
Abstract
Fungal keratitis (FK) is a dangerous corneal infection that is common in tropical and subtropical areas. Its incidence is extremely high, and ocular trauma and contact lenses can lead to FK, but its common treatment such as using topical antifungal eye drop instillation is often less effective because of several drawbacks of the drugs typically used, including limited ocular penetration, high frequency of dosing, poor biocompatibility, and the potential for severe drug reactions. Therefore, the development of novel drug delivery devices for the treatment of FK is urgent. The urgent need for novel drug delivery devices to treat FK has led to the development of several techniques, including nanoparticles (NPs), in situ forming hydrogels, contact lenses, and microneedles (MNs). However, it is important to note that the main mechanisms differ between these techniques. NPs can transport large amounts of drugs and be taken up by cells owing to their large surface area and small size. In situ forming hydrogels can significantly extend the residence time of drugs because of their strong adhesive properties. Contact lenses, with their comfortable shape and drug-carrying capacity, can also act as drug delivery devices. MNs can create channels in the cornea, bypassing its barrier and enhancing drug bioavailability. This article will go over novel medication delivery techniques for treating FK and make a conclusion about their advantages and limitations in anticipation to serve the best option for the individual therapy of FK.
Introduction
Fungal keratitis (FK), commonly known as ocular mycosis, is a serious vision-threatening condition that can result in permanent blindness if the cornea is destroyed by the fungal infection. 1 FK tends to be a poorly treated condition with very high morbidity. 2 It is reported that there are at least 1.4 million instances of FK in the world every year, with the highest incidence in Asia and Europe. 3 FK can be triggered by both ocular and systemic factors, such as trauma, chronic corneal inflammation, contact lenses wear and medications, and diabetes.4,5 Trauma causes ∼55%–65% of all cases of FK, but in recent years, with the increasing use of contact lenses, this has become an important factor in cases of FK, especially in developed countries.6,7 Patients with FK usually present with an insidious onset and gradual progression of symptoms, including pain, tearing, photophobia, foreign body sensation, and loss of vision in severe cases. 8
FK is primarily caused by traumatic implantation of fungal fragments or spores into the surface layer of the cornea. Fungal infections of the cornea can be caused by over 100 different fungi, the majority of which being the filamentous fungi Fusarium and Aspergillus, as well as the yeast Candida. 9 Despite the fact that antifungal medications now used have broad-spectrum antifungal activity, they have limited drug bioavailability because of their low solubility, poor ocular penetration, and short duration of action. 10 In addition, there are barriers such as tight junctional complexes in the corneal epithelium, lacrimal turnover, nasolacrimal drainage, blinking reflexes, efflux transporters, drug metabolism by ocular enzymes, and drug binding to or repulsion from conjunctival mucins, tear proteins, and melanin. 11 To get a greater therapeutic effect, regular medicine must be taken while using eye drops, which causes some discomfort and side effects including redness, foreign body sensation, stinging and burning sensation, and tearing. 12
In addition, intrastromal injection is an alternative treatment option for deep FK where medication is not effective. 13 It ensures adequate drug delivery to the site of active infection. However, at the same time there are some limitations to this therapy including breaching the natural barrier to infection, risk of deeper spread of infection, medical transmission of the fungus at the site of injection, intraocular inflammation, lens damage, glaucoma, anterior chamber hemorrhage, and potential endothelial damage.14,15
As a result, effective drug delivery methods are required to boost the penetration capability and duration of action of antifungal medicines. At the moment, novel drug delivery technologies such as nanoparticles (NPs), in situ forming hydrogels, contact lenses, and microneedles (MNs) have appeared, and antifungal medication efficacy has been greatly enhanced in both in vitro and animal models. As a result, this article discusses innovative medication delivery methods for the treatment of FK and put forward on the problems and future development opportunities encountered by different drug delivery systems, intending to save more people from the terrible consequences of blindness.
