
Abstract
Dry eye disease (DED) is a rapidly growing ocular surface disease with a significant socioeconomic impact that affects the patients’ visual function and, thus, their quality of life. It is distinguished by a loss of tear film homeostasis, leading to tear film instability, hyperosmolarity, ocular surface inflammation, and neurosensory abnormalities, with all of these playing etiological roles in the propagation of the vicious DED circle. While current treatments primarily focus on reducing tear film instability and hyperosmolarity, increasingly more attention is being placed on tackling the underlying inflammation that propagates and potentiates these factors. As such, preclinical models are crucial to further elucidate the DED pathophysiology and develop novel therapeutic strategies. This review outlines the role of inflammation in DED, highlighting related signs and diagnostic tools before focusing on relevant preclinical animal models and potential therapeutic strategies to tackle DED-associated inflammation.
Introduction
Over the past two decades, significant research has been performed in the area of dry eye disease (DED), with several preclinical and clinical studies highlighting the role of ocular surface inflammation in DED.1–4 As a result, the Tear Film & Ocular Surface Society revised the definition of DED in the 2007 TFOS DEWS (Tear Film and Ocular Surface Dry Eye Workshop) I report acknowledging that “…[DED] is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface.” With further research highlighting the significant pathological role of inflammation within the disease pathway, the TFOS DEWS II definition and classification subcommittees of 2017 further acknowledged that ocular surface inflammation is a causal rather than a casual marker of the disease and updated the definition of DED to “a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.” 5 It is now understood that DED is a chronic ocular surface disorder in which tear film instability, tear hyperosmolarity, and inflammation of the ocular surface and lacrimal glands play cyclic etiological roles, forming the vicious circle of DED pathogenesis and propagation.6,7 This multifactorial and chronic nature of DED renders the development of effective therapeutic interventions rather challenging.
Preclinical models provide a useful tool for elucidating the disease pathogenesis and evaluating novel therapeutics. However, preclinical models of DED are often difficult to establish reliably due to the innate tendency of the eye to restore tear fluid quality and quantity in order to achieve homeostasis. Moreover, the cyclic nature of the disease often makes it difficult to establish a direct causal relationship between the triggers and symptoms of DED and replicate clinically relevant DED signs rendering it difficult to understand the clinical relevance of novel therapeutic interventions using preclinical models.
Several therapeutic strategies have been employed for the effective management of DED with tear replenishment traditionally being the first line of treatment, although significant improvement is typically only evident once ocular surface inflammation has also been addressed, especially in moderate-to-severe cases.8,9 Therefore, novel therapeutic strategies aimed at tackling the underlying inflammation have recently been investigated for more efficient management of DED. Most currently available anti-inflammatory agents used for DED management, such as corticosteroids and cyclosporine A (CsA), are broad spectrum immunosuppressants that can have significant adverse effects.10,11 Moreover, achieving therapeutically relevant drug concentrations in the eye while ensuring ocular safety remains an ongoing challenge. 12 In recent years, significant ocular surface toxicity has been reported due to eyedrop excipients, such as preservatives, surfactants, and stabilizers, which can exacerbate ocular surface inflammation resulting in iatrogenic DED, 13 thus necessitating thorough preclinical evaluation of new therapeutics.
This review provides an overview of the classification, pathophysiology, and diagnostic tools typically employed in DED with a specific focus on ocular surface inflammation. Preclinical animal models currently available to understand disease progression and management are detailed, and the role of primary and secondary mediators of inflammation in these models is discussed. Finally, an overview of current and emerging strategies for the management of the inflammatory component in the vicious DED circle is provided.
Classification and Pathophysiology of DED
DED may be triggered by multiple factors that interrupt the healthy tear film. While a considerable overlap between the DED subtypes is typically observed in practice, for this article, DED has been classified into two main etiopathogenic subtypes (Fig. 1), aqueous-deficient dry eye (ADDE) and evaporative dry eye (EDE). 14
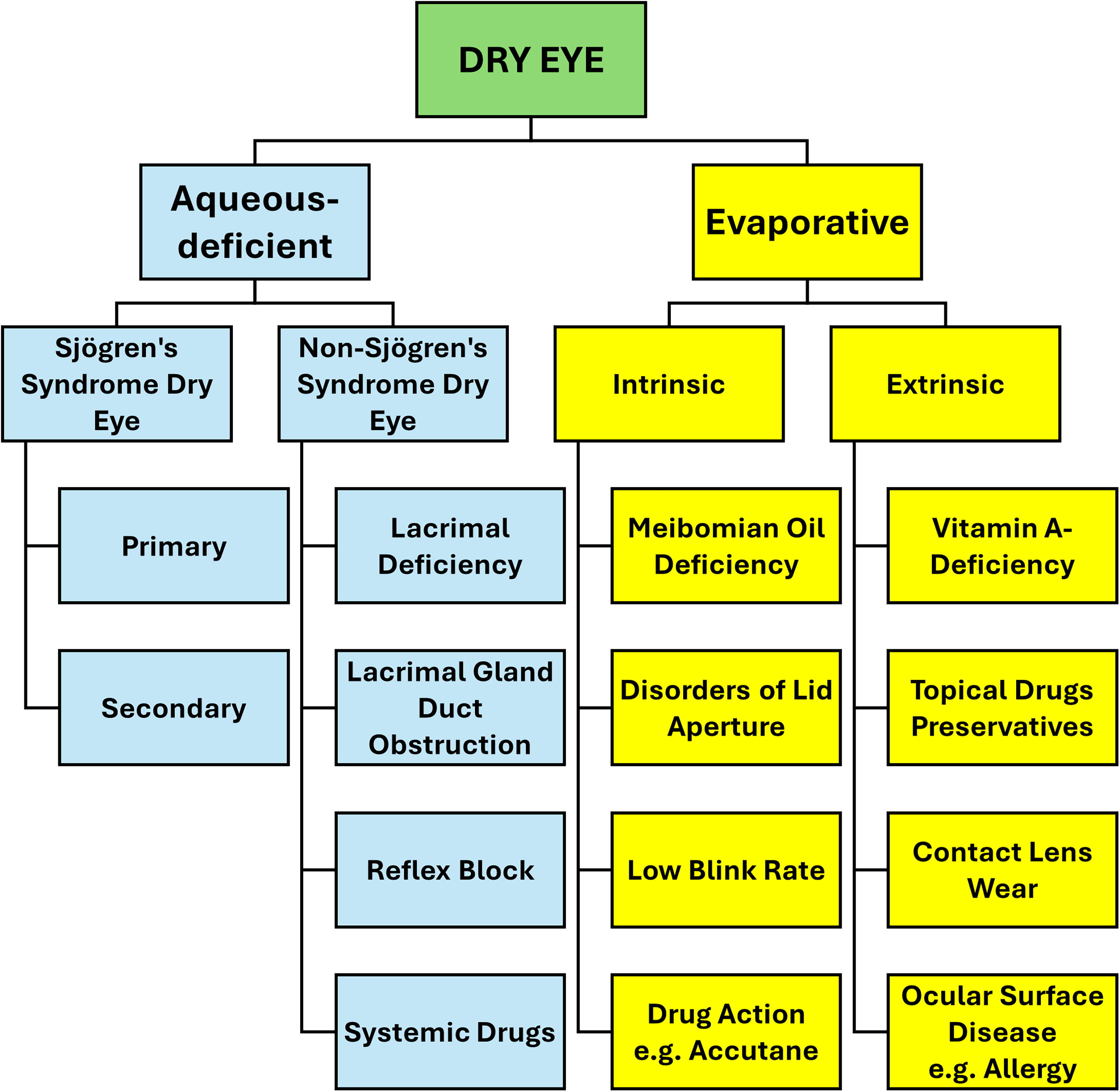
Etiopathogenic classification of DED from the 2007 TFOS DEWS I Report. Adapted with permission from the Report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). 14 DED, dry eye disease.
