase corneal nerve regeneration (CNFD) in DDE participants. Compared to baseline measurements, all DED-related objective parameters improved significantly at 4 weeks (P < 0.05). However, while comparing baseline and 4-week measurements, RS (1.65 ± 0.44 vs. 1.59 ± 0.46, P = 0.172) and CNFD (20.36 ± 8.20 vs. 21.46 ± 8.41, P = 0.163), were found not to have any significant improvements. Furthermore, subjective DE symptom scores obtained using the SPEED questionnaire at baseline assessment was 12.62 ± 3.91 (DE >6). 38 Significant improvements were observed at 4 weeks (7.03 ± 2.70, P < 0.05) and 8 weeks (5.30 ± 2.29, P < 0.05).
MMP-9 is a translational inflammatory biomarker in tears for inflammation-related ocular surface diseases, which are used as a tear protein biomarker in a diagnostic tool. 39 In contrast to inconvenient mass spectrometry and traditional ELISA test, a rapid MMP-9 detection based on colloidal gold and immunochromatographic analysis was used to determine the improvement of tear inflammatory factors after DQS treatment. Our results provide a reference for the clinical treatment of DED and the application of tear biomarkers in the clinical stage of ophthalmology.
In DE cornea, Diquafosol Sodium has been found to promote cell survival and modulate reactive oxygen species-induced apoptosis and inflammation of epithelial cells. 40 As a potent agonist for purinergic P2Y2 receptors, it stimulates the fluid and mucin secretion from conjunctival epithelial cells and conjunctival goblet cells, respectively.21,41,42 Previous research indicates that Diquafosol Sodium rehydrates the ocular surface independently of aqueous fluid secretion from the lacrimal glands by enhancing tear film stability.43,44 While the action of Diquafosol Sodium, as shown in Fig. 3, for relieving the adverse symptoms of DE has been extensively studied, Katagiri et al.45,46 suggest that Diquafosol Sodium attenuates neuronal hyperactivity due to DED damage. Further studies observed that treating 3% DQS potentially promoted subbasal corneal nerve growth in DE patients after LASIK surgery. 47 Interestingly, in our study, CNFD was found not to have any significant improvement at 4 weeks. Still, at 8 weeks, statistically significant improvements were recorded.
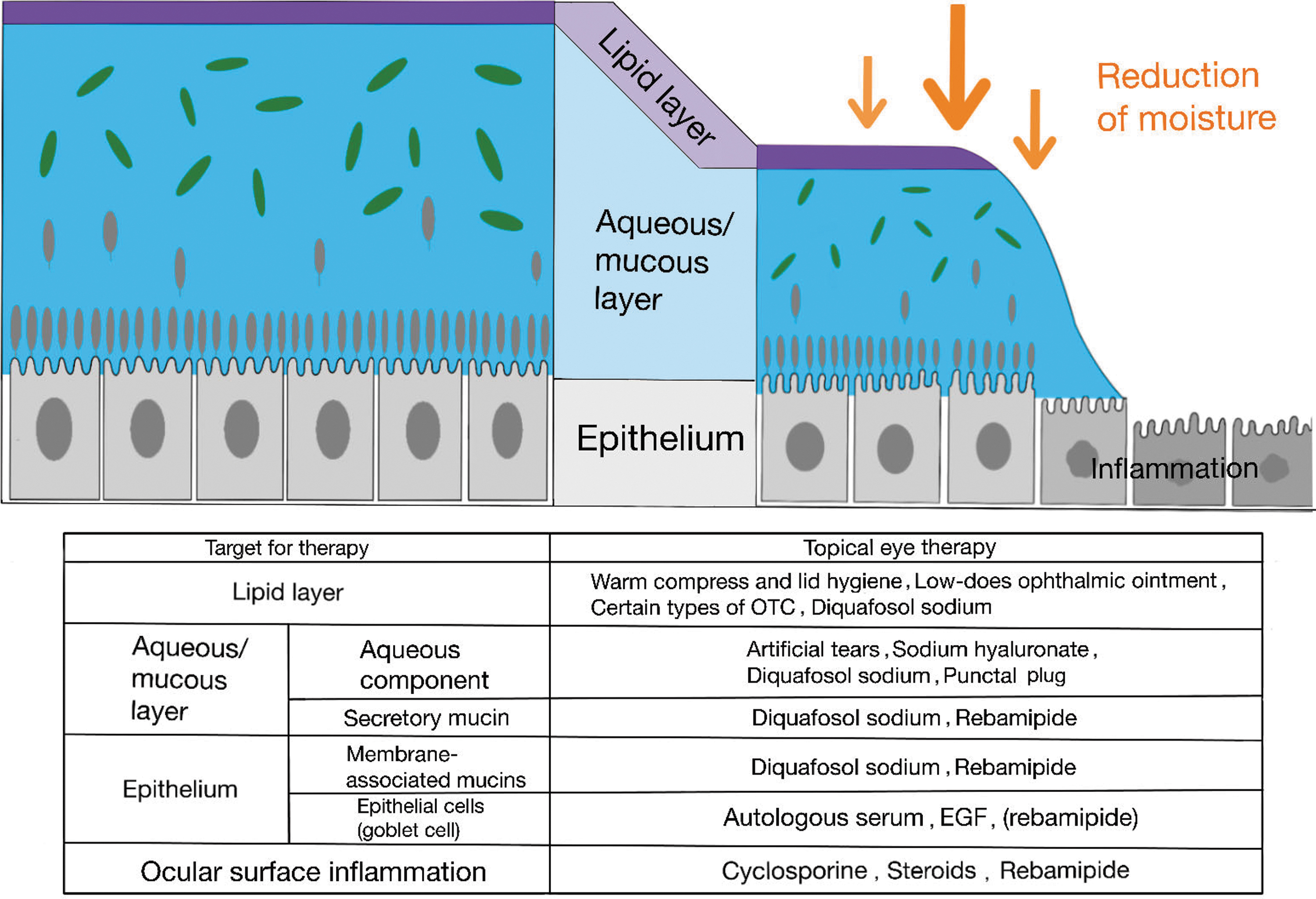
Effect of diquafosol sodium on the ocular surface.
It has been reported that patients with diabetes had decreased CS and reflex-induced tear secretion. 48 Hyperglycemia can result in metabolic injury to the cornea's densely innervated peripheral nerves. 49 Several studies also found that diabetic patients with polyneuropathy have more severe DED than diabetic patients without polyneuropathy.49,50 Several investigations51,52 indicated that pan-retinal photocoagulation may be associated with corneal ciliary nerve injury. Reduced CS also results in a slower blinking rate, which exacerbates tear hyperosmolarity as a consequence of evaporation. 53 Therefore, initial evidence from the past 27 and the current study suggests that Diquafosol Sodium has the ability to improve the DE ocular surface parameters by rejuvenating corneal nerves and reducing inflammation in DDE patients.