Topical Medication Barriers
The use of medication via ocular administration can minimize the side effects arising from systemic absorption. Unfortunately, ocular administration simply is not effective in treating FK. Because of the physiological structures, including nasolacrimal drainage, corneal epithelial barrier, and so on, of the eye causes low drug bioavailability/penetration, it results in low therapeutic impact. Rapid nasolacrimal duct draining and restricted corneal permeability lead to decreased medication absorption and therapeutic effectiveness (Fig. 1).
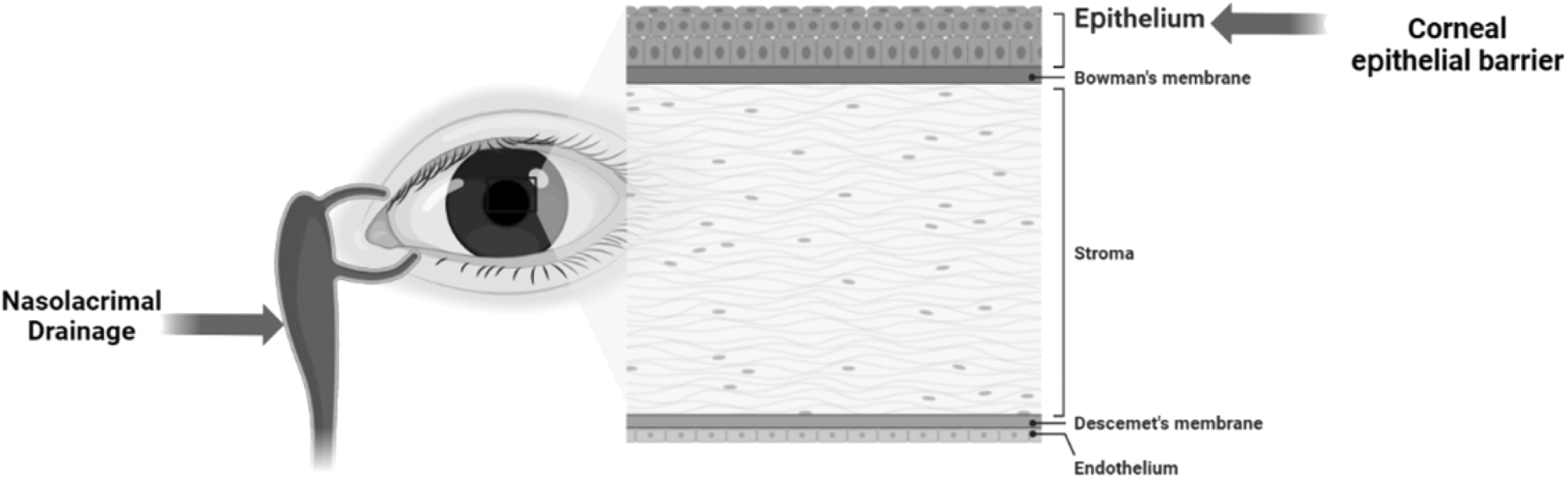
Topical medication barriers such as nasolacrimal ducts and corneal epithelium are the main reasons for the poor results of topical application of antifungal drugs in the treatment of FK. FK, fungal keratitis.