Aqueous-deficient dry eye
ADDE is observed when the lacrimal glands do not adequately secrete the aqueous component of the tear fluid, leading to tear hyperosmolarity despite a normal tear evaporation rate. 15 This typically results in tear film instability, poor wetting, higher friction, and chronic mechanical irritation, triggering a cascade of inflammatory events and damaging the ocular surface. 16
ADDE can be further classified into Sjögren’s syndrome dry eye (SSDE) and non-Sjögren’s syndrome dry eye (NSSDE). SSDE is an autoimmune disorder that mainly affects the exocrine glands of mucous membranes. 17 It is characterized by mononuclear infiltration of the lacrimal and salivary glands, leading to gland destruction and manifestation of the acute symptoms of DED and dry mouth. 18 While the exact etiology of SSDE is still poorly understood, genetic predisposition, environmental factors, including viruses, and hormonal changes, such as estrogen deficiency which accounts for the higher prevalence of SSDE in women, often play a role in the manifestation of the disease. 19 Furthermore, it may also develop secondary to other autoimmune disorders, such as rheumatoid arthritis, lupus, 20 hepatitis C, 21 and HIV-AIDS. 22 The inflammatory processes in SSDE start primarily via glandular epithelial cells, which can express antigen-presenting proteins, promote adhesion, and co-stimulate T lymphocytes. Interferon (IFN)-γ and tumor necrosis factor (TNF)-α may enhance the antigen-presenting function of epithelial cells through upregulation of the Fas protein, a cell surface receptor whose activation leads to programmed cell death. 23 In comparison to controls, the eyes of SSDE patients exhibit significantly higher levels of proinflammatory cytokines including interleukin (IL)-1, IL-6, and IL-8, as well as decreased epidermal growth factor (EGF) levels. 24 In a recent study, increased IL-8 levels were observed in SSDE but not NSSDE patients, suggesting that IL-8 can potentially be used as a biomarker to differentiate between SSDE and NSSDE. 25
In NSSDE, on the contrary, lacrimal dysfunction is observed without the autoimmune features characteristic of SSDE. An age-related increase in ductal pathologies is most commonly responsible for the pathogenesis of NSSDE. 26 Additionally, several other medical conditions, such as congenital alacrima, allergic eye disease, 27 and thyroid disorders 28 may increase predisposition to NSSDE. Certain medications, such as decongestants 29 and hormone replacement therapy, 30 may also trigger NSSDE. While inflammation is a common factor in both ADDE types, the inflammatory pathways involved are believed to be different with incremental changes in IL-1β, IL-10, and TNF, but not IL-8, being evident in NSSDE. 25
Evaporative dry eye
EDE, the more common form of DED, is observed due to a compromised quality and/or quantity of the tear film lipid layer leading to excessive evaporation of the underlying aqueous layer, despite normal lacrimal secretory function. 14 A compromise in tear quality is typically observed in EDE, resulting in tear film instability, poor wetting, increased osmolarity, higher friction, and chronic mechanical irritation on the ocular surface, which in turn triggers a cascade of inflammatory events leading to corneal and conjunctival cell apoptosis. 16 EDE is frequently associated with meibomian gland dysfunction (MGD), with a significant increase in meibomian gland dropout being evident after 40 years of age.31,32 MGD may also be caused by a deficiency in sex hormones, such as androgens, which stimulate meibomian lipid secretion and inhibit keratinization.33,34 Therefore, hormone changes or deficiency can alter the meibomian lipid profile and thus reduce tear film stability.35–37 Posterior blepharitis can also trigger MGD-mediated EDE 6 since it affects the meibomian glands and their orifices, altering glandular secretions both qualitatively and quantitatively. 38
Disorders of the lid aperture, congruity, or dynamics, as well as a low blink rate, may also contribute to the manifestation of EDE. Ocular surface-related EDE due to allergic diseases, such as allergic conjunctivitis or vitamin A deficiency,39,40 topical agents,12,41,42 contact lens wear, and environmental factors may also be observed. Prior literature has confirmed a correlation between tear IFN‐γ concentrations, tear osmolarity, total ocular surface staining, and Schirmer test score, suggesting that IFN‐γ, which is considered a proinflammatory cytokine, is a potential biomarker of tear hyperosmolarity-associated with EDE. 43
Clinical Signs of DED
Various techniques are used to diagnose DED based on tear volume, tear film stability, tear film composition, ocular surface damage, and ocular surface inflammation with the diagnostic tests used in clinics captured in the TFOS DEWS II Diagnostic Methodology Report. 44 This report also suggests using a symptoms questionnaire to screen patients before signs of DED are evaluated. Further testing such as MGD/abnormal lipid tests and tear volume examination can be performed to confirm the DED subtype. 44 In preclinical studies, DED signs are established using at least one homeostasis marker test, that is, noninvasive tear break-up time, osmolarity, or ocular surface staining. The different diagnostic tests and procedures relevant to assessing DED severity in preclinical models are listed in Table 1. While most of these determine ocular surface inflammation indirectly, a few directly measure inflammation and are further described below.
