
Abstract

We published our first work in the field of Ocular Drug Delivery Systems simultaneously with two important milestones related to intravitreal drug delivery (Fig. 1).1,2 First, Macugen® (pegaptanib sodium) was approved by the United States Food and Drug Administration (FDA) in 2004 for treating the wet form of age-related macular degeneration, marking the introduction of the first anti-VEGF drug.3,4 Then, Avastin® (bevacizumab), another anti-VEGF drug approved for treating colorectal cancer in 2004, began to emerge in 2005 as one of the most commonly used off-label treatments in ophthalmology.5–10 However, our research began somewhat earlier, inspired by numerous articles published on the intravitreal administration of triamcinolone acetonide for the treatment of different diseases of the posterior segment of the eye11–13 and by the importance of a ganciclovir implant in the treatment of cytomegalovirus retinitis in patients suffering from the acquired immunodeficiency syndrome.14,15 This implant (Vitrasert®) is a nonbiodegradable device designed for sustained ganciclovir release to avoid its frequent intravitreal dosing. Vitrasert® received FDA approval in 1996 and became the standard of care. This implant is no longer marketed, but its place in history remains important.
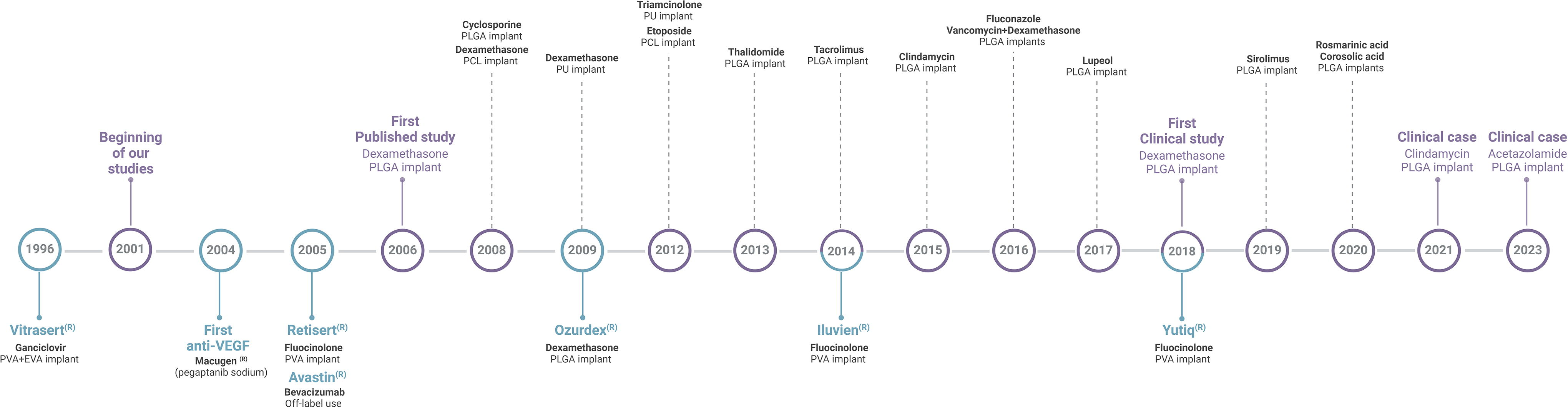
Timeline of preclinical/clinical implant development and commercial milestones. The upper section highlights milestones from our research group in purple. Dashed lines indicate the first publication for each implant developed, including their respective drugs and polymers used. The lower section shows commercial milestones, in blue, along with their corresponding drugs and polymers. PVA, polyvinyl alcohol; EVA, ethylene vinyl acetate; PLGA, poly(lactide-co-glycolide); PCL, polycaprolactone; PU, polyurethane.