Nasolacrimal drainage
The most common reason for short precorneal residence time and limited ocular bioavailability of medicines supplied as eye drops is nasolacrimal duct drainage. The volume of human tears averages 7 μL and is maintained constant by continual generation and release. Eye drops account for ∼90% of ophthalmic medications for front-of-the-eye diseases, but the volume of an eye drop is ∼30 μL. 16 This volume discrepancy between tear film and an eye drop results in the fact that upon instillation of an eye drop, the tear volume rises and most of the fluid of the drug would burst out of the eye. Then most of the remaining drug would go through nasolacrimal dust. 11
Because of this drainage, the medication has a 2-min residence period on the ocular surface and only ∼5% of the drug may be absorbed by the cornea to exert its effect. 17 The medication enters the nasal cavity via the nasolacrimal duct and may potentially be absorbed into circulation. This absorption not only results in drug waste but can also have systemic consequences. In addition to nasolacrimal duct drainage, the lacrimal turnover, meaning the renewal of tears, results in rapid drug elimination although the lacrimal turnover rate is typically 16%/minute under normal conditions. 18
Corneal epithelial barrier
Corneal epithelial tissue has an essential barrier function that may keep the corneal interior environment stable, and it is also the most effective barrier to medication penetration. Tight junctions, adherent junctions, and desmosomes are three separate cell junction complexes that exist between cells in the epithelial basal layer, with tight junctions being critical for the functioning of the corneal epithelial barrier. 19 Tight junctions are made up of two transmembrane proteins, claudin and occludin, as well as a membrane-associated protein called ZO-1. 20 It significantly impedes drug paracellular penetration, rendering the cornea impenetrable to molecules with a molecular weight larger than 5000 g/mol. 21 But fungal infections disrupt the corneal barrier function, which may facilitate the passage of antifungal drugs through the corneal barrier.
Novel Delivery System for Antifungal Drugs
As nanomaterials have advanced, more and more novel drug delivery methods have been developed for the treatment of FK. These systems including NPs, in situ forming hydrogels, contact lenses, and MNs are primarily used to increase the penetration of poorly soluble medications and to extend the actuation duration of pharmaceuticals in the eye, hence improving the therapeutic efficacy of antifungal agents (Fig. 2).

To address the limitations of topical antifungal drugs in the treatment of FK, a number of drug delivery systems such as NPs including lipid NPs, polymer NPs and inorganic NPs, in situ forming hydrogels, contact lens, and MNs have been experimentally demonstrated to increase the penetration and extend the duration of action of the drugs and have been found to be more therapeutically effective than the topical application of drugs alone. MNs, microneedles; NPs, nanoparticles.
Nanoparticles
Because of their numerous unique qualities and benefits, NPs have moved into a wide spectrum of clinical applications in recent years. It has the potential to increase encapsulated drug stability and solubility, promote membrane transport, and extend circulation time for improved safety and effectiveness. 22 NPs have a significant surface area to mass ratio, allowing them to transport a large number of drug molecules. Because of their tiny size (between 10 and 100 nm), they are readily absorbed by cells and hence efficiently carry medicines. Surface adsorption, chemical binding, entrapment, and other methods can be used to combine drug molecules with NPs.23,24 NPs have shown promising results in vitro and in animal models as a drug delivery mechanism (Table 1). 22 NPs are classified into three categories based on their composition: lipid NPs, polymer NPs, and inorganic NPs.
Some Studies of Nanoparticle-Based Drug Delivery Systems for Fungal Keratitis
DL, drug loading; EE, encapsulation efficiency; FK, fungal keratitis; NPs, nanoparticles; PS, particle size; ZP, zeta potential.
Lipid NPs
Lipid NPs can be made of a variety of lipids, including triglycerides, diglycerides, or monoglycerides, as well as free fatty acids or steroids, and their forms are often microspheres or cubes. 25 It is made up of monolayer or bilayer lipids, the center of which is lipophilic and may encapsulate lipophilic antifungal medications such as voriconazole, natamycin, and others, which can be released slowly over time to extend the release period. 26 The pharmacokinetics of numerous lipid NPs for topical application in FK has been studied. Zhen Liang et al. discovered that lipid NPs made of glycerol and methanol delivered the antifungal medication econazole and that its drug release was substantially slower and more regulated, with drug penetration 2.64 times more than that of standard eye drops. 27 Experiment suggests the lipid NPs were prepared using the microemulsion method. The resulting NPs had an average particle size of 19 nm and a spherical morphology.