Diagnostic Tests for Dry Eye Disease
Table adapted with permission from Wolffsohn JS, Arita R, Chalmers R, et al. 44
Diagnostic tests most commonly employed in preclinical studies. 44
ADDE, aqueous-deficient dry eye; CXCL, CXC motif chemokine ligand chemokines; CXCR, C-X-C chemokine receptor; DED, dry eye disease; EDE, evaporative dry eye; IL, interleukin; INF, interferon; LIPCOF, lid parallel conjunctival folds; MMP, matrix metalloproteinases; NIBUT, noninvasive tear film break-up time; TBUT, tear film break-up time; Th, T helper.
Impression cytology
Impression cytology (IC) is a simple and practical approach performed under topical anesthesia in which cells from the conjunctival epithelium, ranging from the most superficial to the third layer, are selectively extracted using cellulose acetate filters or biopore membranes. The extracted cells can then be subjected to diverse analytical techniques, such as microscopy, immunocytochemistry, immunoblotting analysis, polymerase chain reaction, and flow cytometry. The choice of analysis method is contingent upon the specific investigation objectives. 47 The Nelson classification system is most commonly used to assess conjunctival epithelial and goblet cells based on their density, morphology, cytoplasmic staining characteristics, and nucleus-to-cytoplasm ratio. 48 Rajpoot et al. 49 conducted a Nelson grade assessment using conjunctival IC to evaluate the effectiveness of two eyedrops having different CsA concentrations (0.05% and 0.09%). Their findings revealed that there were no statistically significant differences between the two groups in terms of the Nelson grade, goblet cell density, and TFBUT. Yoon et al. 50 employed immunohistochemical staining of conjunctival IC samples obtained from patients with DED (both with and without SSDE) incubated with anti-IL-6 and TNF-α antibodies. IL-6 was found highest in samples from patients with SSDE, but less in patients with NSSDE, and was scarcely detectable in control samples. Furthermore, a significant correlation was observed between IL-6 levels and conjunctival goblet cell density in DED patients, while TNF-α was undetectable in all groups.
In vivo confocal imaging
Confocal microscopy is a noninvasive technology that allows in vivo assessment of morphological changes in ocular surface tissues. 51 It is used to evaluate ocular surface damage in DED at the cellular level, such as decreased corneal and conjunctival epithelial cell density, conjunctival squamous metaplasia, and corneal nerve changes. 44 Lately, in vivo confocal imaging of corneal dendritic cells was found helpful in forecasting and monitoring the effect of anti-inflammatory drugs. 52 Villani et al. 53 performed in vivo confocal microscopy on the cornea of DED patients and reported that the ocular surface disease index score and dendritic cell density significantly decreased after treatment with corticosteroids. Qazi et al. 54 used this technique to investigate palpebral conjunctival and corneal inflammation in patients with MGD with increased immune cells found in the palpebral conjunctiva, but not in the cornea. Meanwhile, Wu et al. 55 used this technique to investigate the effect of seasonal environmental factors on the morphodynamic features of human corneal immune cell subsets. These findings suggest that corneal intraepithelial dendritic cells are influenced by seasonal changes, whereas T cells remain unaffected. These studies further discuss that these two immune cell subsets likely exhibit different behaviors in the corneal epithelium.
Matrix metalloproteinases
Increased levels of matrix metalloproteinases (MMP) have been found in tears 44 and corneal epithelial cells 56 of DED patients, with quantification of MMP-9 in tears being a direct measure of ocular surface inflammation. Different methods, such as an enzyme-linked immunosorbent assay, polymerase chain reaction, and the InflammaDry® assay (Quidel Corporation, CA, USA), have been used to detect MMP-9 in tears.44,57 InflammaDry is a rapid and sensitive immunoassay method based on a direct sampling microfiltration technology, which can detect MMP-9 levels in tears of patients suspected to have DED. 56 Normal tear MMP-9 levels typically fall between 3 and 40 ng/mL. 58 However, in cases of moderate-to-severe DED, MMP-9 levels can exceed 40 ng/mL. 57 Sambursky et al.58,59 conducted two studies with sample sizes of 143 and 237 patients, respectively, both of which demonstrated that the InflammaDry was a useful diagnostic tool for DED having a sensitivity of 85%, specificity of 94%, negative predictive value of 73%, and positive predictive value of 97%.