The idea of bypassing the blood–ocular barriers with intravitreal dosing to treat chronic posterior segment diseases has proven effective. However, due to the need for repeated intravitreal dosing to maintain pharmacological activity in the posterior segment, intravitreal injections placed a substantial burden on the patients.16,17 Thus, over the past 25 years, an enormous effort to develop effective intravitreal therapies with reduced treatment burden and frequency of administration has been ongoing. Intravitreal delivery systems are great choices for prolonged release of therapeutic levels of drugs in the vitreous, retina, and choroid, increased bioavailability, and reduced systemic adverse effects. In this context, some of our ocular drug delivery studies were focused on developing slow-release implants based on biodegradable materials for intravitreal dosing. Our first drug of choice was dexamethasone, a corticosteroid with a relative anti-inflammatory potency six times greater than triamcinolone and our poly(lactide-co-glycolide) (PLGA) implant was developed as a minimally invasive administration device, called DDS-25G (drug delivery system dosed with a 25G needle). Patented by the Brazilian National Institute for Intellectual Property, this device was evaluated in a Phase I clinical trial (Clinical Trial registry: NCT01662518). It was the first clinical study of an intravitreal implant fully developed in Brazil.2,18–21 In this Phase I study, we demonstrated the feasibility of intravitreal DDS-25G insertion for the treatment of decreased vision due to macular edema associated with retinal vein occlusion, and no safety concerns were evident. 21
The promising results obtained with the DDS-25G paved the way for the development of implants containing other drugs. Thus, various implant delivery systems containing immunosuppressants such as cyclosporine, mycophenolic acid, tacrolimus, and sirolimus were developed and evaluated in preclinical studies intended for the treatment of uveitis,22–30 etoposide for the treatment of intraocular tumors,31–33 and natural products for their antiangiogenic activity.34–37 More recently, we developed a DDS-25G containing rosmarinic acid and published this work in “Planta Medica journal,” for which we received the “Most Innovative Paper Award for 2020”. 36
Of special note is a DDS-25G containing clindamycin, developed to treat recurring cases of ocular toxoplasmosis or for those patients allergic to medications normally used in treatment protocols, which is a combination of pyrimethamine, sulfadiazine, and corticosteroids, also known as the “conventional triple therapy.”38,39 Posterior uveitis caused by toxoplasmosis is prevalent in Brazil. A retrospective study reported 40% incidence of adverse effects related to the medications commonly used (sulfadiazine, pyrimethamine, sulfamethoxazole–trimethoprim, clindamycin, and atovaquone) for the treatment of posterior uveitis caused by toxoplasmosis. Therefore, in a special case study, we opted for the compassionate use of a slow-release clindamycin intravitreal implant (DDS-25G) to protect the retina of a patient for a much longer time than a simple intravitreal injection of the drug. According to studies conducted in rabbits, this implant released doses of clindamycin four times higher than a simple intravitreal injection and achieved concentrations above the 50% inhibitory concentration for Toxoplasma gondii for at least 6 weeks. The clinical improvement observed in this patient, with gradual resolution of intraocular inflammation and healing of the retinochoroidal lesion with cicatricial changes, suggests that the implant may have contributed to the control of the parasite. To our knowledge, this is the first report of the use of an intravitreal slow-release clindamycin implant for the treatment of ocular toxoplasmosis in humans.40–43
We have also developed DDS-25G containing other drugs, such as thalidomide (antiangiogenic effect), 44 fluconazole (antifungal activity), 45 vancomycin (used in the treatment of serious Gram-positive bacterial infections), 46 acetazolamide (carbonic anhydrase inhibitor), and promising results have been obtained. Among these, it is worth highlighting the case study with the DDS-25G containing acetazolamide. In this case study, we opted for the compassionate use of the implant to treat a case of cystoid macular edema. After implant insertion, examinations were performed during 4 months, and we observed that the implant progressively decreased in size with the macular morphology at the final follow-up showing no edema. To our knowledge, this is the first report of intravitreal injection of an acetazolamide implant in a human, and this case provides evidence that it might be a treatment option based on further evidence in studies to treat macular edema. 47