The ratio of econazole encapsulated in the lipid particles was 99.35% ± 0.16% and there was a significant slow and controlled release of econazole from the lipid particles, with ∼98% of the drug being released after 96 h. Antifungal tests showed that the lipid NPs that delivered econazole had stronger antifungal activity compared with econazole suspension. 27 Liang Zhen et al. found through in vivo and in vitro experiments that charge modification can affect the penetration of lipid NPs in the cornea, and positive charge can make the penetration of lipid NPs stronger. 28 The findings show that lipid NPs can encapsulate and preserve labile pharmaceuticals from degradation, enhance the bioavailability of weakly water-soluble medications, and modify drug release and drug targeting. 29 They are limited owing to the difficulty of scale-up and problems associated with stability during the manufacturing process.30,31 Further basic research into liposomes for FK therapy are likely to resolve these problems.
Polymer NPs
Polymeric NPs can be prepared as nanospheres or nanocapsules using a variety of techniques including nanoprecipitation, double emulsification, polymer coating, and emulsification diffusion. 32 It can improve drug stability and penetrate deep into cells and tissues, allowing it to be used to deliver drugs. 33 Polymer NPs may be created from both natural and synthetic materials, with poly(lactic-co-glycolic acid) and chitosan being the best options for antimicrobial drug delivery system research. 17 Polylactic acid–glycolic acid copolymer and chitosan, on the contrary, are both hydrophilic polymers, whereas antifungal medicines are typically lipophilic. As a result, polymer NPs are frequently coupled with lecithin or polylactic acid, a very hydrophobic molecule, in a drug delivery system for FK to improve the loading of lipophilic drugs.34,35 The lecithin–chitosan NPs demonstrated evident mucoadhesive characteristics when researchers investigated amphiphilic NPs of chitosan and lecithin for the delivery of amphotericin B.
The lecithin–chitosan NPs were in the size range of 161.9–230.5 nm, entrapment efficiency of amphotericin B was 70%–75%, and the amount of amphotericin-B released at 10 h was 83%. The bioavailability of amphotericin B was enhanced by 2.04 times in a rabbit FK model, the residence duration in front of the cornea was increased by 3.36 times, and the NPs did not produce significant eye irritation, indicating a greater level of safety. 35 Of course, in addition to poly(lactic-co-glycolic acid) and chitosan, additional polymers can be used as antifungal medication carriers. Cell-penetrating peptides are low molecular weight polymers with short amino acid sequences that can penetrate cell membranes. 36 Jain et al. used a cell-penetrating peptide (Tat 2) as a nanocarrier for natamycin in the treatment of FK, demonstrating the conjugated natamycin's strong solubility and superior permeability through the corneal epithelium, as well as the two antifungal activities of clinical isolates of Fusarium spp. 37
Although polymer NPs have led to many promising results and clinical trials and because of the safety and low toxicity of the material, it has been appreciated by many studies. This approach has important limitations owing to the fact that this approach has several problems to solve such as: the phenomenon of burst release 38 ; very low encapsulation of certain active principles that are poorly miscible in the polymer matrix, requiring the use of potentially toxic organic cosolvents 39 ; and very low loading rate of active drugs requiring the administration of a large amount of NPs that can also lead to toxic effects. 40 Overall, polymer NPs can give greater bioavailability and corneal residence duration long enough to successfully treat FK.
Inorganic NPs
Inorganic NPs are mostly made of inorganic materials including gold, silver, and silica. These inorganic NPs are carefully manufactured and may be tailored into a variety of shapes and geometries for drug administration and imaging. 22 Inorganic NPs have received less attention as medication delivery strategies in FK. However, an in vitro investigation conducted in 2013 discovered that silver NPs have a strong antifungal effect against filamentous fungi. They evaluated nanosilver's antifungal activity at concentrations ranging from 0.0156 to 8 g/mL to natamycin's antifungal activity at doses ranging from 0.0313 to 16 g/mL. The activity is 8 times and 32 times that of natamycin, respectively. This might be owing to nano-increased silver's surface area, which allows for greater interaction with microbes and has excellent antibacterial properties. 41 Meanwhile, polypyrrole-coated gold NPs, a type of hybrid metallic-polymeric nanostructures, can also load with Rose Bengal (a photosensitizer was found to be effective in FK management).42,43 Dina Fouad et al. found that the combined photodynamic/photothermal effect of Rose Bengal—polypyrrole-coated gold NPs can function as a novel protocol for treating FK in albino Wistar rats successfully. 44
Although metals have favorable magnetic properties that can offer several advantages for delivering chemotherapeutic drugs over traditional targeted delivery methods, including easier accumulation in tumor tissue, easier penetration of cell membranes into the intracellular environment, and a high specific surface area for more efficient drug loading, 45 their high toxicity profile makes them unsuitable for biomedical use without proper and stable surface treatment. 46 As a result, inorganic NPs might function as transporters of antifungal medicines, increasing broad-spectrum antifungal action. They can be served as a better option if the prospective technologies could solve the problem of metal toxicity.