Cytokines and chemokines
Using multiplex bead assays, many cytokines, chemokines, and chemokine receptors have been identified as tear biomarkers in DED. These include elevated levels of IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12, IL-13, IL-17, IL-21, IFN-γ, TNF-α, CXCL9, CXCL10, CXCL11, IL-1Ra, CCL5/RANTES, and fractalkine/CX3CL1.60–62 Increased cytokine and chemokine levels can often also be correlated to the DED subtype. For example, increased levels of IL-17, IL-22, IL-6, IL-10, IL-4, IFN-γ, and TNF-α have been observed in SSDE, 60 while elevated levels of TNF-α, IL-6, and IL-1β have most commonly been found in mixed DED. 63 Moreover, significantly upregulated levels of IL-1β, IL-6, IL-8, IL-10, IL-17, IL-18, IFN-γ, TFN-α, and transforming growth factor (TGF)-β have been found in experimental DED models.64–68
Animal Models of DED
Animal models have significantly improved our understanding of the pathophysiology of DED and are frequently employed to establish the safety and efficacy of therapeutic interventions. Murine models are often the first choice due to the relatively lower cost, versatility of different knockout and transgenic strains, as well as the excellent availability of mouse-specific antibodies. However, differences in their ocular anatomy and physiology, especially due to the smaller eye size and lower tear volume, 69 limit the translation to clinical studies. Rabbits have a larger eye globe and tear volume and generally enable a better correlation to clinical studies. However, some interspecies differences do exist between the rabbit and human eye, with rabbit eyes having a larger ocular surface area, thinner and less concave cornea, thicker tear fluid lipid layer, lower blinking rate, as well as the presence of a nictitating membrane. 70 Moreover, the rabbit lipidome and tear film composition differ significantly from human tears, which are, in fact, more closely related to the murine tear film. 71 Spontaneous canine models, although closer to the human DED etiology, have been used less frequently, mainly due to ethical and economical constraints.72–74 Moreover, the identification and recruitment of animals with spontaneous DED are challenging and time-consuming.3,74 Although the cause of canine DED is currently unknown, it is believed to have an autoimmune etiology, similar to that observed in SSDE. 74
Various animal models, having characteristic ADDE, EDE, or combined etiologies, have been developed and studied, although the mechanism of disease induction in these models often does not replicate the clinical etiology. Moreover, in most traditionally used preclinical models of DED, the manifestation of inflammation is casual rather than causal, that is, inflammation is developed as a downstream effect (as observed in models with secondary inflammation) rather than being the trigger for entry into the vicious circle of DED (as observed in models with primary inflammation). Table 2 lists preclinical models of DED that have been classified as primary and secondary models, with models used to test anti-inflammatory therapies further discussed below. It should be noted though that while inflammation is not directly induced in the secondary models of DED, downstream inflammation eventually becomes apparent due to the cyclic nature of the disease.
Animal Models of DED
BAC, benzalkonium chloride; MGD, meibomian gland dysfunction; MMP, matrix metalloproteinases; NOD, nonobese diabetic; NSSDE, non-Sjögren’s syndrome dry eye; oGvHD, ocular graft versus host disease; SMA, smooth muscle actin; SSDE, Sjögren’s syndrome dry eye; TBUT, tear film break-up time; TGF, transforming growth factor; TNF, tumor necrosis factor; TSP-1, thrombospondin-1.
The first autoimmune model of Sjögren’s syndrome was developed by Guo et al., 75 who induced autoimmune dacryoadenitis by injecting activated autologous lymphocytes into the contralateral lacrimal gland resulting in inflammatory infiltration observed as CD18, rabbit thymic lymphocyte antigen, and CD4 positive cells along with increased major histocompatibility complex molecule-II expression in interstitial and ductal epithelial cells. 113 Lin et al. 114 used the autoimmune dacryoadenitis model to test the efficacy of a single subconjunctival injection of a dexamethasone-dendrimer (Dex-D) conjugate. The study revealed a significant reduction in the expression of proinflammatory genes, including MMP-9, IL-6, IL-8, and TNF-α, in the group treated with the Dex-D in comparison to the groups treated with free dexamethasone and saline. The study concluded that subconjunctival administered Dex-D effectively mitigated inflammation in the lacrimal glands, resulting in partial restoration of lacrimal gland function and improvement in clinical signs of DED.
The MRL/lpr mouse (SSDE model) was initially developed to study systemic lupus erythematosus, but coexisting Sjögren’s syndrome and T-cell-initiated lacrimal gland inflammation were also observed. 115 Similar to the observations made in humans, female MRL/lpr mice show significantly greater inflammation in lacrimal and salivary glands than male mice of the same age. 116 Jabs et al. 76 used MRL/lpr mice to evaluate the efficacy of CsA in the management of autoimmune DED and found that intraperitoneal CsA administration (2 mg daily from age 1 to 5 months) effectively controlled autoimmune disease and reduced the signs of DED.
TSP-1 null mice, initially exhibiting a normal appearance at birth, subsequently develop chronic ocular surface disease characterized by an increased rate of cell apoptosis, progressive deterioration of the lacrimal glands, and the development of inflammatory infiltrates, ultimately leading to an abnormal composition and secretion of tears. Elevated CD4+ T cells within inflammatory infiltrates of the lacrimal gland in conjunction with the presence of anti-Sjögren’s syndrome antigen A and B antibodies in the serum, closely parallels, the autoimmune characteristics of Sjögren’s syndrome. These mice subsequently develop DED, characterized by disruptions in the corneal epithelial layer, corneal edema, and a notable reduction in conjunctival goblet cells. 77 Basova et al. 117 utilized the TSP-1 null mouse to assess the suppression of inflammation through the modulation of Pannexin-1 (Panx1) membrane channel glycoprotein activity. They found that TSP-1 null mice treated with a Panx1-specific blocking peptide or a self-deliverable RNAi exhibited a significant decrease in the expression of proinflammatory markers and lymphocyte infiltration.
Nonobese diabetic (NOD) mice are another well-established model of SSDE, characterized by autoimmune inflammation of lacrimal (dacryoadenitis) and salivary (sialoadenitis) glands with male and female NOD mice having different patterns of disease development and progression.118,119 At 12 weeks, male NOD mice develop autoimmune dacryoadenitis but not sialoadenitis, while female mice develop autoimmune sialoadenitis at ∼12–20 weeks of age and mild lacrimal gland inflammation at 20 weeks. As such, male NOD mice are better suited for studying DED-associated inflammation. Using this model, Shal et al. 78 demonstrated that 0.05% rapamycin eyedrops instilled twice daily for 12 weeks starting at 8 weeks of age efficiently suppressed autoimmune inflammation of the lacrimal glands and restored ocular surface homeostasis.
In 1979, Quimby et al. 120 first recognized the canine spontaneous DED model, noting significant similarities between SSDE in humans and the severe keratoconjunctivitis sicca exhibited by dogs, featuring clinical symptoms such as xerostomia, vaginal dryness, and the presence of various serum antibodies. Gao et al. 121 used this model to investigate the role of apoptosis in the pathophysiology of DED and assess the therapeutic effects of CsA and, particularly, its impact on apoptosis. Their findings suggested that topical CsA enhances lymphocytic apoptosis, reduces epithelial cell apoptosis, and helps restore the normal apoptotic balance.