The study's main limitation is that it lacks a control group, and the current study is a single-center study. Nevertheless, our previous randomized control study with an active control group demonstrated the safety and efficacy of Diquafosol Sodium on DDE patients. 27 Furthermore, the use of visual terminal devices and electronic display units was not considered in this study, which has been reported to significantly influence DED progression. 54
While prior studies have reported that proteomic changes have also been described in patients with DR,55,56 the scope of the current study was to assess the effects of 3% DQS on ocular surface inflammation and corneal nerve density in DDE patients. Thus, fundus fluorescein angiography and dilated fundus examination were not performed in our current study. Besides, the subjects in this study had relatively good visual acuity and no end-stage DR. It will be important to focus on the association between tear protein and DR in future studies. In addition, we did not assess peripheral CS, which may be superior to central CS. 57 Therefore, further multicenter research is necessary to study the impact and mechanism of DQS on DDE patients.
Conclusion
The topical ophthalmic 3% solution of Diquafosol Sodium was found to be safe and well tolerated, with no adverse effects, in patients with type 2 DDE. Overall, Diquafosol Sodium ophthalmic improved not only improves the signs and symptoms of severe DED in type 2 diabetic patients but also the corneal nerve density and the tear film inflammatory MMP-9 marker level in this preliminary short-term study. Further research is required to elucidate the therapeutic effect of 3% DQS in diabetic patient cohorts with varying degrees of diabetic duration and severity.
Footnotes
Acknowledgments
The authors wish to thank all participants, postgraduate students, and researchers for data collection. We also acknowledge the support from the Dry Eye and Ocular Surface Clinic at HESH, Shenyang.
Authors' Contributions
G.Q.: writing—original draft; J.C., L.L., Y.Q., and Y.C.: formal analysis; Q.Z., N.G., S.M., and S.B.: Methodology; Y.W., Y.Y.. and L.Y.: Software;; J.E.M.: writing—review and editing; L.X., W.H., S.Y., and X.H.: Conceptualization; E.E.P.: writing—original draft and conceptualization.
Informed Consent
Informed consent was obtained from all subjects involved in the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by He Eye Specialist Hospital, Shenyang, China.