In situ forming hydrogels
Hydrogels are water-soluble networks made up of strongly cross-linked hydrophilic polymers that have good biocompatibility and resemble natural extracellular matrix components. As a result, they can be widely exploited for medication delivery and tissue regeneration. 50 When used as a carrier for ocular antifungal medications, the hydrogel's strong adherence can prevent it from being washed away by tears or other liquids, extending the residence time in the eye and allowing for the drug's delayed release to achieve an optimal antifungal effect. 51 Hydrogels may be made from several natural and synthetic components, including gelatin, starch, hyaluronic acid, and polylysine.52,53
In situ forming hydrogel creation is achieved by prefabricating hydrogels to create a sol-gel transition under physiological circumstances such as specified pH or temperature. The antifungal properties of several in situ–formed hydrogels as drug carriers have been studied in vitro and in animal models of FK. The findings suggest that, when compared with free medicines, drug-carrying in situ forming hydrogels can improve drug retention and penetration into the corneal tissue.52,54–56 The key distinction between the numerous in situ forming hydrogels used for FK is the composition of the gel and the antifungal medicines contained. The delayed release of the medicine extends the length of the drug's activity in the eye. To induce this transition, the most often utilized method in pharmaceutical formulations is the insertion of heat-sensitive materials pluronics.
Pluronics are amphiphilic synthetic copolymers, with the hydrophobic portion made up of polypropylene oxide blocks and the hydrophilic portion made up of polyethylene oxide blocks. 57 Pluronics, owing to its amphiphilic qualities, can rapidly self-assemble to create tiny micelles at low temperatures and then construct massive micellar cross-linked networks known as gels at higher temperatures. 58 Furthermore, when compared with other heat-sensitive polymers, such as polyester-based polymers, pluronics are more stable when degraded in vivo without having substantial negative effects. 59 However, because the temperature at which it is turned into a gel is significantly different from body temperature, the present gel must be adjusted before it can be utilized more effectively in clinical settings. At the moment, hydroxypropyl methylcellulose is primarily used in pluronics because it can absorb a large number of water molecules, resulting in desolvation of the pluronic molecules and subsequent conversion to more micelles at lower temperatures. 60
Munmun et al. used an optimized in situ–formed hydrogel made by pluronics and hydroxypropyl methylcellulose to deliver itraconazole and discovered that it could extend the drug action period to 8 h while also considerably increasing permeability. 61 However, it is worth noting that some materials used to make the in situ forming hydrogels may be toxic and cause hypersensitivity reactions, so the choice of materials needs to be careful and requires further study. 62 It may be inferred that in situ forming hydrogels comprising mostly of pluronics can be used as an efficient carrier for hydrophobic medicines in the treatment of FK.
Contact lenses
Contact lenses are most commonly used to treat refractive problems, although there is rising interest in their possible medicinal use. In terms of therapy, contact lenses have been shown to preserve corneal epithelial hydration, alleviate eye discomfort, and promote corneal healing.63,64 Furthermore, because of their pleasant form and drug-carrying capacity, contact lenses can be used to manage the release of medications to treat ocular diseases. 65 The primary drug delivery studies in FK include drug soaking, vitamin E coating, and contact lenses based on hydrogel hybrid treatment (Table 2).