Another model of lacrimal gland inflammation was reported by Nagelhout et al. 80 by injecting T-cell mitogen Concanavalin A in rabbit lacrimal glands. Concanavalin A is a prototypic T-cell mitogen that develops and triggers T-cell-mediated inflammation of the lacrimal glands leading to inadequate secretion of the aqueous component of tears and disrupting ocular surface homeostasis. 80 Elevated levels of MMP-9 along with proinflammatory cytokines such as IL-1β, IL-8, and TGF-β1 were detected in the lacrimal glands.80,81 Lee et al. 122 used this model to evaluate the ability of mesenchymal stem cells (MSCs) to suppress ocular surface inflammation by repairing tissues that modulate excessive immune responses. They found that MSCs lowered inflammatory cytokines and infiltration of CD4+ T cells into the intraorbital lacrimal glands and ocular surface, while also enhancing tear production and goblet cell density to maintain ocular surface homeostasis. 122
The benzalkonium chloride (BAC)-induced EDE mouse model has also been used to evaluate the therapeutic effect of anti-inflammatory agents. BAC is a quaternary ammonium compound used as a preservative in eyedrops. However, it also alters the tear film’s lipid layer and damages epithelial cell membranes causing rapid and progressive tear instability. Clinical data have demonstrated that topical administration of 0.2% BAC can result in the manifestation of ocular surface disorders, including inflammation, epithelial apoptosis, squamous metaplasia, and reduced TBUT, which are all considered key players in the pathogenesis of DED.90,123 While BAC-induced DED models are often categorized as EDE models, reduced tear secretion also becomes evident after prolonged instillation of BAC, leading to the manifestation of a mixed form of DED with features of both EDE and ADDE typically observed clinically. Xiao et al. 124 used this model to investigate the therapeutic effects and mechanism of action of EGF. They found that topical application of EGF (3 ng per day for 6 days) significantly reduced DED signs by stabilizing the tear film and maintaining epithelial integrity. 124 Wang et al. 125 used the model to investigate the efficacy and mechanisms of mouse adipose-derived MSC-derived exosomes. They found that exosomes promoted ocular surface epithelial repair, restored goblet cells, increased tear secretion, and prevented the production of proinflammatory cytokines by inhibiting the NLRP3 inflammasome pathway. 125 Meanwhile, Shanmugham et al. 91 evaluated the effects of oral capsanthin in a BAC-induced DED model and showed clinical benefits by maintaining corneal surface integrity and ameliorating ocular surface inflammation. Capsanthin treatment resulted in a noteworthy suppression of proinflammatory cytokines, TNF-α, interleukins (IL-2, IL-4, IL-6), and the proinflammatory mediator, MMP-9.
Surgical removal of the lacrimal glands is one of the most commonly employed approaches for DED induction in murine and leporine models. The excision of the principal lacrimal gland promptly leads to a reduction in the production of the aqueous component of the tears. Yousefi-Manesh et al. 126 utilized this model to investigate the anti-inflammatory properties of saffron, observing a decrease in TNF-α, IL-1β, and IL-6 levels. Xiao et al. 127 employed this model to evaluate the effect of daidzin by targeting the suppression of inflammation and oxidative stress in the cornea. After 2 weeks of treatment, administered four times a day, daidzin effectively suppressed the expressions of IL-6 and MMP-9.
The botulinum toxin B-induced mouse model is an ADDE model mimicking human NSSDE. Injection of botulinum toxin B into the lacrimal gland blocks lacrimal secretion, resulting in ocular surface changes such as reduced corneal integrity95,128,129 and ocular surface inflammation.129–131 A significant elevation IL-1β and TNF-α mRNA expression in corneal and conjunctival epithelia has been observed within 2 weeks of injection, although by week 4, a return to baseline values was reported. 129 Lekhanont et al. 8 used this model to compare the efficacy of anti-inflammatory agents (CsA or fluorometholone), either individually or in combination with lubricant eyedrops, reporting restoration of baseline tear production within 2 weeks of administration. On the contrary, no significant difference was observed between saline and artificial tear application, suggesting that inflammation plays a key role in the manifestation of DED after injection of botulinum toxin B. 8
Zheng et al. 105 first reported the presence of inflammasome components on the ocular surface of mice exposed to desiccating stress. They found that increased reactive oxygen species (ROS) generation leads to NLRP3 inflammasome activation and caspase-1-mediated IL-1β secretion. This was the first study to demonstrate a direct association between a time-dependent increase in ROS generation and the development of established DED indicators. 105 The study found that using 0.3% N-acetyl-L-cysteine ophthalmic solution resulted in a substantial reduction of ROS generation, subsequently leading to a downregulation in NLRP3 and IL-1β levels in ocular tissues of mice exposed to a desiccating environment.62,105
Combined ADDE and EDE models closely mirror the clinical manifestation of DED where a significant overlap between the two DED subtypes is commonly observed. Dursun et al. 106 developed a combined DED model with mice exposed to desiccating stress in a controlled environment chamber after inhibiting the lacrimal functional unit with systemic anticholinergic agents. Desiccation activated NF-κB and MAPK innate signaling pathways in the immune cells present in ocular surface tissues, causing secretion of proinflammatory cytokines (IL-17 and IFN-γ), chemokines, and MMPs. 132 Topical application of CsA in this model significantly reduced conjunctival epithelial cell apoptosis and protected against goblet cell loss. 133 Kessal et al. 112 also compared combined DED mouse models in which mice were exposed to desiccating stress and either treated with scopolamine or subjected to bilateral excision of the exorbital lacrimal glands. They suggested the involvement of different pathophysiological mechanisms affecting different targets in each model, resulting in the modulation of different inflammatory mediators depending on the causative factor even when similar biological responses were observed. Their results demonstrated that irrespective of the pathology, inflammation plays a key role in the mediation of downstream effects and propagation of the vicious circle of DED, thus highlighting the need to include anti-inflammatory therapy in the management of DED.
Therapeutic Strategies to Manage Inflammation in DED
Management of DED can be highly challenging due to its multifactorial and chronic nature. Historically, tear insufficiency was considered the principal cause of DED; therefore, tear supplementation is usually the first line of treatment. Other management strategies include improved lid hygiene, tear supplementation, anti-inflammatory therapies, antibiotics, surgical approaches, dietary modifications, environmental management, and other complementary therapies, including natural and herbal medicines, honey, milk, and acupuncture (Fig. 2). Topical medications specifically targeting inflammation in DED that are currently available in the United States include Restasis® (0.05% CsA ophthalmic emulsion), Cequa® (0.09% CsA ophthalmic solution), VEVYE™ (0.1% CsA ophthalmic solution), Xiidra® (5% lifitegrast ophthalmic solution), and various steroid eyedrops.134–136 This section briefly summarizes current strategies for the management of inflammation in DED and discusses future developments in the field.