During the progress of our research, the need to find new options to prepare slow-release delivery systems for peptides and proteins became evident since these drugs are labile and cannot be formulated in our system due to their sensitivity to the manufacturing processes. Therefore, other biodegradable polymeric materials including polycaprolactone (PCL) and polyurethane have been considered to prepare the implants.48,49 PCL is a biodegradable and biocompatible polymer suitable for controlled drug delivery due to its ability to be fully excreted from the body and the possibility of prolonged drug release.50,51 Biodegradable polyurethanes can be an interesting alternative for manufacturing implants for soft tissue applications. Polyurethanes can be tailored to display high elasticity and softness, and they can also be easily chemically modified to exhibit chemical functionalities that can interact with small and large molecule drugs. In this context, the studies using polyurethanes synthesized by our team have shown promising results for intravitreal drug delivery.52–58
Polymeric nanofibers prepared using electrospinning technology have been the best alternative developed by our group for the preparation of drug delivery systems containing thermo-labile substances.59–62 This approach does not require the use of organic solvents during preparation, allowing the incorporation of bioactive and hydrophilic drugs efficiently, without the risk of losing structural conformation and activity. Biodegradable polymeric nanofibers allow the modulation of drug release due to the flexibility of their composition. Based on these principles, we developed an implant coated with polymeric nanofibers. Specifically, we developed an innovative device composed of a PLGA implant coated with polymeric polyvinyl alcohol and PCL nanofibers, aiming for the delivery of dexamethasone from the core and bevacizumab from the coat for treating age-related macular degeneration (AMD). This new implant resulted in the reduction of vessels and was safe for intravitreal use as demonstrated by the clinical and histological analysis as well as by electroretinography and optical coherence tomography. 62 Considering that the nanofiber-coated implants allow the sustained delivery of two drugs at the same time, they may be able to reduce the side effects associated with frequent intravitreal administrations, thereby increasing patient compliance. By targeting VEGF as well as inflammatory events, the delivery system developed in this work may offer a new and effective treatment for AMD. Furthermore, the concept of implants coated with nanofibers to deliver two or more drugs can be applied to other diseases of the eye. Thus, a new and promising drug delivery system has been developed by our group, and studies are underway to improve this system.
The first biodegradable implant for intravitreal therapy (Ozurdex®-dexamethasone intravitreal implant) gained FDA approval in 2009 for the treatment of macular edema after retinal vein occlusion or central vein occlusion. This implant offers sustained release of dexamethasone in the vitreous cavity, and this novel drug delivery system has proven useful both in improving clinical outcomes and in reducing injection burden, and its utilization continues to expand for the treatment of other vitreoretinal disorders.63,64 However, several challenges remain to be addressed, such as expanding the drug-carrying capacity and ensuring the possibility of sustained peptide and protein delivery. The development of implants for intravitreal delivery of protein drugs is crucial to broaden the antiangiogenic therapy options for retinal and choroidal neovascularization. Moreover, the possibility of combination therapies, such as anti-inflammatory drugs together with anti-VEGF or other biomolecules, for more personalized medicine seems to be an interesting option.
The development of drug delivery systems for the treatment of diseases that affect the anterior segment of the eye and the discovery of new drugs for the treatment of ocular disorders is also an objective of study of our research group. In total, our group co-authored 129 scientific papers on ocular drug delivery systems and 4 patents that have been licensed, in addition to several conference proceedings. The development of drug delivery systems for the treatment of diseases of the posterior segment of the eye has been our most important contribution to the ocular pharmacology and therapeutics field.
This editorial highlighted the articles published by Fialho SL and Silva-Cunha, a team from 2002 until date, with an emphasis on drug delivery systems for the treatment of diseases of the posterior segment of the eye. Obviously, many other research groups work in this area, and the number of articles published on this topic in recent years is remarkably high. To add to the understanding of the state of the art in this field, we refer the readers to some reviews published in the last 10 years that describe implant drug delivery systems, developed with nonbiodegradable or biodegradable materials, intended for intravitreal administration.65–70