Some Studies of Contact Lens–Based Drug Delivery Systems for Fungal Keratitis
3D, three dimensional.
Immersion
The most convenient technique to transport the antifungal medicine is to immerse contact lenses directly in it. Experiments have demonstrated that, although this approach can attach the drug to the contact lenses, it is simply dispersed when the drug is released, resulting in a faster release rate and a shorter residence period in the eye. 66 Cheng-Chun Peng et al. immersed three different contact lenses in the antifungal medication fluconazole and discovered that the three contact lenses released fluconazole for 1–10 h, with the release duration varying greatly. The length of release time is only a function of the material from which the contact lenses is made. 67 None of the contact lenses are suitable for long-term drug release, probably owing to a lack of precise drug–polymer interactions. Antifungal medicines with higher water solubility dissolve fast in the aqueous medium of the eye, making it impossible to properly regulate drug release. 68 As a result, the method of immersion for drug transport has limits and cannot be used directly in clinical applications.
Vitamin E nanobarriers into contact lenses
Although contact lenses cannot be used directly to administer antifungal drugs, they can be optimized as a suitable drug delivery technology. If a barrier can be formed inside of the contact lenses, then the drug release can be prolonged. 69 At present, contact lenses are soaked in solutions of vitamin E dissolved in ethanol–water mixtures and nanobarriers are formed at the surface of the contact lenses that can increase the duration of drug delivery for both hydrophilic and hydrophobic drugs. This method not only achieves comparable vitamin E loading but also reduces the possibility of lens damage.70,71 Cesar Torres-Luna et al. used vitamin E nanobarriers into contact lenses to administer flurbiprofen (a nonsteroidal anti-inflammatory medication). Vitamin E nanobarriers of merely 11% enhanced drug release time by 20 times, whereas the vitamin E nanobarriers of 21% raised it by 45 times. 72
In another study, the release period of fluconazole from contact lenses without vitamin E nanobarriers was shown to be between 1 and 10 h, but adding vitamin E nanobarriers prolonged the duration to 1 week. 67 Vitamin E nanobarriers into contact lenses can extend drug-release time through different mechanisms. Hydrophilic drug molecules like fluconazole can be forced to diffuse out of the lens through tortuous pathways, whereas hydrophobic drug molecules like amphotericin B, natamycin, and dexamethasone can be dissolved at high concentrations.73,74 Oxygen permeability must be high enough for long-term contact lenses wear to avoid corneal hypoxia, which can lead to adverse reactions. 75 Although the oxygen permeability of contact lenses decreases with the application of vitamin E nanobarriers, the decrease is within acceptable ranges and does not affect the cornea in any way.67,70,76 As a result, the practicality of using vitamin E nanobarriers into contact lenses containing antifungal medications to treat FK is still rather high.
Hydrogel-based hybrid therapeutic contact lenses
A polymer hydrogel-based contact lenses for transporting and releasing medications has evolved as a result of breakthroughs in hydrogel research and nanotechnology. Huang Jianfei et al. created a hybrid therapy contact lenses based on the hydrogel. Quaternized chitosan, graphene, silver NPs, and voriconazole make up this hydrogel. The cationic groups of quaternized chitosan and the anionic groups of graphene are electrostatically cross-linked to create a network; voriconazole is loaded in graphene, and both positively charged quaternized chitosan and silver NPs show antifungal action. In both in vitro and in vivo tests, this hybrid treatment hydrogel demonstrated significant antifungal efficacy. 77
In addition to these three types of contact lenses, molecular imprinting technology is one of the most recent technologies for achieving continuous drug release from contact lenses. This approach generates molecular templates, that is, cavities with extremely high affinity for the loaded drug. 78 This can considerably extend the medication's release duration, but because this template can only be compatible with the target drug, it has severe limits in a wide range of therapeutic applications. 68 Overall, contact lenses can be regarded as an appropriate drug delivery technology for antifungal medicines, although several concerns require more investigation and modification.