Management strategies for inflammation in DED. MMP, matrix metalloproteinases; NSAIDs, nonsteroidal anti-inflammatory drugs.
Current therapeutic strategies for management of inflammation in DED
Anti-inflammatory agents
While artificial tear supplements may transiently reduce tear hyperosmolarity and thus inflammation, specific anti-inflammatory agents are often required in moderate-to-severe cases to address the underlying inflammation and inhibit downstream effects that potentiate DED.137,138 Indeed, a number of therapeutic agents available for the management of DED exert an anti-inflammatory effect, with the criteria for selection based on disease severity and different patient populations outlined in the DEWS II management and therapy report. 137
Corticosteroids
Topical corticosteroids inhibit MMPs, inflammatory cytokines, and adhesion molecule expression, leading to decreased ocular surface inflammation. 139 Randomized controlled clinical studies have shown that the application of preservative-free corticosteroid eyedrops improves the symptoms and clinical signs of moderate-to-severe DED within 2 – 4 weeks.140,141 However, long-term use of corticosteroids can cause ocular complications, including elevated intraocular pressure and cataract formation. Therefore, short-term therapy with “soft” corticosteroids is preferred.6,140 Regular monitoring of intraocular pressure and lens clarity before and during corticosteroid treatment is generally recommended. 142 Several corticosteroid formulations, such as loteprednol etabonate suspension, prednisolone acetate suspension, and fluorometholone suspension, are prescribed for treatment of DED-associated inflammation.143–145 Eysuvis® 0.25% loteprednol etabonate ophthalmic suspension based on the mucus penetrating particle technology by Kala Pharmaceuticals (Watertown, MA, USA) was the first ocular corticosteroid approved by the United States Food and Drug Administration (FDA) (on-label) in 2020 for short-term (up to 2 weeks) DED therapy. 143
Cyclosporine A
CsA is an immunosuppressant that reduces ocular inflammation by blocking T-cell infiltration, activation, and the subsequent release of inflammatory cytokines. 146 CsA disrupts the ongoing immune reaction by preventing activation of conjunctival T cells, restoring conjunctival goblet cell density, reducing transcription of inflammatory cytokines such as IL-2, and decreasing epithelial cell apoptosis. 147 Because of its hydrophobic nature, CsA has poor aqueous solubility (27.67 μg/mL at 25°C), 148 which makes it challenging to formulate for safe and efficient ocular drug delivery. As such, CsA formulations have traditionally been developed using oil-based solvents such as castor oil; however, oils may cause adverse effects such as blurred vision, burning, and stinging.149,150 In addition, oil-solubilized CsA has very low bioavailability, as lipophilic CsA has a greater affinity for the oil-based vehicle than for the target tissues. 151
The first commercial CsA formulation, Restasis® 0.05% CsA ophthalmic emulsion (Allergan, Irvine, CA, USA), was approved by the FDA in 2003 to increase tear production in patients with lacrimal compromise. 146 It is a white opaque to slightly translucent homogeneous emulsion, having an osmolality of 230–320 mOsmol/kg and a pH between 6.5 and 8.0. It contains CsA, glycerin, castor oil, polysorbate 80, carbomer copolymer type A, sodium hydroxide, and purified water.152,153 In 2015, the European Medical Agency (EMA) approved Ikervis® (0.1% CsA, Santen, France) for the treatment of severe keratitis in adults with DED, which has not improved despite tear supplementation. 146 Ikervis is an opaque emulsion containing medium-chain triglycerides, cetalkonium chloride, glycerol, tyloxapol, poloxamer 188, sodium hydroxide, and water for injection. 154 In 2018, the FDA-approved Cequa® (0.09% CsA, Sun Pharmaceutical Industries, NJ, USA), 146 a clear nanomicellar formulation of CsA having an osmolality of 160–190 mOsmol/kg and a pH of 6.5–7.2. In addition to CsA, it contains polyoxyl-40 hydrogenated castor oil, octoxynol-40, polyvinylpyrrolidone, sodium phosphate monobasic dihydrate, sodium phosphate dibasic anhydrous, sodium chloride, water for injection, and sodium hydroxide or hydrochloric acid. 155 Recently (in 2023), the FDA also approved VEVYE™ (0.1% CsA, Harrow, USA), which represents a groundbreaking advancement in the field of DED treatment, as it is the sole commercially available water-free CsA formulation that is devoid of preservatives and surfactants.156–160 In addition to CsA, it contains perfluorobutylpentane and ethanol (anhydrous) and has demonstrated efficacy in treating clinical signs of DED within 4 weeks.104,161
Lifitegrast
Lifitegrast is a small-molecule lymphocyte function-associated antigen-1 (LFA-1) antagonist. 162 It suppresses inflammation by binding to LFA-1 and stops it from interacting with intercellular adhesion molecule-1, resulting in inhibition of the adhesion, activation, migration, and proliferation of lymphocytes, which ultimately leads to cytokine secretion (e.g., IFN-γ, IL-4), cell destruction, and self-amplification of the inflammatory immune response that further intensifies DED.137,162,163 In 2016, the FDA-approved Xiidra (5% lifitegrast ophthalmic solution, Shire Pharmaceuticals, MA, USA).136,164 Several clinical trials have proven the efficacy of 5% lifitegrast in improving DED signs and symptoms.165–167 The most commonly reported adverse effects were eye irritation, dysgeusia, and reduced visual acuity. 162
Nonsteroidal anti-inflammatory drugs
Various topical nonsteroidal anti-inflammatory drugs (NSAIDs) have also been used to manage DED. NSAIDs tackle inflammation by impeding the production of prostaglandins via the cyclooxygenase enzyme. 168 Currently used topical NSAIDs include Acular® (0.5% ketorolac tromethamine ophthalmic solution, Allergan Inc., CA, USA), 169 and Bromday™ (0.09%, Bromfenac ophthalmic solution, Bausch and Lomb Inc., FL, USA). 170 However, several cases of corneal melt associated with topical NSAID application have been reported171,172; therefore, NSAIDs are only recommended for short-term use (<1 month) under supervision.137,173,174
Azithromycin