Microneedles
MNs are micron-scale (60–1000 m in height) technology that has gained popularity in the last 15 years owing to its minimally invasive tissue, effective treatment, ease of administration, controlled drug release, and low manufacturing cost. Transdermal drug delivery has been extensively researched for a variety of therapeutic approaches (eg, antidiabetic and antiobesity drugs, vaccines). 81
The mechanism of MNs on ocular application is the creation of aqueous conduits on the cornea, bypassing the corneal barrier, and improving the bioavailability of ophthalmic drugs. 82 To date, numerous types of MNs have been developed and tested, ranging from solid, hollow, to dissolving MNs. 83 Although these solid and hollow MN types effectively improve ocular drug delivery, some drawbacks, such as brittleness and fabrication difficulty, may limit their applicability and efficacy in the long run. 84 Dissolving MNs can discover these shortcomings and they are always made of biocompatible or biodegradable polymers that cause little damage to ocular tissue, allowing it to heal in 24 h and producing nonmedical waste after complete dissolution. So dissolving MNs can minimize the potential accidental corneal damage and irritation. 85
The microneedle patch (MOP) can be made of biodegradable materials such as hyaluronic acid, polylactic acid, and others, and studies have shown that it can deliver antifungal drugs such as amphotericin B, fluconazole, and others in the eye.82,86 It reversibly penetrates the corneal epidermis without causing significant eye irritation and can control drug release, extending drug action time on the cornea. Furthermore, to be more clinically applicable, the MOP can mimic the curvature of the contact lenses, allowing it to better adapt to the cornea during ocular drug delivery. 87 GirdhariRoy et al. 88 used polyvinyl alcohol and polyvinylpyrrolidone as materials to mimic an MN eye patch made of contact lenses and loaded with amphotericin B to treat Candida albicans–induced FK in 5 min.
When amphotericin B is dissolved, it diffuses into the cornea via the dissolved polymer matrix, resulting in a good therapeutic effect. Eventually, the dissolving MOP is easy to apply in the eye and has the potential to be developed for the efficient delivery of ophthalmic drugs.
MNs, as promising drug delivery devices, have been fabricated using a variety of materials and methods. Metals such as titanium, 89 silicon, and ceramics90,91; biodegradable polymers such as poly(lactic-co-glycolic acid) and polyglycolic acid92,93; and nonbiodegradable polymers such as photolithographic epoxy resins 94 have all been used to fabricate MNs. Similarly, many current methods such as micromolding, droplet air-blowing, and three dimensional (3D) printing have been applied to the fabrication of MNs. First and foremost, most MNs are produced by micromolding, where a solution, slurry, or suspension of material is filled (usually by centrifugation or vacuum) into an MN mold, allowed to dry and cure, and then removed from the mold.95,96 The polydimethylsiloxane mold (5 × 5 arrays, tip parameters H500 B250 P500) is the most common mold used to produce MNs.
In addition to micromolding, other MN fabrication techniques have been investigated for the delivery of a variety of drugs. Kim et al. fabricated insulin-loaded MN arrays by blow-molding polymer droplets, which produced in vivo therapeutic effects similar to subcutaneous injection controls. 97 In addition, with the rapid development of 3D printing technology, it has shown great potential in MN fabrication. 3D printing techniques, including fused deposition modeling, stereolithography, and two-photon polymerization, have been widely used to fabricate MNs.98–100 3D printing can produce MNs in a reproducible manner with high resolution and quality. It can also rapidly change key characteristics such as needle height, tip radius, base diameter, thickness, and density, which play an important role in the performance of MNs. 101
Corneal collagen cross-linking and novel drug delivery system combination therapy
Photoactivated chromophore for collagen cross-linking (PACK-CXL) of the cornea is a therapy that has been successfully used to treat eye conditions such as keratoconus and corneal ectasia.102,103 Recently, PACK-CXL has been investigated as a potential adjuvant treatment option for FK. This technique uses the photosensitizers riboflavin and ultraviolet A to induce photochemical cross-linking in the anterior stromal collagen fibers, thereby increasing the biochemical and mechanical strength of the cornea. 104 Thus, corneal stiffening resulting from this treatment could reduce melting and reduce or prevent corneal perforation caused by FK.