Azithromycin is a broad-spectrum macrolide antibiotic that can be used to treat MGD in association with rosacea and blepharitis.175,176 AzaSite® (1% azithromycin in polycarbophil, InSite Vision Inc., Alameda, CA, USA) is an FDA-approved eyedrop and Azyter® (1.5% w/w azithromycin in MCT, Laboratories Thea, Clermont-Ferrand, France) is an EMA-approved eyedrop to treat bacterial conjunctivitis. 12 However, azithromycin has also been used off-label for the management of several other ocular conditions, including blepharitis, MGD, DED, trachoma, and infectious keratitis.156,177,178 The anti-inflammatory effect of azithromycin has been attributed to the suppression of proinflammatory mediators in cultured human corneal epithelial cells. 179 Studies have shown that topical application of 1 – 1.5% azithromycin ophthalmic solution once or twice daily for 3–30 days improved DED signs and symptoms and restored lipid layer properties in patients with chronic blepharitis.180–184
Tetracycline derivatives
Oral tetracyclines and their derivatives (doxycycline and minocycline) are frequently used to treat various forms of MGD and DED associated with anterior blepharitis and rosacea. Tetracyclines are antibiotics with additional anti-inflammatory properties and exert their anti-inflammatory effect by decreasing the activity of collagenase, phospholipase A2, and several MMPs while also reducing the production of inflammatory mediators, such as IL-1β and TNF-α, in a wide range of tissues, including the corneal epithelium.137,178,185,186
Artificial tear supplements
Tear supplementation is traditionally considered the mainstay of DED therapy, irrespective of the subtype. 6 While artificial tear supplements are typically recommended to provide symptomatic relief due to an immediate reduction in tear osmolarity, replacement of absent tear constituents, and reduction of friction between the palpebral conjunctiva and cornea, there is some evidence that artificial tear supplements can also directly ameliorate ocular surface inflammation by diluting tear inflammatory cytokines and/or reducing the susceptibility of the ocular surface to inflammation. 142
Aqueous artificial tear supplements
Aqueous supplements attempt to mimic tears and improve tear stability to provide symptomatic relief and improve patient comfort. 187 Often, they can also ameliorate ocular surface inflammation by transiently reducing hyperosmolarity.188,189 Certain components may also exert a direct anti-inflammatory effect. 190 Hyaluronic acid (HA), for instance, has been shown to suppress CD4+ expression in DED.191–193 Meanwhile, trehalose eyedrops have been shown to suppress proinflammatory cytokine upregulation in preclinical models.194–196
Lipid-containing artificial tear supplements
Lipids are often incorporated in artificial tear supplements to help stabilize the tear film lipid layer, especially in EDE.197,198 Systane® Balance (Alcon Laboratories, Fort Worth, TX, USA), for example, contains hydroxypropyl guar (in situ gelling agent), dimyristoyl phosphatidylglycerol (a phospholipid), and propylene glycol and mineral oil (lipids) for stabilization of the tear film lipid layer.199,200 Lipid-containing eyedrops are typically formulated as emulsions using stabilizing agents or surfactants, in addition to preservatives, which may cause toxicity on the ocular surface, 13 especially in DED. Cationorm® (Santen Pharmaceutical, Osaka, Japan), a commercial lipid-containing, preservative-free, hydrating, and lubricating emulsion eyedrop, has shown anti-inflammatory action by reducing inflammatory cells in vivo and decreasing IL-6 and IL-8 secretion in vitro. 190
Liposomal sprays
Liposomal sprays can also improve patient outcomes in EDE, 201 by improving the polar properties of the lipid layer due to enriching it with phospholipids and enhancing the spreading of tear film lipids. 202 Tears Again® (Optima Pharmazeutische GmbH, Hallbergmoos, Germany) is a commercially available liposomal formulation believed to be beneficial in EDE. The spray is applied to the closed eyelids, and the liposomes migrate via the lid margins into tear film to improve lipid layer stability and patient comfort.201,203 In a double-blind study with 382 patients, Lee et al. 204 reported a considerable reduction in inflammation at the periphery of the eyelid. Notably, the group undergoing treatment with Tears Again exhibited statistically significant improvements in key clinical parameters, including lid parallel conjunctival folds, tear film break-up time, and Schirmer test results, surpassing the outcomes observed in the control group.
Autologous serum
The biochemical characteristics of serum, such as pH, osmolarity, nutrient content, including vitamins and fibronectin, and growth factors such as EGF or nerve growth factor, are similar to that of human tears, with a few exceptions including higher concentrations of vitamin A, lysozyme, TGF‐β, and fibronectin as well as lower concentrations of immunoglobulin A, EGF, and vitamin C.205,206 Hence, autologous serum can be used as a lacrimal substitute since it not only provides lubrication but also contains other biochemical components that enable them to more closely mimic natural tears. 206 Serum can suppress the release of proinflammatory cytokines and increase goblet cell density and mucin expression in the conjunctiva. 137 In addition, serum contains anti-inflammatory components thought to be packed inside extracellular vesicles, 207 such as the IL-1 receptor antagonist, which has been reported to decrease DED signs in murine models.208,209 Although autologous serum has many advantages, its application in the management of DED is met with practical limitations, such as susceptibility to contamination, short shelf-life, 210 and the cost of manufacturing and dispensing autologous serum eyedrops. 211 However, despite these limitations, the use of autologous serum in the management of severe DED cases has been found promising. 212
Anti-inflammatory therapeutics in the pipeline
Due to the high prevalence and debilitating nature of DED, new therapeutics are constantly being developed to improve the patients’ quality of life. In addition to the currently available anti-inflammatory therapeutics discussed above, new therapeutic moieties as well as improved formulations of currently approved molecules are being developed to manage the inflammatory component of DED more effectively.
MC2-03
MC2-03 is a CsA eyedrop based on the PAD™ technology (MC2 Therapeutics, Hørsholm, Denmark), with polyaphrons dispersed in a carbomer hydrogel to transport CsA to the target site. Polyaphrons are lipid-based formulations with a high concentration of the dispersed oil phase and a low ratio of surfactant to oil in comparison to conventional emulsions. 158 Preliminary results from a Phase 2 study (EudraCT 2015-000937-54) in DED patients with moderate-to-severe keratitis have shown a clinically relevant response (defined as two-grade improvement in corneal staining on the modified Oxford scale) in a significantly higher percentage of patients after 6 months of treatment with 0.06% MC2-03 in comparison to a lubricant eyedrop (43.1% vs. 22.8%, p = 0.0289). 158
Reproxalap
Reproxalap ophthalmic solution (Aldeyra Therapeutics Inc., Lexington, MA, USA) contains 0.25% reproxalap, a novel small-molecule immune-modulating covalent inhibitor of reactive aldehyde species. 213 As reported in Phase 2a/2b clinical trials (NCT03162783 and NCT03404115), reproxalap is well-tolerated and effective in mitigating DED symptoms.214,215 In a randomized, double-masked, vehicle-controlled Phase 2b trial (NCT03404115), reproxalap demonstrated rapid, broad, and clinically relevant symptomatic control in DED patients over 12 weeks of therapy, with a significant reduction in fluorescein staining. 215 In the Phase 3 TRANQUILITY clinical trial (NCT04674358), while the primary endpoint (ocular redness) was not successfully met, a statistically significant outcome was observed for the secondary endpoint (Schirmer test result). 216
Visomitin®
Visomitin eyedrops (Mitotech S.A., Luxembourg) contain SkQ1, a novel small-molecule cardiolipin peroxidation inhibitor that enters cells and accumulates in the inner leaflet of the mitochondrial membrane. It decreases damage induced by the overproduction of mitochondrial ROS through the transition between the reduced and the charged form. Furthermore, it reduces the production of TNF-α and IL-6, exerting an anti-inflammatory effect on the cornea. 217 Treatment with SkQ1 has shown improved tear film stability and regeneration of the corneal epithelium in DED patients.218,219 A Phase 3 clinical trial (VISTA-2 trial; NCT04206020) demonstrating safety and efficacy in a Controlled Adverse Environmental (CAE®) Model has recently been completed. 220 While the data have not been published yet, the company website has reported positive results. 220
SDP-4
Silk-derived protein 4 (SDP-4; SilkTech Biopharmaceutical, Plymouth, MN, USA), a purified molecule derived from Bombyx mori silkworm cocoon fibers, 221 reportedly inhibits inflammatory signaling mediated by NF-κB. 222 SDP-4 1% ophthalmic solution has a dual action, as it not only ameliorates inflammation but also improves tear film stability by inherent spreading and wetting properties of the soluble protein.221,222 Phase 2 clinical trials (SDP-4-CS201 and SDP-4-CS202) have recently been completed, and the results are awaiting review.
Tanfanercept
Tanfanercept, also known as HBM9036 (Harbour Biomed, Shanghai, China), is a modified 19 kDa TNF receptor 1 fragment that binds to TNF-α and blocks downstream effects, resulting in reduced inflammation. 223 Tanfanercept eyedrops have shown significant clinical improvements in clinical signs and Schirmer scores in DED animal models. 224 In Phase 2 clinical trials (NCT04092907), a 0.25% tanfanercept eyedrop was well-tolerated and showed statistically significant improvements in DED signs and symptoms, specifically a reduction of inferior corneal staining and ocular burning in comparison to placebo treatment. 223 Two Phase 3 trials, VELOS-2 (NCT03846453) and VELOS-3 (NCT05109702) have recently been completed, and a Phase 3 study (NCT04633213) in Chinese subjects is currently recruiting. 225
Isunakinra (EBI-005)
Isunakinra, formerly known as EBI-005 (Eleven Biotherapeutics, Inc., MA, USA), is a chimera of protein sequences from human IL-1β and IL-1 receptor antagonist (IL-1Ra or anakinra), which bind and inhibit the IL-1 receptor and thus block signaling. 226 IL-1 is a cytokine already known for its proinflammatory properties and its role in DED-associated ocular inflammation. 225 In a Phase 3 clinical trial (NCT01998802), Isunakinra demonstrated a favorable safety profile and was well-tolerated by the study participants. Moreover, it exhibited statistically significant improvements when compared with baseline measurements in addressing the signs and symptoms of DED during the 12-week treatment period. However, it is worth noting that no statistically significant differences were observed between the Isunakinra-treated group and the vehicle-only group with respect to the study endpoints. 227
Conclusion
Although the role of inflammation in the pathogenesis of the vicious circle of DED is becoming increasingly more obvious, the relation between clinical markers of DED and inflammation remains a classical chicken-and-egg conundrum. Recent evidence has overwhelmingly demonstrated the involvement of an inflammatory component in the various DED subtypes, and it is now established that inflammation often plays a causal rather than casual role in the manifestation of the disease. Here, we have discussed the involvement of inflammation in various DED subtypes and the diagnostic tools currently available to specifically characterize inflammation. Furthermore, the application of preclinical models in elucidating the role of inflammation in DED and preclinical evaluation of therapeutic interventions to specifically tackle the inflammatory component has been highlighted. A major limitation of many of the currently utilized animal models is that the method of disease induction is not clinically relevant bearing poor construct validity, which may influence our understanding of the disease pathogenesis and the therapeutic response observed with experimental therapeutics. Finally, this review has discussed pharmacological interventions targeting inflammation that are currently available and in the pipeline to manage the inflammatory component of DED more effectively.
Footnotes
Acknowledgments
The authors thank the Health Research Council of New Zealand for supporting S.B.’s doctoral scholarship and P.A.’s salary [20/317].
Authors’ Contributions
S.B.: Visualization, investigation, and writing—original draft. I.D.R.: Resources, funding acquisition, conceptualization, writing—reviewing and editing, supervision, and project administration. P.A.: Conceptualization, visualization, investigation, supervision, and writing—reviewing and editing.
Author Disclosure Statement
S.B.’s doctoral scholarship and P.A.’s salary were funded by the Health Research Council of New Zealand [20/317]. I.D.R.’s directorship was funded by the Buchanan Charitable Foundation. The authors declare no conflict of interest.
Funding Information
This research was funded by the Health Research Council of New Zealand Grant (Grant number: 20/317).