In an experiment using an isolated human corneal infection model, PACK-CXL was found to be a valuable method of inhibiting fusarium growth and spore formation and inhibiting the progression of FK. 105 In addition, the combination of PACK-CXL and voriconazole was found to be effective in reducing fungi and complications of FK compared with voriconazole alone for FK. 106 The combination of PACK-CXL and novel drug delivery systems has been less studied in the treatment of FK. However, there is a study showing that PACK-CXL combined with liposomal amphotericin B can significantly reduce corneal inflammation, accelerate corneal repair, and shorten the course of the disease in the treatment of FK. 107 Therefore, it can be assumed that PACK-CXL has great potential in the treatment of FK, and the combination with new drug delivery systems such as NPs, in situ forming hydrogels, and MNs will be more conducive to the treatment of FK as well as the reduction of its complications.
Summary and Prognosis
FK is a common condition, but because of the insoluble nature of most antifungal medicines and the defensive mechanism of the eye itself, it seldom has a good therapeutic impact when applied locally. In recent years, researchers have discovered that innovative drug delivery technologies such as NPs, in situ forming hydrogels, contact lenses, MNs can dramatically boost drug penetration and lengthen drug action time when administering antifungal medications. NPs are considered the most promising ocular drug delivery system for the treatment of FK. They protect encapsulated drugs from degradation and metabolism, increase residence time in front of the cornea, and enhance corneal permeability. However, their production cost is high. Although the materials used for NPs preparation are safe and nontoxic, there are still problems such as toxic reactions caused by material degradation. 118
Although NPs have the potential to improve bioavailability and patient compliance in preclinical studies, few have received market approval for clinical use. In situ forming hydrogels have been shown to prolong the duration of drug action in several in vivo and in vitro experiments and can be used for the simultaneous delivery of multiple drugs. 119 However, most studies have focused on locally delivering small molecules. 120 In situ forming hydrogels are disadvantageous owing to their poor stability and susceptibility to degradation. 121 Contact lenses can serve as drug reservoirs to continuously release drugs and reduce systemic losses. However, contact lenses currently available on the market are mostly stored in care solutions, which may lead to premature elution of drug-carrying contact lenses for long-term use, rendering the drug delivery system ineffective. In contrast, MNs deliver drugs in a minimally invasive manner by bypassing the body's physical barriers. 122
However, they may cause adverse effects such as pain and irritation. 123 For intractable FK, CXL in combination with novel drug delivery systems may yield better therapeutic results. To conclude, drug delivery systems for FK have both advantages and disadvantages depending on the mechanism (Table 3). To select the most appropriate drug delivery system and treatment method, it is important to evaluate the size and nature of the drug to be delivered, the severity of the patient's disease, and the sensitivity to polymers and other materials used. Simultaneously, many issues, such as finding more biocompatible delivery device materials and controlling the stable release of drugs, still necessitate more in vitro and in vivo research experiments to investigate, evaluate, and provide a theory for the early application of drug delivery devices in later clinical treatment to improve the therapeutic effect.
Comparisons Among the Techniques Mentioned PReviously
MNs, microneedles.
Footnotes
Authors' Contributions
M.R. drafted the work or substantively revised it; R.W. provided valuable guidance in every stage of the writing of this article. Y.H. made the design of the work, and gave enlightening instruction, impressive encouragement, and support.
Consent to Publish
All authors have given approval for the final revision of the article.
Author Disclosure Statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this article.
Funding Information
The authors would like to thank the funding support from Health Commission of Jilin Province, China (Grant No. 2021JC015); Interdisciplinary Training Program for Young Teachers and Students of Jilin University, China (Grant No. 2020-JCXK-26), Natural Science Foundation of Jilin Province (YDZJ202301zyTS067). The funding are of great importance when writing the article.